
Real-Time Feedback of the Applied Light-Curing Technique and Its Impact on Degree of Conversion of Composite Restorations—A Study with Undergraduate Dental Students




Abstract
:1. Introduction
2. Materials and Methods
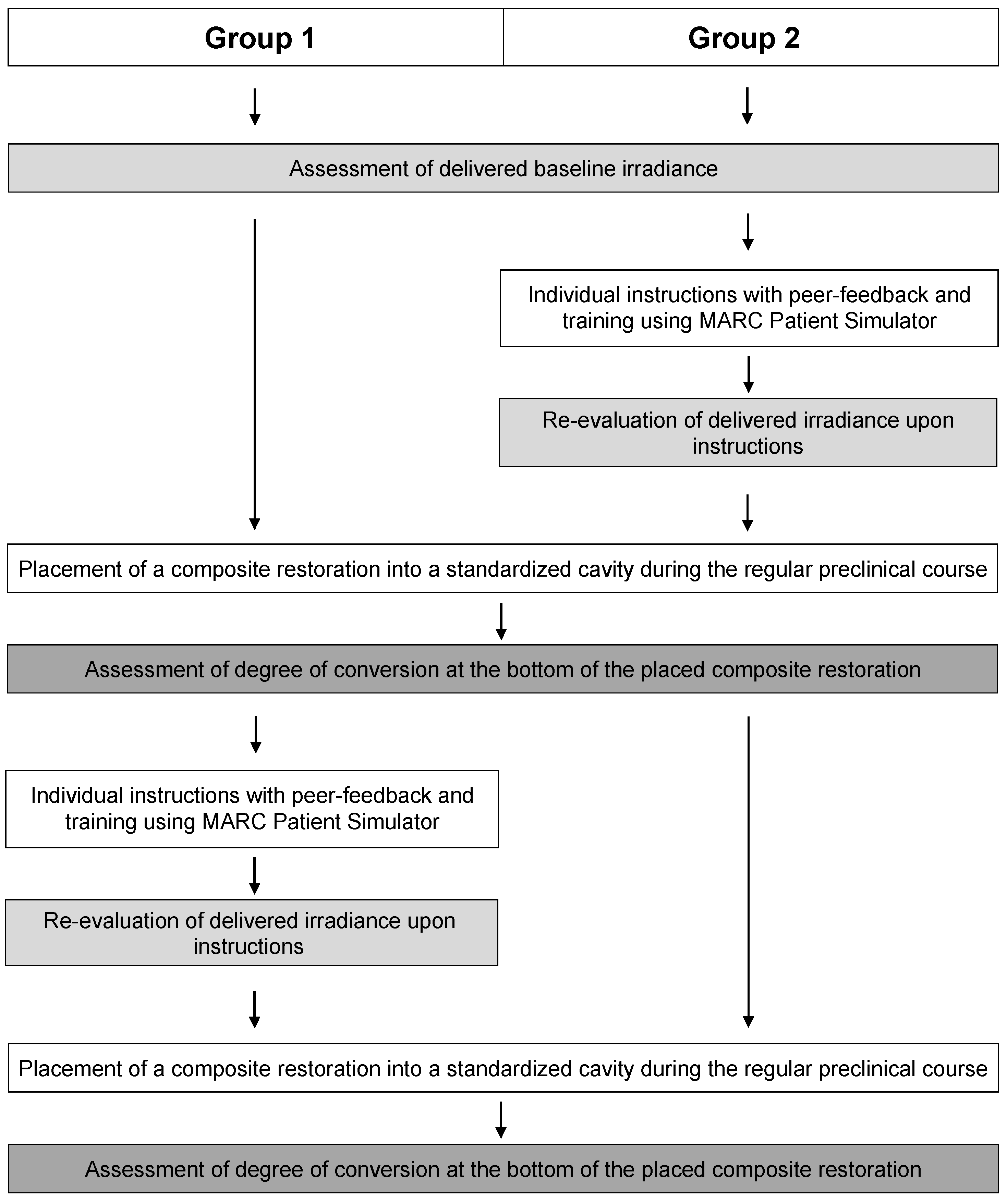
2.1. Test Groups
2.2. Individual Instructions on Light-Curing with MARC Patient Simulator
2.3. Placement of First Composite Restoration
2.4. Individual Instructions with MARC Patient Simulator of Group 1 and Placement of Second Composite Restoration for Both Groups
2.5. Degree of Conversion Analysis
2.6. Statistical Analysis
3. Results
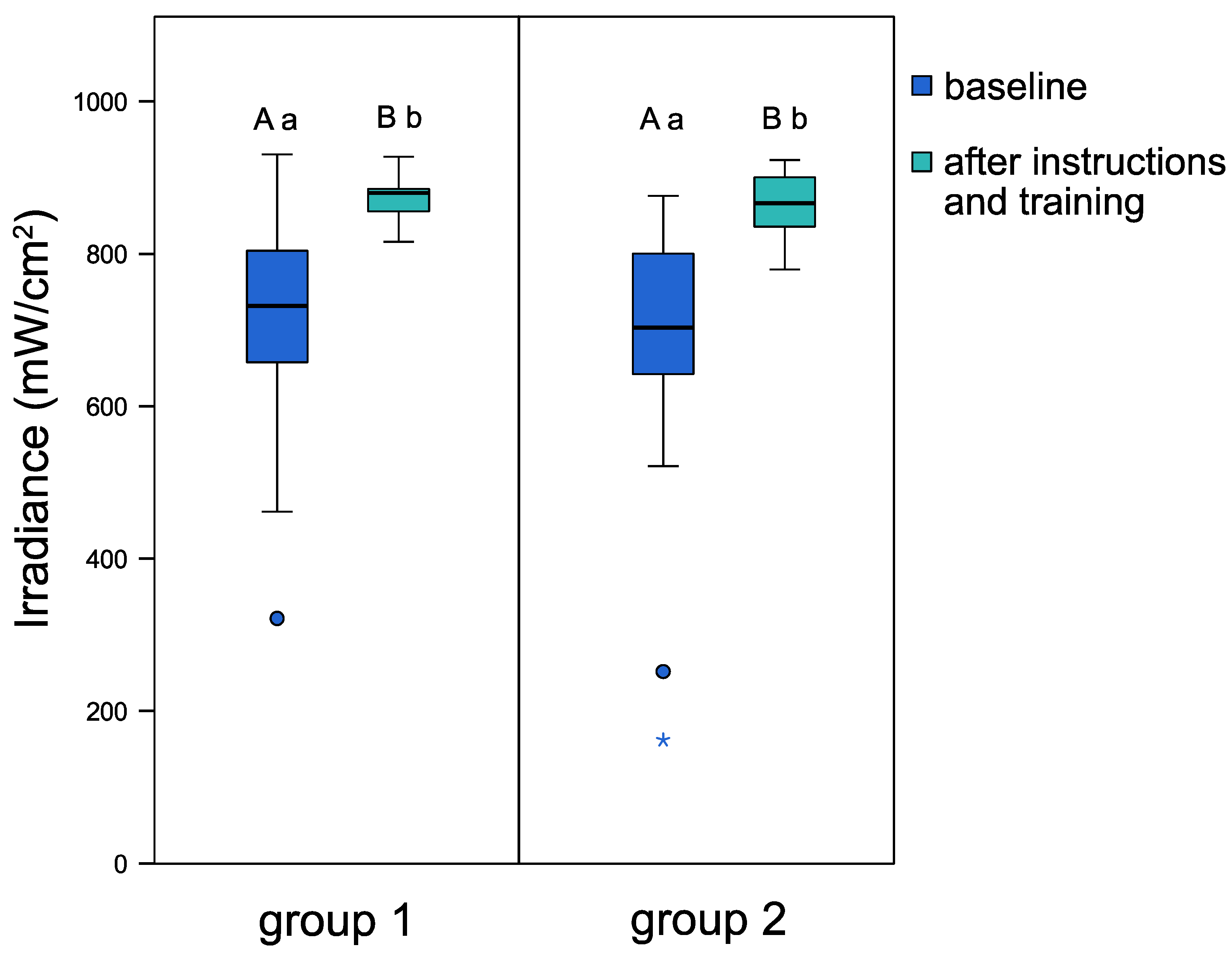
3.1. Light Irradiances before and after Individual Instructions
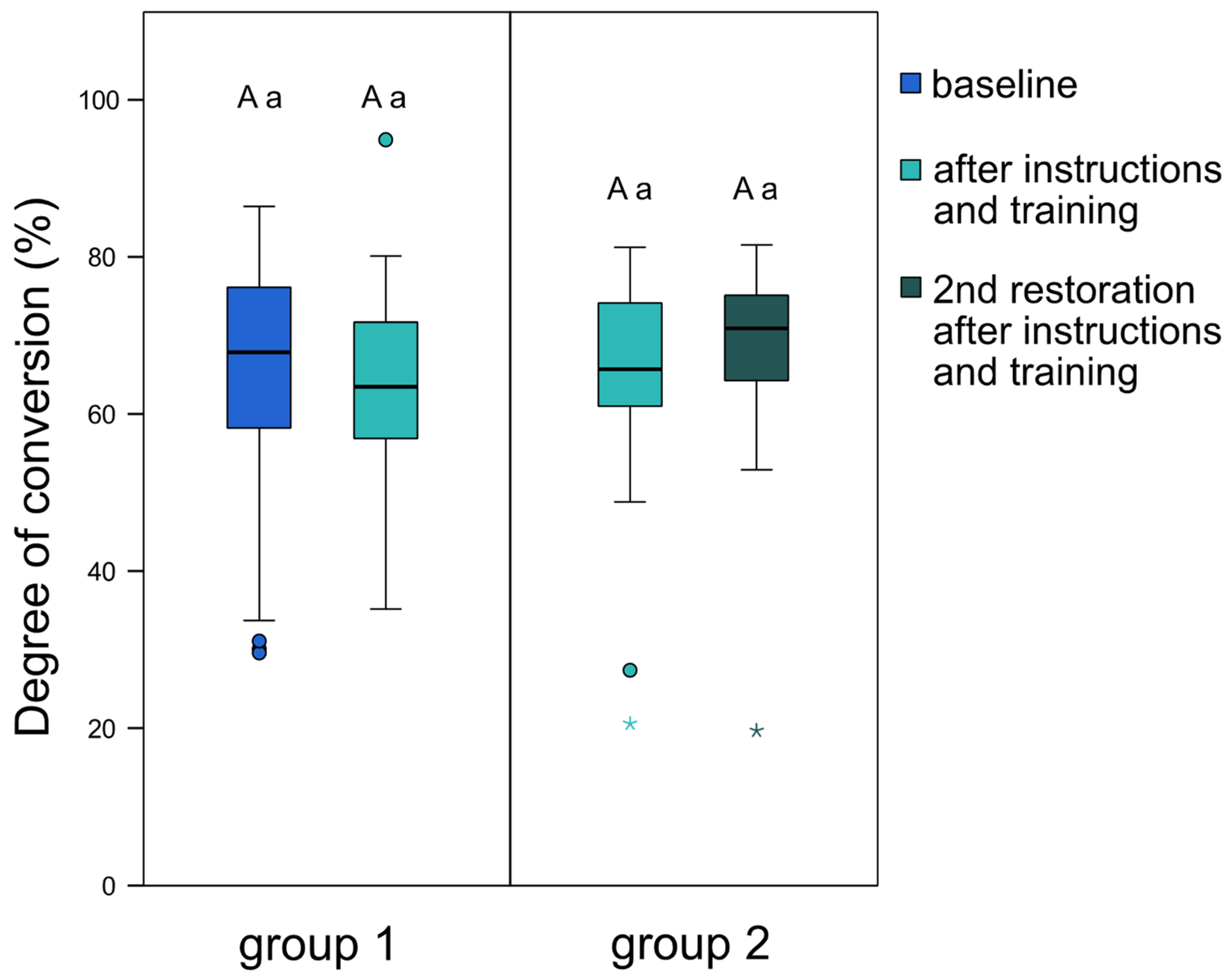
3.2. Degree of Conversion of the Composite Restorations
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Samaha, S.; Bhatt, S.; Finkelman, M.; Papathanasiou, A.; Perry, R.; Strassler, H.; Kugel, G.; Garcia-Godoy, F.; Price, R. Effect of instruction, light curing unit, and location in the mouth on the energy delivered to simulated restorations. Am. J. Dent. 2017, 30, 343–349. [Google Scholar] [PubMed]
- Barghi, N.; Fischer, D.E.; Pham, T. Revisiting the intensity output of curing lights in private dental offices. Compend. Contin. Educ. Dent. 2007, 28, 380–384. [Google Scholar] [PubMed]
- Calheiros, F.C.; Daronch, M.; Rueggeberg, F.A.; Braga, R.R. Influence of irradiant energy on degree of conversion, polymerization rate and shrinkage stress in an experimental resin composite system. Dent. Mater. 2008, 24, 1164–1168. [Google Scholar] [CrossRef]
- Ferracane, J.L.; Lawson, N.C. Probing the hierarchy of evidence to identify the best strategy for placing class II dental composite restorations using current materials. J. Esthet. Restor. Dent. 2021, 33, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Karacolak, G.; Turkun, L.S.; Boyacioglu, H.; Ferracane, J.L. Influence of increment thickness on radiant energy and microhardness of bulk-fill resin composites. Dent. Mater. J. 2018, 37, 206–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demarco, F.F.; Collares, K.; Correa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J. Should my composite restorations last forever? Why are they failing? Braz. Oral Res. 2017, 31, e56. [Google Scholar] [CrossRef] [Green Version]
- Jandt, K.D.; Mills, R.W. A brief history of LED photopolymerization. Dent. Mater. 2013, 29, 605–617. [Google Scholar] [CrossRef]
- Brambilla, E.; Gagliani, M.; Ionescu, A.; Fadini, L.; García-Godoy, F. The influence of light-curing time on the bacterial colonization of resin composite surfaces. Dent. Mater. 2009, 25, 1067–1072. [Google Scholar] [CrossRef]
- Fan, P.L.; Schumacher, R.M.; Azzolin, K.; Geary, R.; Eichmiller, F.C. Curing-light intensity and depth of cure of resin-based composites tested according to international standards. J. Am. Dent. Assoc. 2002, 133, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Al-Zain, A.O.; Platt, J.A. Effect of light-curing distance and curing time on composite microflexural strength. Dent. Mater. J. 2021, 40, 202–208. [Google Scholar] [CrossRef]
- Par, M.; Repusic, I.; Skenderovic, H.; Milat, O.; Spajic, J.; Tarle, Z. The effects of extended curing time and radiant energy on microhardness and temperature rise of conventional and bulk-fill resin composites. Clin. Oral Investig. 2019, 23, 3777–3788. [Google Scholar] [CrossRef]
- Leprince, J.G.; Palin, W.M.; Hadis, M.A.; Devaux, J.; Leloup, G. Progress in dimethacrylate-based dental composite technology and curing efficiency. Dent. Mater. 2013, 29, 139–156. [Google Scholar] [CrossRef]
- Hussain, M.; Wang, Y. Influence of prolonged light-curing time on the shear bonding strength of resin to bleached enamel. Oper. Dent. 2010, 35, 672–681. [Google Scholar] [CrossRef]
- Price, R.B.; McLeod, M.E.; Felix, C.M. Quantifying light energy delivered to a Class I restoration. J. Can. Dent. Assoc. 2010, 76, a23. [Google Scholar] [PubMed]
- Al-Zain, A.O.; Eckert, G.J.; Lukic, H.; Megremis, S.; Platt, J.A. Polymerization pattern characterization within a resin-based composite cured using different curing units at two distances. Clin. Oral Investig. 2019, 23, 3995–4010. [Google Scholar] [CrossRef] [PubMed]
- Lovell, L.G.; Lu, H.; Elliott, J.E.; Stansbury, J.W.; Bowman, C.N. The effect of cure rate on the mechanical properties of dental resins. Dent. Mater. 2001, 17, 504–511. [Google Scholar] [CrossRef]
- Par, M.; Spanovic, N.; Mohn, D.; Attin, T.; Tauböck, T.T.; Tarle, Z. Curing potential of experimental resin composites filled with bioactive glass: A comparison between Bis-EMA and UDMA based resin systems. Dent. Mater. 2020, 36, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Schattenberg, A.; Lichtenberg, D.; Stender, E.; Willershausen, B.; Ernst, C.P. Minimal exposure time of different LED-curing devices. Dent. Mater. 2008, 24, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Bouschlicher, M.R.; Rueggeberg, F.A.; Wilson, B.M. Correlation of bottom-to-top surface microhardness and conversion ratios for a variety of resin composite compositions. Oper. Dent. 2004, 29, 698–704. [Google Scholar]
- Lohbauer, U.; Rahiotis, C.; Krämer, N.; Petschelt, A.; Eliades, G. The effect of different light-curing units on fatigue behavior and degree of conversion of a resin composite. Dent. Mater. 2005, 21, 608–615. [Google Scholar] [CrossRef]
- Ferrari, R.; Attin, T.; Wegehaupt, F.J.; Stawarczyk, B.; Tauböck, T.T. The effects of internal tooth bleaching regimens on composite-to-composite bond strength. J. Am. Dent. Assoc. 2012, 143, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Wegehaupt, F.J.; Tauböck, T.T.; Attin, T. Durability of the anti-erosive effect of surfaces sealants under erosive abrasive conditions. Acta Odontol. Scand. 2013, 71, 1188–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peutzfeldt, A. Correlation between recordings obtained with a light-intensity tester and degree of conversion of a light-curing resin. Scand. J. Dent. Res. 1994, 102, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Price, R. Guest Editorial: Symposium on light sources in dentistry. Dent. Mater. 2013, 29, 137–138. [Google Scholar] [CrossRef]
- Watts, D.C. Let there be light. Dent. Mater. 2013, 29, 603–604. [Google Scholar] [CrossRef]
- Tauböck, T.T.; Par, M.; Attin, T.; Burrer, P. Effectiveness of using a patient simulator with real-time feedback to improve light-curing skills of dental students. Appl. Sci. 2020, 10, 8269. [Google Scholar] [CrossRef]
- Al-Ahdal, K.; Ilie, N.; Silikas, N.; Watts, D.C. Polymerization kinetics and impact of post polymerization on the degree of conversion of bulk-fill resin-composite at clinically relevant depth. Dent. Mater. 2015, 31, 1207–1213. [Google Scholar] [CrossRef]
- Tauböck, T.T.; Schmidlin, P.R.; Attin, T. Vertical bite rehabilitation of severely worn dentitions with direct composite restorations: Clinical performance up to 11 years. J. Clin. Med. 2021, 10, 1732. [Google Scholar] [CrossRef]
- Pallesen, U.; van Dijken, J.W. A randomized controlled 30 years follow up of three conventional resin composites in Class II restorations. Dent. Mater. 2015, 31, 1232–1244. [Google Scholar] [CrossRef]
- Nedeljkovic, I.; De Munck, J.; Vanloy, A.; Declerck, D.; Lambrechts, P.; Peumans, M.; Teughels, W.; Van Meerbeek, B.; Van Landuyt, K.L. Secondary caries: Prevalence, characteristics, and approach. Clin. Oral Investig. 2020, 24, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Opdam, N.J.; van de Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.; van Dijken, J.W. Longevity of posterior composite restorations: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef]
- Hasanain, F.A.; Nassar, H.M. Utilizing light cure units: A concise narrative review. Polymers 2021, 13, 1596. [Google Scholar] [CrossRef] [PubMed]
- Eltahlah, D.; Lynch, C.D.; Chadwick, B.L.; Blum, I.R.; Wilson, N.H.F. An update on the reasons for placement and replacement of direct restorations. J. Dent. 2018, 72, 1–7. [Google Scholar] [CrossRef]
- Demarco, F.F.; Corrêa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J. Longevity of posterior composite restorations: Not only a matter of materials. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Al-Zain, A.O.; Al-Osaimi, T.M. Effectiveness of using an instructional video in teaching light-curing technique. Adv. Med. Educ. Pract. 2021, 12, 289–302. [Google Scholar] [CrossRef] [PubMed]
- Rocha, M.G.; de Oliveira, D.; Correa, I.C.; Correr-Sobrinho, L.; Sinhoreti, M.; Ferracane, J.L.; Correr, A.B. Light-emitting diode beam profile and spectral output influence on the degree of conversion of bulk fill composites. Oper. Dent. 2017, 42, 418–427. [Google Scholar] [CrossRef]
- Federlin, M.; Price, R. Improving light-curing instruction in dental school. J. Dent. Educ. 2013, 77, 764–772. [Google Scholar] [CrossRef]
- Price, R.B.; Strassler, H.E.; Price, H.L.; Seth, S.; Lee, C.J. The effectiveness of using a patient simulator to teach light-curing skills. J. Am. Dent. Assoc. 2014, 145, 32–43. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Product | Composition | Lot No. | Manufacturer |
|---|---|---|---|
| Ceram.x universal | Matrix: methacrylic polysiloxane nanoparticles, poly-urethane-methacrylate, Bis-EMA 1, TEGDMA 2, dimethacrylate resin, ethyl-4-(dimethylamino)-benzoate Filler: spherical, pre-polymerized SphereTEC fillers (d3,50 ≈ 15 μm), non-agglomerated barium glass, ytterbium fluoride, camphorchinone Filler content: 77–79 wt%, 59–61 vol% | 1801000916 | Dentsply Sirona, Bensheim, Germany |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burrer, P.; Par, M.; Attin, T.; Tauböck, T.T. Real-Time Feedback of the Applied Light-Curing Technique and Its Impact on Degree of Conversion of Composite Restorations—A Study with Undergraduate Dental Students. J. Pers. Med. 2021, 11, 1012. https://doi.org/10.3390/jpm11101012
Burrer P, Par M, Attin T, Tauböck TT. Real-Time Feedback of the Applied Light-Curing Technique and Its Impact on Degree of Conversion of Composite Restorations—A Study with Undergraduate Dental Students. Journal of Personalized Medicine. 2021; 11(10):1012. https://doi.org/10.3390/jpm11101012
Chicago/Turabian StyleBurrer, Phoebe, Matej Par, Thomas Attin, and Tobias T. Tauböck. 2021. "Real-Time Feedback of the Applied Light-Curing Technique and Its Impact on Degree of Conversion of Composite Restorations—A Study with Undergraduate Dental Students" Journal of Personalized Medicine 11, no. 10: 1012. https://doi.org/10.3390/jpm11101012
APA StyleBurrer, P., Par, M., Attin, T., & Tauböck, T. T. (2021). Real-Time Feedback of the Applied Light-Curing Technique and Its Impact on Degree of Conversion of Composite Restorations—A Study with Undergraduate Dental Students. Journal of Personalized Medicine, 11(10), 1012. https://doi.org/10.3390/jpm11101012