

Comparative Clinical Evaluation of a Novel FluA/FluB/SARS-CoV-2 Multiplex LAMP and Commercial FluA/FluB/SARS-CoV-2/RSV RT-qPCR Assays


Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples and RNA Extraction
2.2. Primer Design
2.3. FluA/FluB/SARS-CoV-2 Multiplex LAMP Assay
2.4. RT-PCR
2.5. Limit of Detection (LOD) Tests of the FluA/FluB/SARS-CoV-2 Multiplex LAMP Assay
2.6. Statistics
3. Results
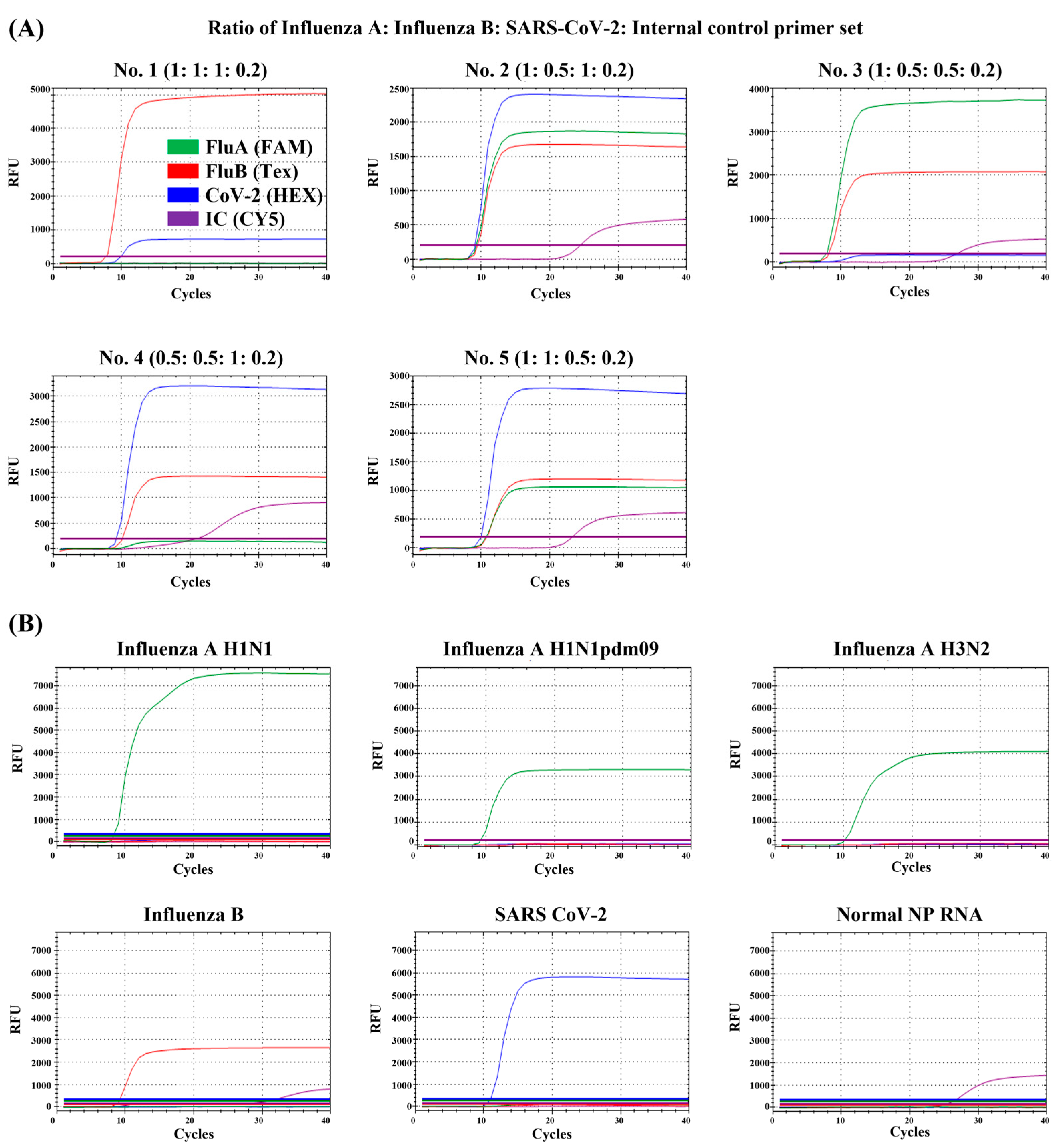
3.1. Optimization of the FluA/FluB/SARS-CoV-2 Multiplex LAMP Assay Primer Set
3.2. Detection Limit of the FluA/FluB/SARS-CoV-2 Multiplex LAMP Assay and Allplex™ SARS-CoV-2/FluA/FluB/RSV Assay
3.3. Comparison of Performance between the FluA/FluB/SARS-CoV-2 Multiplex LAMP and Allplex™ SARS-CoV-2/FluA/FluB/RSV Assays Using Clinical Samples
3.4. Cross-Reactivity Test
3.5. SARS-CoV-2 Mutant Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Javanian, M.; Barary, M.; Ghebrehewet, S.; Koppolu, V.; Vasigala, V.; Ebrahimpour, S. A brief review of influenza virus infection. J. Med. Virol. 2021, 93, 4638–4646. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Weekly Epidemiological Update, 127th ed.; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 25 January 2023).
- Lampejo, T. The impact of the COVID-19 pandemic on the global burden of influenza. J. Med. Virol. 2022, 94, 2357–2359. [Google Scholar] [CrossRef] [PubMed]
- Heiskanen, A.; Galipeau, Y.; Little, J.; Mortimer, L.; Ramotar, K.; Langlois, M.; Cooper, C.L. Seasonal respiratory virus circulation was diminished during the COVID-19 Ppandemic. Influenza Other Respir. Viruses 2023, 17, e13065. [Google Scholar] [CrossRef]
- Dhanasekaran, V.; Sullivan, S.; Edwards, K.M.; Xie, R.; Khvorov, A.; Valkenburg, S.A.; Cowling, B.J.; Barr, I.G. Human seasonal influenza under COVID-19 and the potential consequences of influenza lineage elimination. Nat. Commun. 2022, 13, 1721. [Google Scholar] [CrossRef] [PubMed]
- Mboumba Bouassa, R.-S.; Tonen-Wolyec, S.; Veyer, D.; Péré, H.; Bélec, L. Analytical performances of the AMPLIQUICK® respiratory triplex assay for simultaneous detection and differentiation of SARS-CoV-2, influenza A/B and respiratory syncytial viruses in respiratory specimens. PLoS ONE 2022, 17, e0262258. [Google Scholar] [CrossRef]
- Dinç, H.Ö.; Karabulut, N.; Alaçam, S.; Uysal, H.K.; Daşdemir, F.O.; Önel, M.; Tuyji Tok, Y.; Sirekbasan, S.; Agacfidan, A.; Gareayaghi, N.; et al. Evaluation of the diagnostic performance of a SARS-CoV-2 and influenza A/B combo rapid antigen test in respiratory samples. Diagnostics 2023, 13, 972. [Google Scholar] [CrossRef]
- Mautner, L.; Baillie, C.-K.; Herold, H.M.; Volkwein, W.; Guertler, P.; Eberle, U.; Ackermann, N.; Sing, A.; Pavlovic, M.; Goerlich, O.; et al. Rapid point-of-care detection of SARS-CoV-2 using reverse transcription loop-mediated isothermal amplification (RT-LAMP). Virol. J. 2020, 17, 160. [Google Scholar] [CrossRef] [PubMed]
- Mak, G.C.; Cheng, P.K.; Lau, S.S.; Wong, K.K.; Lau, C.; Lam, E.T.; Chan, R.C.; Tsang, D.N. Evaluation of rapid antigen test for detection of SARS-CoV-2 virus. J. Clin. Virol. 2020, 129, 104500. [Google Scholar] [CrossRef] [PubMed]
- Notomi, T. Loop-mediated isothermal amplification of DNA. Nucleic. Acids Res. 2000, 28, e63. [Google Scholar] [CrossRef]
- Nagamine, K.; Hase, T.; Notomi, T. Accelerated reaction by loop-mediated isothermal amplification using loop primers. Mol. Cell Probes 2002, 16, 223–229. [Google Scholar] [CrossRef]
- Gadkar, V.J.; Goldfarb, D.M.; Gantt, S.; Tilley, P.A.G. Real-time detection and monitoring of loop mediated amplification (LAMP) reaction using self-quenching and de-quenching fluorogenic probes. Sci. Rep. 2018, 8, 5548. [Google Scholar] [CrossRef]
- Londono-Avendano, M.A.; Libreros, G.; Osorio, L.; Parra, B. A rapid RT-LAMP assay for SARS-CoV-2 with colorimetric detection assisted by a mobile application. Diagnostics 2022, 12, 848. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, J.H.; Kim, S.; Park, J.S.; Cha, B.S.; Lee, E.S.; Han, J.; Shin, J.; Jang, Y.; Park, K.S. Loop-mediated isothermal amplification-based nucleic acid lateral flow assay for the specific and multiplex detection of genetic markers. Anal. Chim. Acta. 2022, 1205, 339781. [Google Scholar] [CrossRef] [PubMed]
- Cao, D.; Hu, L.; Lin, M.; Li, M.; Ye, Z.; Sun, H.; Huang, J.; Yang, H.; Tian, J. Real-time fluorescence loop-mediated isothermal amplification (LAMP) for rapid and reliable diagnosis of pulmonary tuberculosis. J. Microbiol. Methods 2015, 109, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Shirato, K.; Semba, S.; El-Kafrawy, S.A.; Hassan, A.M.; Tolah, A.M.; Takayama, I.; Kageyama, T.; Notomi, T.; Kamitani, W.; Matsuyama, S.; et al. Development of fluorescent reverse transcription loop-mediated isothermal amplification (RT-LAMP) using quenching probes for the detection of the Middle East Respiratory Syndrome Coronavirus. J. Virol. Methods 2018, 258, 41–48. [Google Scholar] [CrossRef]
- Kubota, R.; Alvarez, A.M.; Su, W.W.; Jenkins, D.M. Jenkins FRET-based assimilating probe for sequence-specific real-time monitoring of loop-mediated isothermal amplification (LAMP). Biol. Eng. Trans. 2011, 4, 81–100. [Google Scholar] [CrossRef]
- Kim, M.-J.; Kim, H.-Y. Direct duplex real-time loop mediated isothermal amplification assay for the simultaneous detection of cow and goat species origin of milk and yogurt products for field use. Food Chem. 2018, 246, 26–31. [Google Scholar] [CrossRef]
- Jang, W.S.; Lim, D.H.; Nam, J.; Mihn, D.-C.; Sung, H.W.; Lim, C.S.; Kim, J. Development of a multiplex isothermal amplification molecular diagnosis method for on-site diagnosis of influenza. PLoS ONE 2020, 15, e0238615. [Google Scholar] [CrossRef]
- Jang, W.S.; Lim, D.H.; Yoon, J.; Kim, A.; Lim, M.; Nam, J.; Yanagihara, R.; Ryu, S.-W.; Jung, B.K.; Ryoo, N.-H.; et al. Development of a multiplex loop-mediated isothermal amplification (LAMP) assay for on-site diagnosis of SARS CoV-2. PLoS ONE 2021, 16, e0248042. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Lau, Y.L.; Ismail, I.B.; Mustapa, N.I.B.; Lai, M.Y.; Tuan Soh, T.S.; Haji Hassan, A.; Peariasamy, K.M.; Lee, Y.L.; Abdul Kahar, M.K.B.; Chong, J.; et al. Development of a reverse transcription recombinase polymerase amplification assay for rapid and direct visual detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). PLoS ONE 2021, 16, e0245164. [Google Scholar] [CrossRef]
- Inaba, M.; Higashimoto, Y.; Toyama, Y.; Horiguchi, T.; Hibino, M.; Iwata, M.; Imaizumi, K.; Doi, Y. Diagnostic accuracy of LAMP versus PCR over the course of SARS-CoV-2 infection. Int. J. Infect. Dis. 2021, 107, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Nandi, S.; Lambe, U.; Sawant, S.; Gohil, T.; Deshpande, J. Development of a RT-LAMP assay for detection of SARS-CoV-2. Indian J. Med. Res. 2022, 155, 148. [Google Scholar] [CrossRef] [PubMed]
- Brandsma, E.; Verhagen, H.J.M.P.; van de Laar, T.J.W.; Claas, E.C.J.; Cornelissen, M.; van den Akker, E. Rapid, sensitive, and specific severe acute respiratory syndrome coronavirus 2 detection: A multicenter comparison between standard quantitative reverse-transcriptase polymerase chain reaction and CRISPR-based DETECTR. J. Infect. Dis. 2021, 223, 206–213. [Google Scholar] [CrossRef]
- Ahn, S.J.; Baek, Y.H.; Lloren, K.K.S.; Choi, W.-S.; Jeong, J.H.; Antigua, K.J.C.; Kwon, H.; Park, S.-J.; Kim, E.-H.; Kim, Y.; et al. Rapid and simple colorimetric detection of multiple influenza viruses infecting humans using a reverse transcriptional loop-mediated isothermal amplification (RT-LAMP) diagnostic platform. BMC Infect. Dis. 2019, 19, 676. [Google Scholar] [CrossRef]
- Takayama, I.; Nakauchi, M.; Takahashi, H.; Oba, K.; Semba, S.; Kaida, A.; Kubo, H.; Saito, S.; Nagata, S.; Odagiri, T.; et al. Development of real-time fluorescent reverse transcription loop-mediated isothermal amplification assay with quenching primer for influenza virus and respiratory syncytial virus. J. Virol. Methods 2019, 267, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Chen, F.; Li, Q.; Wang, L.; Fan, C. Isothermal amplification of nucleic acids. Chem. Rev. 2015, 115, 12491–12545. [Google Scholar] [CrossRef]
- Heskin, J.; Pallett, S.J.C.; Al-Hindawi, A.; Davies, G.W.; Rayment, M.; Mughal, N.; Randell, P.; Jones, R.; Moore, L.S.P. Evaluating the performance characteristics of five lateral flow assays for the detection of the SARS-CoV-2 nucleocapsid antigen. Sci. Rep. 2022, 12, 8811. [Google Scholar] [CrossRef]
- Irsara, C.; Egger, A.E.; Prokop, W.; Nairz, M.; Loacker, L.; Sahanic, S.; Pizzini, A.; Sonnweber, T.; Mayer, W.; Schennach, H.; et al. Evaluation of four commercial, fully automated SARS-CoV-2 antibody tests suggests a revision of the siemens SARS-CoV-2 IgG assay. Clin. Chem. Lab. Med. 2021, 59, 1143–1154. [Google Scholar] [CrossRef]


{kind=link}
| Target | Name | Sequence (5′-3′) | µM |
|---|---|---|---|
| Influenza A | IAV F3 | GAC TKG AAR RTG TCT TTG C | 1 |
| IAV B3 | TGT TRT TYG GGT CYC CAT T | 1 | |
| IAV FIP | TTA GTC AGA GGT GAC ARR ATT GCA GAT CTT GAG GCT CTC | 32 | |
| IAV BIP | TTG TKT TCA CGC TCA CCG TGT TTG GAC AAA GCG TCT ACG | 32 | |
| IAV BLP | CMA GTG AGC GAG GAC TG | 10 | |
| IAV FLP | GTC TTG TCT TTA GCC A | 4 | |
| IAV FLP probe 1 | [FAM]-CGG GCC CGT ACA AAG GGA ACA CCC ACA CTC CGG TCT TGT CTT TAG CCA | 6 | |
| Influenza B | IBV F3 | GAG CTG CCT ATG AAG ACC | 1 |
| IBV B3 | CGT CTC CAC CTA CTT CGT | 1 | |
| IBV FIP | GAA CAT GGA AAC CCT TGC ATT TTA AGT TTT GTC TGC ATT AAC AGG C | 32 | |
| IBV BIP | GAA CAG RTR GAA GGA ATG GGR GCG ATC TGG TCA TTG GAG CC | 32 | |
| IBV BLP | TGC TGA TCT AGG CTT GAA TTC TGT | 10 | |
| IBV FLP | AGC TCT GAT GTC CAT CAA GCT CC | 4 | |
| IBV FLP probe 1 | [TEX]-CGG GCC CGT ACA AAG GGA ACA CCC ACA CTC CGA GCT CTG ATG TCC ATC AAG CTC C | 6 | |
| SARS-CoV-2 (RdRP gene) | RdRP F3 | CCG ATA AGT ATG TCC GCA AT | 4 |
| RdRP B3 | GCT TCA GAC ATA AAA ACA TTG T | 4 | |
| RdRP FIP | ATG CGT AAA ACT CAT TCA CAA AGT CCA ACA CAG ACT TTA TGA GTG TC | 32 | |
| RdRP BIP | TGA TAC TCT CTG ACG ATG CTG TTT AAA GTT CTT TAT GCT AGC CAC | 32 | |
| RdRP LF | TGT GTC AAC ATC TCT ATT TCT ATA G | 10 | |
| RdRP LB | TCA ATA GCA CTT ATG CAT CTC AAG G | 4 | |
| RdRP LB probe 1 | [HEX]-CGG GCC CGT ACA AAG GGA ACA CCC ACA CTC CGT CAA TAG CAC TTA TGC ATC TCA AGG | 6 | |
| Human (Actin beta gene) | IC F3 | AGT ACC CCA TCG AGC ACG | 4 |
| IC B3 | AGC CTG GAT AGC AAC GTA CA | 4 | |
| IB FIP | GAG CCA CAC GCA GCT CAT TGT ATC ACC AAC TGG GAC GAC A | 32 | |
| IC BIP | CTG AAC CCC AAG GCC AAC CGG CTG GGG TGT TGA AGG TC | 32 | |
| IC LF | TGT GGT GCC AGA TTT TCT CCA | 10 | |
| IC LB | CGA GAA GAT GAC CCA GAT CAT GT | 6 | |
| IC LB Probe 2 | [CY5]-GTC AGT GCA GGC TCC CGT GTT AGG ACG AGG GTA GGC GAG AAG ATG ACC CAG ATC ATG T | 4 | |
| Quencher probe 1 | GAG TGT GGG TGT TCC CTT TGT ACG GGC CCG-BHQ1 | ||
| Quencher probe 2 | CCT ACC CTC GTC CTA ACA CGG GAG CCT GCA CTG AC-BHQ2 |
| No | Ratio of Primer Set Mixture (FluA:FluB:SARS-CoV-2:IC) | FluA/FluB/SARS-CoV-2 Multiplex LAMP Assay Cycle Threshold Values (Ct Values) | ||||
|---|---|---|---|---|---|---|
| Channels | FAM | Texas Red | HEX | Cy5 | ||
| Targets | Flu A H1N1 | Flu B | SARS-CoV-2 | IC-ACTB | ||
| 1 | 1:1:1:0.2 | N/A | 7.69 | 9.90 | N/A | |
| 2 | 1:0.5:1:0.2 | 9.27 | 9.44 | 9.08 | 24.46 | |
| 3 | 1:0.5:0.5:0.2 | 7.92 | 8.21 | N/A | 27.03 | |
| 4 | 0.5:0.5:1:0.2 | N/A | 10.12 | 9.23 | 23.93 | |
| 5 | 1:1:0.5:0.2 | 10.76 | 10.92 | 10.01 | 23.39 | |
| Sample | Concentration | FluA/FluB/SARS-CoV-2 Multiplex LAMP Assay Cycle Threshold Values (Ct Values) | |||
|---|---|---|---|---|---|
| FluA | FluB | RdRP | IC-ACTB | ||
| Influenza A H1N1 | 2 × 105 TCID50/mL | 8.28 | N/A | N/A | N/A |
| Influenza A H1N1pdm09 | 7 × 1012 TCID50/mL | 9.22 | N/A | N/A | N/A |
| Influenza A H3N2 | 2 × 105 TCID50/mL | 10.17 | N/A | N/A | N/A |
| Influenza B | 7 × 105 TCID50/mL | N/A | 8.52 | N/A | 27.27 |
| SARS-CoV-2 | 1 × 102 PFU/mL | N/A | N/A | 11.03 | N/A |
| NP RNA sample | N/A | N/A | N/A | 25.47 | |
| Virus | TCID50/mL | Allplex™ SARS-CoV-2/Flua/Flub/RSV Assay | FluA/FluB/SARS-CoV-2 Multiplex LAMP Assay | ||||||
|---|---|---|---|---|---|---|---|---|---|
| FluA | FluB | CoV-2 | IC | FluA | FluB | CoV-2 | IC | ||
| Cycle Threshold Values (Ct Values) | Cycle Threshold Values (Ct Values) | ||||||||
| Influenza A H1N1 | 2 × 106 | 18.83 ± 0.17 | N/A | N/A | 26.65 ± 0.24 | 8.55 ± 0.19 | N/A | N/A | N/A |
| 2 × 105 | 21.05 ± 0.08 | N/A | N/A | 30.99 ± 0.30 | 10.42 ± 0.19 | N/A | N/A | N/A | |
| 2 × 104 | 24.01 ± 0.19 | N/A | N/A | 34.84 ± 0.04 | 13.15 ± 0.86 | N/A | N/A | N/A | |
| 2 × 103 | 30.85 ± 0.51 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 2 × 102 | 37.32 ± 0.64 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 2 × 101 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 2 × 100 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| Influenza A H1N1pdm09 | 7 × 1012 | 18.05 ± 0.07 | N/A | N/A | 26.28 ± 0.07 | 8.95 ± 0.40 | N/A | N/A | N/A |
| 7 × 1011 | 22.03 ± 0.30 | N/A | N/A | 29.94 ± 1.10 | 10.10 ± 0.61 | N/A | N/A | N/A | |
| 7 × 1010 | 25.81 ± 0.33 | N/A | N/A | 34.89 ± 1.34 | 13.4 ± 2.0 | N/A | N/A | N/A | |
| 7 × 109 | 30.75 ± 0.51 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 7 × 108 | 36.29 ± 0.55 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 7 × 107 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 7 × 106 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| Influenza A H3N2 | 2 × 106 | 18.11 ± 0.02 | N/A | N/A | 27.37 ± 0.29 | 9.29 ± 0.10 | N/A | N/A | N/A |
| 2 × 105 | 22.52 ± 0.10 | N/A | N/A | 32.31 ± 0.74 | 10.28 ± 0.67 | N/A | N/A | N/A | |
| 2 × 104 | 26.93 ± 0.33 | N/A | N/A | 35.46 ± 0.65 | 11.92 ± 0.70 | N/A | N/A | N/A | |
| 2 × 103 | 31.62 ± 0.48 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 2 × 102 | 35.19 ± 0.65 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 2 × 101 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 2 × 100 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| Influenza B | 7 × 106 | N/A | 17.24 ± 0.14 | N/A | 27.21 ± 0.40 | N/A | 7.21 ± 0.08 | N/A | 21.90 ± 1.94 |
| 7 × 105 | N/A | 19.36 ± 0.45 | N/A | 31.23 ± 1.08 | N/A | 8.12 ± 0.08 | N/A | 26.13 ± 0.30 | |
| 7 × 104 | N/A | 23.28 ± 0.65 | N/A | 34.93 ± 0.87 | N/A | 9.48 ± 0.12 | N/A | 28.69 ± 0.46 | |
| 7 × 103 | N/A | 27.11 ± 1.18 | N/A | N/A | N/A | 10.81 ± 0.18 | N/A | 35.37 ± 1.03 | |
| 7 × 102 | N/A | 32.49 ± 0.70 | N/A | N/A | N/A | 13.27 ± 1.38 | N/A | N/A | |
| 7 × 101 | N/A | 36.16 ± 1.08 | N/A | N/A | N/A | N/A | N/A | N/A | |
| 7 × 100 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| SARS-CoV-2 (NCCP43346) | PFU/mL | ||||||||
| 1 × 100 | N/A | N/A | 27.10 ± 0.08 | 30.86 ± 0.06 | N/A | N/A | 10.13 ± 0.11 | N/A | |
| 1 × 10−1 | N/A | N/A | 33.73 ± 0.67 | 34.62 ± 0.25 | N/A | N/A | 11.03 ± 0.04 | N/A | |
| 1 × 10−2 | N/A | N/A | 37.07 ± 1.03 | N/A | N/A | N/A | N/A | N/A | |
| 1 × 10−3 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 1 × 10−4 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 1 × 10−5 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 1 × 10−6 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| Clinical Samples | Assay | P/N | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|---|
| Influenza A (n = 117) | Allplex™ SARS-CoV-2/FluA/FluB/RSV assay | 111/6 | 94.87 (88.71–97.90) | 99.03 (93.93–99.95) | 99.10 (94.40–99.95) | 94.44 (87.81–97.72) |
| FluA/FluB/SARS-CoV-2 multiplex LAMP assay | 106/11 | 90.60 (83.43–94-98) | 100 (95.48–100) | 100 (95.64–100) | 90.27 (82.88–94.80) | |
| Influenza B (n = 61) | Allplex™ SARS-CoV-2/FluA/FluB/RSV assay | 54/7 | 88.52 (77.17–94.88) | 99.03 (93.93–99.95) | 98.18 (89.01–99.91) | 93.58 (86.76–97.16) |
| FluA/FluB/SARS-CoV-2 multiplex LAMP assay | 53/8 | 86.89 (75.23–93.77) | 100 (95.48–100) | 100 (91.58–100) | 92.72 (85.74–96.58) | |
| SARS-CoV-2 (n = 96) | Allplex™ SARS-CoV-2/FluA/FluB/RSV assay | 94/2 | 97.92 (91.96–99.94) | 100 (95.48–100) | 100 (95.12–100) | 98.08 (92.55–99.97) |
| FluA/FluB/SARS-CoV-2 multiplex LAMP assay | 95/1 | 98.96 (93.51–99.94) | 100 (95.48–100) | 100 (95.16–100) | 99.03 (93.93–99.95) |
| Allplex™ SARS-CoV-2/FluA/FluB/RSV Assay | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Influenza A | Influenza B | SARS-CoV-2 | ||||||||
| P | N | Total | P | N | Total | P | N | Total | ||
| FluA/FluB/SARS-CoV-2 multiplex LAMP assay | P | 100 | 6 | 106 | 46 | 7 | 53 | 93 | 2 | 95 |
| N | 11 | 102 | 113 | 8 | 102 | 110 | 1 | 102 | 103 | |
| Total | 111 | 108 | 219 | 54 | 109 | 163 | 94 | 104 | 198 | |
| Cohen’s kappa index (p-value) | 0.845 (<0.001) | 0.791 (<0.001) | 0.970 (<0.001) | |||||||
| Strength of agreement | Almost perfect | Substantial | Almost perfect | |||||||
| Tested Clinical Samples | FluA/FluB/SARS-CoV-2 Multiplex LAMP Assay (Positive No./Test No.) | |||
|---|---|---|---|---|
| Flu A | Flu B | SARS-CoV-2 | IC-ACTB | |
| CoV 229E | 0/3 | 0/3 | 0/3 | 3/0 |
| CoV NL63 | 0/3 | 0/3 | 0/3 | 3/0 |
| CoV OC43 | 0/3 | 0/3 | 0/3 | 3/0 |
| HEV | 0/3 | 0/3 | 0/3 | 3/0 |
| AdV | 0/3 | 0/3 | 0/3 | 3/0 |
| PIV | 0/3 | 0/3 | 0/3 | 3/0 |
| MPV | 0/3 | 0/3 | 0/3 | 3/0 |
| HboV | 0/3 | 0/3 | 0/3 | 3/0 |
| HRV | 0/3 | 0/3 | 0/3 | 3/0 |
| RSV A | 0/3 | 0/3 | 0/3 | 3/0 |
| RSV B | 0/3 | 0/3 | 0/3 | 0/3 |
| Virus | Genotype (GSAID *) | Lineage | NCCP No. | FluA/FluB/SARS-CoV-2 Multiplex LAMP Assay | |||
|---|---|---|---|---|---|---|---|
| Flu A | Flu B | RdRP | IC-ACTB | ||||
| Cycle Threshold Values (Ct Values) | |||||||
| SARS-CoV-2 | GV (wild-type) | B.1.177 | 43346 | N/A | N/A | 7.12 | N/A |
| GRY | B.1.1.7 | 43381 | N/A | N/A | 7.29 | N/A | |
| GH | B.1.351 | 43382 | N/A | N/A | 8.01 | N/A | |
| GR | P.2 | 43383 | N/A | N/A | 7.03 | N/A | |
| GH | B.1.427 | 43384 | N/A | N/A | 8.07 | N/A | |
| GH | B.1.429 | 43385 | N/A | N/A | 8.35 | N/A | |
| G | B.1.525 | 43386 | N/A | N/A | 12.78 | N/A | |
| GH | B.1.526 | 43387 | N/A | N/A | 10.89 | N/A | |
| GR | P.1 | 43388 | N/A | N/A | 7.12 | N/A | |
| G | B.1.617.1 | 43389 | N/A | N/A | 8.06 | N/A | |
| G | B.1.620 | 43404 | N/A | N/A | 7.33 | N/A | |
| GK | B.1.617.2 | 43405 | N/A | N/A | 8.63 | N/A | |
| GH | B.1.621 | 43407 | N/A | N/A | 8.35 | N/A | |
| GRA | BA.1 | 43408 | N/A | N/A | 7.15 | N/A | |
| GRA | BA.1.1 | 43411 | N/A | N/A | 8.20 | N/A | |
| GRA | BA.2 | 43412 | N/A | N/A | 9.08 | N/A | |
| GRA | BA.2.12.1 | 43423 | N/A | N/A | 8.19 | N/A | |
| GRA | BA.2.3 | 43424 | N/A | N/A | 10.82 | N/A | |
| GRA | BA.4 | 43425 | N/A | N/A | 9.75 | N/A | |
| GRA | BA.5 | 43426 | N/A | N/A | 10.80 | N/A | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jee, H.; Park, S.; Lee, J.; Lim, C.S.; Jang, W.S. Comparative Clinical Evaluation of a Novel FluA/FluB/SARS-CoV-2 Multiplex LAMP and Commercial FluA/FluB/SARS-CoV-2/RSV RT-qPCR Assays. Diagnostics 2023, 13, 1432. https://doi.org/10.3390/diagnostics13081432
Jee H, Park S, Lee J, Lim CS, Jang WS. Comparative Clinical Evaluation of a Novel FluA/FluB/SARS-CoV-2 Multiplex LAMP and Commercial FluA/FluB/SARS-CoV-2/RSV RT-qPCR Assays. Diagnostics. 2023; 13(8):1432. https://doi.org/10.3390/diagnostics13081432
Chicago/Turabian StyleJee, Hyunseul, Seoyeon Park, Junmin Lee, Chae Seung Lim, and Woong Sik Jang. 2023. "Comparative Clinical Evaluation of a Novel FluA/FluB/SARS-CoV-2 Multiplex LAMP and Commercial FluA/FluB/SARS-CoV-2/RSV RT-qPCR Assays" Diagnostics 13, no. 8: 1432. https://doi.org/10.3390/diagnostics13081432
APA StyleJee, H., Park, S., Lee, J., Lim, C. S., & Jang, W. S. (2023). Comparative Clinical Evaluation of a Novel FluA/FluB/SARS-CoV-2 Multiplex LAMP and Commercial FluA/FluB/SARS-CoV-2/RSV RT-qPCR Assays. Diagnostics, 13(8), 1432. https://doi.org/10.3390/diagnostics13081432