Quiescent-Interval Single-Shot Magnetic Resonance Angiography

 ,
,
Abstract
:1. Introduction
2. Non-Enhanced MRA Techniques
2.1. Time of Flight
2.2. Phase-Contrast
2.3. 3D Half-Fourier Fast Spin Echo
2.4. Balanced Steady-State Free Precession
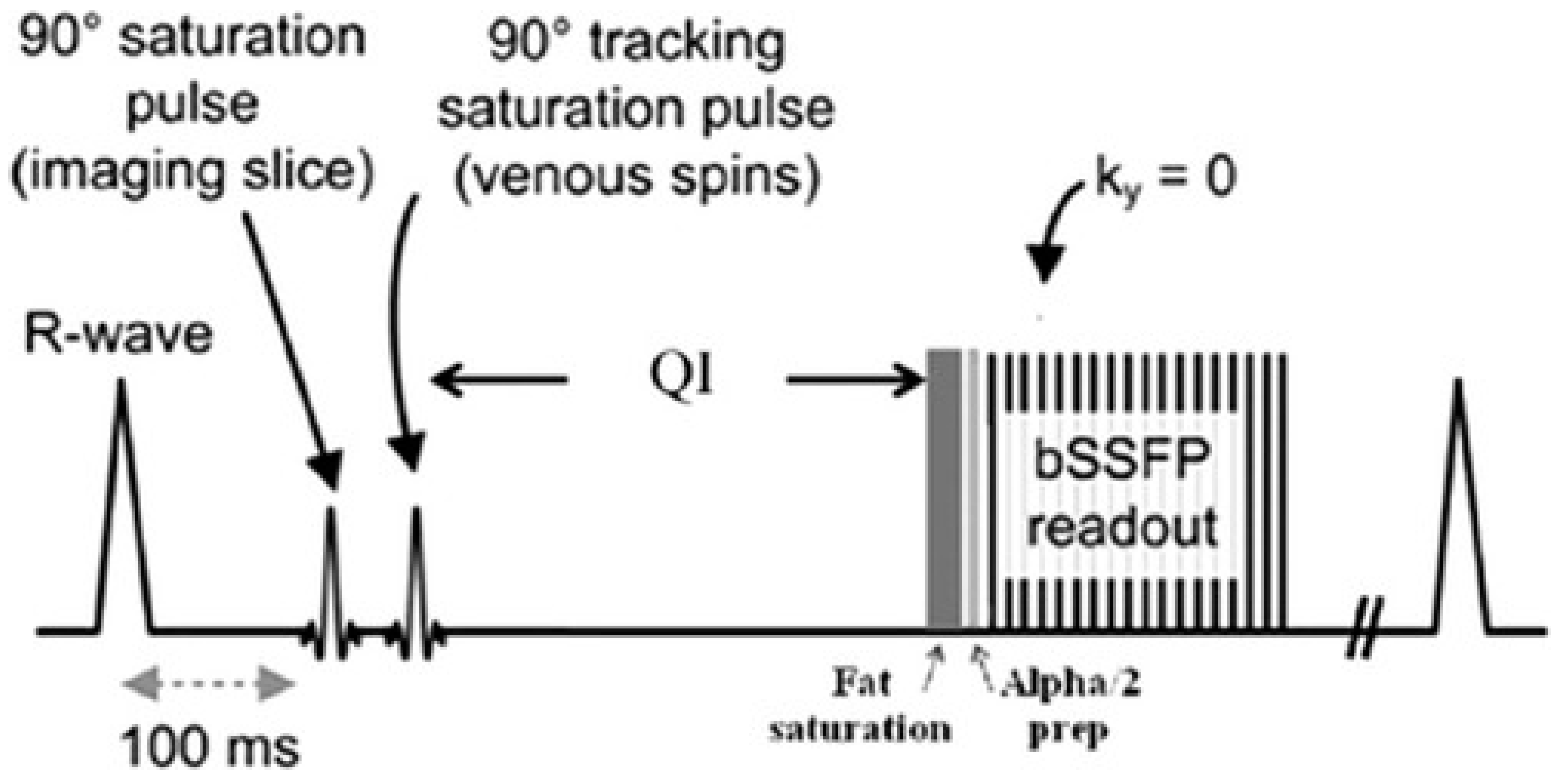
2.5. Quiescent-Interval Single-Shot MRA
3. Discussion
3.1. QISS: Technical Considerations and Early Feasibility studies
3.2. Comparisons with Existing Non-Invasive Diagnostic Techniques
3.3. Comparison to Non-Enhanced MRA Techniques
3.4. Technical Advancements and Alternative Applications
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.R. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J. Vasc. Surg. 2007, 45, S5–S67. [Google Scholar] [CrossRef] [PubMed]
- Fowkes, F.G.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.; Williams, L.J.; Mensah, G.A.; et al. Comparison of Global Estimates of Prevalence and Risk Factors for Peripheral Artery Disease in 2000 and 2010: A Systematic Review and Analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Resnick, H.E.; Lindsay, R.S.; McDermott, M.M.; Devereux, R.B.; Jones, K.L.; Fabsitz, R.R.; Howard, B.V. Relationship of High and Low Ankle Brachial Index to All-Cause and Cardiovascular Disease Mortality: The Strong Heart Study. Circulation 2004, 109, 733–739. [Google Scholar] [CrossRef] [PubMed]
- O’Hare, A.M.; Rodriguez, R.A.; Bacchetti, P. Low Ankle-Brachial Index Associated with Rise in Creatinine Level over Time: Results from the Atherosclerosis Risk in Communities Study. Arch. Intern. Med. 2005, 165, 1481–1485. [Google Scholar] [CrossRef] [PubMed]
- Murabito, J.M.; Evans, J.C.; Larson, M.G.; Nieto, K.; Levy, D.; Wilson, P.W. The Ankle-Brachial Index in the Elderly and Risk of Stroke, Coronary Disease, and Death: The Framingham Study. Arch. Intern. Med. 2003, 163, 1939–1942. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Li, J.; Pang, W.; Zhao, M.; Luo, Y.; Sun, Y.; Hu, D. Sensitivity and Specificity of Ankle-Brachial Index for Detecting Angiographic Stenosis of Peripheral Arteries. Circ. J. 2008, 72, 605–610. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.O.; Hunink, M.G.; Polak, J.F. Summary Receiver Operating Characteristic Curves as a Technique for Meta-Analysis of the Diagnostic Performance of Duplex Ultrasonography in Peripheral Arterial Disease. Acad Radiol 1996, 3, 361–369. [Google Scholar] [CrossRef]
- Wicky, S.; Pinto, E.; Oklu, R. Catheter-Directed Thrombolysis of Arterial Thrombosis. Semin. Thromb. Hemost. 2013, 39, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Heijenbrok-Kal Kock, M.C.J.M.; Myriam Hunink, M.G.M. Lower Extremity Arterial Disease: Multidetector CT Angiography-Meta Analysis. Radiology 2007, 245, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Collins, R.; Burch, J.; Cranny, G.; Aguiar-Ibanez, R.; Craig, D.; Wright, K.; Berry, E.; Gough, M.; Kleijnen, J.; Westwood, M. Duplex Ultrasonography, Magnetic Resonance Angiography, and Computed Tomography Angiography for Diagnosis and Assessment of Symptomatic, Lower Limb Peripheral Arterial Disease: Systematic Review. BMJ 2007, 334, 1257. [Google Scholar] [CrossRef] [PubMed]
- Ouwendijk, R.; de Vries, M.; Stijnen, T.; Pattynama, P.M.; van Sambeek, M.R.; Buth, J.; Tielbeek, A.V.; van der Vliet, D.A.; SchutzeKool, L.J.; Kitslaar, P.J.; et al. Multicenter Randomized Controlled Trial of the Costs and Effects of Noninvasive Diagnostic Imaging in Patients with Peripheral Arterial Disease: The DIPAD Trial. Am. J. Roentgenol. 2008, 190, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Meyersohn, N.M.; Walker, T.G.; Oliveira, G.R. Advances in Axial Imaging of Peripheral Vascular Disease. Curr. Cardiol. Rep. 2015, 17, 87. [Google Scholar] [CrossRef] [PubMed]
- Leiner, T. Magnetic Resonance Angiography of Abdominal and Lower Extremity Vasculature. Top. Magn. Reson. Imaging 2005, 16, 21–66. [Google Scholar] [CrossRef] [PubMed]
- Wheaton, A.J.; Miyazaki, M. Non-Contrast Enhanced MR Angiography: Physical Principles. J. Magn. Reson. Imaging 2012, 36, 286–304. [Google Scholar] [CrossRef] [PubMed]
- Morita, S.; Masukawa, A.; Suzuki, K.; Hirata, M.; Kojima, S.; Ueno, E. Unenhanced MR Angiography: Techniques and Clinical Applications in Patients with Chronic Kidney Disease. Radiographics 2011, 31, E13–E33. [Google Scholar] [CrossRef] [PubMed]
- De Haan, M.W.; Kouwenhoven, M.; Thelissen, R.P.; Koster, D.; Kessels, A.G.; de Leeuw, P.W.; van Engelshoven, J.M. Renovascular Disease in Patients with Hypertension: Detection with Systolic and Diastolic Gating in Three-Dimensional, Phase-Contrast MR Angiography. Radiology 1996, 198, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Lim, R.P.; Hecht, E.M.; Xu, J.; Babb, J.S.; Oesingmann, N.; Wong, S.; Muhs, B.E.; Gagne, P.; Lee, V.S. 3D Nongadolinium-Enhanced ECG-Gated MRA of the Distal Lower Extremities: Preliminary Clinical Experience. J. Magn. Reson. Imaging 2008, 28, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Miyazaki, M.; Kuroki, K.; Yamamoto, A.; Hiramine, A.; Admiraal-Behloul, F. Noncontrast-Enhanced Peripheral MRA: Technical Optimization of Flow-Spoiled Fresh Blood Imaging for Screening Peripheral Arterial Diseases. Magn. Reson. Med. 2011, 65, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, M.; Akahane, M. Non-Contrast Enhanced MR Angiography: Established Techniques. J. Magn. Reson. Imaging 2012, 35, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Foo, T.K.; Ho, V.B.; Marcos, H.B.; Hood, M.N.; Choyke, P.L. MR Angiography Using Steady-State Free Precession. Magn. Reson. Med. 2002, 48, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Edelman, R.R.; Sheehan, J.J.; Dunkle, E.; Schindler, N.; Carr, J.; Koktzoglou, I. Quiescent-Interval Single-Shot Unenhanced Magnetic Resonance Angiography of Peripheral Vascular Disease: Technical Considerations and Clinical Feasibility. Magn. Reson. Med. 2010, 63, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Edelman, R.R.; Carr, M.; Koktzoglou, I. Advances in Non-Contrast Quiescent-Interval Slice-Selective (QISS) Magnetic Resonance Angiography. Clin. Radiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Hodnett, P.A.; Koktzoglou, I.; Davarpanah, A.H.; Scanlon, T.G.; Collins, J.D.; Sheehan, J.J.; Dunkle, E.E.; Gupta, N.; Carr, J.C.; Edelman, R.R. Evaluation of Peripheral Arterial Disease with Nonenhanced Quiescent-Interval Single-Shot MR Angiography. Radiology 2011, 260, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Hodnett, P.A.; Ward, E.V.; Davarpanah, A.H.; Scanlon, T.G.; Collins, J.D.; Glielmi, C.B.; Bi, X.; Koktzoglou, I.; Gupta, N.; Carr, J.C.; et al. Peripheral Arterial Disease in a Symptomatic Diabetic Population: Prospective Comparison of Rapid Unenhanced MR Angiography (MRA) with Contrast-Enhanced MRA. Am. J. Roentgenol. 2011, 197, 1466–1473. [Google Scholar] [CrossRef] [PubMed]
- Klasen, J.; Blondin, D.; Schmitt, P.; Bi, X.; Sansone, R.; Wittsack, H.J.; Kropil, P.; Quentin, M.; Kuhlemann, J.; Miese, F.; et al. Nonenhanced ECG-Gated Quiescent-Interval Single-Shot MRA (QISS-MRA) of the Lower Extremities: Comparison with Contrast-Enhanced MRA. Clin. Radiol. 2012, 67, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Thierfelder, K.M.; Meimarakis, G.; Nikolaou, K.; Sommer, W.H.; Schmitt, P.; Kazmierczak, P.M.; Reiser, M.F.; Theisen, D. Non-Contrast-Enhanced MR Angiography at 3 Tesla in Patients with Advanced Peripheral Arterial Occlusive Disease. PLoS ONE 2014, 9, e91078. [Google Scholar] [CrossRef] [PubMed]
- Hansmann, J.; Morelli, J.N.; Michaely, H.J.; Riester, T.; Budjan, J.; Schoenberg, S.O.; Attenberger, U.I. Nonenhanced ECG-Gated Quiescent-Interval Single Shot MRA: Image Quality and Stenosis Assessment at 3 Tesla Compared with Contrast-Enhanced MRA and Digital Subtraction Angiography. J. Magn. Reson. Imaging 2014, 39, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Amin, P.; Collins, J.D.; Koktzoglou, I.; Molvar, C.; Markl, M.; Edelman, R.R.; Carr, J.C. Evaluating Peripheral Arterial Disease with Unenhanced Quiescent-Interval Single-Shot MR Angiography at 3 T. Am. J. Roentgenol. 2014, 202, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Knobloch, G.; Gielen, M.; Lauff, M.T.; Romano, V.C.; Schmitt, P.; Rick, M.; Kroncke, T.J.; Huppertz, A.; Hamm, B.; Wagner, M. ECG-Gated Quiescent-Interval Single-Shot MR Angiography of the Lower Extremities: Initial Experience at 3 T. Clin. Radiol. 2014, 69, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.; Knobloch, G.; Gielen, M.; Lauff, M.T.; Romano, V.; Hamm, B.; Kroncke, T. Nonenhanced Peripheral MR-Angiography (MRA) at 3 Tesla: Evaluation of Quiescent-Interval Single-Shot MRA in Patients Undergoing Digital Subtraction Angiography. Int. J. Cardiovasc. Imaging 2015, 31, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.V.M.; Usman, A.A.; Hodnett, P.A.; Carr, J.C.; Edelman, R.R. Ankle-Brachial Index (ABI) and Quiescent-Interval Single Shot (QISS) MRA in Peripheral Arterial Disease (PAD): Comparison of Diagnostic Accuracy and Need for Additional Imaging Procedures. J. Cardiovasc. Magn. Reson. 2011, 13. [Google Scholar] [CrossRef]
- Varga-Szemes, A.; Wichmann, J.L.; Schoepf, U.J.; Suranyi, P.; De Cecco, C.N.; Muscogiuri, G.; Caruso, D.; Yamada, R.T.; Litwin, S.E.; Tesche, C.; et al. Accuracy of Noncontrast Quiescent-Interval Single-Shot Lower Extremity MR Angiography Versus CT Angiography for Diagnosis of Peripheral Artery Disease: Comparison With Digital Subtraction Angiography. JACC Cardiovasc. Imaging 2017, 10, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Yang, J.; Zhang, T.; Morelli, J.N.; Giri, S.; Li, X.; Tang, W. The Diagnostic Value of Non-Contrast Enhanced Quiescent Interval Single Shot (QISS) Magnetic Resonance Angiography at 3T for Lower Extremity Peripheral Arterial Disease, in Comparison to CT Angiography. J. Cardiovasc. Magn. Reson. 2016, 18, 71. [Google Scholar] [CrossRef] [PubMed]
- Offerman, E.J.; Hodnett, P.A.; Edelman, R.R.; Koktzoglou, I. Nonenhanced Methods for Lower-Extremity MRA: A Phantom Study Examining the Effects of Stenosis and Pathologic Flow Waveforms at 1.5T. J. Magn. Reson. Imaging 2011, 33, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.V.; Galizia, M.S.; Usman, A.; Popescu, A.R.; Dunkle, E.; Edelman, R.R. Comparison of Quiescent Inflow Single-Shot and Native Space for Nonenhanced Peripheral MR Angiography. J. Magn. Reson. Imaging 2013, 38, 1531–1538. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Zou, L.; Huang, Y.; Liu, D.; Tang, Y.; Fan, Z.; Chen, H.; Liu, X. Non-Contrast Enhanced MR Angiography (NCE-MRA) of the Calf: A Direct Comparison between Flow-Sensitive Dephasing (FSD) Prepared Steady-State Free Precession (SSFP) and Quiescent-Interval Single-Shot (QISS) in Patients with Diabetes. PLoS ONE 2015, 10, e0128786. [Google Scholar] [CrossRef] [PubMed]
- Altaha, M.A.; Jaskolka, J.D.; Tan, K.; Rick, M.; Schmitt, P.; Menezes, R.J.; Wintersperger, B.J. Non-Contrast-Enhanced MR Angiography in Critical Limb Ischemia: Performance of Quiescent-Interval Single-Shot (QISS) and TSE-Based Subtraction Techniques. Eur. Radiol. 2017, 27, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- Edelman, R.R.; Giri, S.; Dunkle, E.; Galizia, M.; Amin, P.; Koktzoglou, I. Quiescent-Inflow Single-Shot Magnetic Resonance Angiography Using a Highly Undersampled Radial k-Space Trajectory. Magn. Reson. Med. 2013, 70, 1662–1668. [Google Scholar] [CrossRef] [PubMed]
- Edelman, R.R.; Giri, S.; Murphy, I.G.; Flanagan, O.; Speier, P.; Koktzoglou, I. Ungated Radial Quiescent-Inflow Single-Shot (UnQISS) Magnetic Resonance Angiography Using Optimized Azimuthal Equidistant Projections. Magn. Reson. Med. 2014, 72, 1522–1529. [Google Scholar] [CrossRef] [PubMed]
- Koktzoglou, I.; Murphy, I.G.; Giri, S.; Edelman, R.R. Quiescent Interval Low Angle Shot Magnetic Resonance Angiography of the Extracranial Carotid Arteries. Magn. Reson. Med. 2016, 75, 2072–2077. [Google Scholar] [CrossRef] [PubMed]
- Edelman, R.R.; Silvers, R.I.; Thakrar, K.H.; Metzl, M.D.; Nazari, J.; Giri, S.; Koktzoglou, I. Nonenhanced MR Angiography of the Pulmonary Arteries Using Single-Shot Radial Quiescent-Interval Slice-Selective (QISS): A Technical Feasibility Study. J. Cardiovasc. Magn. Reson. 2017, 19, 48. [Google Scholar] [CrossRef] [PubMed]
- Shen, D.; Edelman, R.R.; Robinson, J.D.; Haji-Valizadeh, H.; Messina, M.; Giri, S.; Koktzoglou, I.; Rigsby, C.K.; Kim, D. Single-Shot Coronary Quiescent-Interval Slice-Selective Magnetic Resonance Angiography Using Compressed Sensing: A Feasibility Study in Patients With Congenital Heart Disease. J. Comput. Assist. Tomogr. 2018. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Technique | Strengths | Limitations |
|---|---|---|
| ABI | Quick, inexpensive, highly sensitive for arterial stenosis >50% | Cannot characterize extent or exact location of stenosis/occlusion, limited accuracy in presence of highly calcified vessels |
| Duplex US | Quick, inexpensive, can characterize extent and location of disease, utility in post-interventional surveillance | Limited by operator experience, irregular anatomy, shadowing artifact |
| DSA | High resolution, provides physiologic information, allows for simultaneous intervention and assessment | Invasive, potential for vessel injury, ionizing radiation, nephrotoxic iodinated contrast use, allergic reactions |
| CTA | Quick, high resolution, 3D reconstructions assist in interventions, high diagnostic accuracy, cost-effective | Nephrotoxic iodinated contrast use, ionizing radiation, blooming artifact |
| CEMRA | High resolution, no ionizing radiation, 3D reconstructions assist in interventions, high diagnostic accuracy | Costly, reduced availability, metal and motion artifact, concern for NSF with gadolinium-based contrast |
| NEMRA | No iodinated or gadolinium based contrast removes concerns for renal toxicity/NSF, no ionizing radiation, allow for repeat screening/follow-up exams | Variable image quality, diagnostic accuracy and artifact susceptibility, costly, longer exam times, reduced availability |
| ABI | CTA | CEMRA | 2D TOF | 3D FSE | (FSD) SSFP | |
|---|---|---|---|---|---|---|
| Reference | [31] | [32] | [23] | [21] | [35] | [36] |
| Sensitivity/Specificity | QISS: 96%/92%, ABI: 76%/83% | QISS: 85%/97%, CTA: 87%/95% | QISS: 85-90%/95-97%, CEMRA: Ref. Std. | N/A | QISS: 85%*/96%, 3D FSE 87%*/87% | QISS: 93%*/92%, (FSD) SSFP: 95%*/99% |
| Strengths of QISS compared to study modality | Allows for characterization of extent/degree of stenosis | No iodinated contrast use, no radiation exposure | No gadolinium based contrast, allows for repeat examinations | No post-stenotic signal loss when compared to 2D TOF, improved image quality, reduced artifacts, shorter scan time | Increased image quality, no patient dependent changes to imaging parameters, less sensitive to motion | Does not require tailoring of imaging parameters, shorter scan time |
| Limitations of QISS compared to study modality | Costly, not readily available, longer exam times | Not readily available, certain stents can make some images non-diagnostic | Lower image quality in abdominopelvic vessels | In-plane signal loss for vessels not perpendicular to imaging slice, sensitive to static field inhomogeneities | Sensitive to static field homogeneities, in-plane signal loss for vessels not perpendicular to imaging slice | Lower image quality in peroneal and posterior tibial artery, lower diagnostic accuracy |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saini, A.; Wallace, A.; Albadawi, H.; Naidu, S.; Alzubaidi, S.; Knuttinen, M.G.; Panda, A.; Oklu, R. Quiescent-Interval Single-Shot Magnetic Resonance Angiography. Diagnostics 2018, 8, 84. https://doi.org/10.3390/diagnostics8040084
Saini A, Wallace A, Albadawi H, Naidu S, Alzubaidi S, Knuttinen MG, Panda A, Oklu R. Quiescent-Interval Single-Shot Magnetic Resonance Angiography. Diagnostics. 2018; 8(4):84. https://doi.org/10.3390/diagnostics8040084
Chicago/Turabian StyleSaini, Aman, Alex Wallace, Hassan Albadawi, Sailendra Naidu, Sadeer Alzubaidi, M. Grace Knuttinen, Anshuman Panda, and Rahmi Oklu. 2018. "Quiescent-Interval Single-Shot Magnetic Resonance Angiography" Diagnostics 8, no. 4: 84. https://doi.org/10.3390/diagnostics8040084
APA StyleSaini, A., Wallace, A., Albadawi, H., Naidu, S., Alzubaidi, S., Knuttinen, M. G., Panda, A., & Oklu, R. (2018). Quiescent-Interval Single-Shot Magnetic Resonance Angiography. Diagnostics, 8(4), 84. https://doi.org/10.3390/diagnostics8040084