
Management of Traumatic Femur Fractures: A Focus on the Time to Intramedullary Nailing and Clinical Outcomes
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ghouri, S.; Asim, M.; Mustafa, F.; Kanbar, A.; Ellabib, M.; Al Jogol, H.; Muneer, M.; Abdurraheim, N.; Goel, A.; Abdelrahman, H.; et al. Patterns, Management, and Outcome of Traumatic Femur Fracture: Exploring the Experience of the Only Level 1 Trauma Center in Qatar. Int. J. Environ. Res. Public Health 2021, 18, 5916. [Google Scholar] [CrossRef]
- Bäcker, H.C.; Heyland, M.; Wu, C.H.; Perka, C.; Stöckle, U.; Braun, K.F. Breakage of intramedullary femoral nailing or femoral plating: How to prevent implant failure. Eur. J. Med. Res. 2022, 27, 7. [Google Scholar] [CrossRef] [PubMed]
- Yoon, R.S.; Liporace, F.A. Impact of Intramedullary Nailing in the Treatment of Femur Fractures An Evolutionary Perspective. Bull. Hosp. Jt. Dis. 2018, 76, 9–13. [Google Scholar]
- O’Brien, P.J. Fracture fixation in patients having multiple injuries. Can. J. Surg. 2003, 46, 124–128. [Google Scholar] [PubMed]
- Denisiuk, M.; Afsari, A. Femoral Shaft Fractures. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Enninghorst, N.; McDougall, D.; Evans, J.A.; Sisak, K.; Balogh, Z.J. Population-based epidemiology of femur shaft fractures. J. Trauma Acute Care Surg. 2013, 74, 1516–1520. [Google Scholar] [CrossRef] [PubMed]
- Xiong, R.; Mai, Q.-G.; Yang, C.-L.; Ye, S.-X.; Zhang, X.; Fan, S.-C. Intramedullary nailing for femoral shaft fractures in adults. Cochrane Database Syst. Rev. 2018, 2018, CD010524. [Google Scholar] [CrossRef]
- Hamahashi, K.; Uchiyama, Y.; Kobayashi, Y.; Ebihara, G.; Ukai, T.; Watanabe, M. Clinical outcomes of intramedullary nailing of femoral shaft fractures with third fragments: A retrospective analysis of risk factors for delayed union. Trauma Surg. Acute Care Open 2019, 4, e000203. [Google Scholar] [CrossRef] [Green Version]
- Zlowodzki, M.; Prakash, J.S.; Aggarwal, N.K. External fixation of complex femoral shaft fractures. Int. Orthop. 2007, 31, 409–413. [Google Scholar] [CrossRef] [Green Version]
- El-Menyar, A.; Muneer, M.; Samson, D.; Al-Thani, H.; Alobaidi, A.; Mussleman, P.; Latifi, R. Early versus late intramedullary nailing for traumatic femur fracture management: Meta-analysis. J. Orthop. Surg. Res. 2018, 13, 160, Erratum in J. Orthop. Surg. Res. 2018, 13, 182. [Google Scholar] [CrossRef] [Green Version]
- Davidson, A.; Houri, S.S.; Cohen, J.; Feldman, G.; Mosheiff, R.; Liebergall, M.; Weil, Y.A. Initial definitive treatment of open femoral shaft fractures with retrograde nailing—Is it safe? A retrospective analysis comparing antegrade to retrograde nailing. Injury 2022, 53, 1231–1236. [Google Scholar] [CrossRef]
- Blair, J.A.; Kusnezov, N.; Fisher, T.; Prabhakar, G.; Bader, J.O.; Belmont, P.J. Early Stabilization of Femur Fractures in the Setting of Polytrauma Is Associated with Decreased Risk of Pulmonary Complications and Mortality. J. Surg. Orthop. Adv. 2019, 28, 137–143. [Google Scholar] [PubMed]
- Lempert, M.; Halvachizadeh, S.; Ellanti, P.; Pfeifer, R.; Hax, J.; Jensen, K.; Pape, H.-C. Incidence of Fat Embolism Syndrome in Femur Fractures and Its Associated Risk Factors over Time—A Systematic Review. J. Clin. Med. 2021, 10, 2733. [Google Scholar] [CrossRef] [PubMed]
- Young, S.; Banza, L.N.; Hallan, G.; Beniyasi, F.; Manda, K.G.; Munthali, B.S.; Dybvik, E.; Engesæter, L.B.; Havelin, L.I. Complications after intramedullary nailing of femoral fractures in a low-income country. Acta Orthop. 2013, 84, 460–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedi, A.; Karunakar, M.A. Physiologic effects of intramedullary reaming. Instr. Course Lect. 2006, 55, 359–366. [Google Scholar]
- Karaman, O.; Ayhan, E.; Kesmezacar, H.; Seker, A.; Unlu, M.C.; Aydingoz, O. Rotational malalignment after closed intramedullary nailing of femoral shaft fractures and its influence on daily life. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 1243–1247. [Google Scholar] [CrossRef]
- Paterno, M.V.; Archdeacon, M.T. Is There a Standard Rehabilitation Protocol after Femoral Intramedullary Nailing? J. Orthop. Trauma 2009, 23 (Suppl. S5), S39–S46. [Google Scholar] [CrossRef]
- Paterno, M.V.; Archdeacon, M.T.; Ford, K.R.; Galvin, D.; Hewett, T.E. Early Rehabilitation following Surgical Fixation of a Femoral Shaft Fracture. Phys. Ther. 2006, 86, 558–572. [Google Scholar] [CrossRef] [Green Version]
- Röder, F.; Schwab, M.; Aleker, T.; Mörike, K.; Thon, K.P.; Klotz, U. Proximal femur fracture in older patients–rehabilitation and clinical outcome. Age Ageing 2003, 32, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Wu, K.-J.; Li, S.-H.; Yeh, K.-T.; Chen, I.-H.; Lee, R.-P.; Yu, T.-C.; Peng, C.-H.; Liu, K.-L.; Yao, T.-K.; Wang, J.-H.; et al. The risk factors of nonunion after intramedullary nailing fixation of femur shaft fracture in middle age patients. Medicine 2019, 98, e16559. [Google Scholar] [CrossRef]
- Dhar, S.A.; Gani, N.U.; Butt, M.F.; Farooq, M.; Mir, M.R. Delayed union of an operated fracture of the femoral neck. J. Orthop. Traumatol. 2008, 9, 97–99. [Google Scholar] [CrossRef] [Green Version]
- Somford, M.P.; van den Bekerom, M.P.; Kloen, P. Operative treatment for femoral shaft nonunions, a systematic review of the literature. Strateg. Trauma Limb Reconstr. 2013, 8, 77–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alobaidi, A.S.; Al-Hassani, A.; El-Menyar, A.; Abdelrahman, H.; Tuma, M.; Al-Thani, H.; Aldosari, M.A. Early and late intramedullary nailing of femur fracture: A single center experience. Int. J. Crit. Illn. Inj. Sci. 2016, 6, 143–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, H.; Yu, H.; Zhu, Y.; Xiang, L.; Wang, H. Effect of Age on the Patterns of Traumatic Femoral Fractures: Seven Years of Experience at a Regional Tertiary Hospital. Orthop. Surg. 2022, 14, 2132–2140. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Merchan, E.C.; Moraleda, L.; Gomez-Cardero, P. Injuries associated with femoral shaft fractures with special emphasis on occult injuries. Arch. Bone Jt. Surg. 2013, 1, 59–63. [Google Scholar]
- Salminen, S.T.; Pihlajamäki, H.K.; Avikainen, V.J.; Böstman, O.M. Population Based Epidemiologic and Morphologic Study of Femoral Shaft Fractures. Clin. Orthop. Relat. Res. 2000, 372, 241–249. [Google Scholar] [CrossRef]
- Sonbol, A.M.; Almulla, A.A.; Hetaimish, B.M.; Taha, W.S.; Mohmmedthani, T.S.; Alfraidi, T.A.; Alrashidi, Y.A. Prevalence of femoral shaft fractures and associated injuries among adults after road traffic accidents in a Saudi Arabian trauma center. J. Musculoskelet. Surg. Res. 2018, 2, 62–65. [Google Scholar] [CrossRef]
- Kuhmola, A.; Simons, T.; Handolin, L.; Brinck, T. Surgical strategy for femoral shaft fractures in severely injured patients: A 13-year experience from a tertiary trauma centre. Injury 2021, 52, 956–960. [Google Scholar] [CrossRef]
- Ibeanusi, S.E.; Chioma, J. Pattern and Outcome of Femoral Fractures Treated in a Regional Trauma Centre in South South, Nigeria. Int. Arch. Orthop. Surg. 2019, 2, 006. [Google Scholar] [CrossRef]
- Reynders, P.A.; Broos, P.L. Healing of closed femoral shaft fractures treated with the AO unreamed femoral nail. A comparative study with the AO reamed femoral nail. Injury 2000, 31, 367–371. [Google Scholar] [CrossRef]
- Morshed, S.; Mikhail, C.; Iii, T.M. Timing of Femoral Shaft Fracture Fixation Affects Length of Hospital Stay in Patients with Multiple Injuries. Open Orthop. J. 2015, 9, 324–331. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.C.; Jung, K.H.; Kyoung, K.H.; Choi, S.H. The Timing of Femur Fracture Fixation is an Important Factor for Prolonged Mechanical Ventilation. J. Trauma Inj. 2019, 32, 220–225. [Google Scholar] [CrossRef] [Green Version]
- Rixen, D.; Grass, G.; Sauerland, S.; Lefering, R.; Raum, M.R.; Yücel, N.; Bouillon, B.; Neugebauer, E.A.M.; Polytrauma Study Group of the German Trauma Society. Evaluation of Criteria for Temporary External Fixation in Risk-Adapted Damage Control Orthopedic Surgery of Femur Shaft Fractures in Multiple Trauma Patients: “Evidence-Based Medicine” versus “Reality” in the Trauma Registry of the German Trauma Society. J. Trauma Inj. Infect. Crit. Care 2005, 59, 1375–1395. [Google Scholar] [CrossRef]
- Mitchell, S.M.; Chung, A.S.; Walker, J.B.; Hustedt, J.W.; Russell, G.V.; Jones, C.B. Delay in Hip Fracture Surgery Prolongs Postoperative Hospital Length of Stay but Does Not Adversely Affect Outcomes at 30 Days. J. Orthop. Trauma 2018, 32, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Pincus, D.; Ravi, B.; Wasserstein, D.; Huang, A.; Paterson, J.M.; Nathens, A.B.; Kreder, H.J.; Jenkinson, R.J.; Wodchis, W.P. Association Between Wait Time and 30-Day Mortality in Adults Undergoing Hip Fracture Surgery. JAMA 2017, 318, 1994–2003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scalea, T.M.; Boswell, S.A.; Scott, J.D.; Mitchell, K.A.; Kramer, M.E.; Pollak, A.N. External Fixation as a Bridge to Intramedullary Nailing for Patients with Multiple Injuries and with Femur Fractures: Damage Control Orthopedics. J. Trauma Inj. Infect. Crit. Care 2000, 48, 613–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowotarski, P.J.; Turen, C.H.; Brumback, R.J.; Scarboro, J.M. Conversion of external fixation to intramedullary nailing for fractures of the shaft of the femur in multiply injured patients. J. Bone Jt. Surg. 2000, 82, 781–788. [Google Scholar] [CrossRef]
- Volpin, G.; Pfeifer, R.; Saveski, J.; Hasani, I.; Cohen, M.; Pape, H.-C. Damage control orthopaedics in polytraumatized patients- current concepts. J. Clin. Orthop. Trauma 2021, 12, 72–82. [Google Scholar] [CrossRef]
- Alonso, J.; Geissler, W.; Hughes, J.L. External fixation of femoral fractures: Indications and limitations. Clin. Orthop. Relat. Res. 1989, 241, 83–88. [Google Scholar] [CrossRef]
- Cunningham, B.P.; Brazina, S.; Morshed, S.; Miclau, T., 3rd. Fracture healing: A review of clinical, imaging and laboratory diagnostic options. Injury 2017, 48 (Suppl. S1), S69–S75. [Google Scholar] [CrossRef]
- Ma, Y.-G.; Hu, G.-L.; Hu, W.; Liang, F. Surgical factors contributing to nonunion in femoral shaft fracture following intramedullary nailing. Chin. J. Traumatol. 2016, 19, 109–112. [Google Scholar] [CrossRef]
- Pihlajamäki, H.K.; Salminen, S.T.; Böstman, O.M. The Treatment of Nonunions Following Intramedullary Nailing of Femoral Shaft Fractures. J. Orthop. Trauma 2002, 16, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Papadokostakis, G.; Papakostidis, C.; Dimitriou, R.; Giannoudis, P.V. The role and efficacy of retrograding nailing for the treatment of diaphyseal and distal femoral fractures: A systematic review of the literature. Injury 2005, 36, 813–822. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.S.; Jensen, N.M.; Gundtoft, P.H.; Kold, S.; Zura, R.; Viberg, B. Risk factors for nonunion following surgically managed, traumatic, diaphyseal fractures: A systematic review and meta-analysis. EFORT Open Rev. 2022, 7, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Wertheimer, A.; Olaussen, A.; Perera, S.; Liew, S.; Mitra, B. Fractures of the femur and blood transfusions. Injury 2018, 49, 846–851. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Choi, D.-H.; Ahn, S.; Sohn, C.H.; Seo, D.-W.; Kim, W.Y. Timing of pulmonary embolisms in femur fracture patients: Incidence and outcomes. J. Trauma Acute Care Surg. 2016, 80, 952–956. [Google Scholar] [CrossRef]
- Nahm, N.J.; Como, J.; Wilber, J.H.; Vallier, H.A. Early Appropriate Care: Definitive Stabilization of Femoral Fractures Within 24 Hours of Injury Is Safe in Most Patients with Multiple Injuries. J. Trauma Inj. Infect. Crit. Care 2011, 71, 175–185. [Google Scholar] [CrossRef]
- Oliveira, P.R.; Leonhardt, M.C.; Carvalho, V.C.; Kojima, K.E.; Silva, J.S.; Rossi, F.; Lima, A.L.L. Incidence and risk factors associated with infection after intramedullary nailing of femoral and tibial diaphyseal fractures: Prospective study. Injury 2018, 49, 1905–1911. [Google Scholar] [CrossRef]
- Young, S.; Lie, S.A.; Hallan, G.; Zirkle, L.G.; Engesæter, L.B.; Havelin, L.I. Risk Factors for Infection after 46,113 Intramedullary Nail Operations in Low- and Middle-income Countries. World J. Surg. 2013, 37, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Kobbe, P.; Micansky, F.; Lichte, P.; Sellei, R.M.; Pfeifer, R.; Dombroski, D.; Lefering, R.; Pape, H.C.; The TraumaRegister DGU. Increased morbidity and mortality after bilateral femoral shaft fractures: Myth or reality in the era of damage control? Injury 2013, 44, 221–225. [Google Scholar] [CrossRef]
- Wolf, O.; Mukka, S.; Ekelund, J.; Möller, M.; Hailer, N.P. How deadly is a fracture distal to the hip in the elderly? An observational cohort study of 11,799 femoral fractures in the Swedish Fracture Register. Acta Orthop. 2021, 92, 40–46. [Google Scholar] [CrossRef]
- Basile, G. Remarks on the management of proximal femoral fractures in times of COVID-19 pandemic. Clin Ter. 2022, 173, 398–399. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Value | Variables | Value |
|---|---|---|---|
| Age (mean ± SD) | 34.5 ± 15.8 | Abbreviated injury scores (AIS) | |
| Males | 607 (90.9%) | Head AIS | 3.2 ± 1.0 |
| Females | 61(9.1%) | Chest AIS | 2.6 ± 0.8 |
| Mechanism of Injury | Abdominal AIS | 2.5 ± 0.9 | |
| Road traffic accidents | 359 (53.7%) | Spine AIS | 2.0 ± 0.3 |
| Fall from height | 159 (23.8%) | Lower extremity AIS | 3.0 ± 0.1 |
| Pedestrian | 71 (10.6%) | Pelvis AIS | 2.3 ± 0.7 |
| Fall of heavy object | 41 (6.1%) | Hemoglobin level (n = 509) | 12.7 ± 2.2 |
| All-terrain vehicle | 13 (1.9%) | White blood cell count (n = 488) | 15.9 ± 6.9 |
| Others | 25 (3.7%) | Neutrophil (n = 255) | 49.0 ± 34.6 |
| Co-morbidities | Platelets count (n = 499) | 247 ± 88 | |
| Diabetes mellitus | 61 (9.1%) | INR (n = 466) | 1.13 ± 0.16 |
| Hypertension | 56 (8.4%) | X-ray | 621 (93.0%) |
| Asthma | 5 (0.7%) | Pan CT scan | 554 (82.9%) |
| Coronary Artery Disease | 19 (2.8%) | Blood transfusion | 334 (50.0%) |
| Initial heart rate | 94.8 ± 21.4 | Blood units transfused | 4 (1–55) |
| Initial systolic blood pressure | 122.4 ± 23.3 | Complications | |
| Body temperature | 36.7 ± 0.5 | Pneumonia | 30 (4.5%) |
| Respiratory rate | 19.7 ± 5.5 | Wound Infection | 29 (4.3%) |
| Initial Glasgow coma scale | 15 (3–15) | Acute Respiratory Distress Syndrome | 17 (2.5%) |
| Injury Severity Score | 16.9 ± 9.1 | Pulmonary Embolism | 15 (2.2%) |
| Associated injuries | Acute renal failure | 14 (2.1%) | |
| Chest | 239 (35.8%) | Sepsis | 11 (1.6%) |
| Pelvis | 173 (25.9%) | Hospital length of stay | 10 (1–185) |
| Spine | 170 (25.4%) | intensive care unit stay days | 4 (1–112) |
| Head | 139 (20.8%) | Mortality | 23 (3.4%) |
| Abdomen | 136 (20.4%) | ||
| Tibia | 121 (18.1%) | ||
| Fibula | 71 (10.6%) | ||
| Ankle | 54 (8.1%) | ||
| Knee | 64 (9.6%) |
| Variables | Value | Variables | Value |
|---|---|---|---|
| DVT prophylaxis (n = 639) | 520 (81.4%) | Time to IMN; hours; (n = 480) * | |
| Unilateral femur fracture | 623 (93.3%) | <12 H | 149 (31.0%) |
| Bilateral femur fracture | 45 (6.7%) | 12–24 H | 161 (33.5%) |
| Type of Fracture (n = 640) | >24 H | 170 (35.4%) | |
| Close fracture | 540 (84.4%) | External fixation prior to IMN | 68 (13.8%) |
| Open fracture | 100 (15.6%) | Implant type (n = 435) | |
| Site of fracture | Antegrade nail | 365 (83.9%) | |
| Proximal | 231 (34.6%) | Retrograde nail | 70 (16.1%) |
| Diaphyseal | 471 (70.5%) | Site of entry (n = 502) | |
| Distal | 100 (15.0%) | Trochanteric | 385 (76.7%) |
| AO classification | Piriformis | 60 (12.0%) | |
| 31A | 97 (14.5%) | Retrograde | 57 (11.4%) |
| 31B | 36 (5.4%) | Locking (n = 489) | 457 (93.5%) |
| 31C | 16 (2.4%) | Number of procedures (n = 602) | 1 (1–6) |
| 32A | 202 (30.2%) | Fracture outcomes | |
| 32B | 157 (23.5%) | Union | 513 (76.8%) |
| 32C | 93 (13.9%) | Delayed union | 28 (4.2%) |
| 33A | 23 (3.4%) | Non-union | 22 (3.3%) |
| 33B | 17 (2.5%) | Lost to follow-up | 82 (12.3%) |
| 33C | 27 (4.0%) | Died before fixation | 23 (3.4%) |
| Reamed IMN | 483 (72.3%) |
| Time to Intramedullary Nailing | p Value | |||
|---|---|---|---|---|
| Group-1 <12 h (n = 149) | Group-2 12–24 h (n = 161) | Group-3 >24 h (n = 170) | ||
| Age (mean ± SD) | 31.2 ± 11.2 | 31.2 ± 14.5 | 31.7 ± 11.9 | 0.78 |
| Males; N (%) | 137 (91.9%) | 143 (88.8%) | 158 (92.9%) | 0.38 |
| Initial GCS (mean, 95%CI) | 14.1 (13.6–14.6) | 14.5 (14.2–14.8) | 12.5 (11.8–13.2) | 0.001 |
| Injury Severity Score | 14.5 ± 6.8 | 13.8 ± 5.7 | 20.4 ± 9.6 | 0.001 |
| Associated injuries; N (%) | ||||
| Chest | 37 (24.8%) | 41 (25.5%) | 89 (52.4%) | 0.001 |
| Pelvis | 26 (17.4%) | 24 (14.9%) | 66 (38.8%) | 0.001 |
| Spine | 30 (20.1%) | 31 (19.3%) | 62 (36.5%) | 0.001 |
| Head | 19 (12.8%) | 14 (8.7%) | 53 (31.2%) | 0.001 |
| Abdomen | 16 (10.7%) | 19 (11.8%) | 62 (36.5%) | 0.001 |
| Lower extremity AIS | 3.0 ± 0.1 | 3.0 ± 0.0 | 3.0 ± 0.0 | 0.10 |
| Pelvis AIS | 2.1 ± 0.3 | 2.3 ± 0.6 | 2.2 ± 0.5 | 0.46 |
| Head AIS | 3.05 ± 0.9 | 2.9 ± 0.9 | 3.3 ± 0.8 | 0.36 |
| DVT prophylaxis (n = 474) | 119 (80.4%) | 132 (82.5%) | 141 (84.9%) | 0.56 |
| Unilateral femur fracture | 142 (95.3%) | 158 (98.1%) | 147 (86.5%) | 0.001 for all |
| Bilateral femur fracture | 7 (4.7%) | 3 (1.9%) | 23 (13.5%) | |
| Type of fracture | ||||
| Close fracture | 125 (83.9%) | 141 (87.6%) | 144 (84.7%) | 0.62 for all |
| Open fracture | 24 (16.1%) | 20 (12.4%) | 26 (15.3%) | |
| AO classification | ||||
| 31A | 14 (9.4%) | 18 (11.2%) | 14 (8.2%) | 0.04 for all |
| 31B | 1 (0.7%) | 0 (0.0%) | 2 (1.2%) | |
| 31C | 2 (1.3%) | 1 (0.6%) | 0 (0.0%) | |
| 32A | 60 (40.3%) | 72 (44.7%) | 57 (33.5%) | |
| 32B | 49 (32.9%) | 48 (29.8%) | 46 (27.1%) | |
| 32C | 22 (14.8%) | 19 (11.8%) | 41 (24.1%) | |
| 33A | 1 (0.7%) | 2 (1.2%) | 4 (2.4%) | |
| 33B | 0 (0.0%) | 1 (0.6%) | 3 (1.8%) | |
| 33C | 0 (0.0%) | 0 (0.0%) | 3 (1.8%) | |
| Site of entry | ||||
| Trochanteric | 121 (81.2%) | 125 (77.6%) | 120 (70.6%) | 0.23 for all |
| Piriformis | 14 (9.4%) | 20 (12.4%) | 25 (14.7%) | |
| Retrograde | 14 (9.4%) | 16 (9.9%) | 25 (14.7%) | |
| Implant type (n = 429) | ||||
| Antegrade nail | 118 (85.5%) | 122 (87.8%) | 121 (79.6%) | 0.14 for all |
| Retrograde nail | 20 (14.5%) | 17 (12.2%) | 31 (20.4%) | |
| External fixation prior to IMN | 9 (6.0%) | 3 (1.9%) | 55 (32.4%) | 0.001 |
| Fracture outcomes | ||||
| Union | 121 (81.2%) | 144 (89.4%) | 146 (85.9%) | 0.13 for all |
| Delayed union | 7 (4.7%) | 5 (3.1%) | 11 (6.5%) | |
| Nonunion | 5 (3.4%) | 6 (3.7%) | 3 (1.8%) | |
| Lost to follow-up | 16 (10.7%) | 6 (3.7%) | 10 (5.9%) | |
| Blood transfusion | 58 (38.9%) | 61 (37.9%) | 117 (68.8%) | 0.001 |
| Blood units transfused | 4 (1–41) | 2 (1–29) | 6 (1–55) | 0.001 |
| Complications | ||||
| Wound infection | 5 (3.4%) | 0 (0.0%) | 15 (8.8%) | 0.001 |
| Sepsis | 1 (0.7%) | 0 (0.0%) | 4 (2.4%) | 0.09 |
| Pulmonary Embolism | 1 (0.7%) | 4 (2.5%) | 8 (4.7%) | 0.08 |
| Acute Respiratory Distress Syndrome | 2 (1.3%) | 0 (0.0%) | 8 (4.7%) | 0.008 |
| Acute renal failure | 1 (0.7%) | 0 (0.0%) | 4 (2.4%) | 0.09 |
| Pneumonia | 3 (2.0%) | 3 (1.9%) | 13 (7.6%) | 0.009 |
| ICU stay; days | 4 (1–26) | 2 (1–62) | 7 (1–112) | 0.001 |
| Hospital length of stay; days | 8 (1–85) | 7 (2–79) | 19 (1–134) | 0.001 |
| Union (n = 513) | Delayed Union * (n = 28) | Nonunion ** (n = 22) | p Value | |
|---|---|---|---|---|
| Age (mean ± SD) years | 33.6 ± 15.4 | 35.6 ± 13.6 | 36.9 ± 14.2 | 0.51 |
| <50 years | 445 (86.9%) | 25 (89.3%) | 19 (86.4%) | 0.93 for all |
| ≥50 years | 67 (13.1%) | 3 (10.7%) | 3 (13.6%) | |
| Hypertension | 42 (8.2%) | 4 (14.3%) | 2 (9.1%) | 0.52 |
| Diabetes mellitus | 48 (9.4%) | 2 (7.1%) | 2 (9.1%) | 0.92 |
| Injury Severity Score (ISS) | 16.5 ± 8.7 | 13.8 ± 5.2 | 14.5 ± 5.9 | 0.14 |
| ISS > 15 | 206 (40.2%) | 6 (21.4%) | 8 (36.4%) | 0.13 |
| Associated injuries | ||||
| Tibia | 91 (17.7%) | 6 (21.4%) | 4 (18.2%) | 0.88 |
| Fibula | 51 (9.9%) | 3 (10.7%) | 2 (9.1%) | 0.98 |
| Pelvis | 128 (25.0%) | 6 (21.4%) | 8 (36.4%) | 0.43 |
| Unilateral femur fracture | 482 (94.0%) | 24 (85.7%) | 17 (77.3%) | 0.003 for all |
| Bilateral femur fracture | 31 (6.0%) | 4 (14.3%) | 5 (22.7%) | |
| Type of fracture | ||||
| Close fracture | 442 (86.2%) | 20 (71.4%) | 18 (81.8%) | 0.09 for all |
| Open fracture | 71 (13.8%) | 8 (28.6%) | 4 (18.2%) | |
| Implant type (n = 405) | ||||
| Antegrade nail | 321 (86.3%) | 13 (68.4%) | 9 (64.3%) | 0.01 for all |
| Retrograde nail | 51 (13.7%) | 6 (31.6%) | 5 (35.7%) | |
| Site of entry (n = 466) | ||||
| Trochanteric | 333 (77.6%) | 17 (73.9%) | 10 (71.4%) | 0.005 for all |
| Piriformis | 56 (13.1%) | 0 (0.0%) | 0 (0.0%) | |
| Retrograde | 40 (9.3%) | 6 (26.1%) | 4 (28.6%) | |
| Reamed IMN | 414 (80.7%) | 23 (82.1%) | 14 (63.6%) | 0.14 |
| Site of fracture | ||||
| Proximal | 172 (33.5%) | 9 (32.1%) | 8 (36.4%) | 0.95 |
| Diaphyseal | 383 (74.7%) | 21 (75.0%) | 14 (63.6%) | 0.50 |
| Distal | 60 (11.6%) | 6 (21.4%) | 5 (22.7%) | 0.11 |
| AO classification | ||||
| 31A | 69 (13.5%) | 2 (7.1%) | 4 (18.2%) | 0.04 for all |
| 31B | 24 (4.7%) | 3 (10.7%) | 2 (9.1%) | |
| 31C | 13 (2.5%) | 0 (0.0%) | 0 (0.0%) | |
| 32A | 174 (33.9%) | 4 (14.3%) | 2 (9.1%) | |
| 32B | 122 (23.8%) | 11 (39.3%) | 7 (31.8%) | |
| 32C | 73 (14.2%) | 4 (14.3%) | 4 (18.2%) | |
| 33A | 13 (2.5%) | 3 (10.7%) | 0 (0.0%) | |
| 33B | 12 (2.3%) | 0 (0.0%) | 1 (4.5%) | |
| 33C | 13 (2.5%) | 1 (3.6%) | 2 (9.1%) | |
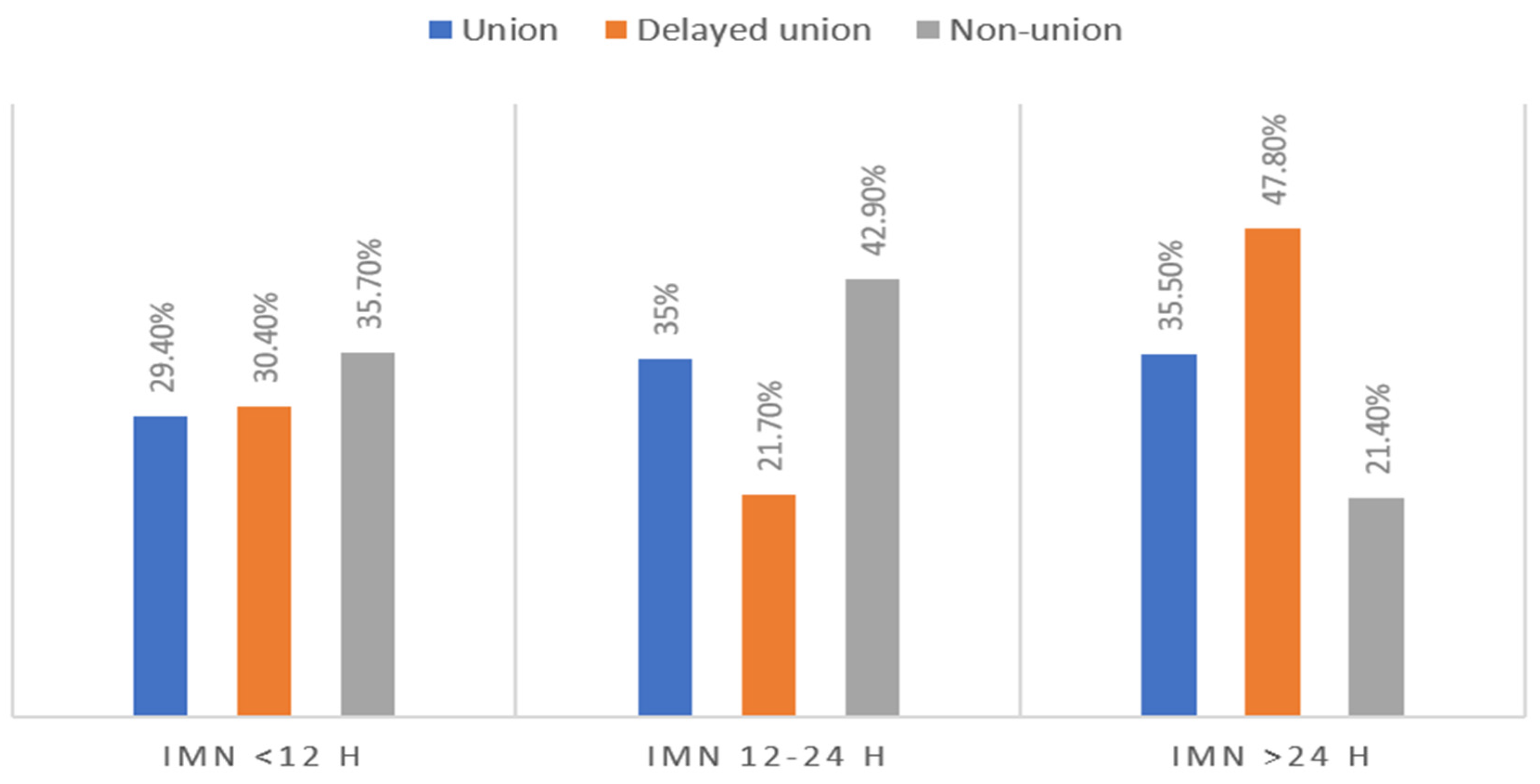
| Time to IMN (hours) | ||||
| <12 | 121 (29.4%) | 7 (30.4%) | 5 (35.7%) | 0.50 for all |
| 12–24 | 144 (35.0%) | 5 (21.7%) | 6 (42.9%) | |
| >24 | 146 (35.5%) | 11 (47.8%) | 3 (21.4%) | |
| External fixation prior to IMN | 61 (14.6%) | 4 (17.4%) | 1 (7.1%) | 0.68 |
| Wound Infection | 22 (4.3%) | 2 (7.1%) | 2 (9.1%) | 0.46 |
| Hospital length of stay | 10 (1–185) | 8 (2–127) | 10.5 (2–129) | 0.32 |
| ICU LOS | 4 (1–112) | 3 (1–16) | 2 (1–30) | 0.11 |
| Open Fractures (n = 26) | Number of Procedures |
|---|---|
| Open reduction and internal fixation (ORIF) | 7 |
| External fixation | 5 |
| Plate and screw fixation | 6 |
| External fixation, screw and plate | 2 |
| External fixation and wound debridement | 1 |
| Plate cementing | 1 |
| Wound debridement and exploration | 1 |
| ORIF and wound debridement | 1 |
| Skeletal traction | 1 |
| Vascular repair | 1 |
| Closed fractures (n = 136) | |
| Conservative | 31 |
| Open reduction and internal fixation | 20 |
| Plate and Screw | 18 |
| Closed reduction | 16 |
| Screw fixation | 13 |
| Dynamic Hip Screw (DHS) | 12 |
| External fixation | 7 |
| Hemiarthroplasty and DHS | 5 |
| Skeletal traction | 4 |
| Plate and wire | 2 |
| External fixation and ORIF | 2 |
| Screw fixation | 1 |
| K-wire and screw fixation | 1 |
| Peri-loc plating | 1 |
| Cannulated hip screw fixation of femur neck | 1 |
| Cemented left hip Bipolar hemiarthroplasty | 1 |
| Calcaneal fracture fixation | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghouri, S.I.; Mustafa, F.; Kanbar, A.; Al Jogol, H.; Shunni, A.; Almadani, A.; Abdurraheim, N.; Goel, A.P.; Abdelrahman, H.; Babikir, E.; et al. Management of Traumatic Femur Fractures: A Focus on the Time to Intramedullary Nailing and Clinical Outcomes. Diagnostics 2023, 13, 1147. https://doi.org/10.3390/diagnostics13061147
Ghouri SI, Mustafa F, Kanbar A, Al Jogol H, Shunni A, Almadani A, Abdurraheim N, Goel AP, Abdelrahman H, Babikir E, et al. Management of Traumatic Femur Fractures: A Focus on the Time to Intramedullary Nailing and Clinical Outcomes. Diagnostics. 2023; 13(6):1147. https://doi.org/10.3390/diagnostics13061147
Chicago/Turabian StyleGhouri, Syed Imran, Fuad Mustafa, Ahad Kanbar, Hisham Al Jogol, Adam Shunni, Ammar Almadani, Nuri Abdurraheim, Atirek Pratap Goel, Husham Abdelrahman, Elhadi Babikir, and et al. 2023. "Management of Traumatic Femur Fractures: A Focus on the Time to Intramedullary Nailing and Clinical Outcomes" Diagnostics 13, no. 6: 1147. https://doi.org/10.3390/diagnostics13061147
APA StyleGhouri, S. I., Mustafa, F., Kanbar, A., Al Jogol, H., Shunni, A., Almadani, A., Abdurraheim, N., Goel, A. P., Abdelrahman, H., Babikir, E., Ramzee, A. F., Ahmed, K., Alhardallo, M., Asim, M., Al-Thani, H., & El-Menyar, A. (2023). Management of Traumatic Femur Fractures: A Focus on the Time to Intramedullary Nailing and Clinical Outcomes. Diagnostics, 13(6), 1147. https://doi.org/10.3390/diagnostics13061147