
Liver Magnetic Resonance Elastography: Focus on Methodology, Technique, and Feasibility

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
1.1. The Importance of Identifying Liver Cirrhosis
1.2. Clinical Indications
1.3. Imaging Methods to Identify Liver Fibrosis and Cirrhosis
1.4. Diagnostic Accuracy of MRE to Identify Liver Fibrosis
1.5. Limitations and Contraindications of MRE
1.6. Other Utilities and Future Applications of MRE
2. Technical Aspects
Basic Principles of MRE
3. How We Do It
3.1. Patient Preparation
3.2. Technical Details of MR Scan
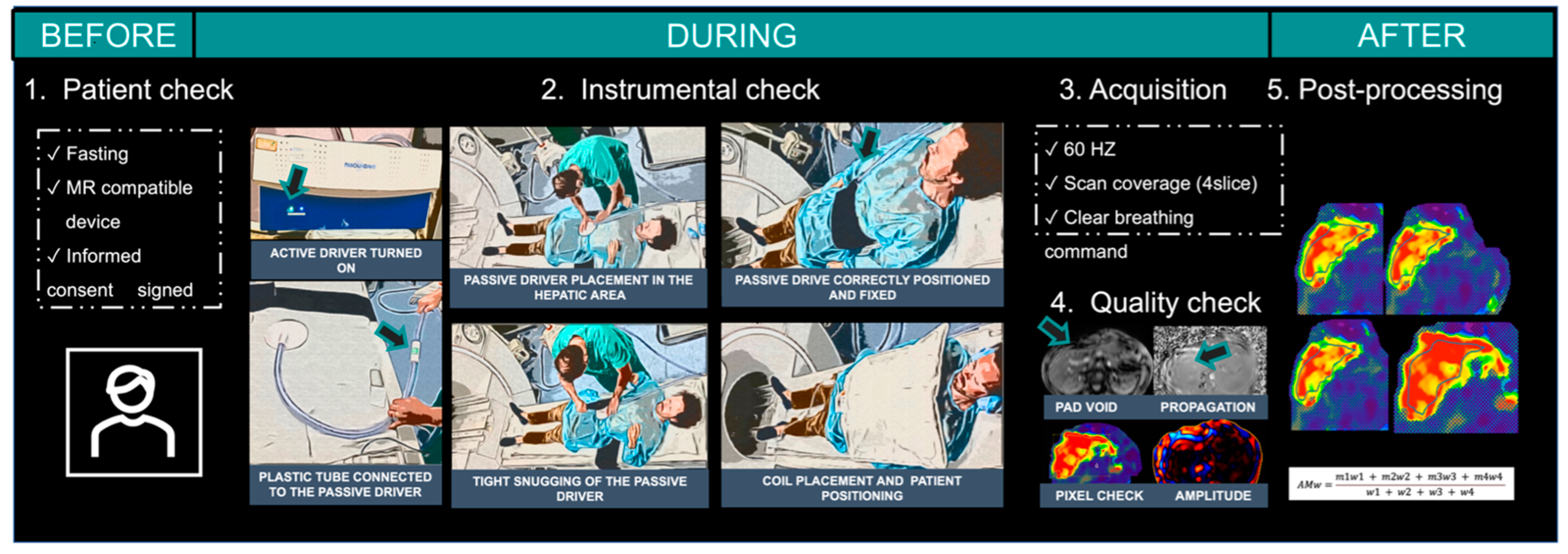
4. Performing MRE Step-by-Step
4.1. Passive Driver Positioning
4.2. Abdominal Coil
4.3. Slices’ Positioning
4.4. Acquiring the Images
4.5. Passive Driver Vibration and Amplitude
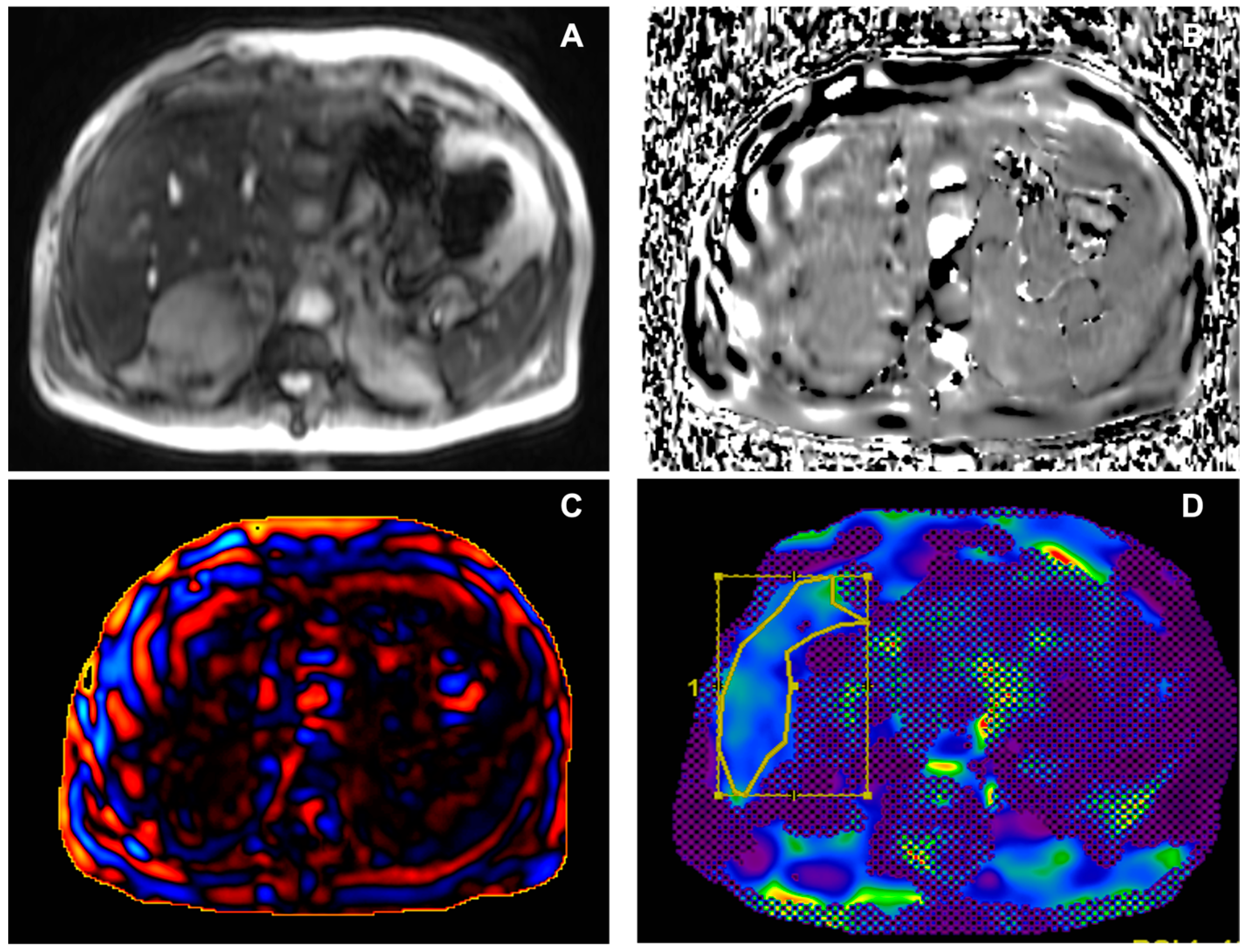
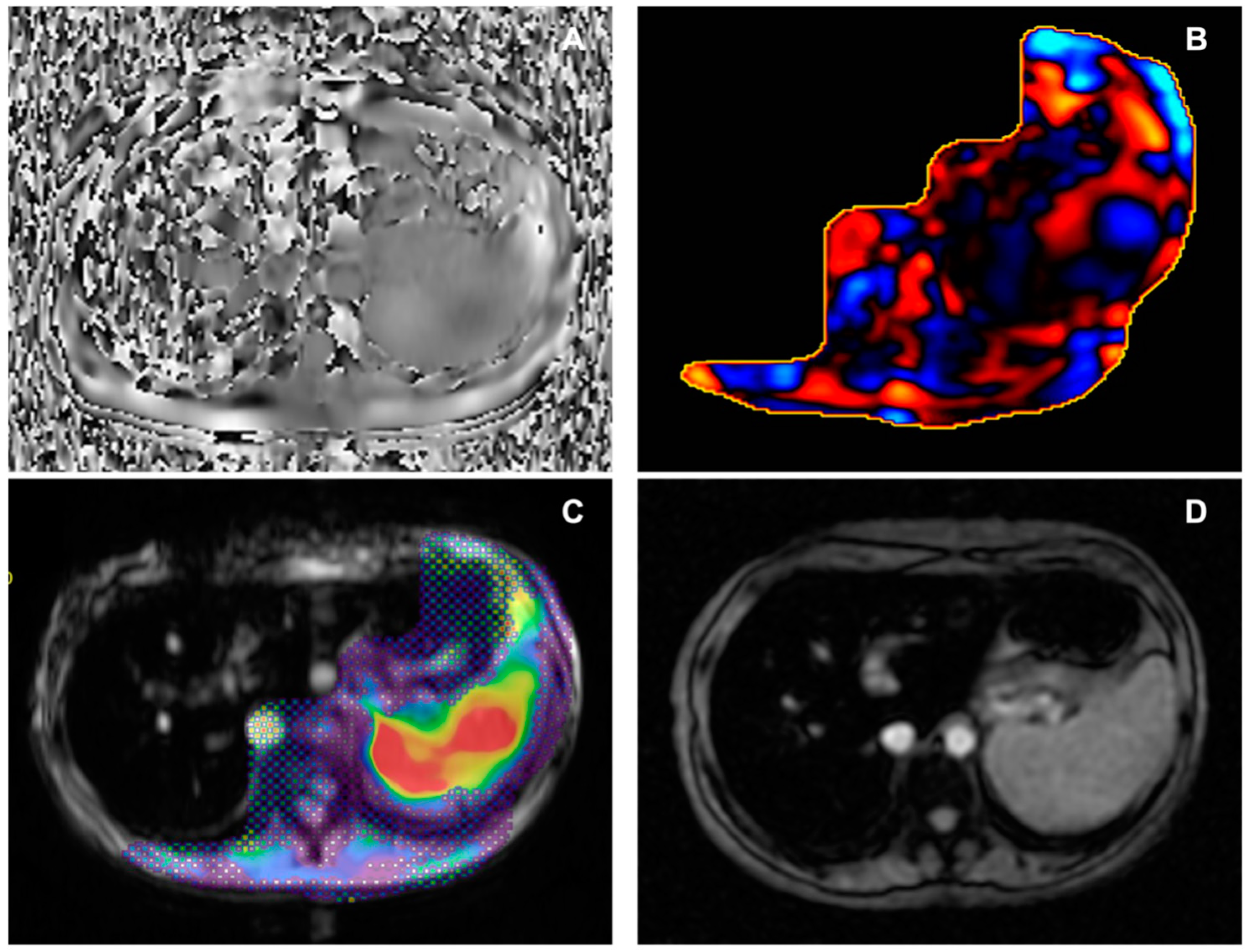
4.6. Quality Control
4.7. Image Analysis
4.8. Frequently Observed Pitfalls
4.9. Accuracy of MRE
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manduca, A.; Bayly, P.J.; Ehman, R.L.; Kolipaka, A.; Royston, T.J.; Sack, I.; Sinkus, R.; Van Beers, B.E. MR elastography: Principles, guidelines, and terminology. Magn. Reson. Med. 2021, 85, 2377–2390. [Google Scholar] [CrossRef]
- Zhang, Y.N.; Fowler, K.J.; Hamilton, G.; Cui, J.Y.; Sy, E.Z.; Balanay, M.; Hooker, J.C.; Szeverenyi, N.; Sirlin, C.B. Liver fat imaging-a clinical overview of ultrasound, CT, and MR imaging. Br. J. Radiol. 2018, 91, 20170959. [Google Scholar] [CrossRef]
- Venkatesh, S.K.; Yin, M.; Ehman, R.L. Magnetic resonance elastography of liver: Technique, analysis, and clinical applications. J. Magn. Reson. Imaging 2013, 37, 544–555. [Google Scholar] [CrossRef]
- Taouli, B.; Alves, F.C. Imaging biomarkers of diffuse liver disease: Current status. Abdom. Radiol. 2020, 45, 3381–3385. [Google Scholar] [CrossRef]
- Guglielmo, F.F.; Venkatesh, S.K.; Mitchell, D.G. Liver MR Elastography Technique and Image Interpretation: Pearls and Pitfalls. Radiographics 2019, 39, 1983–2002. [Google Scholar] [CrossRef]
- Joshi, A.; Muthe, M.M.; Firke, V.; Badgujar, H. Preliminary experience with 3T magnetic resonance elastography imaging of the liver. SA J. Radiol. 2021, 25, a2072. [Google Scholar] [CrossRef]
- Park, C.C.; Nguyen, P.; Hernandez, C.; Bettencourt, R.; Ramirez, K.; Fortney, L.; Hooker, J.; Sy, E.; Savides, M.T.; Alquiraish, M.H.; et al. Magnetic Resonance Elastography vs Transient Elastography in Detection of Fibrosis and Noninvasive Measurement of Steatosis in Patients with Biopsy-Proven Nonalcoholic Fatty Liver Disease. Gastroenterology 2017, 152, 598–607.e2. [Google Scholar] [CrossRef]
- Imajo, K.; Kessoku, T.; Honda, Y.; Tomeno, W.; Ogawa, Y.; Mawatari, H.; Fujita, K.; Yoneda, M.; Taguri, M.; Hyogo, H.; et al. Magnetic Resonance Imaging More Accurately Classifies Steatosis and Fibrosis in Patients with Nonalcoholic Fatty Liver Disease Than Transient Elastography. Gastroenterology 2016, 150, 626–637.e7. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ganger, D.R.; Levitsky, J.; Sternick, L.A.; McCarthy, R.J.; Chen, Z.E.; Fasanati, C.W.; Bolster, B.; Shah, S.; Zuehlsdorff, S.; et al. Assessment of chronic hepatitis and fibrosis: Comparison of MR elastography and diffusion-weighted imaging. AJR Am. J. Roentgenol. 2011, 196, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Jameson, J.L.; Kasper, D.L.; Longo, D.L.; Fauci, A.S.; Hauer, S.L.; Loscalzo, J. Harrison’s Principles of Internal Medicine, 20e; McGraw Hill Medical: New York, NY, USA, 2018. [Google Scholar]
- Chartampilas, E. Imaging of nonalcoholic fatty liver disease and its clinical utility. Hormones 2018, 17, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Thursz, M.; Kamath, P.S.; Mathurin, P.; Szabo, G.; Shah, V.H. Alcohol-related liver disease: Areas of consensus, unmet needs and opportunities for further study. J. Hepatol. 2019, 70, 521–530. [Google Scholar] [CrossRef]
- Venkatesh, S.K.; Wells, M.L.; Miller, F.H.; Jhaveri, K.S.; Silva, A.C.; Taouli, B.; Ehman, R.L. Magnetic resonance elastography: Beyond liver fibrosis-a case-based pictorial review. Abdom. Radiol. 2018, 43, 1590–1611. [Google Scholar] [CrossRef]
- Quock, T.P.; Yan, T.; Chang, E.; Guthrie, S.; Broder, M.S. Epidemiology of AL amyloidosis: A real-world study using US claims data. Blood Adv. 2018, 2, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, L.; Toma, L.; Mercan-Stanciu, A.; Grumeza, M.; Dodot, M.; Isac, T.; Ioanitescu, S. Budd-Chiari syndrome—Various etiologies and imagistic findings. A pictorial review. Med. Ultrason. 2019, 21, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Baumgartner, K.; Bositis, C. Cirrhosis: Diagnosis and Management. Am. Fam. Physician 2019, 100, 759–770. [Google Scholar] [PubMed]
- Gonzalez, R.S.; Washington, K. Primary Biliary Cholangitis and Autoimmune Hepatitis. Surg. Pathol. Clin. 2018, 11, 329–349. [Google Scholar] [CrossRef]
- Horowitz, J.M.; Venkatesh, S.K.; Ehman, R.L.; Jhaveri, K.; Kamath, P.; Ohliger, M.A.; Samir, A.E.; Silva, A.C.; Taouli, B.; Torbenson, M.S.; et al. Evaluation of hepatic fibrosis: A review from the society of abdominal radiology disease focus panel. Abdom. Radiol. 2017, 42, 2037–2053. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.; Talwalkar, J.A.; Glaser, K.J.; Manduca, A.; Grimm, R.C.; Rossman, P.J.; Fidler, J.L.; Ehman, R.L. Assessment of hepatic fibrosis with magnetic resonance elastography. Clin. Gastroenterol. Hepatol. 2007, 5, 1207–1213.e2. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, S.K.; Wang, G.; Lim, S.G.; Wee, A. Magnetic resonance elastography for the detection and staging of liver fibrosis in chronic hepatitis B. Eur. Radiol. 2014, 24, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Talwalkar, J.A.; Yin, M.; Glaser, K.J.; Sanderson, S.O.; Ehman, R.L. Early detection of nonalcoholic steatohepatitis in patients with nonalcoholic fatty liver disease by using MR elastography. Radiology 2011, 259, 749–756. [Google Scholar] [CrossRef]
- Sangha, K.; Chang, S.T.; Cheung, R.; Deshpande, V.S. Cost-effectiveness of MRE versus VCTE in staging fibrosis for nonalcoholic fatty liver disease (NAFLD) patients with advanced fibrosis. Hepatology 2023, 77, 1702–1711. [Google Scholar] [CrossRef] [PubMed]
- Low, G.; Kruse, S.A.; Lomas, D.J. General review of magnetic resonance elastography. World J. Radiol. 2016, 8, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Ghadimi, M.; Sapra, A. Magnetic Resonance Imaging Contraindications. 1 May 2023. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar] [PubMed]
- Venkatesh, S.K.; Yin, M.; Ehman, R.L. Magnetic resonance elastography of liver: Clinical applications. J. Comput. Assist. Tomogr. 2013, 37, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.U.; Lee, J.M.; Yu, M.H.; Yoon, J.H.; Han, J.K.; Choi, B.I.; Glaser, K.J.; Ehman, R.L. Prediction of esophageal varices in patients with cirrhosis: Usefulness of three-dimensional MR elastography with echo-planar imaging technique. Radiology 2014, 272, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Low, G.; Owen, N.E.; Joubert, I.; Patterson, A.J.; Graves, M.J.; Glaser, K.J.; Alexander, G.J.; Lomas, D.J. Reliability of magnetic resonance elastography using multislice two-dimensional spin-echo echo-planar imaging (SE-EPI) and three-dimensional inversion reconstruction for assessing renal stiffness. J. Magn. Reson. Imaging 2015, 42, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Siegmann, K.C.; Xydeas, T.; Sinkus, R.; Kraemer, B.; Vogel, U.; Claussen, C.D. Diagnostic value of MR elastography in addition to contrast-enhanced MR imaging of the breast-initial clinical results. Eur. Radiol. 2010, 20, 318–325. [Google Scholar] [CrossRef]
- Idilman, I.S.; Li, J.; Yin, M.; Venkatesh, S.K. MR elastography of liver: Current status and future perspectives. Abdom. Radiol. 2020, 45, 3444–3462. [Google Scholar] [CrossRef]
- Trout, A.T.; Serai, S.; Mahley, A.D.; Wang, H.; Zhang, Y.; Zhang, B.; Dillman, J.R. Liver Stiffness Measurements with MR Elastography: Agreement and Repeatability across Imaging Systems, Field Strengths, and Pulse Sequences. Radiology 2016, 281, 793–804. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, B.; Yu, H.J.; Huh, J.; Lee, J.H.; Lee, S.S.; Kim, K.W.; Kim, J.K. Reproducibility of hepatic MR elastography across field strengths, pulse sequences, scan intervals, and readers. Abdom. Radiol. 2020, 45, 107–115. [Google Scholar] [CrossRef]
- Wang, K.; Manning, P.; Szeverenyi, N.; Wolfson, T.; Hamilton, G.; Middleton, M.S.; Vaida, F.; Yin, M.; Glaser, K.; Ehman, R.L.; et al. Repeatability and reproducibility of 2D and 3D hepatic MR elastography with rigid and flexible drivers at end-expiration and end-inspiration in healthy volunteers. Abdom. Radiol. 2017, 42, 2843–2854. [Google Scholar] [CrossRef]
- Plaikner, M.; Kremser, C.; Zoller, H.; Steurer, M.; Glodny, B.; Jaschke, W.; Henninger, B. Does gadoxetate disodium affect MRE measurements in the delayed hepatobiliary phase? Eur. Radiol. 2019, 29, 829–837. [Google Scholar] [CrossRef]
- Dzyubak, B.; Venkatesh, S.K.; Manduca, A.; Glaser, K.J.; Ehman, R.L. Automated liver elasticity calculation for MR elastography. J. Magn. Reson. Imaging 2016, 43, 1055–1063. [Google Scholar] [CrossRef]
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic hepatitis C. Hepatology 1996, 24, 289–293. [Google Scholar] [CrossRef]
- Venkatesh, S.K.; Ehman, R.L. Magnetic resonance elastography of liver. Magn. Reson. Imaging Clin. N. Am. 2014, 22, 433–446. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.; Glaser, K.J.; Talwalkar, J.A.; Chen, J.; Manduca, A.; Ehman, R.L. Hepatic MR Elastography: Clinical Performance in a Series of 1377 Consecutive Examinations. Radiology 2016, 278, 114–124. [Google Scholar] [CrossRef]
- Ghoz, H.M.; Kröner, P.T.; Stancampiano, F.F.; Bowman, A.W.; Vishnu, P.; Heckman, M.G.; Diehl, N.N.; McLeod, E.; Nikpour, N.; Palmer, W.C. Hepatic iron overload identified by magnetic resonance imaging-based T2* is a predictor of non-diagnostic elastography. Quant. Imaging Med. Surg. 2019, 9, 921–927. [Google Scholar] [CrossRef]
- Serai, S.D.; Trout, A.T. Can MR elastography be used to measure liver stiffness in patients with iron overload? Abdom. Radiol. 2019, 44, 104–109. [Google Scholar] [CrossRef]
- Wagner, M.; Corcuera-Solano, I.; Lo, G.; Esses, S.; Liao, J.; Besa, C.; Chen, N.; Abraham, G.; Fung, M.; Babb, J.S.; et al. Technical Failure of MR Elastography Examinations of the Liver: Experience from a Large Single-Center Study. Radiology 2017, 284, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Morisaka, H.; Motosugi, U.; Ichikawa, S.; Nakazawa, T.; Kondo, T.; Funayama, S.; Matsuda, M.; Ichikawa, T.; Onishi, H. Magnetic resonance elastography is as accurate as liver biopsy for liver fibrosis staging. J. Magn. Reson. Imaging 2018, 47, 1268–1275. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Wolfson, T.; Ang, B.; Hooker, J.; Behling, C.; Peterson, M.; Valasek, M.; Lin, G.; Brenner, D.; Gamst, A.; et al. Magnetic resonance elastography predicts advanced fibrosis in patients with nonalcoholic fatty liver disease: A prospective study. Hepatology 2014, 60, 1920–1928. [Google Scholar] [CrossRef]
- Selvaraj, E.A.; Mózes, F.E.; Jayaswal, A.N.A.; Zafarmand, M.H.; Vali, Y.; Lee, J.A.; Levick, C.K.; Young, L.A.J.; Palaniyappan, N.; Liu, C.H.; et al. Diagnostic accuracy of elastography and magnetic resonance imaging in patients with NAFLD: A systematic review and meta-analysis. J. Hepatol. 2021, 75, 770–785. [Google Scholar] [CrossRef] [PubMed]
- Schambeck, J.P.L.; Forte, G.C.; Gonçalves, L.M.; Stuker, G.; Kotlinski, J.B.F.; Tramontin, G.; Altmayer, S.; Watte, G.; Hochhegger, B. Diagnostic accuracy of magnetic resonance elastography and point-shear wave elastography for significant hepatic fibrosis screening: Systematic review and meta-analysis. PLoS ONE 2023, 18, e0271572. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Parameters 2D GRE 1.5 T | Driver Parameters | ||
|---|---|---|---|
| Pulse sequence | MR-Touch | Amplitude (%) | 90 |
| Bandwidth (kHz) | 62.50 | Frequency (Hz) | 60 |
| FOV (mm) | 430 × 430 | ||
| Matrix | 224 × 64 | ||
| TE (msec) | Minimum TE (~20) | ||
| TR(msec) | 50 | ||
| Flip angle (°) | 30 | ||
| NEX | 1 | ||
| Fat suppression | active | ||
| Slice thickness (mm) | 10 | ||
| Slice gap (mm) | 0 | ||
| N. of slices | 4 |
| Technical Issues | Liver Diseases/Anatomical Conditions |
|---|---|
| Active driver failure | Liver iron overload (70%) |
| Incorrectly positioned/secured passive driver | Severe steatosis |
| Improper slice selection | |
| Disconnected/Kinked tube connecting active to passive driver | |
| Poor breath-hold |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zerunian, M.; Masci, B.; Caruso, D.; Pucciarelli, F.; Polici, M.; Nardacci, S.; De Santis, D.; Iannicelli, E.; Laghi, A. Liver Magnetic Resonance Elastography: Focus on Methodology, Technique, and Feasibility. Diagnostics 2024, 14, 379. https://doi.org/10.3390/diagnostics14040379
Zerunian M, Masci B, Caruso D, Pucciarelli F, Polici M, Nardacci S, De Santis D, Iannicelli E, Laghi A. Liver Magnetic Resonance Elastography: Focus on Methodology, Technique, and Feasibility. Diagnostics. 2024; 14(4):379. https://doi.org/10.3390/diagnostics14040379
Chicago/Turabian StyleZerunian, Marta, Benedetta Masci, Damiano Caruso, Francesco Pucciarelli, Michela Polici, Stefano Nardacci, Domenico De Santis, Elsa Iannicelli, and Andrea Laghi. 2024. "Liver Magnetic Resonance Elastography: Focus on Methodology, Technique, and Feasibility" Diagnostics 14, no. 4: 379. https://doi.org/10.3390/diagnostics14040379
APA StyleZerunian, M., Masci, B., Caruso, D., Pucciarelli, F., Polici, M., Nardacci, S., De Santis, D., Iannicelli, E., & Laghi, A. (2024). Liver Magnetic Resonance Elastography: Focus on Methodology, Technique, and Feasibility. Diagnostics, 14(4), 379. https://doi.org/10.3390/diagnostics14040379