
Evaluation of a ddPCR Commercial Assay for the Absolute Quantification of the Monkeypox Virus West Africa in Clinical Samples

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting of the Study
2.2. Automated DNA Extraction
2.3. ddPCR
2.4. Limit of Detection Analysis
2.5. Statistics
3. Results
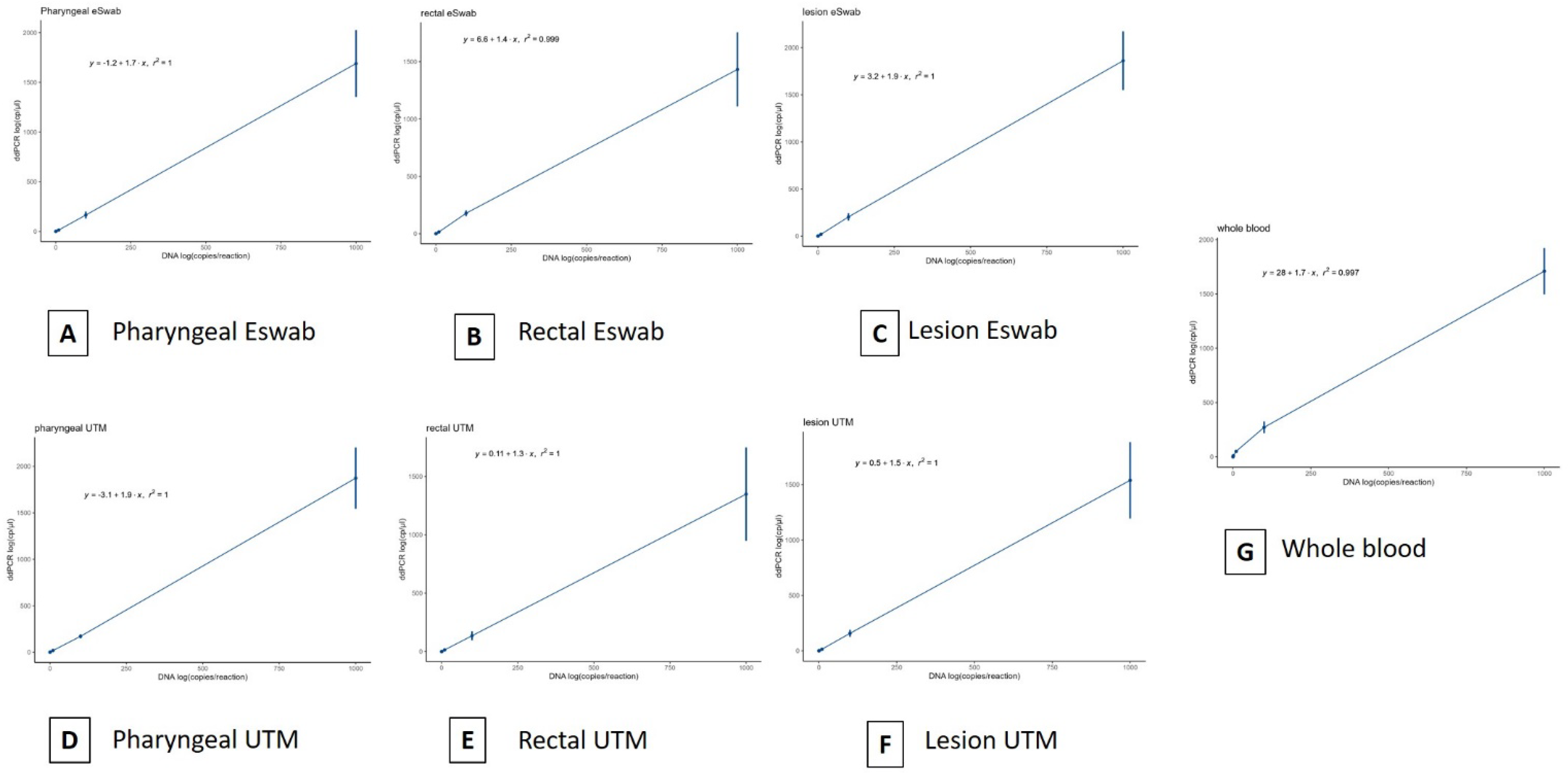
3.1. Limit of Detection Analysis and Assessment of Variability
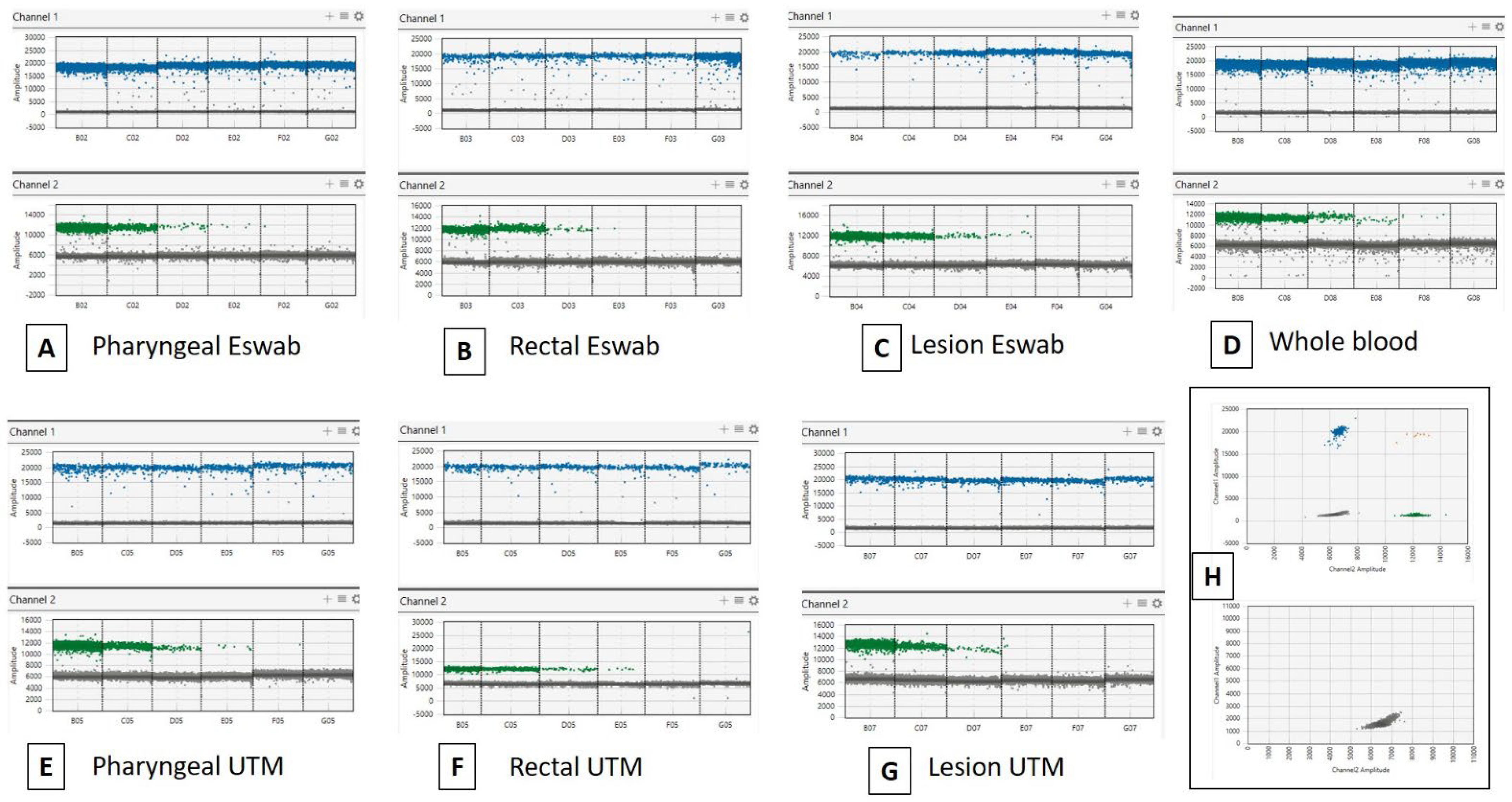
3.2. Clinical Samples
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, N.; Acharya, A.; Gendelman, H.E.; Byrareddy, S.N. The 2022 outbreak and the pathobiology of the monkeypox virus. J. Autoimmun. 2022, 131, 102855. [Google Scholar] [CrossRef]
- McCollum, A.M.; Shelus, V.; Hill, A.; Traore, T.; Onoja, B.; Nakazawa, Y.; Doty, J.B.; Yinka-Ogunleye, A.; Petersen, B.W.; Hutson, C.L.; et al. Epidemiology of Human Mpox—Worldwide, 2018–2021. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 68–72. [Google Scholar] [CrossRef]
- Isidro, J.; Borges, V.; Pinto, M.; Sobral, D.; Santos, J.D.; Nunes, A.; Mixão, V.; Ferreira, R.; Santos, D.; Duarte, S.; et al. Phylogenomic characterization and signs of microevolution in the 2022 multi-country outbreak of monkeypox virus. Nat. Med. 2022, 28, 1569–1572. [Google Scholar] [CrossRef]
- Velavan, T.P.; Meyer, C.G. Monkeypox 2022 outbreak: An update. Trop. Med. Int. Health 2022, 27, 604–605. [Google Scholar] [CrossRef]
- Likos, A.M.; Sammons, S.A.; Olson, V.A.; Frace, A.M.; Li, Y.; Olsen-Rasmussen, M.; Davidson, W.; Galloway, R.; Khristova, M.L.; Reynolds, M.G.; et al. A tale of two clades: Monkeypox viruses. J. Gen. Virol. 2005, 86, 2661–2672. [Google Scholar] [CrossRef]
- WHO. Laboratory Testing for the Monkeypox Virus. 2022. Available online: https://www.who.int/publications/i/item/WHO-MPX-laboratory-2022.1 (accessed on 12 March 2023).
- Brown, K.; Leggat, P.A. Human Monkeypox: Current State of Knowledge and Implications for the Future. Trop. Med. Infect. Dis. 2016, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Migaud, P.; Hosmann, K.; Drauz, D.; Mueller, M.; Haumann, J.; Stocker, H. A case of occupational transmission of mpox. Infection 2023, 3, 1–5. [Google Scholar] [CrossRef]
- Low, N.; Bachmann, L.H.; Ogoina, D.; McDonald, R.; Ipekci, A.M.; Quilter, L.A.S.; Cevik, M. Mpox virus and transmission through sexual contact: Defining the research agenda. PLoS Med. 2023, 20, e1004163. [Google Scholar] [CrossRef]
- Ndodo, N.; Ashcroft, J.; Lewandowski, K.; Yinka-Ogunleye, A.; Chukwu, C.; Ahmad, A.; King, D.; Akinpelu, A.; de Motes, C.M.; Ribeca, P.; et al. Different Coexisting Mpox Lineages Were Continuously Circulating in Humans Prior to 2022. bioRxiv 2023. [Google Scholar] [CrossRef]
- Allan-Blitz, L.T.; Gandhi, M.; Adamson, P.; Park, I.; Bolan, G.; Klausner, J.D. A Position Statement on Mpox as a Sexually Transmitted Disease. Clin. Infect. Dis. 2022, 22, ciac960. [Google Scholar] [CrossRef]
- Nuzzo, J.B.; Borio, L.L.; Gostin, L.O. The WHO Declaration of Monkeypox as a Global Public Health Emergency. JAMA 2022, 328, 615–617. [Google Scholar] [CrossRef]
- Lim, C.K.; Roberts, J.; Moso, M.; Liew, K.C.; Taouk, M.L.; Williams, E.; Tran, T.; Steinig, E.; Caly, L.; Williamson, D.A. Mpox diagnostics: Review of current and emerging technologies. J. Med. Virol. 2023, 95, e28429. [Google Scholar] [CrossRef]
- Peiró-Mestres, A.; Fuertes, I.; Camprubí-Ferrer, D.; Marcos, M.Á.; Vilella, A.; Navarro, M.; Rodriguez-Elena, L.; Riera, J.; Català, A.; Martínez, M.J.; et al. Frequent detection of monkeypox virus DNA in saliva, semen, and other clinical samples from 12 patients, Barcelona, Spain, May to June 2022. Euro Surveill. 2022, 27, 2200503. [Google Scholar] [CrossRef]
- Palich, R.; Burrel, S.; Monsel, G.; Nouchi, A.; Bleibtreu, A.; Seang, S.; Bérot, V.; Brin, C.; Gavaud, A.; Wakim, Y.; et al. Viral loads in clinical samples of men with monkeypox virus infection: A French case series. Lancet. Infect. Dis. 2023, 23, 74–80. [Google Scholar] [CrossRef]
- Coppens, J.; Vanroye, F.; Brosius, I.; Liesenborghs, L.; van Henten, S.; Vanbaelen, T.; Bracke, S.; Berens-Riha, N.; De Baetselier, I.; Kenyon, C.; et al. Alternative sampling specimens for the molecular detection of mpox (Formerly monkeypox) virus. J. Clin. Virol. 2023, 159, 105372. [Google Scholar] [CrossRef]
- Kojabad, A.A.; Farzanehpour, M.; Galeh, H.E.G.; Dorostkar, R.; Jafarpour, A.; Bolandian, M.; Nodooshan, M.M. Droplet digital PCR of viral DNA/RNA, current progress, challenges, and future perspectives. J. Med. Virol. 2021, 93, 4182–4197. [Google Scholar] [CrossRef]
- Chen, B.; Jiang, Y.; Cao, X.; Liu, C.; Zhang, N.; Shi, D. Droplet digital PCR as an emerging tool in detecting pathogens nucleic acids in infectious diseases. Clin. Chim. Acta 2021, 517, 156–161. [Google Scholar] [CrossRef]
- Carletti, F.; Di Caro, A.; Calcaterra, S.; Grolla, A.; Czub, M.; Ippolito, G.; Capobianchi, M.R.; Horejsh, D. Rapid, differential diagnosis of orthopox- and herpesviruses based upon real-time PCR product melting temperature and restriction enzyme analysis of amplicons. J. Virol. Methods 2005, 129, 97–100. [Google Scholar] [CrossRef]
- Americo, J.L.; Earl, P.L.; Moss, B. Droplet digital PCR for rapid enumeration of viral genomes and particles from cells and animals infected with orthopoxviruses. Virology 2017, 511, 19–22. [Google Scholar] [CrossRef]
- Liu, B.; Panda, D.; Mendez-Rios, J.D.; Ganesan, S.; Wyatt, L.S.; Moss, B. Identification of Poxvirus Genome Uncoating and DNA Replication Factors with Mutually Redundant Roles. J. Virol. 2018, 92, e02152-17. [Google Scholar] [CrossRef] [Green Version]
- Wang, N.; Zhang, Z.; Jing, H.; Zhang, M.; Wu, S.; Lin, X. Development of a novel droplet digital PCR assay for the sensitive detection of carp edema virus. Aquaculture 2021, 545, 737162. [Google Scholar] [CrossRef]
- Yang, J.; Guo, R.; Li, H.; Chen, G.; Lin, Y.; Wang, X.; Niu, C.; Dong, L. Development of highly accurate digital PCR method and reference material for monkeypox virus detection. Anal. Bioanal. Chem. 2023, 415, 1333–1337. [Google Scholar] [CrossRef]
- Colavita, F.; Mazzotta, V.; Rozera, G.; Abbate, I.; Carletti, F.; Pinnetti, C.; Matusali, G.; Meschi, S.; Mondi, A.; Lapa, D.; et al. Kinetics of viral DNA in body fluids and antibody response in patients with acute Monkeypox virus infection. Iscience 2023, 26, 106102. [Google Scholar] [CrossRef]
- Jones, G.M.; Busby, E.; Garson, J.A.; Grant, P.R.; Nastouli, E.; Devonshire, A.S.; Whale, A.S. Digital PCR dynamic range is approaching that of real-time quantitative PCR. Biomol. Detect. Quantif. 2016, 10, 31–33. [Google Scholar] [CrossRef] [Green Version]
- Dyavar, S.R.; Ye, Z.; Byrareddy, S.N.; Scarsi, K.K.; Winchester, L.C.; Weinhold, J.A.; Fletcher, C.V.; Podany, A.T. Normalization of cell associated antiretroviral drug concentrations with a novel RPP30 droplet digital PCR assay. Sci. Rep. 2018, 8, 3626. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wang, C.; Han, M.; Ye, J.; Gao, Y.; Liu, Z.; He, T.; Li, T.; Xu, M.; Zhou, L.; et al. Discrimination of False Negative Results in RT-PCR Detection of SARS-CoV-2 RNAs in Clinical Specimens by Using an Internal Reference. Virol. Sin. 2020, 35, 758–767. [Google Scholar] [CrossRef]
- Kinloch, N.N.; Ritchie, G.; Dong, W.; Cobarrubias, K.D.; Sudderuddin, H.; Lawson, T.; Matic, N.; Montaner, J.S.G.; Leung, V.; Romney, M.G.; et al. SARS-CoV-2 RNA Quantification Using Droplet Digital RT-PCR. J. Mol. Diagn. 2021, 23, 907–919. [Google Scholar] [CrossRef]
- De Kock, R.; Baselmans, M.; Scharnhorst, V.; Deiman, B. Sensitive detection and quantification of SARS-CoV-2 by multiplex droplet digital RT-PCR. Eur. J. Clin. Microbiol. Infect. Dis. Off Publ. Eur. Soc. Clin. Microbiol. 2021, 40, 807–813. [Google Scholar] [CrossRef]
- De Oliveira, M.F.; Gianella, S.; Letendre, S.; Scheffler, K.; Kosakovsky Pond, S.L.; Smith, D.M.; Strain, M.; Ellis, R.J. Comparative Analysis of Cell-Associated HIV DNA Levels in Cerebrospinal Fluid and Peripheral Blood by Droplet Digital PCR. PLoS ONE 2015, 10, e0139510. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| qPCR for Orthopoxvirus (Reference) | |||||
|---|---|---|---|---|---|
| Specimen | ddPCR for Crmb MPXV | Positive | Negative | SE [95% CI] | SP [95% CI] |
| Skin lesion | Positive | 10 | 0 | 100% [69.15–100.00] | 100% [47.82–100.00] |
| Negative | 0 | 5 | |||
| Positive | 10 | 0 | 100% [69.15–100.00] | 100% [47.82–100.00] | |
| Rectal swab | Negative | 0 | 5 | ||
| Positive | 9 | 0 | |||
| Pharyngeal swab | Negative | 1 | 5 | 90% [55.50–99.75] | 100% [47.82–100.00] |
| Positive | 6 | 0 | 60% [26.24–87.84] | 100% [47.82–100.00] | |
| Whole blood | Negative | 4 | 5 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomari, E.; Mori, A.; Accordini, S.; Donini, A.; Cordioli, M.; Tacconelli, E.; Castilletti, C. Evaluation of a ddPCR Commercial Assay for the Absolute Quantification of the Monkeypox Virus West Africa in Clinical Samples. Diagnostics 2023, 13, 1349. https://doi.org/10.3390/diagnostics13071349
Pomari E, Mori A, Accordini S, Donini A, Cordioli M, Tacconelli E, Castilletti C. Evaluation of a ddPCR Commercial Assay for the Absolute Quantification of the Monkeypox Virus West Africa in Clinical Samples. Diagnostics. 2023; 13(7):1349. https://doi.org/10.3390/diagnostics13071349
Chicago/Turabian StylePomari, Elena, Antonio Mori, Silvia Accordini, Annalisa Donini, Maddalena Cordioli, Evelina Tacconelli, and Concetta Castilletti. 2023. "Evaluation of a ddPCR Commercial Assay for the Absolute Quantification of the Monkeypox Virus West Africa in Clinical Samples" Diagnostics 13, no. 7: 1349. https://doi.org/10.3390/diagnostics13071349
APA StylePomari, E., Mori, A., Accordini, S., Donini, A., Cordioli, M., Tacconelli, E., & Castilletti, C. (2023). Evaluation of a ddPCR Commercial Assay for the Absolute Quantification of the Monkeypox Virus West Africa in Clinical Samples. Diagnostics, 13(7), 1349. https://doi.org/10.3390/diagnostics13071349