
Referable Diabetic Retinopathy Prediction Algorithm Applied to a Population of 120,389 Type 2 Diabetics over 11 Years Follow-Up

 , ,
, ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
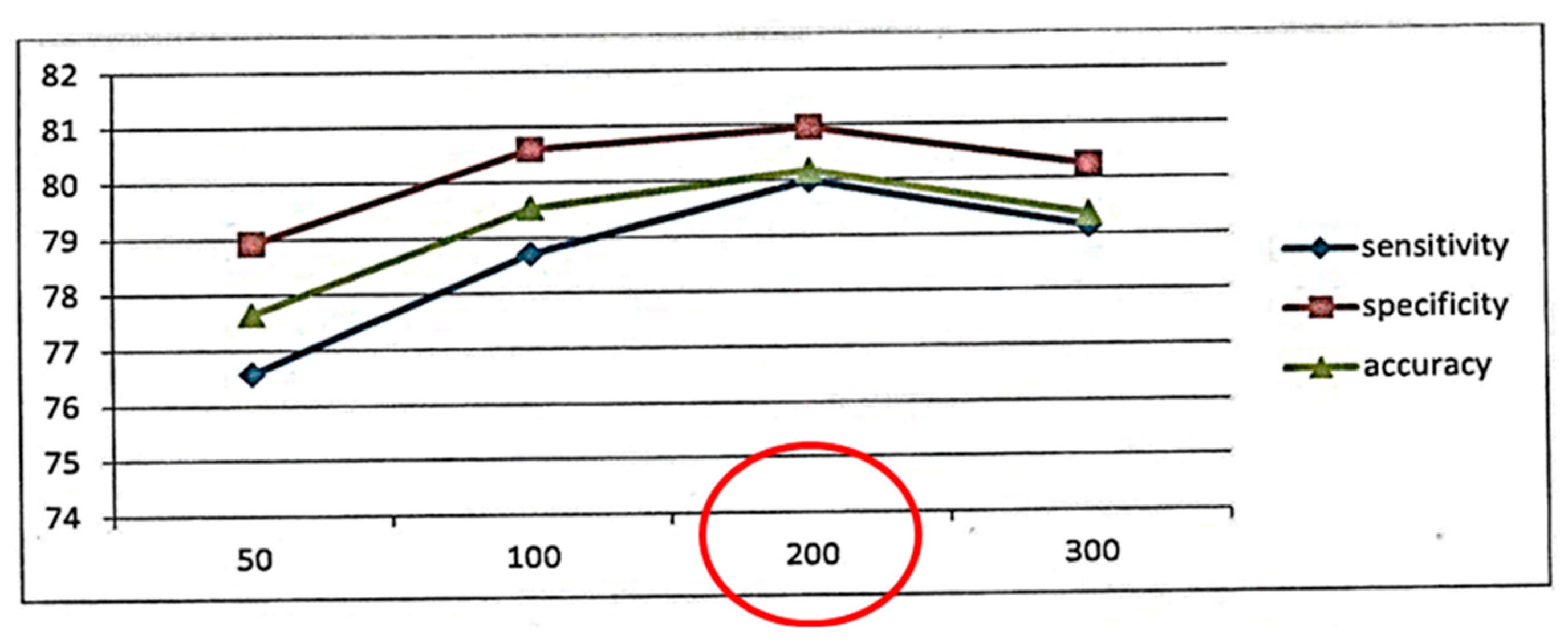
2.2. Sample Size
2.3. Inclusion Criteria
- Patients with type 2 DM.
- Patients without DR or with mild DR.
2.4. Exclusion Criteria
- Patients with type 1 DM.
- Patients included in diabetes group III and other specific types (i.e., diseases of the exocrine pancreas, endocrinopathy, genetic defects in ß-cell function, genetic defects in insulin action).
- Patients included in diabetes group IV and gestational diabetes mellitus (GDM).
- Patients who did not have a complete EHR.
- Patients with DR more serious than mild.
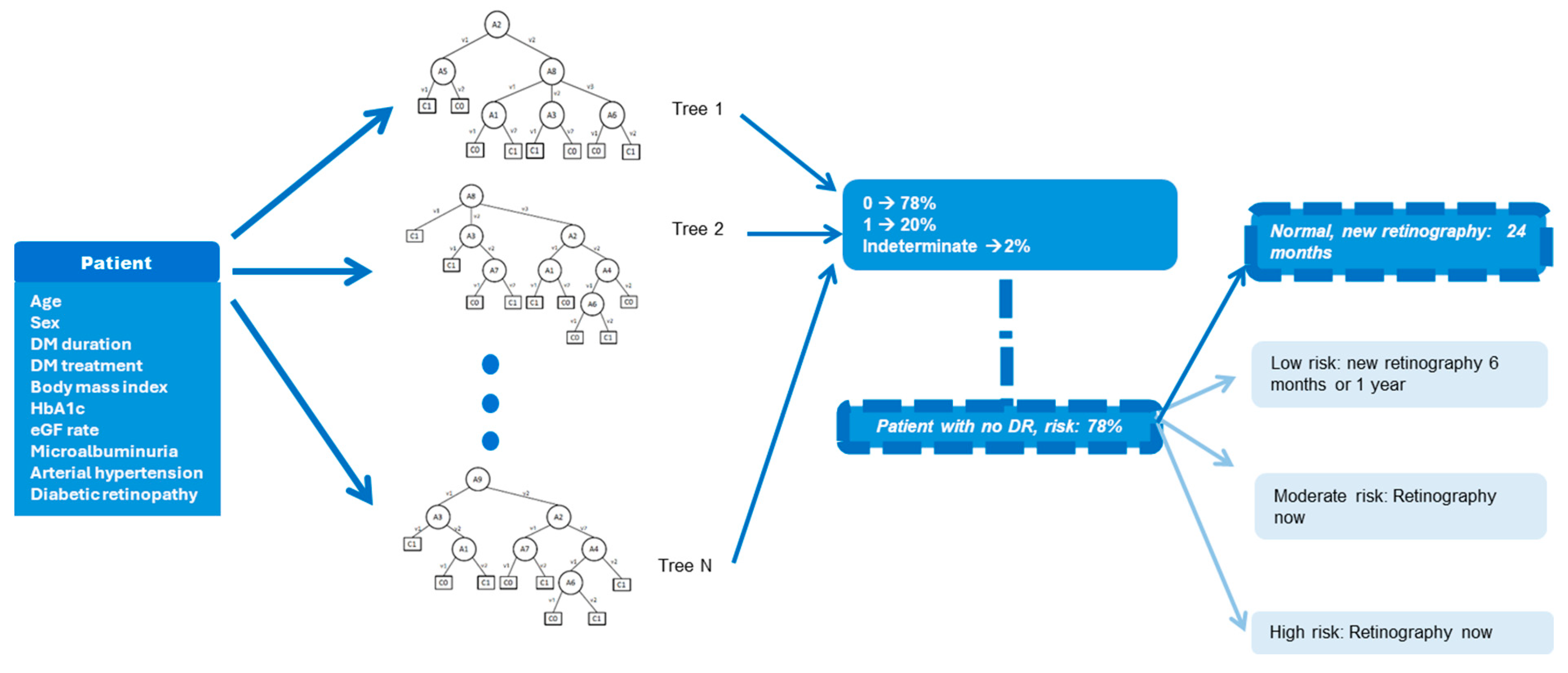
2.5. Construction of the Algorithm
- Current age
- Sex
- Body mass index
- Duration of T2DM in units of one year
- T2DM treatment, diet, oral antidiabetics, insulin, insulin analogues
- Control of arterial hypertension (normal values: systolic BP < 140, diastolic BP < 90)
- HbA1c% in 1% fractions
- Estimated glomerular filtration rate, calculated from plasma creatinine using the chronic kidney disease epidemiology collaboration equation (CKD-EPI equation)
- Microalbuminuria value 30 mg/min up to 300 mg/min
- 10.
- Mild DR (yes or no)
2.6. Statistical Methods
3. Results
3.1. Demographic Data
3.2. Statistical Analysis of the Confusion Matrix/Contingency
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teo, Z.L.; Tham, Y.C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y.; et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-Analysis. Ophthalmology 2021, 128, 1580–1591. [Google Scholar] [CrossRef] [PubMed]
- Soriguer, F.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R. Prevalence of diabetes mellitus and impaired glucose regulation in Spain: The [email protected] Study. Diabetologia 2012, 55, 88–93. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 12. Retinopathy, Neuropathy, and Foot Care: Standards of Care in Diabetes—2024. Diabetes Care 2024, 47 (Suppl. S1), S231–S243. Available online: https://diabetesjournals.org/care/article/47/Supplement_1/S231/153941/12-Retinopathy-Neuropathy-and-Foot-Care-Standards (accessed on 16 April 2024). [CrossRef] [PubMed]
- Diabetes care and research in Europe: The Saint Vincent declaration. Diabet. Med. 1990, 7, 360. [CrossRef]
- IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussles, Belgium, 2021; Available online: https://diabetesatlas.org/atlas/tenth-edition/ (accessed on 16 April 2024).
- Wong, T.Y.; Sun, J.; Kawasaki, R.; Ruamviboonsuk, P.; Gupta, N.; Lansingh, V.C.; Maia, M.; Mathenge, W.; Moreker, S.; Muqit, M.M.K.; et al. Guidelines on Diabetic Eye Care: The International Council of Ophthalmology Recommendations for Screening, Follow-Up, Referral, and Treatment Based on Resource Settings. Ophthalmology 2018, 125, 1608–1622. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Kumar, N.; Feuer, W.J.; Chou, C.F.; Rosa, P.R.; Schiffman, J.C.; Morante, A.; Aldahan, A.; Staropoli, P.; Fernandez, C.A.; et al. Dilated eye examination screening guideline compliance among patients with diabetes without a diabetic retinopathy diagnosis: The role of geographic access. BMJ Open Diabetes Res. Care 2014, 2, e000031. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Serpas, L.; Genter, P.; Anderson, B.; Campa, D.; Ipp, E. Divergent Perceptions of Barriers to Diabetic Retinopathy Screening among Patients and Care Providers, Los Angeles, California, 2014–2015. Prev. Chronic. Dis. 2016, 13, E140. [Google Scholar] [CrossRef] [PubMed]
- Drinkwater, J.J.; Kalantary, A.; Turner, A.W. A systematic review of diabetic retinopathy screening intervals. Acta Ophthalmol. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Soto-Pedre, E.; Pinies, J.A.; Hernaez-Ortega, M.C. External validation of a risk assessment model to adjust the frequency of eye-screening visits in patients with diabetes mellitus. J. Diabetes Complicat. 2015, 29, 508–511. [Google Scholar] [CrossRef]
- Lund, S.H.; Aspelund, T.; Kirby, P.; Russell, G.; Einarsson, S.; Palsson, O.; Stefánsson, E. Individualised risk assessment for diabetic retinopathy and optimisation of screening intervals: A scientific approach to reducing healthcare costs. Br. J. Ophthalmol. 2016, 100, 683–687. [Google Scholar] [CrossRef]
- Eleuteri, A.; Fisher, A.C.; Broadbent, D.M.; García-Fiñana, M.; Cheyne, C.P.; Wang, A.; Stratton, I.M.; Gabbay, M.; Seddon, D.; Harding, S.P.; et al. Individualised variable-interval risk-based screening for sight-threatening diabetic retinopathy: The Liverpool Risk Calculation Engine. Diabetologia 2017, 60, 2174–2182. [Google Scholar] [CrossRef]
- Aspelund, T.; Thornórisdóttir, O.; Olafsdottir, E.; Gudmundsdottir, A.; Einarsdóttir, A.B.; Mehlsen, J.; Einarsson, S.; Pálsson, O.; Einarsson, G.; Bek, T.; et al. Individual risk assessment and information technology to optimise screening frequency for diabetic retinopathy. Diabetologia 2011, 54, 2525–2532. [Google Scholar] [CrossRef] [PubMed]
- Scanlon, P.H.; Aldington, S.J.; Leal, J.; Luengo-Fernandez, R.; Oke, J.; Sivaprasad, S.; Gazis, A.; Stratton, I.M. Development of a cost-effectiveness model for optimisation of the screening interval in diabetic retinopathy screening. Health Technol. Assess. 2015, 19, 1–116. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, D.M.; Sampson, C.J.; Wang, A.; Howard, L.; Williams, A.E.; Howlin, S.U.; Appelbe, D.; Moitt, T.; Cheyne, C.P.; Rahni, M.M. Individualised screening for diabetic retinopathy: The ISDR study-rationale, design and methodology for a randomised controlled trial comparing annual and individualised risk-based variable-interval screening. BMJ Open 2019, 9, e025788. [Google Scholar] [CrossRef] [PubMed]
- Romero-Aroca, P.; Verges-Pujol, R.; Santos-Blanco, E.; Maarof, N.; Valls, A.; Mundet, X.; Moreno, A.; Galindo, L.; Baget-Bernaldiz, M. Validation of a Diagnostic Support System for Diabetic Retinopathy Based on Clinical Parameters. Transl. Vis. Sci. Technol. 2021, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.sidiap.org/index.php/es/qui-som-2/el-sidiap (accessed on 5 March 2023).
- Romero-Aroca, P.; Valls, A.; Moreno, A.; Sagarra-Alamo, R.; Basora-Gallisa, J.; Saleh, E.; Baget-Bernaldiz, M.; Puig, D. A Clinical Decision Support System for Diabetic Retinopathy Screening: Creating a Clinical Support Application. Telemed. e-Health 2019, 25, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Shaw, M.J. Induction of fuzzy decision trees. Fuzzy Sets Syst. 1995, 69, 125–135. [Google Scholar] [CrossRef]
- Saleh, E.; Błaszczyński, J.; Moreno, A.; Valls, A.; Romero-Aroca, P.; de la Riva-Fernández, S.; Słowiński, R. Learning ensemble classifiers for diabetic retinopathy assessment. Artif. Intell. Med. 2018, 85, 50–63. [Google Scholar] [CrossRef] [PubMed]
- BDA Retinal Photography Screening for Diabetic Eye Disease; British Diabetic Association: London, UK, 1997; Report No. 1997.
- Shreffler, J.; Huecker, M.R. Diagnostic Testing Accuracy: Sensitivity, Specificity, Predictive Values and Likelihood Ratios. [Updated 2023 Mar 6]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557491/ (accessed on 16 April 2024).
- Nunes, S.; Pires, I.; Rosa, A.; Duarte, L.; Bernardes, R.; Cunha-Vaz, J. Microaneurysm turnover is a biomarker for diabetic retinopathy progression to clinically significant macular edema: Findings for type 2 diabetics with nonproliferative retinopathy. Ophthalmologica 2009, 223, 292–297. [Google Scholar] [CrossRef]
- Bernardes, R.; Nunes, S.; Pereira, I.; Torrent, T.; Rosa, A.; Coelho, D.; Cunha-Vaz, J. Computer-assisted microaneurysm turnover in the early stages of diabetic retinopathy. Ophthalmologica 2009, 223, 2842–2891. [Google Scholar] [CrossRef]
- Nunes, S.; Ribeiro, L.; Lobo, C.; Cunha-Vaz, J. Three different phenotypes of mild nonproliferative diabetic retinopathy with different risks for development of clinically significant macular edema. Investig. Ophthalmol. Vis. Sci. 2013, 54, 595–604. [Google Scholar] [CrossRef] [PubMed]
- van der Heijden, A.A.; Walraven, I.; van’t Riet, E.; Aspelund, T.; Lund, S.H.; Elders, P.; Polak, B.C.; Moll, A.C.; Keunen, J.E.; Dekker, J.M.; et al. Validation of a model to estimate personalised screening frequency to monitor diabetic retinopathy. Diabetologia 2014, 57, 1332–1338. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean | |
|---|---|
| Age in years | 68.01 ± 10.41 |
| Men | 68,578 (57%) |
| Women | 51,811 (43%) |
| DM duration in years | 9.11 ± 5.48 |
| DM treatment: diet | 11,840 (9.8%) |
| DM treatment: oral agents | 92,325 (76.7%) |
| DM treatment: insulin | 16,224 (13.5%) |
| Arterial hypertension | 37,209 (30.9%) |
| Body mass index in kg/m2 | 27.86 ± 5.17 |
| HbA1c in % | 7.75 ± 1.59 |
| Microalbuminuria mg/24 h | 25.44 ± 125.92 |
| CKD-EPI in mil/min/1.73 m2 | 75.08 ± 16.55 |
| Patients’ Status at the Beginning of the Study | Percentage | Patients’ Status at the End of the Study | Percentage | |
|---|---|---|---|---|
| No DR | 111,172 | 92.36% | 101,695 | 84.5% |
| Mild DR | 9207 | 7.64% | 12,919 | 10.7% |
| Moderate DR | 4194 | 3.5% | ||
| Severe DR | 598 | 0.5% | ||
| Proliferative DR | 492 | 0.4% | ||
| Diabetic macular edema | 491 | 0.4% | ||
| Total of patients with DR | 18,694 | 15.5% |
| Any DR | RDR | |
|---|---|---|
| True positive | 8387 | 4727 |
| False positive | 2324 | 1466 |
| True negative | 108,588 | 113,148 |
| False negative | 1090 | 1048 |
| Accuracy | 0.97 (95% CI, 0.96–0.98) | 0.97 (95% CI, 0.95–0.99) |
| AUC (area under the curve ROC) | 0.93 (95% CI, 0.92–0.94) | 0.90 (95% CI, 0.89–0.91) |
| Sensitivity or recall | 0.88 (95% CI, 0.86–0.90) | 0.82 (95% CI, 0.80–0.84) |
| Specificity | 0.98 (95% CI, 0.96–0.99) | 0.99 (95% CI, 0.95–0.994) |
| HM or F1 score | 0.83 (95% CI, 0.81–0.84) | 0.79 (95% CI, 0.78–0.80) |
| Precision or positive predictive values | 0.78 (95% CI, 0.75–0.80) | 0.76 (95% CI, 0.74–0.80) |
| Negative predictive values | 0.99 (95% CI, 0.98–0.999) | 0.99 (95% CI, 0.97–0.997) |
| Author (Name of Algorithm) Country | Country (Author) Type of Study | Number of Patients in Sample | AUC |
|---|---|---|---|
| Aspelund [13] (RETIRISK) Denmark | Denmark (Aspelund) Validation | 5199 T1DM/T2DM patients with a 20-year follow-up | |
| Spain (Soto Pedre) Real-world test | 508 T1DM/T2DM patients | 0.74 | |
| Netherlands (van der Heijden) Real-world test | 76 T1DM/T2DM patients with a 26-month follow-up | 0.83 | |
| United Kingdom (Lund) Validation | 9690 T1DM/T2DM patient with a 2-year follow-up | 0.83 | |
| Scanlon [14] United Kingdom | Gloucestershire (Scanlon) Real-world test | 15,877 T1DM/T2DM patients | 0.77 |
| Broadbent [15] United Kingdom | Liverpool (Broadbent) Real-world test | 4460 T1DM/T2DM patients | 0.88 |
| Romero-Aroca [16] (RETIPROGRAM) Spain | Spain (Romero-Aroca) Validation | 101,802 T2DM patients | 0.87 |
| Spain (Romero-Aroca) Real-world test | 602 T2DM patients | 0.98 | |
| Spain (Romero-Aroca) Real-world test | 120,384 T2DM patients with an 11-year follow-up Prediction of any type of DR | 0.93 | |
| 120,384 T2DM patients with an 11-year follow-up Prediction of RDR | 0.90 |
| Aspelund | Scanlon | Broadbent | Authors | |
|---|---|---|---|---|
| Current age | √ | √ | √ | |
| Age at diagnosis | √ | |||
| Sex | √ | √ | ||
| DM duration | √ | √ | √ | |
| DM treatment | √ | |||
| Systolic blood pressure | √ | √ | √ | |
| Diastolic blood pressure | √ | |||
| Total cholesterol | √ | √ | ||
| HbA1c % | √ | √ | √ | √ |
| Microalbuminuria | √ | |||
| Glomerular filtration rate measured using the CKD-EPI algorithm | √ | |||
| Body mass index | √ | |||
| DM type | √ | |||
| Diabetic retinopathy | √ | √ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Aroca, P.; Verges, R.; Pascual-Fontanilles, J.; Valls, A.; Franch-Nadal, J.; Mundet, X.; Moreno, A.; Basora, J.; Garcia-Curto, E.; Baget-Bernaldiz, M. Referable Diabetic Retinopathy Prediction Algorithm Applied to a Population of 120,389 Type 2 Diabetics over 11 Years Follow-Up. Diagnostics 2024, 14, 833. https://doi.org/10.3390/diagnostics14080833
Romero-Aroca P, Verges R, Pascual-Fontanilles J, Valls A, Franch-Nadal J, Mundet X, Moreno A, Basora J, Garcia-Curto E, Baget-Bernaldiz M. Referable Diabetic Retinopathy Prediction Algorithm Applied to a Population of 120,389 Type 2 Diabetics over 11 Years Follow-Up. Diagnostics. 2024; 14(8):833. https://doi.org/10.3390/diagnostics14080833
Chicago/Turabian StyleRomero-Aroca, Pedro, Raquel Verges, Jordi Pascual-Fontanilles, Aida Valls, Josep Franch-Nadal, Xavier Mundet, Antonio Moreno, Josep Basora, Eugeni Garcia-Curto, and Marc Baget-Bernaldiz. 2024. "Referable Diabetic Retinopathy Prediction Algorithm Applied to a Population of 120,389 Type 2 Diabetics over 11 Years Follow-Up" Diagnostics 14, no. 8: 833. https://doi.org/10.3390/diagnostics14080833
APA StyleRomero-Aroca, P., Verges, R., Pascual-Fontanilles, J., Valls, A., Franch-Nadal, J., Mundet, X., Moreno, A., Basora, J., Garcia-Curto, E., & Baget-Bernaldiz, M. (2024). Referable Diabetic Retinopathy Prediction Algorithm Applied to a Population of 120,389 Type 2 Diabetics over 11 Years Follow-Up. Diagnostics, 14(8), 833. https://doi.org/10.3390/diagnostics14080833