
Clinical Biochemistry of Serum Troponin

 , ,
, ,
Abstract
:1. Introduction
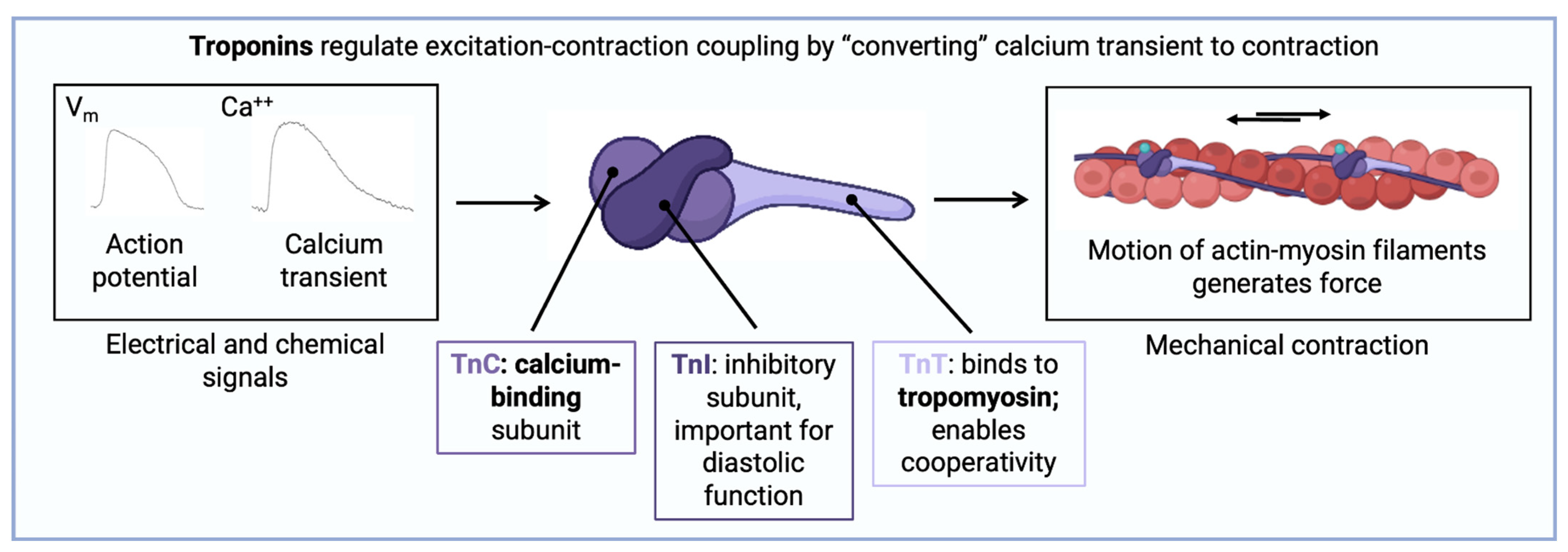
2. Molecular Structure of Troponins
3. Identity and Source of Troponin Complexes
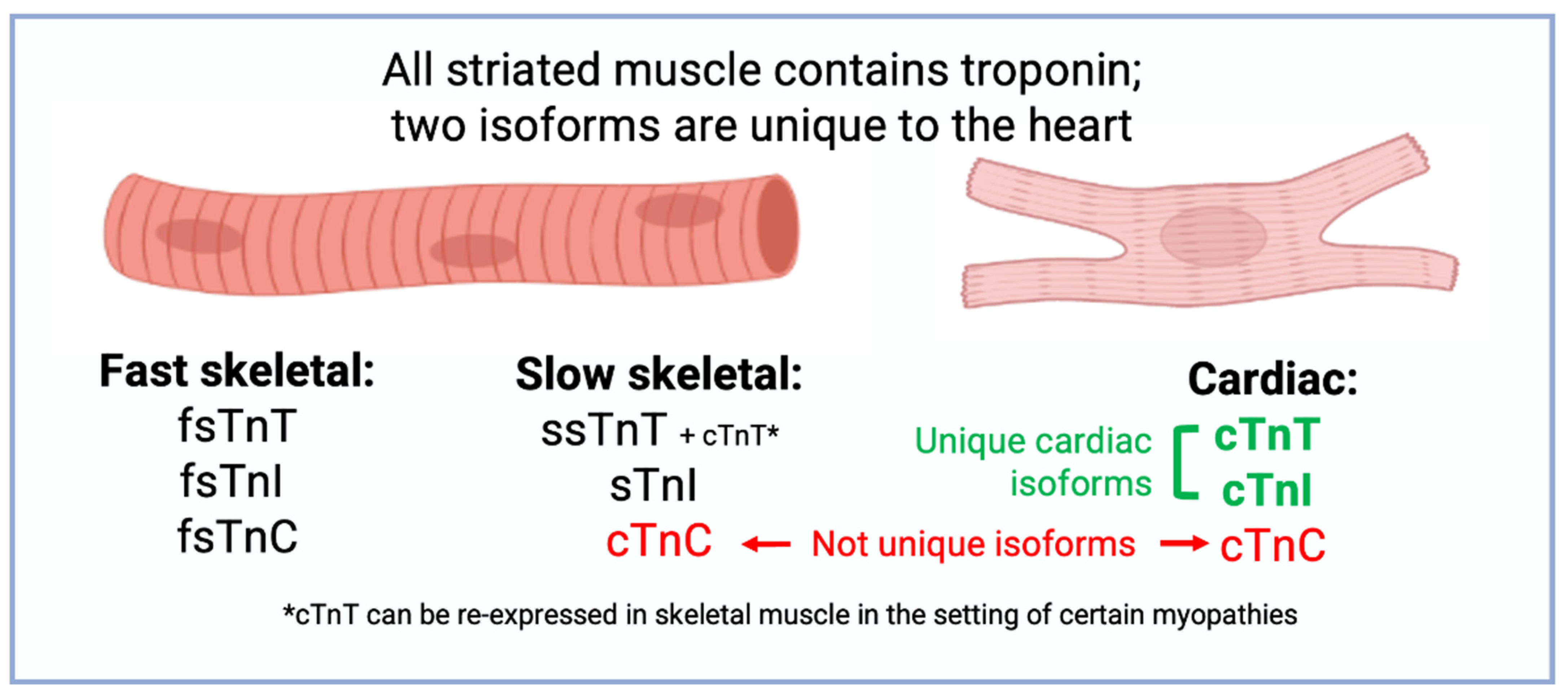
4. Isoforms of Troponin
5. Reference Limit Definitions
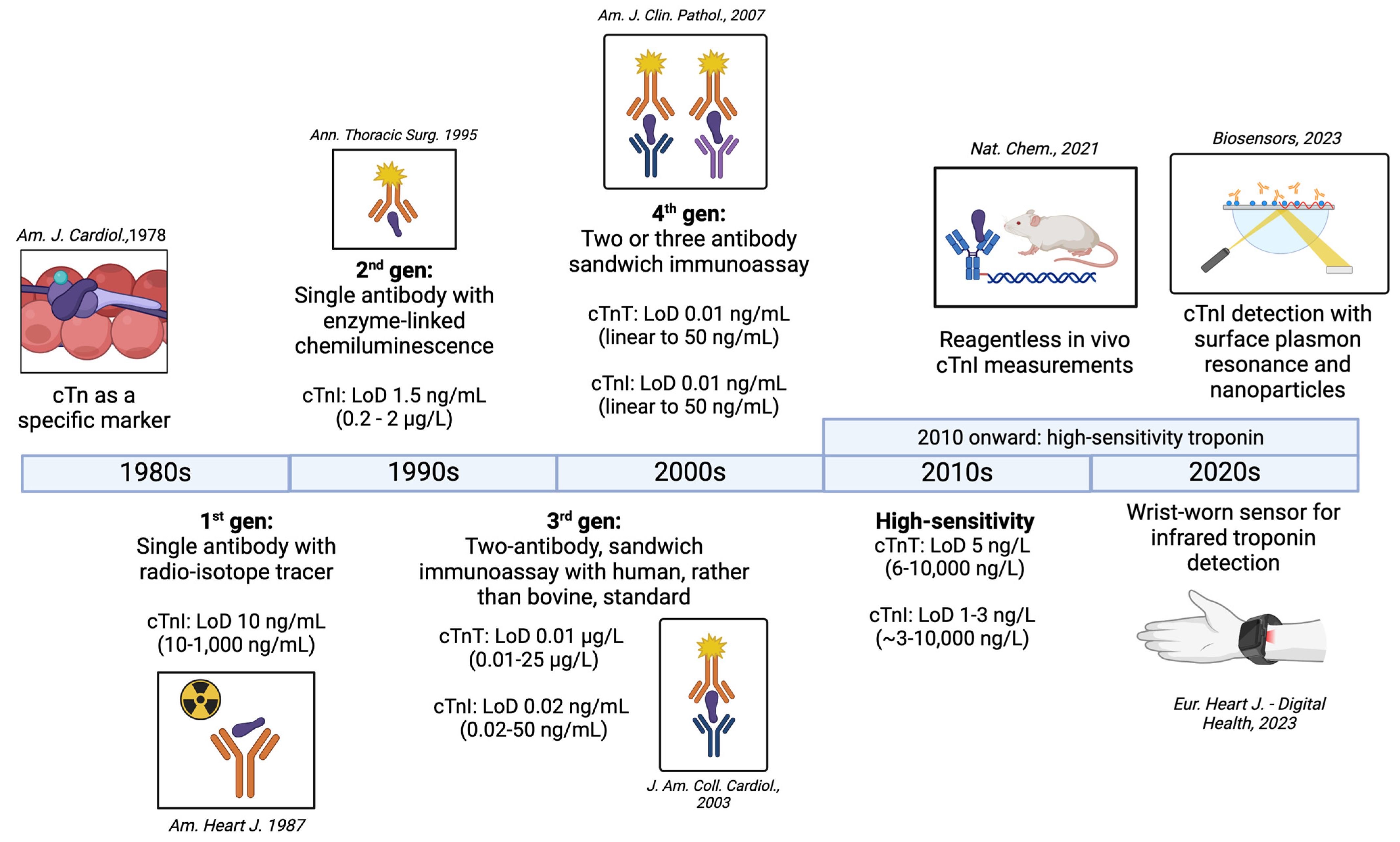
6. Generations of Troponin Assays
6.1. First Generation
6.2. Second Generation
6.3. Third Generation
6.4. Fourth Generation
7. High-Sensitivity Troponin
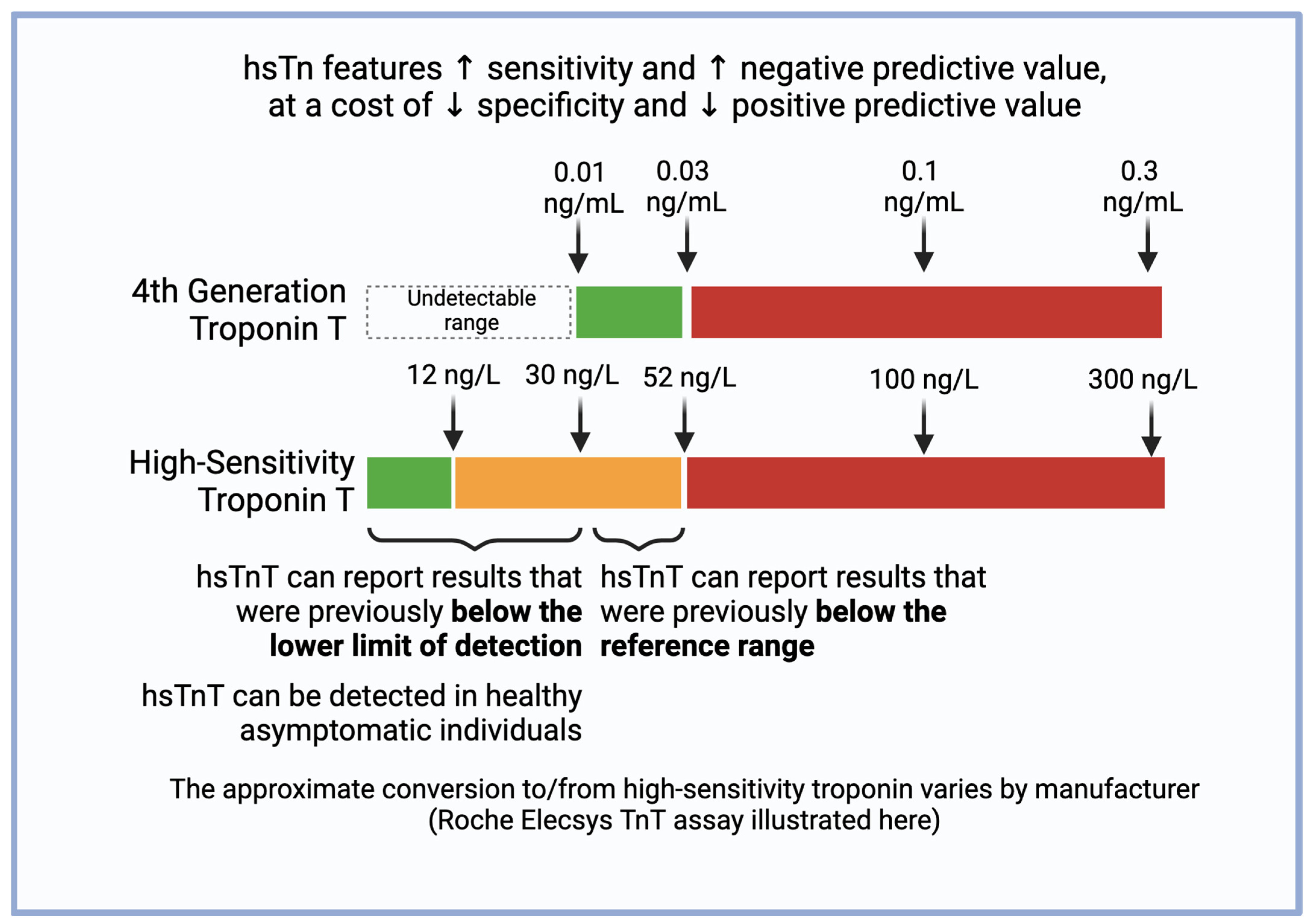
7.1. Definition of High Sensitivity
7.2. Conceptualizing Equivalence of Fourth-Generation and High-Sensitivity Values
7.3. Clinical Implications of High-Sensitivity Troponin
7.4. Sex-Specific Considerations of High-Sensitivity Troponin
8. Future of Troponin Assays
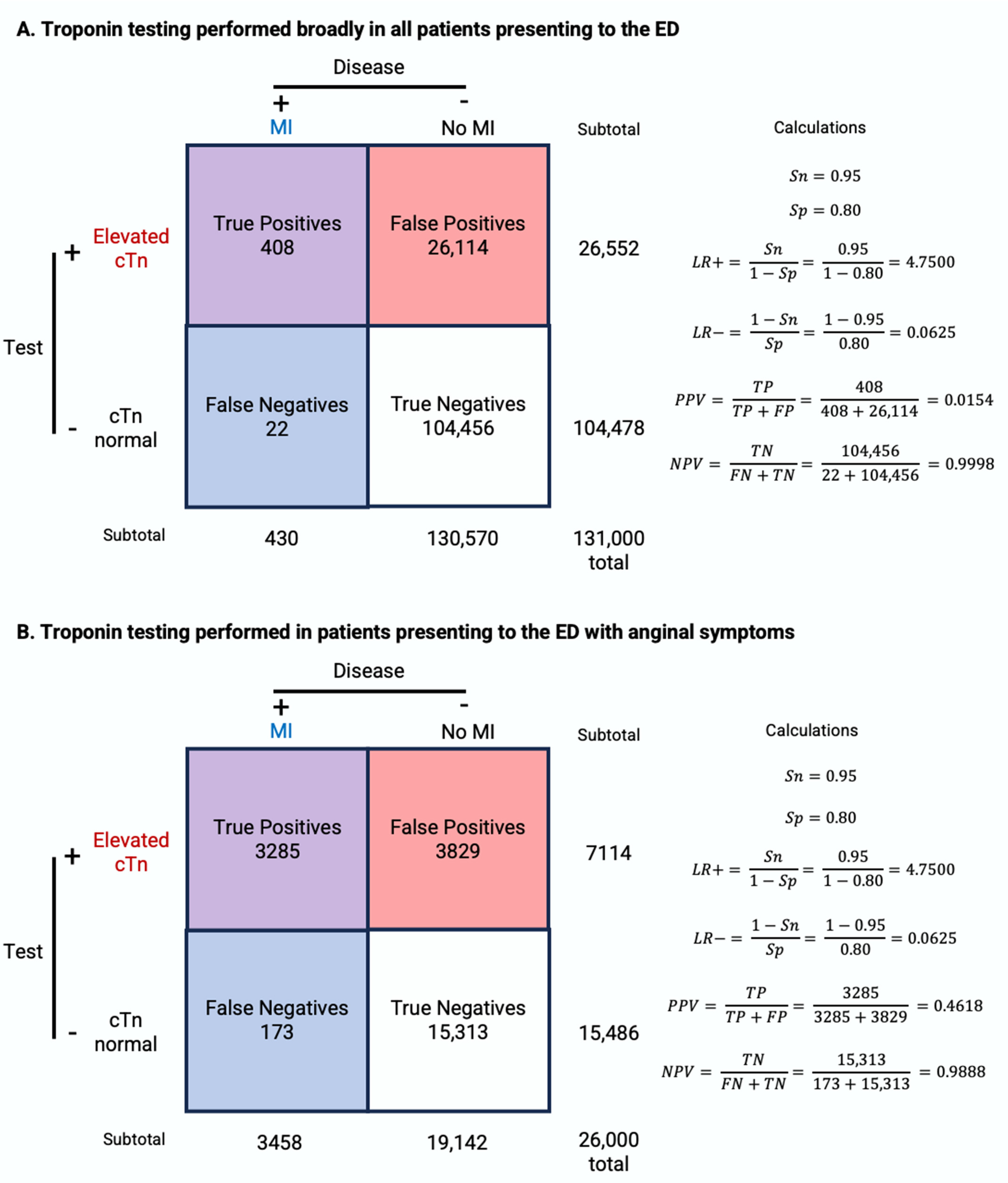
9. Conditional Probability for the Interpretation of Troponin Testing
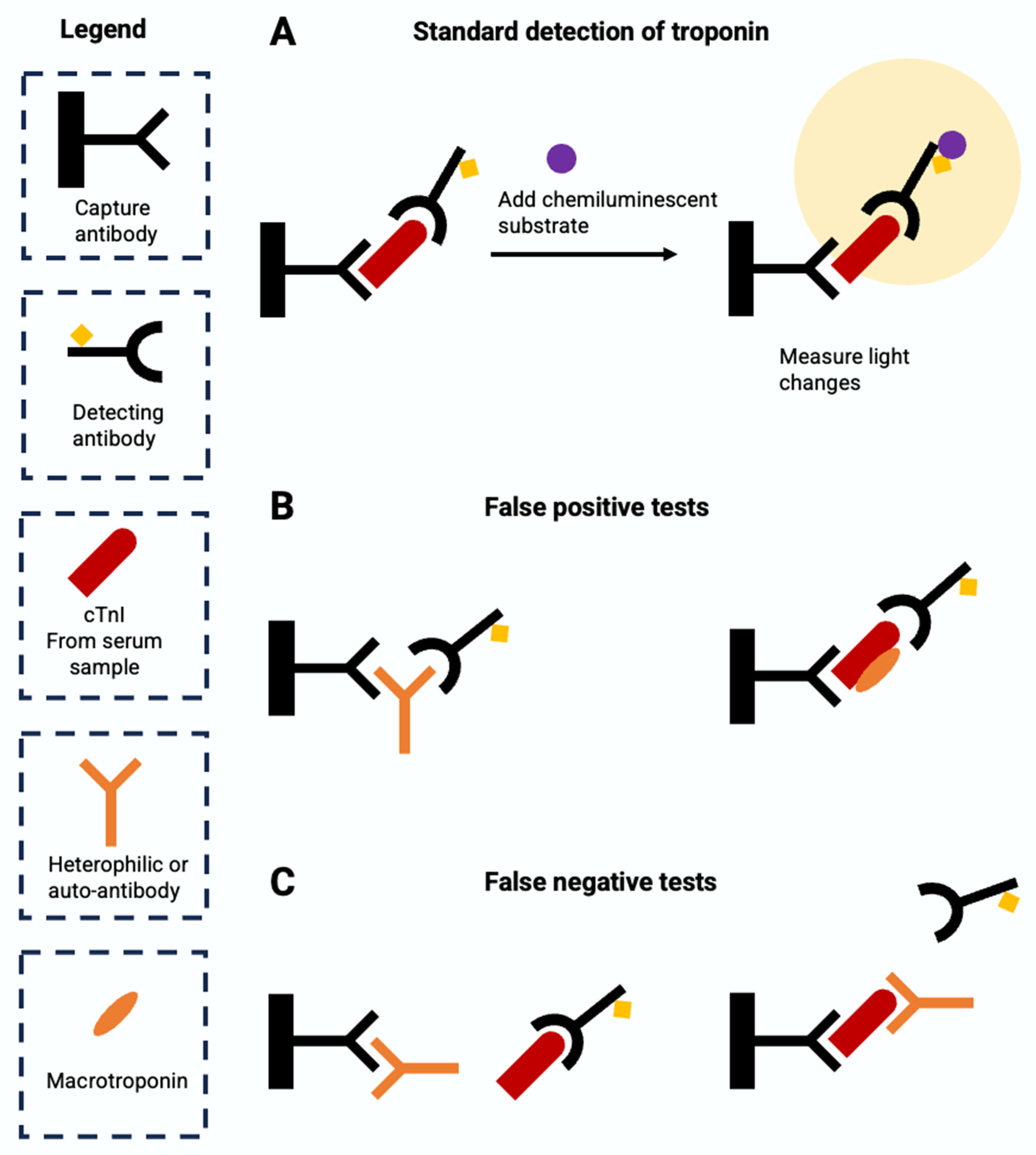
10. Causes of False Positive and False Negative Results
11. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Marah, M.; Grubman, S.; Allen, S.; Ye, Z.; Park, D.Y.; Vemmou, E.; Gokhan, I.; Sun, W.; Possick, S.; Kwan, J.; et al. Interpretation of Serum Troponin in the Era of High-Sensitivity Troponin Testing. Diagnostics, 2024; under review. [Google Scholar]
- Wu, Q.L.; Jha, P.K.; Raychowdhury, M.K.; Du, Y.; Leavis, P.C.; Sarkar, S. Isolation and Characterization of Human Fast Skeletal Beta Troponin T cDNA: Comparative Sequence Analysis of Isoforms and Insight into the Evolution of Members of a Multigene Family. DNA Cell Biol. 1994, 13, 217–233. [Google Scholar] [CrossRef]
- Yang, S.; Barbu-Tudoran, L.; Orzechowski, M.; Craig, R.; Trinick, J.; White, H.; Lehman, W. Three-Dimensional Organization of Troponin on Cardiac Muscle Thin Filaments in the Relaxed State. Biophys. J. 2014, 106, 855–864. [Google Scholar] [CrossRef]
- Spudich, J.A. The Myosin Swinging Cross-Bridge Model. Nat. Rev. Mol. Cell Biol. 2001, 2, 387–392. [Google Scholar] [CrossRef]
- Kobayashi, T.; Solaro, R.J. Calcium, Thin Filaments, and the Integrative Biology of Cardiac Contractility. Annu. Rev. Physiol. 2005, 67, 39–67. [Google Scholar] [CrossRef]
- Greaser, M.L.; Gergely, J. Reconstitution of Troponin Activity from Three Protein Components. J. Biol. Chem. 1971, 246, 4226–4233. [Google Scholar] [CrossRef]
- Hartshorne, D.J.; Mueller, H. Fractionation of Troponin into Two Distinct Proteins. Biochem. Biophys. Res. Commun. 1968, 31, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Greaser, M.L.; Gergely, J. Purification and Properties of the Components from Troponin. J. Biol. Chem. 1973, 248, 2125–2133. [Google Scholar] [CrossRef]
- Heeley, D.H.; Golosinska, K.; Smillie, L.B. The Effects of Troponin T Fragments T1 and T2 on the Binding of Nonpolymerizable Tropomyosin to F-Actin in the Presence and Absence of Troponin I and Troponin C. J. Biol. Chem. 1987, 262, 9971–9978. [Google Scholar] [CrossRef]
- Sia, S.K.; Li, M.X.; Spyracopoulos, L.; Gagné, S.M.; Liu, W.; Putkey, J.A.; Sykes, B.D. Structure of Cardiac Muscle Troponin C Unexpectedly Reveals a Closed Regulatory Domain. J. Biol. Chem. 1997, 272, 18216–18221. [Google Scholar] [CrossRef]
- Li, M.X.; Hwang, P.M. Structure and Function of Cardiac Troponin C (TNNC1): Implications for Heart Failure, Cardiomyopathies, and Troponin Modulating Drugs. Gene 2015, 571, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Dean, K.J. Biochemistry and Molecular Biology of Troponins I and T. In Cardiac Markers; Wu, A.H.B., Ed.; Pathology and Laboratory Medicine; Humana Press: Totowa, NJ, USA, 1998; pp. 193–204. ISBN 978-1-4612-1806-7. [Google Scholar]
- Creso, J.G.; Campbell, S.G. Potential Impacts of the Cardiac Troponin I Mobile Domain on Myofilament Activation and Relaxation. J. Mol. Cell. Cardiol. 2021, 155, 50–57. [Google Scholar] [CrossRef]
- Solaro, R.J.; Moir, A.J.G.; Perry, S.V. Phosphorylation of Troponin I and the Inotropic Effect of Adrenaline in the Perfused Rabbit Heart. Nature 1976, 262, 615–617. [Google Scholar] [CrossRef]
- Kentish, J.C.; McCloskey, D.T.; Layland, J.; Palmer, S.; Leiden, J.M.; Martin, A.F.; Solaro, R.J. Phosphorylation of Troponin I by Protein Kinase A Accelerates Relaxation and Crossbridge Cycle Kinetics in Mouse Ventricular Muscle. Circ. Res. 2001, 88, 1059–1065. [Google Scholar] [CrossRef]
- Pi, Y.; Zhang, D.; Kemnitz, K.R.; Wang, H.; Walker, J.W. Protein Kinase C and A Sites on Troponin I Regulate Myofilament Ca2+ Sensitivity and ATPase Activity in the Mouse Myocardium. J. Physiol. 2003, 552, 845–857. [Google Scholar] [CrossRef] [PubMed]
- Venema, R.C.; Kuo, J.F. Protein Kinase C-Mediated Phosphorylation of Troponin I and C-Protein in Isolated Myocardial Cells Is Associated with Inhibition of Myofibrillar Actomyosin MgATPase. J. Biol. Chem. 1993, 268, 2705–2711. [Google Scholar] [CrossRef]
- Hinkle, A.; Goranson, A.; Butters, C.A.; Tobacman, L.S. Roles for the Troponin Tail Domain in Thin Filament Assembly and Regulation: A Deletional Study of Cardiac Troponin T. J. Biol. Chem. 1999, 274, 7157–7164. [Google Scholar] [CrossRef] [PubMed]
- Chaulin, A.M. Cardiac Troponins Metabolism: From Biochemical Mechanisms to Clinical Practice (Literature Review). Int. J. Mol. Sci. 2021, 22, 10928. [Google Scholar] [CrossRef]
- Laugaudin, G.; Kuster, N.; Petiton, A.; Leclercq, F.; Gervasoni, R.; Macia, J.-C.; Cung, T.-T.; Dupuy, A.-M.; Solecki, K.; Lattuca, B.; et al. Kinetics of High-Sensitivity Cardiac Troponin T and I Differ in Patients with ST-Segment Elevation Myocardial Infarction Treated by Primary Coronary Intervention. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 354–363. [Google Scholar] [CrossRef]
- Vylegzhanina, A.V.; Kogan, A.E.; Katrukha, I.A.; Koshkina, E.V.; Bereznikova, A.V.; Filatov, V.L.; Bloshchitsyna, M.N.; Bogomolova, A.P.; Katrukha, A.G. Full-Size and Partially Truncated Cardiac Troponin Complexes in the Blood of Patients with Acute Myocardial Infarction. Clin. Chem. 2019, 65, 882–892. [Google Scholar] [CrossRef]
- Bates, K.J.; Hall, E.M.; Fahie-Wilson, M.N.; Kindler, H.; Bailey, C.; Lythall, D.; Lamb, E.J. Circulating Immunoreactive Cardiac Troponin Forms Determined by Gel Filtration Chromatography after Acute Myocardial Infarction. Clin. Chem. 2010, 56, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.B.; Feng, Y.-J.; Moore, R.; Apple, F.S.; McPherson, P.H.; Buechler, K.F.; Bodor, G.; for the American Association; Clinical Chemistry Subcommittee on cTnI Standardization. Characterization of Cardiac Troponin Subunit Release into Serum after Acute Myocardial Infarction and Comparison of Assays for Troponin T and I. Clin. Chem. 1998, 44, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Katrukha, I.A.; Kogan, A.E.; Vylegzhanina, A.V.; Kharitonov, A.V.; Tamm, N.N.; Filatov, V.L.; Bereznikova, A.V.; Koshkina, E.V.; Katrukha, A.G. Full-Size Cardiac Troponin I and Its Proteolytic Fragments in Blood of Patients with Acute Myocardial Infarction: Antibody Selection for Assay Development. Clin. Chem. 2018, 64, 1104–1112. [Google Scholar] [CrossRef]
- Mahmud, Z.; Zahran, S.; Liu, P.B.; Reiz, B.; Chan, B.Y.H.; Roczkowsky, A.; McCartney, C.-S.E.; Davies, P.L.; Li, L.; Schulz, R.; et al. Structure and Proteolytic Susceptibility of the Inhibitory C-Terminal Tail of Cardiac Troponin I. Biochim. Biophys. Acta (BBA) Gen. Subj. 2019, 1863, 661–671. [Google Scholar] [CrossRef]
- van Wijk, X.M.R.; Claassen, S.; Enea, N.S.; Li, P.; Yang, S.; Brouwer, M.A.; Cramer, G.E.; Zuk, R.; Lynch, K.L.; Wu, A.H.B. Cardiac Troponin I Is Present in Plasma of Type 1 Myocardial Infarction Patients and Patients with Troponin I Elevations Due to Other Etiologies as Complex with Little Free I. Clin. Biochem. 2019, 73, 35–43. [Google Scholar] [CrossRef]
- Mingels, A.M.A.; Cardinaels, E.P.M.; Broers, N.J.H.; van Sleeuwen, A.; Streng, A.S.; van Dieijen-Visser, M.P.; Kooman, J.P.; Bekers, O. Cardiac Troponin T: Smaller Molecules in Patients with End-Stage Renal Disease than after Onset of Acute Myocardial Infarction. Clin. Chem. 2017, 63, 683–690. [Google Scholar] [CrossRef]
- Vroemen, W.H.M.; Mezger, S.T.P.; Masotti, S.; Clerico, A.; Bekers, O.; de Boer, D.; Mingels, A. Cardiac Troponin T: Only Small Molecules in Recreational Runners after Marathon Completion. J. Appl. Lab. Med. 2019, 3, 909–911. [Google Scholar] [CrossRef]
- Hammarsten, O.; Mair, J.; Möckel, M.; Lindahl, B.; Jaffe, A.S. Possible Mechanisms behind Cardiac Troponin Elevations. Biomarkers 2018, 23, 725–734. [Google Scholar] [CrossRef]
- Weil, B.R.; Young, R.F.; Shen, X.; Suzuki, G.; Qu, J.; Malhotra, S.; Canty, J.M. Brief Myocardial Ischemia Produces Cardiac Troponin I Release and Focal Myocyte Apoptosis in the Absence of Pathological Infarction in Swine. JACC Basic Transl. Sci. 2017, 2, 105–114. [Google Scholar] [CrossRef]
- Weil, B.R.; Suzuki, G.; Young, R.F.; Iyer, V.; Canty, J.M. Troponin Release and Reversible Left Ventricular Dysfunction after Transient Pressure Overload. J. Am. Coll. Cardiol. 2018, 71, 2906–2916. [Google Scholar] [CrossRef]
- Hessel, M.H.M.; Atsma, D.E.; van der Valk, E.J.M.; Bax, W.H.; Schalij, M.J.; van der Laarse, A. Release of Cardiac Troponin I from Viable Cardiomyocytes Is Mediated by Integrin Stimulation. Pflug. Arch.-Eur. J. Physiol. 2008, 455, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Hickman, P.E.; Potter, J.M.; Aroney, C.; Koerbin, G.; Southcott, E.; Wu, A.H.B.; Roberts, M.S. Cardiac Troponin May Be Released by Ischemia Alone, without Necrosis. Clin. Chim. Acta 2010, 411, 318–323. [Google Scholar] [CrossRef]
- Giordano, S.; Estes, R.; Li, W.; George, R.; Gilford, T.; Glasgow, K.; Hallman, H.; Josephat, F.; Oliveira, A.; Xavier, N.; et al. Troponin Structure and Function in Health and Disease. Am. Soc. Clin. Lab. Sci. 2018, 31, 192–199. [Google Scholar] [CrossRef]
- Schreier, T.; Kedes, L.; Gahlmann, R. Cloning, Structural Analysis, and Expression of the Human Slow Twitch Skeletal Muscle/Cardiac Troponin C Gene. J. Biol. Chem. 1990, 265, 21247–21253. [Google Scholar] [CrossRef]
- Dhoot, G.K.; Frearson, N.; Perry, S.V. Polymorphic Forms of Troponin T and Troponin C and Their Localization in Striated Muscle Cell Types. Exp. Cell Res. 1979, 122, 339–350. [Google Scholar] [CrossRef]
- Sweeney, H.L.; Brito, R.M.; Rosevear, P.R.; Putkey, J.A. The Low-Affinity Ca2(+)-Binding Sites in Cardiac/Slow Skeletal Muscle Troponin C Perform Distinct Functions: Site I Alone Cannot Trigger Contraction. Proc. Natl. Acad. Sci. USA 1990, 87, 9538–9542. [Google Scholar] [CrossRef]
- Sasse, S.; Brand, N.J.; Kyprianou, P.; Dhoot, G.K.; Wade, R.; Arai, M.; Periasamy, M.; Yacoub, M.H.; Barton, P.J. Troponin I Gene Expression during Human Cardiac Development and in End-Stage Heart Failure. Circ. Res. 1993, 72, 932–938. [Google Scholar] [CrossRef]
- Bodor, G.S.; Oakeley, A.E.; Allen, P.D.; Crimmins, D.L.; Ladenson, J.H.; Anderson, P.A.W. Troponin I Phosphorylation in the Normal and Failing Adult Human Heart. Circulation 1997, 96, 1495–1500. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.A.W.; Greig, A.; Mark, T.M.; Malouf, N.N.; Oakeley, A.E.; Ungerleider, R.M.; Allen, P.D.; Kay, B.K. Molecular Basis of Human Cardiac Troponin T Isoforms Expressed in the Developing, Adult, and Failing Heart. Circ. Res. 1995, 76, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.V.; Guzman, G.; Zhao, J.; Potter, J.D. Cardiac Troponin T Isoforms Affect the Ca2+ Sensitivity and Inhibition of Force Development. Insights into the Role of Troponin T Isoforms in the Heart. J. Biol. Chem. 2002, 277, 35341–35349. [Google Scholar] [CrossRef]
- Feng, H.-Z.; Biesiadecki, B.J.; Yu, Z.-B.; Hossain, M.M.; Jin, J.-P. Restricted N-Terminal Truncation of Cardiac Troponin T: A Novel Mechanism for Functional Adaptation to Energetic Crisis. J. Physiol. 2008, 586, 3537–3550. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.; Ren, J.; Guo, W. Sarcomeric Protein Isoform Transitions in Cardiac Muscle: A Journey to Heart Failure. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2015, 1852, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Wens, S.C.A.; Schaaf, G.J.; Michels, M.; Kruijshaar, M.E.; van Gestel, T.J.M.; In’t Groen, S.; Pijnenburg, J.; Dekkers, D.H.W.; Demmers, J.A.A.; Verdijk, L.B.; et al. Elevated Plasma Cardiac Troponin T Levels Caused by Skeletal Muscle Damage in Pompe Disease. Circ. Cardiovasc. Genet. 2016, 9, 6–13. [Google Scholar] [CrossRef]
- du Fay de Lavallaz, J.; Prepoudis, A.; Wendebourg, M.J.; Kesenheimer, E.; Kyburz, D.; Daikeler, T.; Haaf, P.; Wanschitz, J.; Löscher, W.N.; Schreiner, B.; et al. Skeletal Muscle Disorders: A Noncardiac Source of Cardiac Troponin T. Circulation 2022, 145, 1764–1779. [Google Scholar] [CrossRef]
- Januzzi, J.L.; Mahler, S.A.; Christenson, R.H.; Rymer, J.; Newby, L.K.; Body, R.; Morrow, D.A.; Jaffe, A.S. Recommendations for Institutions Transitioning to High-Sensitivity Troponin Testing: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2019, 73, 1059–1077. [Google Scholar] [CrossRef]
- Sandoval, Y.; Apple, F.S.; Mahler, S.A.; Body, R.; Collinson, P.O.; Jaffe, A.S.; International Federation of Clinical Chemistry and Laboratory Medicine Committee on the Clinical Application of Cardiac Biomarkers. High-Sensitivity Cardiac Troponin and the 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guidelines for the Evaluation and Diagnosis of Acute Chest Pain. Circulation 2022, 146, 569–581. [Google Scholar] [CrossRef]
- Sandoval, Y.; Lewis, B.R.; Mehta, R.A.; Ola, O.; Knott, J.D.; De Michieli, L.; Akula, A.; Lobo, R.; Yang, E.H.; Gharacholou, S.M.; et al. Rapid Exclusion of Acute Myocardial Injury and Infarction with a Single High-Sensitivity Cardiac Troponin T in the Emergency Department: A Multicenter United States Evaluation. Circulation 2022, 145, 1708–1719. [Google Scholar] [CrossRef]
- Writing Committee Members; Gulati, M.; Levy, P.D.; Mukherjee, D.; Amsterdam, E.; Bhatt, D.L.; Birtcher, K.K.; Blankstein, R.; Boyd, J.; Bullock-Palmer, R.P.; et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Cardiovasc. Comput. Tomogr. 2022, 16, 54–122. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Sandoval, Y.; Apple, F.S.; Saenger, A.K.; Collinson, P.O.; Wu, A.H.B.; Jaffe, A.S. 99th Percentile Upper-Reference Limit of Cardiac Troponin and the Diagnosis of Acute Myocardial Infarction. Clin. Chem. 2020, 66, 1167–1180. [Google Scholar] [CrossRef]
- Alpert, J.S.; Thygesen, K.; Antman, E.; Bassand, J.P. Myocardial Infarction Redefined—A Consensus Document of The Joint European Society of Cardiology/American College of Cardiology Committee for the Redefinition of Myocardial Infarction. J. Am. Coll. Cardiol. 2000, 36, 959–969. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; White, H.D.; Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal Definition of Myocardial Infarction. Eur. Heart J. 2007, 28, 2525–2538. [Google Scholar] [CrossRef]
- Cummins, B.; Auckland, M.L.; Cummins, P. Cardiac-Specific Troponin-I Radioimmunoassay in the Diagnosis of Acute Myocardial Infarction. Am. Heart J. 1987, 113, 1333–1344. [Google Scholar] [CrossRef]
- Etievent, J.P.; Chocron, S.; Toubin, G.; Taberlet, C.; Alwan, K.; Clement, F.; Cordier, A.; Schipman, N.; Kantelip, J.P. Use of Cardiac Troponin I as a Marker of Perioperative Myocardial Ischemia. Ann. Thorac. Surg. 1995, 59, 1192–1194. [Google Scholar] [CrossRef] [PubMed]
- Melanson, S.E.F.; Morrow, D.A.; Jarolim, P. Earlier Detection of Myocardial Injury in a Preliminary Evaluation Using a New Troponin I Assay with Improved Sensitivity. Am. J. Clin. Pathol. 2007, 128, 282–286. [Google Scholar] [CrossRef]
- Choudhary, S.; Altintas, Z. Development of a Point-of-Care SPR Sensor for the Diagnosis of Acute Myocardial Infarction. Biosensors 2023, 13, 229. [Google Scholar] [CrossRef]
- Das, J.; Gomis, S.; Chen, J.B.; Yousefi, H.; Ahmed, S.; Mahmud, A.; Zhou, W.; Sargent, E.H.; Kelley, S.O. Reagentless Biomolecular Analysis Using a Molecular Pendulum. Nat. Chem. 2021, 13, 428–434. [Google Scholar] [CrossRef]
- Titus, J.; Wu, A.H.B.; Biswal, S.; Burman, A.; Sengupta, S.P.; Sengupta, P.P. Development and Preliminary Validation of Infrared Spectroscopic Device for Transdermal Assessment of Elevated Cardiac Troponin. Commun. Med. 2022, 2, 42. [Google Scholar] [CrossRef]
- Ammann, P.; Maggiorini, M.; Bertel, O.; Haenseler, E.; Joller-Jemelka, H.I.; Oechslin, E.; Minder, E.I.; Rickli, H.; Fehr, T. Troponin as a Risk Factor for Mortality in Critically Ill Patients without Acute Coronary Syndromes. J. Am. Coll. Cardiol. 2003, 41, 2004–2009. [Google Scholar] [CrossRef] [PubMed]
- Trahern, C.A.; Gere, J.B.; Krauth, G.H.; Bigham, D.A. Clinical Assessment of Serum Myosin Light Chains in the Diagnosis of Acute Myocardial Infarction. Am. J. Cardiol. 1978, 41, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Su, X.; Zhang, W.; Yi, S.; Zhang, G.; Jiang, S.; Li, H.; Li, S.; Xia, F. Progress, Opportunities, and Challenges of Troponin Analysis in the Early Diagnosis of Cardiovascular Diseases. Anal. Chem. 2022, 94, 442–463. [Google Scholar] [CrossRef]
- Larue, C.; Calzolari, C.; Bertinchant, J.P.; Leclercq, F.; Grolleau, R.; Pau, B. Cardiac-Specific Immunoenzymometric Assay of Troponin I in the Early Phase of Acute Myocardial Infarction. Clin. Chem. 1993, 39, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Jernberg, T.; Venge, P.; Lindahl, B. Comparison between Second and Third Generation Troponin T Assay in Patients with Symptoms Suggestive of an Acute Coronary Syndrome but without ST Segment Elevation. Cardiology 2003, 100, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, T. 510(k) Approval Letter for Elecsys Troponin T Stat Assay (K051752). U.S. Food and Drug Administration, Office of In Vitro Diagnostic Device Evaluation and Safety. 2005. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf5/K051752.pdf (accessed on 30 January 2024).
- Apple, F.S.; Collinson, P.O. Analytical Characteristics of High-Sensitivity Cardiac Troponin Assays. Clin. Chem. 2012, 58, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Kavsak, P.A.; Andruchow, J.E.; McRae, A.D.; Worster, A. Profile of Roche’s Elecsys Troponin T Gen 5 STAT Blood Test (a High-Sensitivity Cardiac Troponin Assay) for Diagnosing Myocardial Infarction in the Emergency Department. Expert Rev. Mol. Diagn. 2018, 18, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Saenger, A.K.; Beyrau, R.; Braun, S.; Cooray, R.; Dolci, A.; Freidank, H.; Giannitsis, E.; Gustafson, S.; Handy, B.; Katus, H.; et al. Multicenter Analytical Evaluation of a High-Sensitivity Troponin T Assay. Clin. Chim. Acta 2011, 412, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, Y.; Jaffe, A.S. Using High-Sensitivity Cardiac Troponin T for Acute Cardiac Care. Am. J. Med. 2017, 130, 1358–1365.e1. [Google Scholar] [CrossRef] [PubMed]
- Akwe, J.; Halford, B.; Kim, E.; Miller, A. A Review of Cardiac and Non-Cardiac Causes of Troponin Elevation and Clinical Relevance Part II: Non Cardiac Causes. J. Cardiol. Curr. Res. 2018, 11, 00364. [Google Scholar] [CrossRef]
- Wildi, K.; Twerenbold, R.; Mueller, C. How Acute Changes in Cardiac Troponin Concentrations Help to Handle the Challenges Posed by Troponin Elevations in Non-ACS-Patients. Clin. Biochem. 2015, 48, 218–222. [Google Scholar] [CrossRef]
- Zaki, H.A.; Shaban, A.E.; Shaban, A.E.; Shaban, E.E. Interpretation of Cardiac and Non-Cardiac Causes of Elevated Troponin T Levels in Non-Acute Coronary Syndrome Patients in the Emergency Department. Cureus 2022, 14, e22703. [Google Scholar] [CrossRef]
- Agewall, S.; Giannitsis, E.; Jernberg, T.; Katus, H. Troponin Elevation in Coronary vs. Non-Coronary Disease. Eur. Heart J. 2011, 32, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Brush, J.E.; Kaul, S.; Krumholz, H.M. Troponin Testing for Clinicians. J. Am. Coll. Cardiol. 2016, 68, 2365–2375. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.V.; Anand, A.; Sandoval, Y.; Lee, K.K.; Smith, S.W.; Adamson, P.D.; Chapman, A.R.; Langdon, T.; Sandeman, D.; Vaswani, A.; et al. High-Sensitivity Cardiac Troponin I at Presentation in Patients with Suspected Acute Coronary Syndrome: A Cohort Study. Lancet 2015, 386, 2481–2488. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.K.; Bularga, A.; O’Brien, R.; Ferry, A.V.; Doudesis, D.; Fujisawa, T.; Kelly, S.; Stewart, S.; Wereski, R.; Cranley, D.; et al. Troponin-Guided Coronary Computed Tomographic Angiography After Exclusion of Myocardial Infarction. J. Am. Coll. Cardiol. 2021, 78, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Collinson, P.O.; Heung, Y.M.; Gaze, D.; Boa, F.; Senior, R.; Christenson, R.; Apple, F.S. Influence of Population Selection on the 99th Percentile Reference Value for Cardiac Troponin Assays. Clin. Chem. 2012, 58, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Kimenai, D.M.; Shah, A.S.V.; McAllister, D.A.; Lee, K.K.; Tsanas, A.; Meex, S.J.R.; Porteous, D.J.; Hayward, C.; Campbell, A.; Sattar, N.; et al. Sex Differences in Cardiac Troponin I and T and the Prediction of Cardiovascular Events in the General Population. Clin. Chem. 2021, 67, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.V.; Griffiths, M.; Lee, K.K.; McAllister, D.A.; Hunter, A.L.; Ferry, A.V.; Cruikshank, A.; Reid, A.; Stoddart, M.; Strachan, F.; et al. High Sensitivity Cardiac Troponin and the Under-Diagnosis of Myocardial Infarction in Women: Prospective Cohort Study. BMJ 2015, 350, g7873. [Google Scholar] [CrossRef]
- Kimenai, D.M.; Lindahl, B.; Jernberg, T.; Bekers, O.; Meex, S.J.R.; Eggers, K.M. Sex-Specific Effects of Implementing a High-Sensitivity Troponin I Assay in Patients with Suspected Acute Coronary Syndrome: Results from SWEDEHEART Registry. Sci. Rep. 2020, 10, 15227. [Google Scholar] [CrossRef]
- Than, M.P.; Pickering, J.W.; Sandoval, Y.; Shah, A.S.V.; Tsanas, A.; Apple, F.S.; Blankenberg, S.; Cullen, L.; Mueller, C.; Neumann, J.T.; et al. Machine Learning to Predict the Likelihood of Acute Myocardial Infarction. Circulation 2019, 140, 899–909. [Google Scholar] [CrossRef]
- Doudesis, D.; Lee, K.K.; Yang, J.; Wereski, R.; Shah, A.S.V.; Tsanas, A.; Anand, A.; Pickering, J.W.; Than, M.P.; Mills, N.L.; et al. Validation of the Myocardial-Ischaemic-Injury-Index Machine Learning Algorithm to Guide the Diagnosis of Myocardial Infarction in a Heterogenous Population: A Prespecified Exploratory Analysis. Lancet Digit. Health 2022, 4, e300–e308. [Google Scholar] [CrossRef]
- Neumann, J.T.; Weimann, J.; Sörensen, N.A.; Hartikainen, T.S.; Haller, P.M.; Lehmacher, J.; Brocks, C.; Tenhaeff, S.; Karakas, M.; Renné, T.; et al. A Biomarker Model to Distinguish Types of Myocardial Infarction and Injury. J. Am. Coll. Cardiol. 2021, 78, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Yesudasu, V.; Pradhan, H.S.; Pandya, R.J. Recent Progress in Surface Plasmon Resonance Based Sensors: A Comprehensive Review. Heliyon 2021, 7, e06321. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Shokri Kojori, H.; Leblanc, R.M.; Kim, S.J. Ultrasensitive Plasmonic Biosensors for Real-Time Parallel Detection of Alpha-L-Fucosidase and Cardiac-Troponin-I in Whole Human Blood. Anal. Chem. 2018, 90, 7795–7799. [Google Scholar] [CrossRef]
- Xu, W.; Wang, L.; Zhang, R.; Sun, X.; Huang, L.; Su, H.; Wei, X.; Chen, C.-C.; Lou, J.; Dai, H.; et al. Diagnosis and Prognosis of Myocardial Infarction on a Plasmonic Chip. Nat. Commun. 2020, 11, 1654. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.; Biswal, S.; Titus, J.; Burman, A.; Reddy, K.; Fulwani, M.C.; Khan, A.; Deshpande, N.; Shrivastava, S.; Yanamala, N.; et al. A Novel Breakthrough in Wrist-Worn Transdermal Troponin-I-Sensor Assessment for Acute Myocardial Infarction. Eur. Heart J.-Digit. Health 2023, 4, ztad015. [Google Scholar] [CrossRef] [PubMed]
- Cairns, C.; Kang, K. National Hospital Ambulatory Medical Care Survey: 2020 Emergency Department Summary Tables. Cent. Dis. Control Prev. 2020. [Google Scholar] [CrossRef]
- Reichlin, T.; Hochholzer, W.; Bassetti, S.; Steuer, S.; Stelzig, C.; Hartwiger, S.; Biedert, S.; Schaub, N.; Buerge, C.; Potocki, M.; et al. Early Diagnosis of Myocardial Infarction with Sensitive Cardiac Troponin Assays. N. Engl. J. Med. 2009, 361, 858–867. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.T.; Twerenbold, R.; Ojeda, F.; Sörensen, N.A.; Chapman, A.R.; Shah, A.S.V.; Anand, A.; Boeddinghaus, J.; Nestelberger, T.; Badertscher, P.; et al. Application of High-Sensitivity Troponin in Suspected Myocardial Infarction. N. Engl. J. Med. 2019, 380, 2529–2540. [Google Scholar] [CrossRef]
- Ransohoff, D.F.; Feinstein, A.R. Problems of Spectrum and Bias in Evaluating the Efficacy of Diagnostic Tests. N. Engl. J. Med. 1978, 299, 926–930. [Google Scholar] [CrossRef]
- Lipinski, M.J.; Baker, N.C.; Escárcega, R.O.; Torguson, R.; Chen, F.; Aldous, S.J.; Christ, M.; Collinson, P.O.; Goodacre, S.W.; Mair, J.; et al. Comparison of Conventional and High-Sensitivity Troponin in Patients with Chest Pain: A Collaborative Meta-Analysis. Am. Heart J. 2015, 169, 6–16.e6. [Google Scholar] [CrossRef]
- Laguë, M.; Turgeon, P.Y.; Thériault, S.; Steinberg, C. A False-Positive Troponin Assay Leading to the Misdiagnosis of Myopericarditis. CMAJ 2022, 194, E456–E459. [Google Scholar] [CrossRef]
- Kavsak, P.A.; Roy, C.; Malinowski, P.; Mark, C.-T.; Scott, T.; Clark, L.; Lamers, S.; Ainsworth, C. Macrocomplexes and Discordant High-Sensitivity Cardiac Troponin Concentrations. Ann. Clin. Biochem. 2018, 55, 500–504. [Google Scholar] [CrossRef]
- Bolstad, N.; Warren, D.J.; Nustad, K. Heterophilic Antibody Interference in Immunometric Assays. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 647–661. [Google Scholar] [CrossRef]
- Herman, D.S.; Kavsak, P.A.; Greene, D.N. Variability and Error in Cardiac Troponin Testing: An ACLPS Critical Review. Am. J. Clin. Pathol. 2017, 148, 281–295. [Google Scholar] [CrossRef]
- Chaulin, A.M. False-Positive Causes in Serum Cardiac Troponin Levels. J. Clin. Med. Res. 2022, 14, 80–87. [Google Scholar] [CrossRef]
- Mair, J.; Lindahl, B.; Müller, C.; Giannitsis, E.; Huber, K.; Möckel, M.; Plebani, M.; Thygesen, K.; Jaffe, A.S. What to Do When You Question Cardiac Troponin Values. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 577–586. [Google Scholar] [CrossRef]
- Frame, I.J.; Joshi, P.H.; Mwangi, C.; Gunsolus, I.; De Lemos, J.A.; Das, S.R.; Sarode, R.; Balani, J.; Apple, F.S.; Muthukumar, A. Susceptibility of Cardiac Troponin Assays to Biotin Interference. Am. J. Clin. Pathol. 2019, 151, 486–493. [Google Scholar] [CrossRef]
- Lam, L.; Aspin, L.; Heron, R.C.; Ha, L.; Kyle, C. Discrepancy between Cardiac Troponin Assays Due to Endogenous Antibodies. Clin. Chem. 2020, 66, 445–454. [Google Scholar] [CrossRef]
- Graça Santos, L.; Ribeiro Carvalho, R.; Montenegro Sá, F.; Soares, F.; Pernencar, S.; Castro, R.; Morais, J. Circulating Heterophile Antibodies Causing Cardiac Troponin Elevation: An Unusual Differential Diagnosis of Myocardial Disease. JACC Case Rep. 2020, 2, 456–460. [Google Scholar] [CrossRef]
- Gore, M.O.; Seliger, S.L.; Defilippi, C.R.; Nambi, V.; Christenson, R.H.; Hashim, I.A.; Hoogeveen, R.C.; Ayers, C.R.; Sun, W.; McGuire, D.K.; et al. Age- and Sex-Dependent Upper Reference Limits for the High-Sensitivity Cardiac Troponin T Assay. J. Am. Coll. Cardiol. 2014, 63, 1441–1448. [Google Scholar] [CrossRef]
- Kalaria, T.R.; Harris, N.; Sensi, H.; Valentine, R.; Asif, U.; Sharrod-Cole, H.; Coley-Grant, D.; Min, S.S.; Ford, C.; Gama, R. High-Sensitivity Cardiac Troponin I: Is Ethnicity Relevant? J. Clin. Pathol. 2021, 74, 709–711. [Google Scholar] [CrossRef] [PubMed]
- Cullen, L.; Collinson, P.O.; Giannitsis, E. Point-of-Care Testing with High-Sensitivity Cardiac Troponin Assays: The Challenges and Opportunities. Emerg. Med. J. 2022, 39, 861–866. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| In a Population with a Larger Proportion of Disease | In a Population with a Smaller Proportion of Disease |
|---|---|
| Sensitivity = static! | Sensitivity = static! |
| Specificity = static! | Specificity = static! |
| PPV = increased | PPV = decreased |
| NPV = decreased | NPV = increased |
| LR+ = static! | LR+ = static! |
| LR− = static! | LR− = static! |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gokhan, I.; Dong, W.; Grubman, D.; Mezue, K.; Yang, D.; Wang, Y.; Gandhi, P.U.; Kwan, J.M.; Hu, J.-R. Clinical Biochemistry of Serum Troponin. Diagnostics 2024, 14, 378. https://doi.org/10.3390/diagnostics14040378
Gokhan I, Dong W, Grubman D, Mezue K, Yang D, Wang Y, Gandhi PU, Kwan JM, Hu J-R. Clinical Biochemistry of Serum Troponin. Diagnostics. 2024; 14(4):378. https://doi.org/10.3390/diagnostics14040378
Chicago/Turabian StyleGokhan, Ilhan, Weilai Dong, Daniel Grubman, Kenechukwu Mezue, David Yang, Yanting Wang, Parul U. Gandhi, Jennifer M. Kwan, and Jiun-Ruey Hu. 2024. "Clinical Biochemistry of Serum Troponin" Diagnostics 14, no. 4: 378. https://doi.org/10.3390/diagnostics14040378
APA StyleGokhan, I., Dong, W., Grubman, D., Mezue, K., Yang, D., Wang, Y., Gandhi, P. U., Kwan, J. M., & Hu, J. -R. (2024). Clinical Biochemistry of Serum Troponin. Diagnostics, 14(4), 378. https://doi.org/10.3390/diagnostics14040378