
Comprehensive Oral Diagnosis and Management for Women with Turner Syndrome

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Dental Conditions Recorded
2.3. Statistical Analysis
3. Results
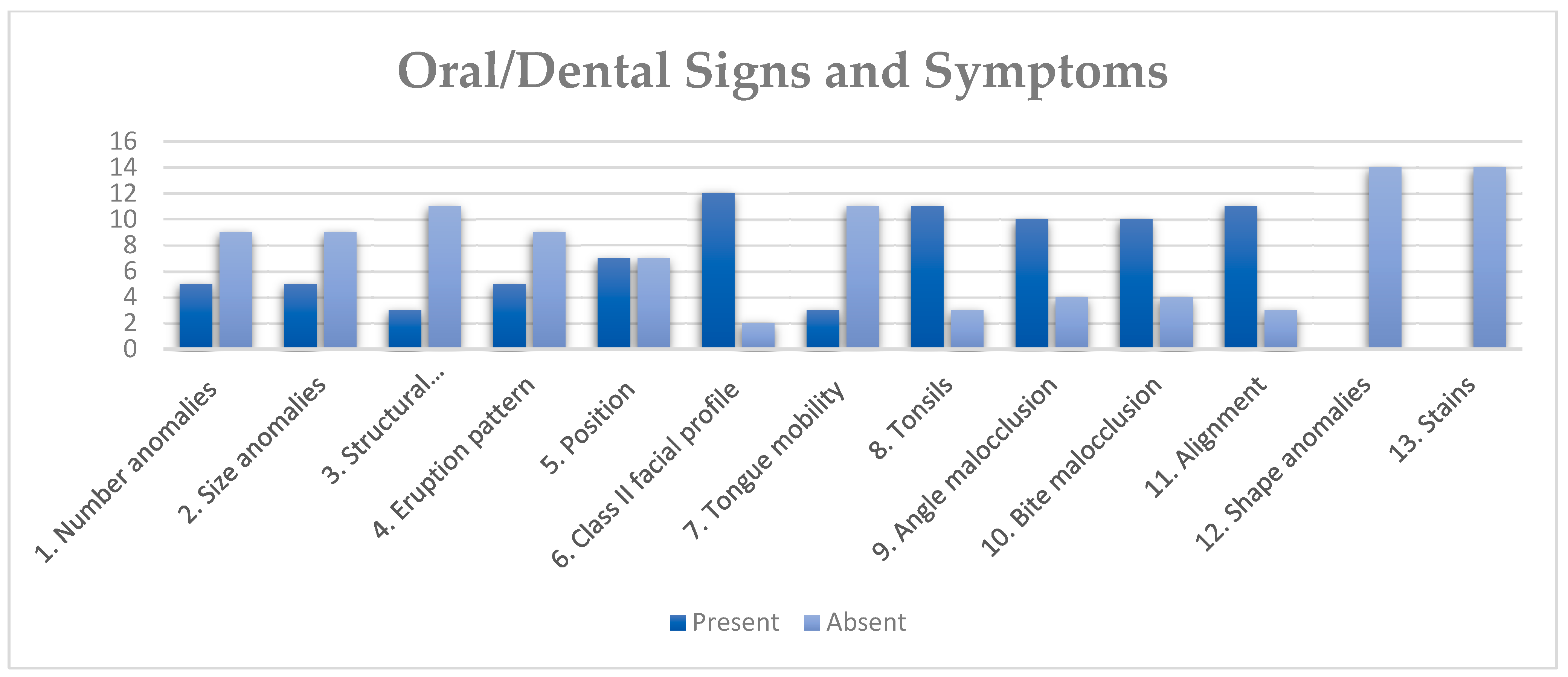
3.1. Clinical Findings
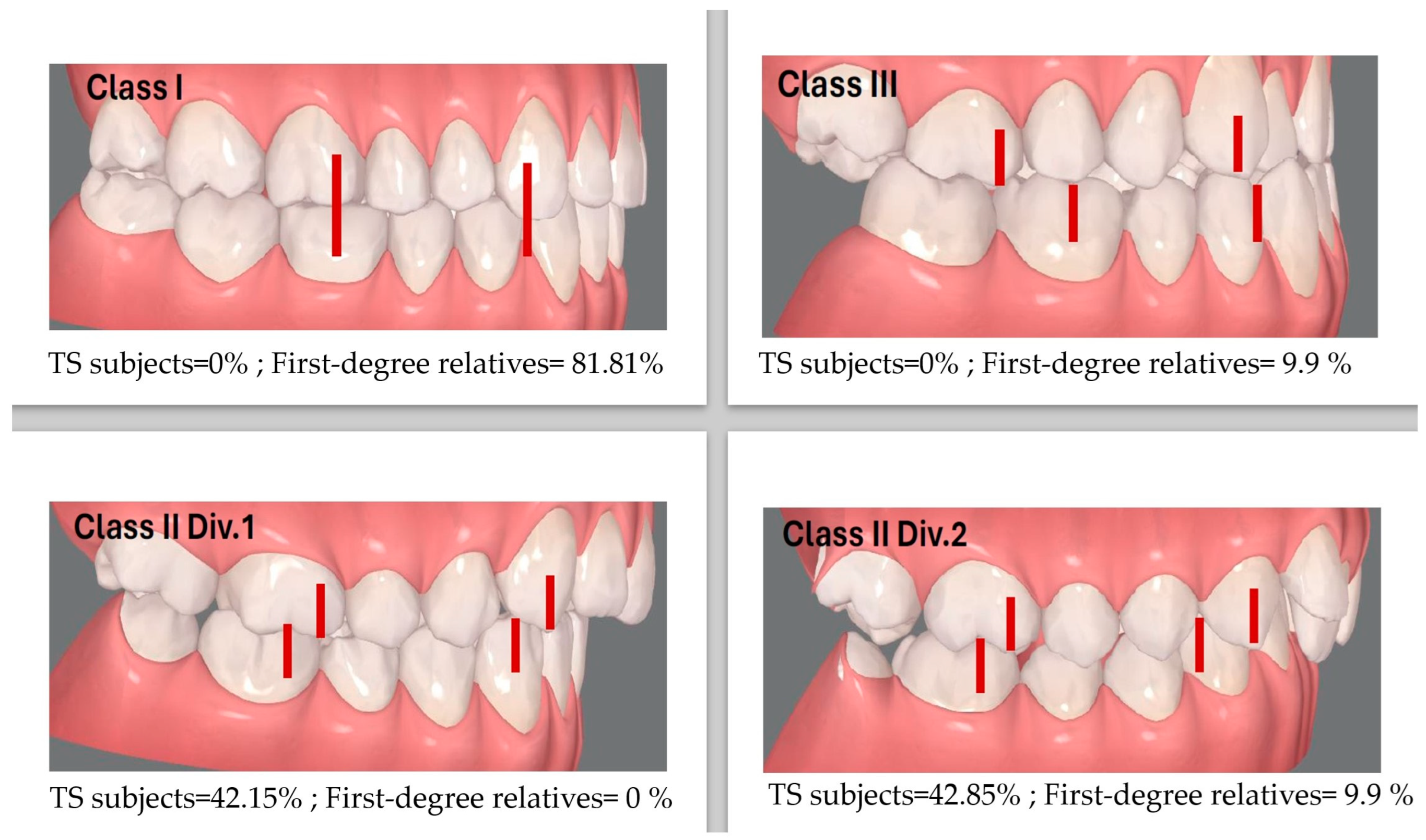
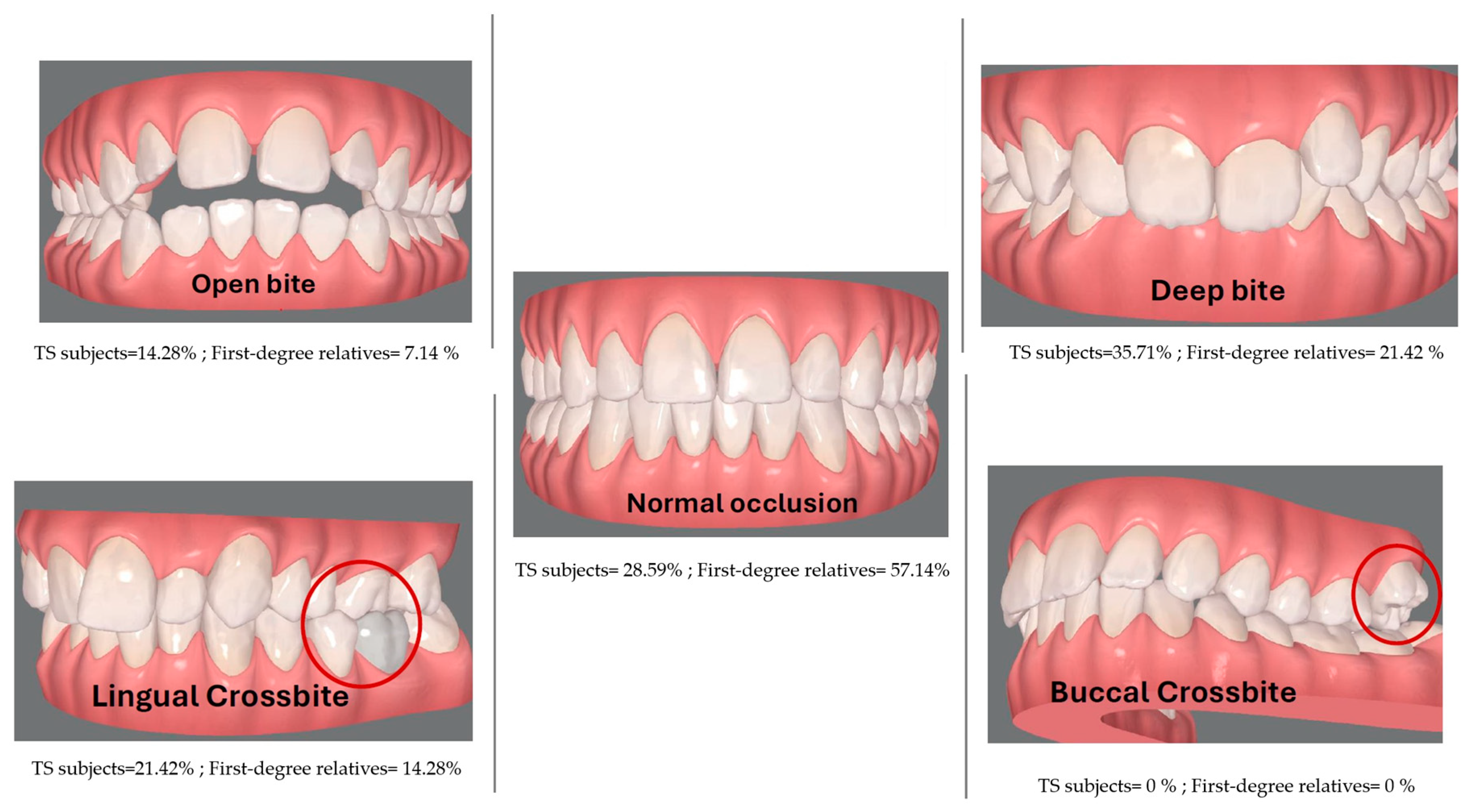
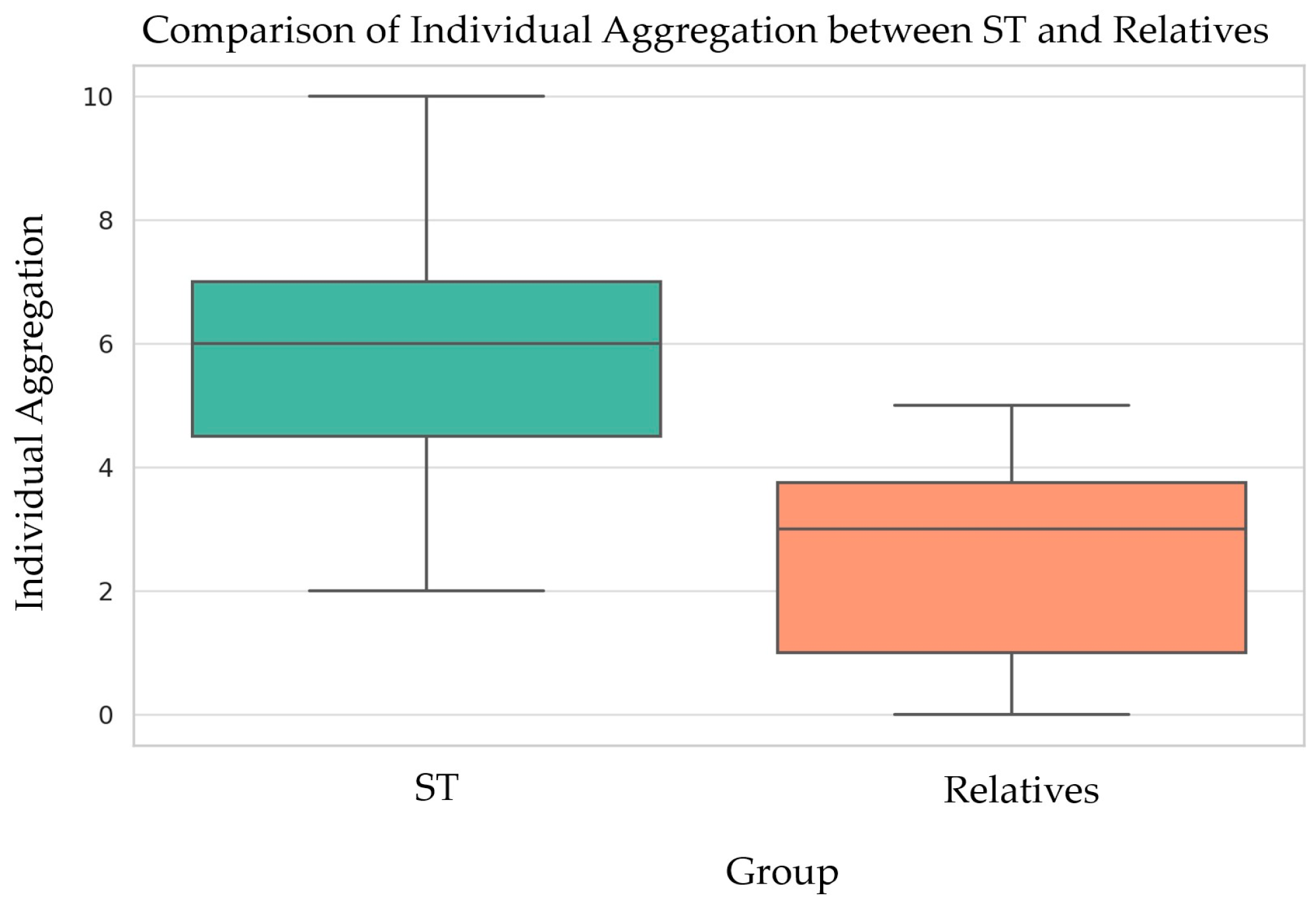
3.2. Dento-Craniofacial Findings
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nielsen, J.; Wohlert, M. Chromosome abnormalities found among 34,910 newborn children: Results from a 13-year incidence study in Arhus, Denmark. Hum. Genet. 1991, 87, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Gardner, R.J.M.; Amor, D.J. Gardner and Sutherland’s Chromosome Abnormalities and Genetic Counseling, 5th ed.; Oxford University Press: Oxford, UK, 2018; pp. 1–7. [Google Scholar]
- Berglund, A.; Stochholm, K.; Gravholt, C.H. The epidemiology of sex chromosome abnormalities. Am. J. Med. Genet. Part C Semin. Med. Genet. 2020, 184, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Brun, J.L.; Gangbo, F.; Wen, Z.Q.; Galant, K.; Taine, L.; Maugey-Laulom, B.; Roux, D.; Mangione, R.; Horovitz, J.; Saura, R. Prenatal diagnosis and management of sex chromosome aneuploidy: A report on 98 cases. Prenat. Diagn. 2004, 24, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Gunther, D.F.; Eugster, E.; Zagar, A.J.; Bryant, C.G.; Davenport, M.L.; Quigley, C.A. Ascertainment Bias in Turner Syndrome: New Insights From Girls Who Were Diagnosed Incidentally in Prenatal Life. Pediatrics 2004, 114, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Stochholm, K.; Juul, S.; Juel, K.; Naeraa, R.W.; Gravholt, C.H. Prevalence, Incidence, Diagnostic Delay, and Mortality in Turner Syndrome. J. Clin. Endocrinol. Metab. 2006, 91, 3897–3902. [Google Scholar] [CrossRef] [PubMed]
- Berglund, A.; Viuff, M.H.; Skakkebæk, A.; Chang, S.; Stochholm, K.; Gravholt, C.H. Changes in the cohort composition of turner syndrome and severe non-diagnosis of Klinefelter, 47,XXX and 47,XYY syndrome: A nationwide cohort study. Orphanet J. Rare Dis. 2019, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Gravholt, C.H.; Andersen, N.H.; Conway, G.S.; Dekkers, O.M.; Geffner, M.E.; Klein, K.O.; Lin, A.E.; Mauras, N.; Quigley, C.A.; Rubin, K.; et al. Clinical practice guidelines for the care of girls and women with Turner syndrome: Proceedings from the 2016 Cincinnati International Turner Syndrome Meeting. Eur. J. Endocrinol. 2017, 177, G1–G70. [Google Scholar] [CrossRef]
- Gravholt, C.H.; Viuff, M.; Just, J.; Sandahl, K.; Brun, S.; Van Der Velden, J.; Andersen, N.H.; Skakkebaek, A. The Changing Face of Turner Syndrome. Endocr. Rev. 2023, 44, 33–69. [Google Scholar] [CrossRef]
- Frelich, J.; Irzyniec, T.; Lepska, K.; Jeż, W. New insights into clinical features, karyotypes, and age at diagnosis in women with Turner syndrome. Endokrynol. Pol. 2019, 70, 342–349. [Google Scholar] [CrossRef]
- Witkowska-Krawczak, E.; Erazmus, M.; Majcher, A.; Pyrżak, B.; Kucharska, A.M. Predicted health care profile after transition to adult care in Turner syndrome children—Experience of single center. Front. Pediatr. 2023, 11, 1173419. [Google Scholar] [CrossRef]
- Lin, A.E.; Prakash, S.K.; Andersen, N.H.; Viuff, M.H.; Levitsky, L.L.; Rivera-Davila, M.; Crenshaw, M.L.; Hansen, L.; Colvin, M.K.; Hayes, F.J.; et al. Recognition and management of adults with Turner syndrome: From the transition of adolescence through the senior years. Am. J. Med. Genet. 2019, 179, 1987–2033. [Google Scholar] [CrossRef] [PubMed]
- Bagattoni, S.; Lardani, L.; Vanni, A.; Costi, T. Craniofacial and occlusal features of individuals with Turner Syndrome: A cephalometric study. J. Biol. Regul. Homeost. Agents. 2021, 35, 95–106. [Google Scholar] [PubMed]
- Svanberg, C.; Norevall, L.I.; Ekman, B.; Wahlberg, J.; Bågesund, M. Cephalometric analysis of adults with Turner syndrome. Swed. Dent. J. 2016, 40, 33–41. [Google Scholar] [PubMed]
- Cazzolla, A.P.; Lo Muzio, L.; Di Fede, O.; Lacarbonara, V.; Colaprico, A.; Testa, N.F.; Giuseppe, T.; Zhurakivska, K.; Marzo, G.; Lacaita, M.G. Orthopedic-orthodontic treatment of the subject with Turner’s syndrome: Review of the literature and case report. Spec. Care Dentist. 2018, 38, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Juloski, J.; Dumančić, J.; Šćepan, I.; Lauc, T.; Milašin, J.; Kaić, Z.; Dumić, M.; Babić, M. Growth hormone positive effects on craniofacial complex in Turner syndrome. Arch. Oral Biol. 2016, 71, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Wójcik, D.; Beń-Skowronek, I. Craniofacial Morphology in Children with Growth Hormone Deficiency and Turner Syndrome. Diagnostics 2020, 10, 88. [Google Scholar] [CrossRef]
- Redhead, Y.; Gibbins, D.; Lana-Elola, E.; Watson-Scales, S.; Dobson, L.; Krause, M.; Liu, K.J.; Fisher, E.M.C.; Green, J.B.A.; Tbulewicz, V.L.J. Craniofacial dysmorphology in Down syndrome is caused by increased dosage of Dyrk1a and at least three other genes. Development. 2023, 150, dev201077. [Google Scholar] [CrossRef]
- Morice, A.; Taverne, M.; Eché, S.; Griffon, L.; Fauroux, B.; Leboulanger, N.; Couloigner, V.; Baujat, G.; Cormier-Daire, V.; Picard, A.; et al. Craniofacial growth and function in achondroplasia: A multimodal 3D study on 15 subjects. Orphanet J. Rare Dis. 2023, 18, 88. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.L.; Li, F.; Chen, W.; Liu, L.; Cheng, H.J.; He, Z.X.; Ai, R. “Liu-Liang-Chung” syndrome with multiple congenital anomalies and the distinctive craniofacial features caused by dominant ZEB2 gene gain mutation. BMC Pediatr. 2023, 23, 480. [Google Scholar] [CrossRef]
- Dumancic, J.; Kaic, Z.; Varga, M.L.; Lauc, T.; Dumic, M.; Milosevic, S.A.; Brkic, H. Characteristics of the craniofacial complex in Turner syndrome. Arch. Oral Biol. 2010, 55, 81–88. [Google Scholar] [CrossRef]
- Perkiomaki, M.R.; Kyrkanides, S.; Niinimaa, A.; Alvesalo, L. The relationship of distinct craniofacial features between Turner syndrome females and their parents. Eur. J. Orthod. 2005, 27, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Kusiak, A.; Sadlak, N.J.; Limon, J.; Kochanska, B. Root morphology of mandibular premolars in 40 subjects with Turner syndrome. Int. Endod. J. 2005, 38, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Townsend, G.; Jensen, B.L.; Alvesalo, L. Reduced tooth size in 45,X (Turner syndrome) females. Am. J. Phys. Anthropol. 1984, 65, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Maier, C.; Dumančić, J.; Brkić, H.; Kaić, Z.; Savić Pavičin, I.; Poje, Z.; Scott, G.R. Tooth Crown Morphology in Turner and Klinefelter Syndrome Individuals from a Croatian Sample. Acta Stomatol. Croat. 2019, 53, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Durán Von Arx, J.; Merino Arends, M.; Echarri, P.; Carrasco, P. Tabla de diagnóstico y tratamiento Multifuncion System “MSF”, herramienta básica de la estimuloterapia programada. DENTUM 2009, 9, 119–125. [Google Scholar]
- Durán Von Arx, J.; Ustrell Torrent, M.J. Técnica, M.S.F. Diagnóstico de la matriz functional: Codificación. Ortodon. Clin. 2003, 6, 138–140. [Google Scholar]
- Pinho, T.; Maciel, P.; Lemos, C.; Sousa, A. Familial aggregation of maxillary lateral incisor agenesis. J. Dent. Res. 2010, 89, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Tallón-Walton, V.; Nieminen, P.; Arte, S.; Ustrell-Torrent, J.M.; Carvalho-Lobato, P.; Manzanares-Céspedes, M.C. Oral findings in Midline Syndrome: A case report and literature review. Med Oral Patol Oral Cir Bucal. 2010, 15, e579–e582. [Google Scholar] [CrossRef]
- Grandi, D. The “Interdisciplinary Orofacial Examination Protocol for Children and Adolescents”: A resource for the interdisciplinary assessment of the stomatognatic system. Int. J. Orofac. Myol. 2012, 38, 15–26. [Google Scholar] [CrossRef]
- De La Dure-Molla, M.; Fournier, B.P.; Manzanares, M.C.; Acevedo, A.C.; Hennekam, R.C.; Friedlander, L.; Boy-Lefèvre, M.L.; Kerner, S.; Toupenay, S.; Garrec, P.; et al. Elements of morphology: Standard terminology for the teeth and classifying genetic dental disorders. Am. J. Med. Genet. A. 2019, 179, 1913–1981. [Google Scholar] [CrossRef]
- ORPHANET. Available online: https://www.orpha.net/es/disease/detail/881?name=S%C3%ADndrome%20de%20Turner&mode=name (accessed on 26 March 2024).
- Human Phenotype Ontology (HPO). Available online: https://hpo.jax.org/app/browse/term/HP:0000347 (accessed on 26 March 2024).
- Kruszka, P.; Addissie, Y.A.; Tekendo-Ngongang, C.; Jones, K.L.; Savage, S.K.; Gupta, N.; Sirisena, N.D.; Dissanayake, V.H.W.; Paththinige, C.S.; Aravena, T.; et al. Turner syndrome in diverse populations. Am. J. Med. Genet. A. 2020, 182, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.D.; Bamba, V.; Bothwell, S.; Fechner, P.Y.; Furniss, A.; Ikomi, C.; Nahata, L.; Nokoff, N.J.; Pyle, L.; Seyoum, H.; et al. Development and Validation of a Computable Phenotype for Turner Syndrome Utilizing Electronic Health Records from a National Pediatric Network. medRxiv. 2023. preprint. [Google Scholar] [CrossRef]
- Bilge, N.H.; Yeşiltepe, S.; Törenek Ağırman, K.; Çağlayan, F.; Bilge, O.M. Investigation of prevalence of dental anomalies by using digital panoramic radiographs. Folia Morphol. 2018, 77, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Wagner, V.P.; Arrué, T.; Hilgert, E.; Arús, N.A.; Da Silveira, H.L.D.; Martins, M.D.; Rodrigues, J.A. Prevalence and distribution of dental anomalies in a paediatric population based on panoramic radiographs analysis. Eur. J. Paediatr. Dent. 2020, 21, 292–298. [Google Scholar] [PubMed]
- Sella Tunis, T.; Sarne, O.; Hershkovitz, I.; Finkelstein, T.; Pavlidi, A.M.; Shapira, Y.; Davidovitch, M.; Shpack, N. Dental Anomalies’ Characteristics. Diagnostics 2021, 11, 1161. [Google Scholar] [CrossRef] [PubMed]
- Pandey, P.; Ansari, A.A.; Choudhary, K.; Saxena, A. Familial aggregation of maxillary lateral incisor agenesis (MLIA). BMJ Case Rep. 2013, 26, bcr2012007846. [Google Scholar] [CrossRef] [PubMed]
- Jeong, K.H.; Kim, D.; Song, Y.M.; Sung, J.; Kim, Y.H. Epidemiology and genetics of hypodontia and microdontia: A study of twin families. Angle Orthod. 2015, 85, 980–985. [Google Scholar] [CrossRef]
- Kantaputra, P.; Jatooratthawichot, P.; Chintakanon, K.; Intachai, W.; Pradermdutsadeeporn, P.; Adisornkanj, P.; Tongsima, S.; Ngamphiw, C.; Olsen, B.; Tucker, A.S.; et al. Mutations in LRP6 highlight the role of WNT signaling in oral exostoses and dental anomalies. Arch Oral Biol. 2022, 142, 105514. [Google Scholar] [CrossRef]
- Salanitri, S.; Seow, W.K. Developmental enamel defects in the primary dentition: Aetiology and clinical management. Aust. Dent. J. 2013, 58, 133–140. [Google Scholar] [CrossRef]
- Vélez-León, E.; Albaladejo-Martínez, A.; Pacheco-Quito, E.M.; Armas-Vega, A.; Delgado-Gaete, A.; Pesántez-Ochoa, D.; Melo, M. Developmental Enamel Defects in Children from the Southern Region of Ecuador. Children 2022, 9, 1755. [Google Scholar] [CrossRef]
- Reis, C.L.B.; Barbosa, M.C.F.; De Lima, D.C.; Brancher, J.A.; Lopes, C.M.C.F.; Baratto-Filho, F.; Küchler, E.C.; De Oliveira, D.S.B. Risk factors for developmental defects of enamel in children from southeastern Brazil. Community Dent. Health 2021, 38, 178–181. [Google Scholar] [PubMed]
- Torlińska-Walkowiak, N.; Majewska, K.A.; Sowińska, A.; Kędzia, A.; Opydo-Szymaczek, J. Developmental enamel defects and dental anomalies of number and size in children with growth hormone deficiency. Sci. Rep. 2023, 13, 14707. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, M.; Lähdesmäki, R.; Niinimaa, A.; Alvesalo, L. Molar morphology and the expression of Carabelli’s trait in 45,X females. Am. J. Hum. Biol. 2015, 27, 486–493. [Google Scholar] [CrossRef]
- Torlińska-Walkowiak, N.; Majewska, K.A.; Sowińska, A.; Kędzia, A.; Opydo-Szymaczek, J. Skeletal and dental age discrepancy and occlusal traits in children with growth hormone deficiency and idiopathic short stature. Clin. Oral Investig. 2022, 26, 6165–6175. [Google Scholar] [CrossRef] [PubMed]
- Torlińska-Walkowiak, N.; Majewska, K.A.; Kędzia, A.; Opydo-Szymaczek, J. Clinical Implications of Growth Hormone Deficiency for Oral Health in Children: A Systematic Review. J. Clin Med. 2021, 10, 3733. [Google Scholar] [CrossRef] [PubMed]
- Drenski Balija, N.; Aurer, B.; Meštrović, S.; Lapter Varga, M. Prevalence of Dental Anomalies in Orthodontic Subjects. Acta Stomatol. Croat. 2022, 56, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Vinjolli, F.; Zeqaj, M.; Dragusha, E.; Malara, A.; Danesi, C.; Laganà, G. Dental anomalies in an Albanian orthodontic sample: A retrospective study. BMC Oral Health. 2023, 23, 47. [Google Scholar] [CrossRef]
- Laganà, G.; Venza, N.; Borzabadi-Farahani, A.; Fabi, F.; Danesi, C.; Cozza, P. Dental anomalies: Prevalence and associations between them in a large sample of non-orthodontic subjects, a cross-sectional study. BMC Oral Health. 2017, 17, 62. [Google Scholar] [CrossRef] [PubMed]
- Ashoori, N.; Ghorbanyjavadpour, F.; Rakhshan, V. Associations between 44 nonmetric permanent dental traits or anomalies with skeletal sagittal malocclusions and sex, besides correlations across the variations or abnormalities. BMC Oral Health. 2022, 22, 544. [Google Scholar] [CrossRef]
- Salerno, C.; D’Avola, V.; Oberti, L.; Almonte, E.; Bazzini, E.M.; Tartaglia, G.M.; Cagetti, M.G. Rare Genetic Syndromes and Oral Anomalies: A Review of the Literature and Case Series with a New Classification Proposal. Children 2021, 9, 12. [Google Scholar] [CrossRef]
- Vahid-Dastjerdi, E.; Borzabadi-Farahani, A.; Mahdian, M.; Amini, N. Non-syndromic hypodontia in an Iranian orthodontic population. J. Oral. Sci. 2010, 52, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Vahid-Dastjerdi, E.; Borzabadi-Farahani, A.; Mahdian, M.; Amini, N. Supernumerary teeth amongst Iranian orthodontic patients. A retrospective radiographic and clinical survey. Acta Odontol. Scand. 2011, 69, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Golovcencu, L.; Romanec, C.; Martu, M.A.; Anistoroaiei, D.; Pacurar, M. Particularities of orthodontic treatment in patients with dental anomalies that need orthodontic-restorative therapeutic approach. Rev. Chim. 2019, 70, 3046–3049. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Number + Size + Shape + Structure + Position + Alignment | Malocclusion | Tongue Mobility + Tonsils | Class II Facial Profile | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TS Subject | % Signs | % First-Degree Relatives (Mother|Father) | % Signs | % in First-Degree Relatives (Mother|Father) | % Signs | % in First-Degree Relatives (Mother|Father) | % signs | % in First-Degree Relatives (Mother|Father) | |||||
| ESTM0003 | 50% | NA | 100% | NA | 50% | NA | 0% | NA | |||||
| ESTM0016 | 33% | NA | 50% | NA | 0% | NA | 100% | NA | |||||
| ESTM0021 | 0% | 33% | 0% | 0% | 50% | 0% | 0% | 0% | |||||
| ESTM0022 | 50% | 17% | 17% | 100% | 50% | 50% | 50% | 0% | 0% | 100% | 0% | 0% | |
| ESTM0026 | 66% | NA | 100% | NA | 100% | NA | 100% | NA | |||||
| ESTM0027 | 33% | NA | 100% | NA | 50% | NA | 100% | NA | |||||
| ESTM0028 | 33% | 50% | 100% | 100% | 50% | 0% | 100% | 0% | |||||
| ESTM0030 | 50% | NA | 100% | NA | 50% | NA | 100% | NA | |||||
| ESTM0031 | 50% | 0% | 33% | 100% | 50% | 0% | 50% | 0% | 0% | 100% | 0% | 100% | |
| ESTM0034 | 33% | 33% | 17% | 50% | 0% | 0% | 0% | 0% | 50% | 100% | 0% | 0% | |
| ESTM0037 | 50% | 17% | 50% | 100% | 50% | 0% | 100% | 100% | |||||
| ESTM0041 | 16% | 17% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 100% | 0% | 0% | |
| ESTM0045 | 33% | 0% | 50% | 0% | 100% | 0% | 100% | 0% | |||||
| ESTM0047 | 16% | NA | 100% | NA | 100% | NA | 100% | NA | |||||
| Average | 37% | 24% | 71% | 29% | 50% | 4% | 86% | 16% | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tallón-Walton, V.; Sánchez-Molins, M.; Hu, W.; Martínez-Abadías, N.; Casado, A.; Manzanares-Céspedes, M.C. Comprehensive Oral Diagnosis and Management for Women with Turner Syndrome. Diagnostics 2024, 14, 769. https://doi.org/10.3390/diagnostics14070769
Tallón-Walton V, Sánchez-Molins M, Hu W, Martínez-Abadías N, Casado A, Manzanares-Céspedes MC. Comprehensive Oral Diagnosis and Management for Women with Turner Syndrome. Diagnostics. 2024; 14(7):769. https://doi.org/10.3390/diagnostics14070769
Chicago/Turabian StyleTallón-Walton, Victoria, Meritxell Sánchez-Molins, Wenwen Hu, Neus Martínez-Abadías, Aroa Casado, and María Cristina Manzanares-Céspedes. 2024. "Comprehensive Oral Diagnosis and Management for Women with Turner Syndrome" Diagnostics 14, no. 7: 769. https://doi.org/10.3390/diagnostics14070769
APA StyleTallón-Walton, V., Sánchez-Molins, M., Hu, W., Martínez-Abadías, N., Casado, A., & Manzanares-Céspedes, M. C. (2024). Comprehensive Oral Diagnosis and Management for Women with Turner Syndrome. Diagnostics, 14(7), 769. https://doi.org/10.3390/diagnostics14070769