
Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Liver Steatosis Assessment
- (1)
- FLI: (FLI = (e0.953*loge(triglycerides)+0.139*BMI+0.718*loge (GGT)+0.053*WC−15.745)/(1 + e0.953*loge(triglycerides)+0.139*BMI+0.718*loge (GGT)+0.053*WC−15.745) × 100) [14];
- (2)
- HIS: (HSI = 8 × ALT/AST + BMI(+2 if type 2 DM present, +2 if female)) [15];
- (3)
- TyG: Ln [Tg (mg/dL) × fasting glucose (mg/dL)/2] [19];
- (4)
- TyG-BMI: (TyG index × BMI) [25];
- (5)
- TyG-WC (TyG index) × (waist circumference (cm)) [25].
2.3. Statistical Analysis
3. Results
3.1. Study Population
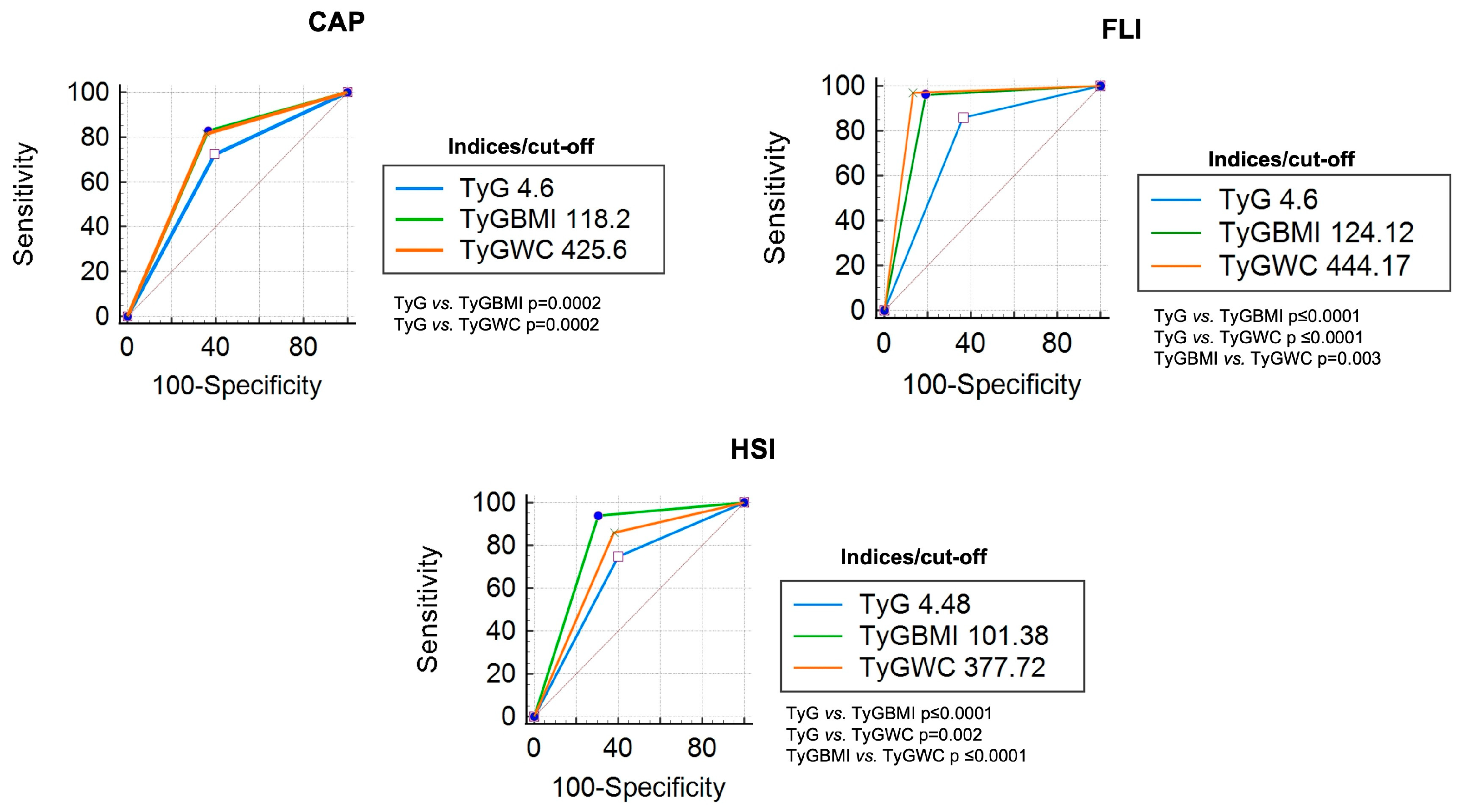
3.2. Diagnostic Accuracy of TyG Index, TyG-BMI Index, and TyG-WC Index
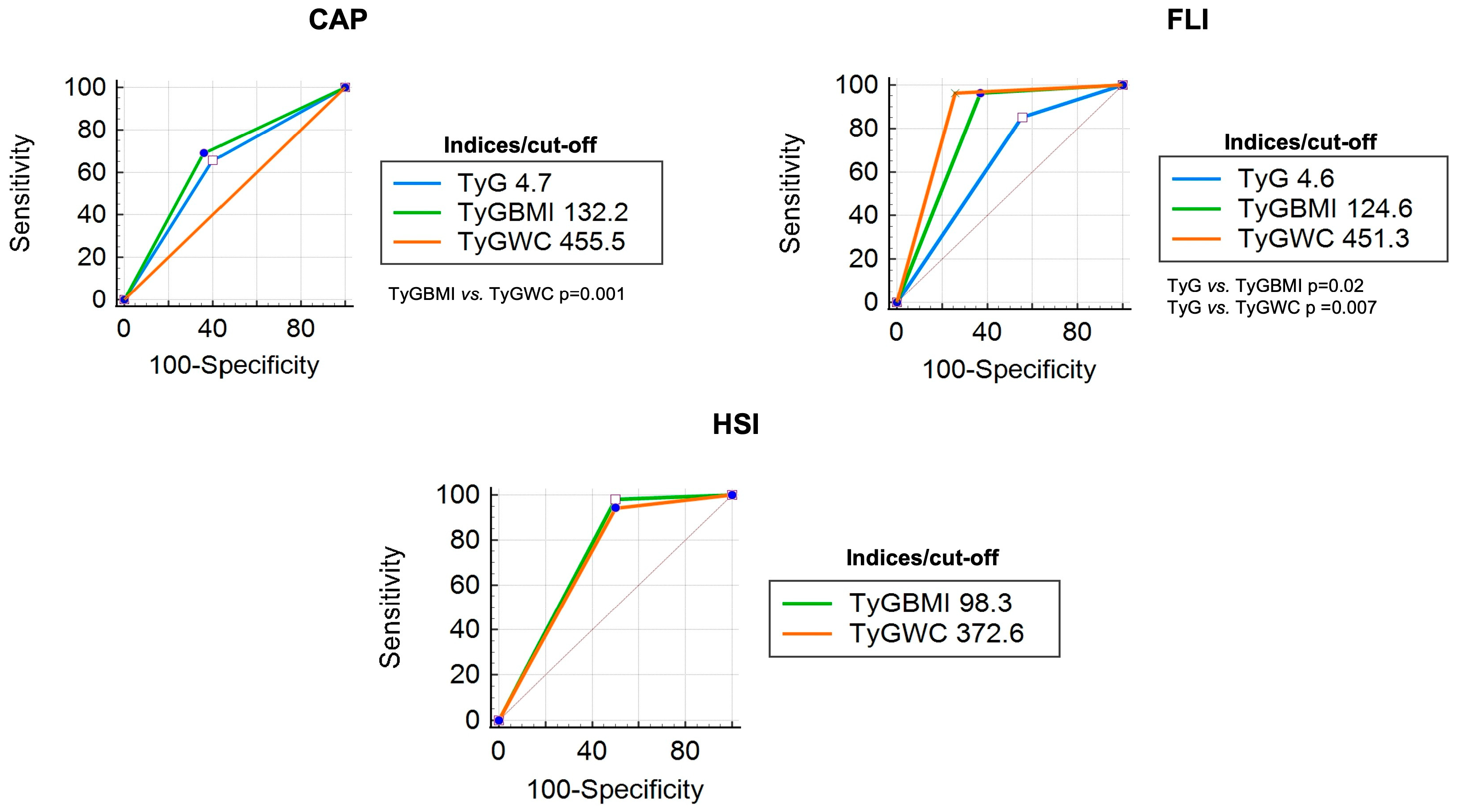
3.3. Diagnostic Accuracy of TyG Index, TyG-BMI Index, and TyG-WC Index in Patients with DM
3.4. Diagnostic Accuracy of TyG Index, TyG-BMI Index, and TyG-WC Index in Overweight/Obese Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A Multisociety Delphi Consensus Statement on New Fatty Liver Disease Nomenclature. J. Hepatol. 2023, 79, 1542–1556. [Google Scholar] [CrossRef]
- Khan, R.S.; Bril, F.; Cusi, K.; Newsome, P.N. Modulation of Insulin Resistance in Nonalcoholic Fatty Liver Disease. Hepatology 2019, 70, 711–724. [Google Scholar] [CrossRef] [PubMed]
- Tomizawa, M.; Kawanabe, Y.; Shinozaki, F.; Sato, S.; Motoyoshi, Y.; Sugiyama, T.; Yamamoto, S.; Sueishi, M. Triglyceride Is Strongly Associated with Nonalcoholic Fatty Liver Disease among Markers of Hyperlipidemia and Diabetes. Biomed. Rep. 2014, 2, 633–636. [Google Scholar] [CrossRef]
- Zhou, F.; Zhou, J.; Wang, W.; Zhang, X.J.; Ji, Y.X.; Zhang, P.; She, Z.G.; Zhu, L.; Cai, J.; Li, H. Unexpected Rapid Increase in the Burden of NAFLD in China From 2008 to 2018: A Systematic Review and Meta-Analysis. Hepatology 2019, 70, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Zhang, X.; Li, G.; Wong, G.L.H.; Wong, V.W.S. Epidemiology and Clinical Outcomes of Metabolic (Dysfunction)-Associated Fatty Liver Disease. J. Clin. Transl. Hepatol. 2021, 9, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The Diagnosis and Management of Non-Alcoholic Fatty Liver Disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease—Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Powell, E.E.; Wong, V.W.S.; Rinella, M. Non-Alcoholic Fatty Liver Disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- Pal, S.C.; Méndez-Sánchez, N. Screening for MAFLD: Who, When and How? Ther. Adv. Endocrinol. Metab. 2023, 14, 20420188221145650. [Google Scholar] [CrossRef]
- Graffigna, M.; Catoira, N.; Soutelo, J.; Azpelicueta, A.; Berg, G.; Perel, C.; Migliano, M.E.; Aranguren, M.; Musso, C.; Farias, J. Diagnóstico de Esteatosis Hepática Por Métodos Clínicos, Bioquímicos y Por Imágenes. Rev. Argent. Endocrinol. Metab. 2017, 54, 37–46. [Google Scholar] [CrossRef]
- Pu, K.; Wang, Y.; Bai, S.; Wei, H.; Zhou, Y.; Fan, J.; Qiao, L. Diagnostic Accuracy of Controlled Attenuation Parameter (CAP) as a Non-Invasive Test for Steatosis in Suspected Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. BMC Gastroenterol. 2019, 19, 51. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Cuevas, J.; Santos, A.; Armendariz-Borunda, J. Pathophysiological Molecular Mechanisms of Obesity: A Link between MAFLD and NASH with Cardiovascular Diseases. Int. J. Mol. Sci. 2021, 22, 11629. [Google Scholar] [CrossRef] [PubMed]
- Pipitone, R.M.; Ciccioli, C.; Infantino, G.; La Mantia, C.; Parisi, S.; Tulone, A.; Pennisi, G.; Grimaudo, S.; Petta, S. MAFLD: A Multisystem Disease. Ther. Adv. Endocrinol. Metab. 2023, 14, 20420188221145549. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A Simple and Accurate Predictor of Hepatic Steatosis in the General Population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic Steatosis Index: A Simple Screening Tool Reflecting Nonalcoholic Fatty Liver Disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V. Performance and Limitations of Steatosis Biomarkers in Patients with Nonalcoholic Fatty Liver Disease. Aliment. Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Du, T.; Zhang, J.; Lu, H.; Lin, X.; Xie, J.; Yang, Y.; Yu, X. The Triglyceride and Glucose Index (TyG) Is an Effective Biomarker to Identify Nonalcoholic Fatty Liver Disease. Lipids Health Dis. 2017, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Romero, F.; Simental-Mendía, L.E.; González-Ortiz, M.; Martínez-Abundis, E.; Ramos-Zavala, M.G.; Hernández-González, S.O.; Jacques-Camarena, O.; Rodríguez-Morán, M. The Product of Triglycerides and Glucose, a Simple Measure of Insulin Sensitivity. Comparison with the Euglycemic-Hyperinsulinemic Clamp. J. Clin. Endocrinol. Metab. 2010, 95, 3347–3351. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendía, L.E.; Rodríguez-Morán, M.; Guerrero-Romero, F. The Product of Fasting Glucose and Triglycerides as Surrogate for Identifying Insulin Resistance in Apparently Healthy Subjects. Metab. Syndr. Relat. Disord. 2008, 6, 299–304. [Google Scholar] [CrossRef]
- Wang, J.; Yan, S.; Cui, Y.; Chen, F.; Piao, M.; Cui, W. The Diagnostic and Prognostic Value of the Triglyceride-Glucose Index in Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD): A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4969. [Google Scholar] [CrossRef]
- Zheng, S.; Shi, S.; Ren, X.; Han, T.; Li, Y.; Chen, Y.; Liu, W.; Hou, P.C.; Hu, Y. Triglyceride Glucose-Waist Circumference, a Novel and Effective Predictor of Diabetes in First-Degree Relatives of Type 2 Diabetes Patients: Cross-Sectional and Prospective Cohort Study. J. Transl. Med. 2016, 14, 260. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Cho, Y.K.; Kim, E.H.; Lee, M.J.; Jung, C.H.; Park, J.Y.; Kim, H.K.; Lee, W.J. Triglyceride Glucose-Waist Circumference Is Superior to the Homeostasis Model Assessment of Insulin Resistance in Identifying Nonalcoholic Fatty Liver Disease in Healthy Subjects. J. Clin. Med. 2021, 11, 41. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Xu, J.; Li, M.; Gao, Y. Potential Screening Indicators for Early Diagnosis of NAFLD/MAFLD and Liver Fibrosis: Triglyceride Glucose Index-Related Parameters. Front. Endocrinol. 2022, 13, 951689. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.T.; Xiang, L.L.; Qi, F.; Zhang, Y.J.; Chen, Y.; Zhou, X.Q. Accuracy of Controlled Attenuation Parameter (CAP) and Liver Stiffness Measurement (LSM) for Assessing Steatosis and Fibrosis in Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. EClinicalMedicine 2022, 51, 101547. [Google Scholar] [CrossRef] [PubMed]
- Khamseh, M.E.; Malek, M.; Abbasi, R.; Taheri, H.; Lahouti, M.; Alaei-Shahmiri, F. Triglyceride Glucose Index and Related Parameters (Triglyceride Glucose-Body Mass Index and Triglyceride Glucose-Waist Circumference) Identify Nonalcoholic Fatty Liver and Liver Fibrosis in Individuals with Overweight/Obesity. Metab. Syndr. Relat. Disord. 2021, 19, 167–173. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Kitae, A.; Hashimoto, Y.; Hamaguchi, M.; Obora, A.; Kojima, T.; Fukui, M. The Triglyceride and Glucose Index Is a Predictor of Incident Nonalcoholic Fatty Liver Disease: A Population-Based Cohort Study. Can. J. Gastroenterol. Hepatol. 2019, 2019, 5121574. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.; Shao, Z.; Shen, G. Association between Triglyceride Glucose-Related Markers and the Risk of Metabolic-Associated Fatty Liver Disease: A Cross-Sectional Study in Healthy Chinese Participants. BMJ Open 2023, 13, e070189. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Chang, M.; Shen, P.; Wei, W.; Li, H.; Shen, G. Application Value of Triglyceride-Glucose Index and Triglyceride-Glucose Body Mass Index in Evaluating the Degree of Hepatic Steatosis in Non-Alcoholic Fatty Liver Disease. Lipids Health Dis. 2023, 22, 186. [Google Scholar] [CrossRef]
- Li, N.; Tan, H.; Xie, A.; Li, C.; Fu, X.; Xang, W.; Kirim, A.; Huang, X. Value of the Triglyceride Glucose Index Combined with Body Mass Index in Identifying Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes. BMC Endocr. Disord. 2022, 22, 101. [Google Scholar] [CrossRef]
- Lim, J.; Kim, J.; Koo, S.H.; Kwon, G.C. Comparison of Triglyceride Glucose Index, and Related Parameters to Predict Insulin Resistance in Korean Adults: An Analysis of the 2007–2010 Korean National Health and Nutrition Examination Survey. PLoS ONE 2019, 14, e0212963. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Son, D.H.; Baik, S.J.; Cho, W.J.; Lee, Y.J. Triglyceride Glucose-Waist Circumference (TyG-WC) Is a Reliable Marker to Predict Non-Alcoholic Fatty Liver Disease. Biomedicines 2022, 10, 2251. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Feng, L.; Ding, J.; Zhou, W.; Yuan, T.; Mao, J. Triglyceride Glucose-Waist Circumference: The Optimum Index to Screen Nonalcoholic Fatty Liver Disease in Non-Obese Adults. BMC Gastroenterol. 2023, 23, 376. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Huang, X.; Qian, Y.; Sun, T. A Non-Linear Relationship between Triglyceride Glucose Waist Circumference and Nonalcoholic Fatty Liver Disease in a Japanese Population: A Secondary Analysis. Front. Endocrinol. 2023, 14, 1188214. [Google Scholar] [CrossRef] [PubMed]
- Castera, L.; Yuen Chan, H.L.; Arrese, M.; Afdhal, N.; Bedossa, P.; Friedrich-Rust, M.; Han, K.H.; Pinzani, M. EASL-ALEH Clinical Practice Guidelines: Non-Invasive Tests for Evaluation of Liver Disease Severity and Prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar]
- Lim, J.K.; Flamm, S.L.; Singh, S.; Falck-Ytter, Y.T.; Gerson, L.; Hirano, I.; Nguyen, G.C.; Rubenstein, J.H.; Smalley, W.E.; Stollman, N.; et al. American Gastroenterological Association Institute Guideline on the Role of Elastography in the Evaluation of Liver Fibrosis. Gastroenterology 2017, 152, 1536–1543. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | General (n = 855) | DM (n = 54) | Overweight/Obesity (n = 505) |
|---|---|---|---|
| %(n)/M [IQR] | %(n)/M [IQR] | %(n)/M [IQR] | |
| Male | 61.1 (522) | 63 (34) | 69.1 (349) |
| Age (years) | 48 (44–54) | 54 (49–61) | 49 (44–54) |
| BMI (kg/m2) | 25.7 [23.4–28.1] | 27.6 [25.3–30.9] | 27.5 [26.1–29.7] |
| DM | 6.3 (54) | - | 8.9 (45) |
| Hypertension | 35.1 (300) | 48.1 (26) | 44 (222) |
| Dyslipidemia | 38.7 (331) | 26.9 (16) | 39.2 (198) |
| Smoking | 20 (171) | 16.7 (1) | 21 (106) |
| WC (cm) | 92 (85–98) | 98 (91–106) | 97 (92–103) |
| Fasting glucose (mg/dL) | 90 (85–96) | 111.5 (91–136) | 91 (87–98) |
| Triglycerides (mg/dL) | 112 (80–159) | 116 [90.5–173.2] | 126 [94.5–181.5] |
| Cholesterol (mg/dL) | 208 (180–235) | 194.5 (157–225) | 208 (179–234) |
| HDL (mg/dL) | 53 (42–74) | 46.5 (41–81) | 49 (39–68) |
| LDL (mg/dL) | 131 (107–157) | 115 [88.7–144.7] | 131 (109–155) |
| HbA1c (%) | 5.3 [5.1–5.5] | 6.3 [5.5–7.3] | 5.4 [5.2–5.7] |
| AST (IU/L) | 26 (20–35) | 25 (21–38) | 28 (22–40) |
| ALT (IU/L) | 23 (20–28) | 24 (19–29) | 24 (21–30) |
| GGT (IU/L) | 21 (15–30) | 21 (14–32) | 24 (18–33) |
| dB | 243 (213–282) | 272 (243–309) | 264 (238–302) |
| kPa | 3.9 [3.3–4.6] | 4.2 [3.6–4.7] | 4.1 [3.4–4.6] |
| LS by CAP | 31.8 (272) | 53.7 (29) | 46.3 (234) |
| FLI | 37 (18–62) | 59.5 [28.7–79.5] | 55 (37–76) |
| LS by FLI | 27.4 (234) | 50 (27) | 45.1 (228) |
| HSI | 40 (43–47) | 42.4 [39.8–46.8] | 43 [40.5–46] |
| LS by HSI | 82.8 (708) | 96.3 (52) | 98.6 (498) |
| TyG | 4.6 [4.4–4.8] | 4.7 [4.5–5.03] | 4.6 [4.5–4.8] |
| TyG-BMI | 118.5 [106.1–133.5] | 133.8 [119.7–154.2] | 129.9 [12.5–142.5] |
| TyG-WC | 425.9 [384.6–467.8] | 470.3 [427.4–508.7] | 453.2 [424–495.3] |
| Index | Cut-Off | AUC | Sensitivity (CI 95%) | Specificity (CI 95%) | PPV | NPV | LR+ (CI 95%) | LR− (CI 95%) |
|---|---|---|---|---|---|---|---|---|
| CAP | ||||||||
| TyG | 4.61 | 0.72 | 0.72 (0.67–0.77) | 0.60 (0.54–0.66) | 0.46 | 0.82 | 1.83 (1.61–2.07) | 0.46 (0.37–0.56) |
| TyG-BMI | 118.2 | 0.82 | 0.82 (0.77–0.87) | 0.63 (0.57–0.69) | 0.51 | 0.88 | 2.26 (2.01–2.55) | 0.27 (0.21–0.36) |
| TyG-WC | 425.6 | 0.81 | 0.81 (0.76–0.86) | 0.64 (0.58–0.70) | 0.51 | 0.88 | 2.29 (2.02–2.59) | 0.29 (0.22–0.37) |
| FLI | ||||||||
| TyG | 4.6 | 0.84 | 0.85 (0.80–0.90) | 0.63 (0.57–0.69) | 0.46 | 0.92 | 2.35 (2.09–2.64) | 0.22 (0.16–0.31) |
| TyG-BMI | 124.12 | 0.96 | 0.96 (0.93–0.99) | 0.80 (0.75–0.85) | 0.65 | 0.98 | 5.02 (4.26–5.91) | 0.05 (0.03–0.09) |
| TyG-WC | 444.17 | 0.96 | 0.97 (0.95–0.99) | 0.86 (0.82–0.90) | 0.73 | 0.98 | 7.26 (5.93–8.88) | 0.03 (0.02–0.07) |
| HSI | ||||||||
| TyG | 4.4 | 0.74 | 0.74 (0.71–0.77) | 0.59 (0.55–0.63) | 0.89 | 0.33 | 1.87 (1.52–2.28) | 0.42 (0.35–0.50) |
| TyG-BMI | 101.38 | 0.93 | 0.93 (0.91–0.95) | 0.69 (0.66–0.72) | 0.93 | 0.70 | 3.07 (2.40–3.92) | 0.09 (0.06–0.12) |
| TyG-WC | 377.7 | 0.85 | 0.85 (0.82–0.88) | 0.61 (0.57–0.65) | 0.91 | 0.47 | 2.25 (1.83–2.78) | 0.23 (0.18–0.28) |
| Index | Cut-Off | AUC | Sensitivity (CI 95%) | Specificity (CI 95%) | PPV | NPV | LR+ (CI 95%) | LR− (CI 95%) |
|---|---|---|---|---|---|---|---|---|
| CAP | ||||||||
| TyG | 4.7 | 0.634 | 0.65 (0.48–0.82) | 0.60 (0.42–0.78) | 0.34 | 0.40 | 1.64 (0.95–2.83) | 0.57 (0.32–1.04) |
| TyG-BMI | 132.2 | 0.683 | 0.69 (0.52–0.86) | 0.36 (0.19–0.53) | 0.44 | 0.50 | 1.08 (0.75–1.58) | 0.86 (0.41–1.83) |
| TyG-WC | 455.5 | 0.708 | 0.72 (0.56–0.88) | 0.60 (0.42–0.78) | 0.32 | 0.34 | 1.81 (1.07–3.08) | 0.46 (0.24–0.90) |
| FLI | ||||||||
| TyG | 4.6 | 0.771 | 0.85 (0.72–0.98) | 0.44 (0.25–0.63) | 0.39 | 0.25 | 1.53 (1.06–2.22) | 0.33 (0.12–0.90) |
| TyG-BMI | 124.6 | 0.975 | 0.96 (0.89–1.03) | 0.63 (0.45–0.81) | 0.27 | 0.05 | 2.60 (1.58–4.28) | 0.06 (0.01–0.41) |
| TyG-WC | 451.3 | 0.966 | 0.96 (0.89–1.03) | 0.74 (0.57–0.91) | 0.21 | 0.04 | 3.71 (1.95–7.96) | 0.05 (0.01–0.35) |
| HSI | ||||||||
| TyG | - | - | - | - | - | - | - | - |
| TyG-BMI | 98.3 | 0.990 | 0.98 (0.94–1.02) | 0.50 (0.36–0.64) | 0.01 | 0.05 | 1.96 (0.49–7.85) | 0.04 (0.0–0.42) |
| TyG-WC | 372.6 | 0.952 | 0.94 (0.88–1.00) | 0.50 (0.36–0.64) | 0.02 | 0.75 | 1.88 (0.47–7.55) | 0.12 (0.02–0.68) |
| Index | Cut-Off | AUC | Sensitivity (CI 95%) | Specificity (CI 95%) | PPV | NPV | LR+ (CI 95%) | LR− (CI 95%) |
|---|---|---|---|---|---|---|---|---|
| CAP | ||||||||
| TyG | 4.6 | 0.674 | 0.74 (0.68–0.80) | 0.50 (0.44–0.56) | 0.43 | 0.30 | 1.49 (1.30–1.72) | 0.51 (0.40–0.65) |
| TyG-BMI | 128.1 | 0.756 | 0.76 (0.71–0.81) | 0.62 (0.56–0.68) | 0.36 | 0.24 | 2.02 (1.71–2.39) | 0.38 (0.30–0.49) |
| TyG-WC | 446.3 | 0.740 | 0.74 (0.68–0.80) | 0.60 (0.54–0.66) | 0.37 | 0.26 | 1.90 (1.61–2.25) | 0.42 (0.33–0.53) |
| FLI | ||||||||
| TyG | 4.6 | 0.827 | 0.85 (0.80–0.90) | 0.58 (0.52–0.64) | 0.36 | 0.16 | 2.08 (1.79–2.42) | 0.25 (0.18–0.34) |
| TyG-BMI | 127.8 | 0.929 | 0.93 (0.90–0.96) | 0.73 (0.67–0.79) | 0.25 | 0.06 | 3.54 (2.90–4.33) | 0.09 (0.05–0.15) |
| TyG-WC | 446.3 | 0.950 | 0.95 (0.92–0.98) | 0.77 (0.72–0.82) | 0.22 | 0.04 | 4.18 (3.36–5.21) | 0.06 (0.03–0.11) |
| HSI | ||||||||
| TyG | 4.5 | 0.695 | 0.76 (0.72–0.80) | 0.42 (0.38–0.46) | 0.01 | 0.97 | 1.34 (0.71–2.55) | 0.54 (0.23–1.30) |
| TyG-BMI | 115.6 | 0.884 | 0.88 (0.85–0.91) | 0.57 (0.53–0.61) | 0.006 | 0.93 | 2.07 (0.88–4.86) | 0.20 (0.10–0.40) |
| TyG-WC | - | - | - | - | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mijangos-Trejo, A.; Gómez-Mendoza, R.; Ramos-Ostos, M.H.; Castro-Narro, G.; Uribe, M.; Juárez-Hernández, E.; López-Méndez, I. Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection. Diagnostics 2024, 14, 762. https://doi.org/10.3390/diagnostics14070762
Mijangos-Trejo A, Gómez-Mendoza R, Ramos-Ostos MH, Castro-Narro G, Uribe M, Juárez-Hernández E, López-Méndez I. Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection. Diagnostics. 2024; 14(7):762. https://doi.org/10.3390/diagnostics14070762
Chicago/Turabian StyleMijangos-Trejo, Alejandra, Raúl Gómez-Mendoza, Martha Helena Ramos-Ostos, Graciela Castro-Narro, Misael Uribe, Eva Juárez-Hernández, and Iván López-Méndez. 2024. "Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection" Diagnostics 14, no. 7: 762. https://doi.org/10.3390/diagnostics14070762
APA StyleMijangos-Trejo, A., Gómez-Mendoza, R., Ramos-Ostos, M. H., Castro-Narro, G., Uribe, M., Juárez-Hernández, E., & López-Méndez, I. (2024). Diagnostic Accuracy of the Triglyceride–Glucose Index (TyG), TyG Body Mass Index, and TyG Waist Circumference Index for Liver Steatosis Detection. Diagnostics, 14(7), 762. https://doi.org/10.3390/diagnostics14070762