

Endometrial Staining of CD56 (Uterine Natural Killer), BCL-6, and CD138 (Plasma Cells) Improve Diagnosis and Clinical Pregnancy Outcomes in Unexplained Infertility and Recurrent IVF Failures: Standardization of Diagnosis with Digital Pathology

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Ethics Approval
2.2. Endometrial Sampling and Immunostaining
2.3. Evaluation by Conventional Light Microscopy (LM)
2.4. Digital Pathology (DP)
2.5. Statistical Analysis
3. Results
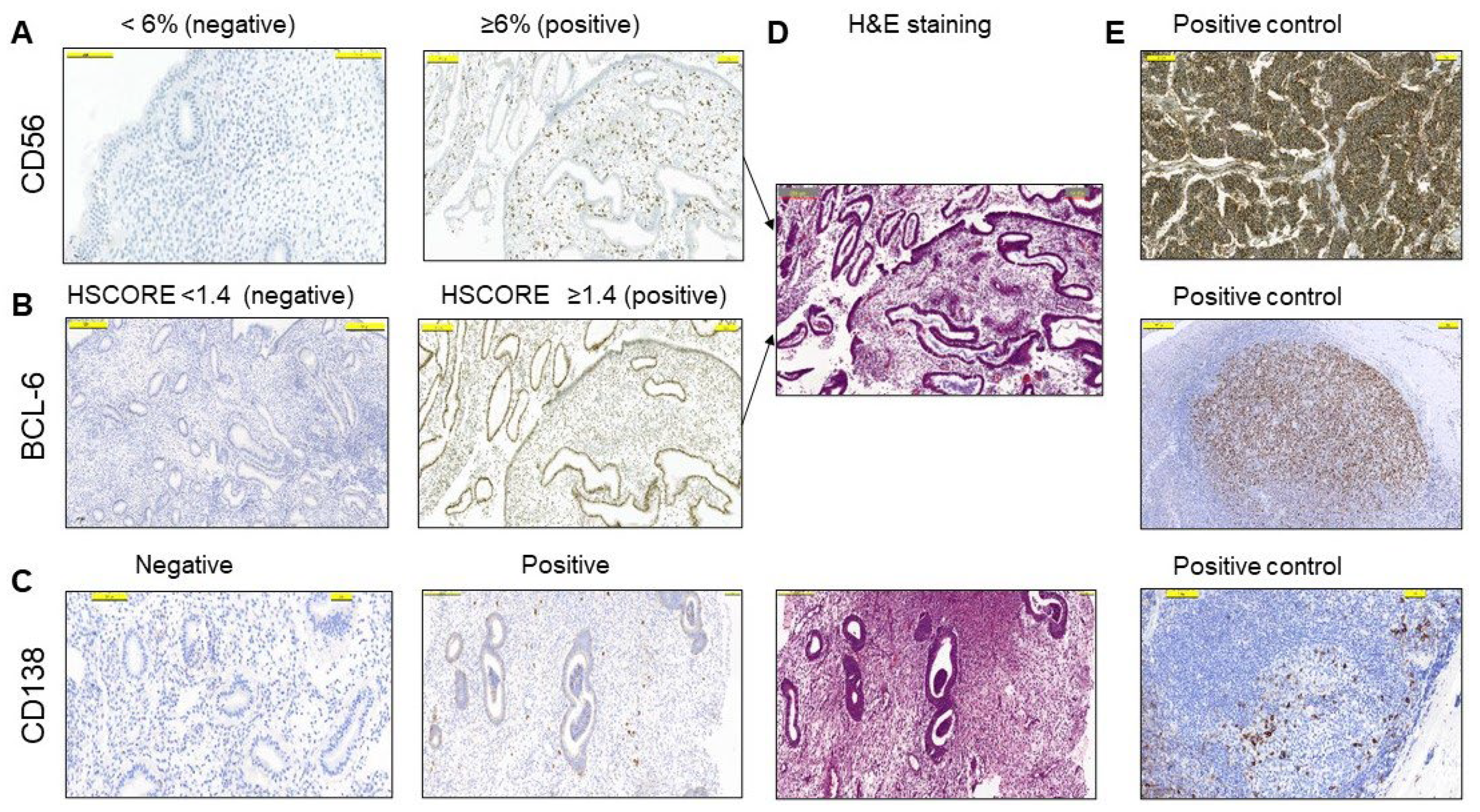
3.1. Immunopathology Detection of the Endometrium by Conventional Light Microscopy
3.2. Targeted Treatment Based on Immune Marker Detection Increased Pregnancy Rates
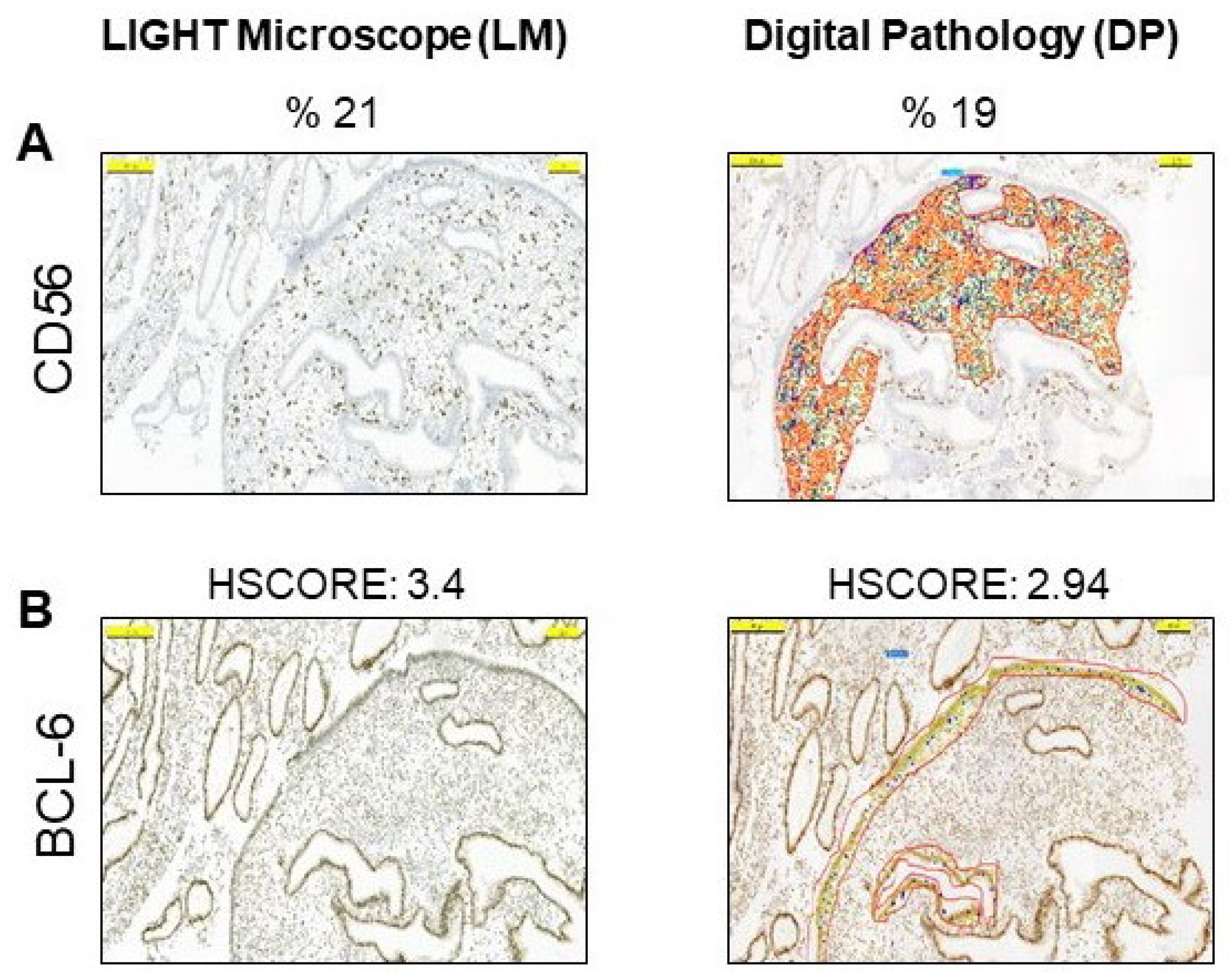
3.3. Digital Pathology Analysis of CD56 and BCL-6 Immunostaining of the Endometrium
4. Discussion
5. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BCL-6 | B-cell lymphoma 6 protein |
| CD138 | Plasma cell marker, also known as Syndecan-1 |
| DP | Digital pathology |
| IVF | In vitro fertilization |
| LM | Light microscopy |
| UI | Unexplained infertility |
| uNK | Uterine natural killer |
References
- Quaas, A.; Dokras, A. Diagnosis and treatment of unexplained infertility. Rev. Obstet. Gynecol. 2008, 1, 69–76. [Google Scholar] [PubMed]
- Russell, P.; Sacks, G.; Tremellen, K.; Gee, A. The distribution of immune cells and macrophages in the endometrium of women with recurrent reproductive failure. III: Further observations and reference ranges. Pathology 2013, 45, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Mettler, L.; Shukla, D.; Schollmeyer, T. Accuracy of laparoscopic diagnosis of endometriosis. JSLS J. Soc. Laparoendosc. Surg. Soc. Laparoendosc. Surg. 2003, 7, S11. [Google Scholar] [CrossRef]
- Máté, G.; Bernstein, L.R.; Török, A.L. Endometriosis Is a Cause of Infertility. Does Reactive Oxygen Damage to Gametes and Embryos Play a Key Role in the Pathogenesis of Infertility Caused by Endometriosis? Front. Endocrinol. 2018, 9, 725. [Google Scholar] [CrossRef] [PubMed]
- Evans-Hoeker, E.; Lessey, B.A.; Jeong, J.W.; Savaris, R.F.; Palomino, W.A.; Yuan, L.; Schammel, D.P.; Young, S.L. Endometrial BCL6 Overexpression in Eutopic Endometrium of Women with Endometriosis. Reprod. Sci. 2016, 23, 1234–1241. [Google Scholar] [CrossRef] [PubMed]
- Tuckerman, E.; Mariee, N.; Prakash, A.; Li, T.C.; Laird, S. Uterine natural killer cells in peri-implantation endometrium from women with repeated implantation failure after IVF. J. Reprod. Immunol. 2010, 87, 60–66. [Google Scholar] [CrossRef]
- Agostinis, C.; Mangogna, A.; Bossi, F.; Ricci, G.; Kishore, U.; Bulla, R. Uterine immunity and microbiota: A shifting paradigm. Front. Immunol. 2019, 10, 2387. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, E.; Parkin, K.L.; Lessey, B.A.; Young, S.L.; Fazleabas, A.T. Characterization of uterine NK cells in women with infertility or recurrent pregnancy loss and associated endometriosis. Am. J. Reprod. Immunol. 2014, 72, 262–269. [Google Scholar] [CrossRef]
- Faas, M.M.; de Vos, P. Uterine NK cells and macrophages in pregnancy. Placenta 2017, 56, 44–52. [Google Scholar] [CrossRef]
- Chen, X.; Mariee, N.; Jiang, L.; Liu, Y.; Wang, C.C.; Li, T.C.; Laird, S. Measurement of uterine natural killer cell percentage in the periimplantation endometrium from fertile women and women with recurrent reproductive failure: Establishment of a reference range. Am. J. Obstet. Gynecol. 2017, 217, 680.e1–680.e6. [Google Scholar] [CrossRef]
- Glover, L.E.; Crosby, D.; Thiruchelvam, U.; Harmon, C.; Ni Chorcora, C.; Wingfield, M.B.; O’Farrelly, C. Uterine natural killer cell progenitor populations predict successful implantation in women with endometriosis-associated infertility. Am. J. Reprod. Immunol. 2018, 79, e12817. [Google Scholar] [CrossRef] [PubMed]
- Kolanska, K.; Bendifallah, S.; Cohen, J.; Placais, L.; Selleret, L.; Johanet, C.; Suner, L.; Delhommeau, F.; Chabbert-Buffet, N.; Darai, E.; et al. Unexplained recurrent implantation failures: Predictive factors of pregnancy and therapeutic management from a French multicentre study. J. Reprod. Immunol. 2021, 145, 103313. [Google Scholar] [CrossRef]
- Xu, H. Expressions of natural cytotoxicity receptor, NKG2D and NKG2D ligands in endometriosis. J. Reprod. Immunol. 2019, 136, 102615. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.-G.; Chen, J.-J.; Zhou, H.-L.; Wu, Y.; Lin, F.; Shi, J.; Wu, H.-Z.; Xiao, H.-Q.; Wang, W. Identification and Validation of the Signatures of Infiltrating Immune Cells in the Eutopic Endometrium Endometria of Women With Endometriosis. Front. Immunol. 2021, 12, 671201. [Google Scholar] [CrossRef]
- Fukui, A.; Mai, C.; Saeki, S.; Yamamoto, M.; Takeyama, R.; Kato, T.; Ukita, Y.; Wakimoto, Y.; Yamaya, A.; Shibahara, H. Pelvic endometriosis and natural killer cell immunity. Am. J. Reprod. Immunol. 2020, 85, e13342. [Google Scholar] [CrossRef] [PubMed]
- Fukui, A.; Kamoi, M.; Funamizu, A.; Fuchinoue, K.; Chiba, H.; Yokota, M.; Fukuhara, R.; Mizunuma, H. NK cell abnormality and its treatment in women with reproductive failures such as recurrent pregnancy loss, implantation failures, preeclampsia, and pelvic endometriosis. Reprod. Med. Biol. 2015, 14, 151–157. [Google Scholar] [CrossRef]
- Lash, G.E.; Bulmer, J.N.; Li, T.C.; Innes, B.A.; Mariee, N.; Patel, G.; Sanderson, J.; Quenby, S.; Laird, S.M. Standardisation of uterine natural killer (uNK) cell measurements in the endometrium of women with recurrent reproductive failure. J. Reprod. Immunol. 2016, 116, 50–59. [Google Scholar] [CrossRef]
- Freitag, N.; Pour, S.J.; Fehm, T.N.; Toth, B.; Markert, U.R.; Weber, M.; Togawa, R.; Kruessel, J.-S.; Baston-Buest, D.M.; Bielfeld, A.P. Are uterine natural killer and plasma cells in infertility patients associated with endometriosis, repeated implantation failure, or recurrent pregnancy loss? Arch. Gynecol. Obstet. 2020, 302, 1487–1494. [Google Scholar] [CrossRef]
- Bulun, S.E.; Yilmaz, B.D.; Sison, C.; Miyazaki, K.; Bernardi, L.; Liu, S.; Kohlmeier, A.; Yin, P.; Milad, M.; Wei, J. Endometriosis. Endocr. Rev. 2019, 40, 1048–1079. [Google Scholar] [CrossRef]
- Likes, C.E.; Cooper, L.J.; Efird, J.; Forstein, D.A.; Miller, P.B.; Savaris, R.; Lessey, B.A. Medical or surgical treatment before embryo transfer improves outcomes in women with abnormal endometrial BCL6 expression. J. Assist. Reprod. Genet. 2019, 36, 483–490. [Google Scholar] [CrossRef]
- Gong, Q.; Zhu, Y.; Pang, N.; Ai, H.; Gong, X.; La, X.; Ding, J. Increased levels of CCR7(lo)PD-1(hi) CXCR5+ CD4+ T cells, and associated factors Bcl-6, CXCR5, IL-21 and IL-6 contribute to repeated implantation failure. Exp. Ther. Med. 2017, 14, 5931–5941. [Google Scholar] [CrossRef] [PubMed]
- Almquist, L.D.; Likes, C.E.; Stone, B.; Brown, K.R.; Savaris, R.; Forstein, D.A.; Miller, P.B.; Lessey, B.A. Endometrial BCL6 testing for the prediction of in vitro fertilization outcomes: A cohort study. Fertil. Steril. 2017, 108, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, S.; Young, S. Diagnostic and therapeutic options in recurrent implantation failure. F1000Res 2020, 9, 208. [Google Scholar] [CrossRef]
- Shaffer, A.L.; Yu, X.; He, Y.; Boldrick, J.; Chan, E.P.; Staudt, L.M. BCL-6 represses genes that function in lymphocyte differentiation, inflammation, and cell cycle control. Immunity 2000, 13, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Inoue, T.; Ise, W.; Matsuo-Dapaah, J.; Wing, J.B.; Temizoz, B.; Kobiyama, K.; Hayashi, T.; Patil, A.; Sakaguchi, S.; et al. B cell-intrinsic TBK1 is essential for germinal center formation during infection and vaccination in mice. J. Exp. Med. 2021, 219, e20211336. [Google Scholar] [CrossRef]
- Choi, J.; Crotty, S. Bcl6-Mediated Transcriptional Regulation of Follicular Helper T cells (TFH). Trends Immunol. 2021, 42, 336–349. [Google Scholar] [CrossRef]
- Chen, J.L.; Yang, J.M.; Huang, Y.Z.; Li, Y. Clinical observation of lymphocyte active immunotherapy in 380 patients with unexplained recurrent spontaneous abortion. Int. Immunopharmacol. 2016, 40, 347–350. [Google Scholar] [CrossRef]
- McQueen, D.B.; Perfetto, C.O.; Hazard, F.K.; Lathi, R.B. Pregnancy outcomes in women with chronic endometritis and recurrent pregnancy loss. Int. Immunopharmacol. 2016, 40, 347–350. [Google Scholar] [CrossRef]
- Drury, J.A.; Tang, A.W.; Turner, M.A.; Quenby, S. A rapid, reliable method for uNK cell density estimation. J. Reprod. Immunol. 2013, 97, 183–185. [Google Scholar] [CrossRef]
- Hallager, T.; Saxtorph, M.H.; Eriksen, J.O.; Hviid, T.V.; Macklon, N.S.; Larsen, L.G. Conventional microscopy versus digital image analysis for histopathologic evaluation of immune cells in the endometrium. J. Reprod. Immunol. 2021, 145, 103294. [Google Scholar] [CrossRef]
- Ekemen, S.; Yapicier, O.; Boler, H.D.; Ince, U. An extremely rare case of back and hip pain due to the metastasis of late recurrent myxopapillary ependymoma to the inguinal lymph node. J. Pathol. Transl. Med. 2018, 52, 67–70. [Google Scholar] [CrossRef]
- Herlihy, N.S.; Klimczak, A.M.; Titus, S.; Scott, C.; Hanson, B.M.; Kim, J.K.; Seli, E.; Scott, R.T. The role of endometrial staining for CD138 as a marker of chronic endometritis in predicting live birth. J. Assist. Reprod. Genet. 2022, 39, 473–479. [Google Scholar] [CrossRef]
- Meyerholz, D.K.; Beck, A.P. Principles and approaches for reproducible scoring of tissue stains in research. Lab. Investig. 2018, 98, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Canberk, S.; Behzatoglu, K.; Caliskan, C.K.; Gelmez, S.; Kayhan, K.C.; Aydemir, S.F.; Akbas, M.; Yıldız, I.; Veiga, R.; Alrefae, N.; et al. The Role of Telecytology in the Primary Diagnosis of Thyroid Fine-Needle Aspiration Specimens. Acta Cytol. 2019, 64, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Coulam, C.B. Intralipid treatment for women with reproductive failures. Am. J. Reprod. Immunol. 2020, 85, e13290. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chen, X.; Huang, J.; Wang, C.-C.; Yu, M.-Y.; Laird, S.; Li, T.-C. Comparison of the prevalence of chronic endometritis as determined by means of different diagnostic methods in women with and without reproductive failure. Fertil. Steril. 2018, 109, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Seshadri, S.; Sunkara, S.K. Natural killer cells in female infertility and recurrent miscarriage: A systematic review and meta-analysis. Hum. Reprod. Updat. 2013, 20, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Quenby, S.; Kalumbi, C.; Bates, M.; Farquharson, R.; Vince, G. Prednisolone reduces preconceptual endometrial natural killer cells in women with recurrent miscarriage. Fertil. Steril. 2005, 84, 980–984. [Google Scholar] [CrossRef]
- Niazi, M.K.K.; Parwani, A.V.; Gurcan, M.N. Digital pathology and artificial intelligence. Lancet Oncol. 2019, 20, e253–e261. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Number (n = 76) | Percentage (%) |
|---|---|---|
| Age groups | ||
| <25 | 1 | 1.3 |
| 25–29 | 17 | 22.4 |
| 30–34 | 25 | 32.9 |
| 35–39 | 25 | 32.9 |
| ≥40 | 8 | 10.5 |
| Number of IVF failures | ||
| 1–2 | 32 | 40.8 |
| 3–4 | 32 | 40.8 |
| 5–6 | 10 | 15.8 |
| 7–8 | 2 | 2.6 |
| Immune Markers | Definition | Positivity Rate n = 76 (%) | Clinical Pregnancy Outcome n = 65 (%) |
|---|---|---|---|
| CD56 Levels | ≥6% | 44 (57.9) | 38 (58.5%) |
| BCL-6 Levels | HSCORE ≥ 1.4 | 35 (46.1) | 30 (46.2%) |
| CD56 or BCL-6 | CD56 ≥ 6% or BCL-6 HSCORE ≥ 1.4 | 46 (60.5) | 40 (61.5%) |
| CD56 or CD138 | CD56 ≥ 6% or CD138 ≥ 1 | 52 (68.4) | 46 (70.8%) |
| CD56, BCL-6, or CD138 | CD56 ≥ 6%, BCL-6 HSCORE ≥ 1.4, or CD138 ≥ 1 | 54 (71.05) | 48 (73.8%) |
| Correlation Coefficient (r) | p * | |
|---|---|---|
| CD56 (LM) vs. CD56 (DP) | 0.906 | <0.001 |
| BCL-6 (LM) vs. BCL-6 (DP) | 0.943 | <0.001 |
| CD56 (LM) vs. BCL-6 (LM) | 0.576 | <0.001 |
| CD56 (DP) vs. BCL-6 (DP) | 0.592 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekemen, S.; Comunoglu, C.; Kayhan, C.K.; Bilir, E.; Cavusoglu, I.; Etiler, N.; Bilgi, S.; Ince, U.; Coban, C.; Erden, H.F. Endometrial Staining of CD56 (Uterine Natural Killer), BCL-6, and CD138 (Plasma Cells) Improve Diagnosis and Clinical Pregnancy Outcomes in Unexplained Infertility and Recurrent IVF Failures: Standardization of Diagnosis with Digital Pathology. Diagnostics 2023, 13, 1557. https://doi.org/10.3390/diagnostics13091557
Ekemen S, Comunoglu C, Kayhan CK, Bilir E, Cavusoglu I, Etiler N, Bilgi S, Ince U, Coban C, Erden HF. Endometrial Staining of CD56 (Uterine Natural Killer), BCL-6, and CD138 (Plasma Cells) Improve Diagnosis and Clinical Pregnancy Outcomes in Unexplained Infertility and Recurrent IVF Failures: Standardization of Diagnosis with Digital Pathology. Diagnostics. 2023; 13(9):1557. https://doi.org/10.3390/diagnostics13091557
Chicago/Turabian StyleEkemen, Suheyla, Cem Comunoglu, Cavit Kerem Kayhan, Ebru Bilir, Ilkay Cavusoglu, Nilay Etiler, Selcuk Bilgi, Umit Ince, Cevayir Coban, and Halit Firat Erden. 2023. "Endometrial Staining of CD56 (Uterine Natural Killer), BCL-6, and CD138 (Plasma Cells) Improve Diagnosis and Clinical Pregnancy Outcomes in Unexplained Infertility and Recurrent IVF Failures: Standardization of Diagnosis with Digital Pathology" Diagnostics 13, no. 9: 1557. https://doi.org/10.3390/diagnostics13091557
APA StyleEkemen, S., Comunoglu, C., Kayhan, C. K., Bilir, E., Cavusoglu, I., Etiler, N., Bilgi, S., Ince, U., Coban, C., & Erden, H. F. (2023). Endometrial Staining of CD56 (Uterine Natural Killer), BCL-6, and CD138 (Plasma Cells) Improve Diagnosis and Clinical Pregnancy Outcomes in Unexplained Infertility and Recurrent IVF Failures: Standardization of Diagnosis with Digital Pathology. Diagnostics, 13(9), 1557. https://doi.org/10.3390/diagnostics13091557