
Uncertainty, Anxiety and Isolation: Experiencing the COVID-19 Pandemic and Lockdown as a Woman with Polycystic Ovary Syndrome (PCOS)

 , ,
, ,  ,
, {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Study Procedure
2.4. Data Collection
2.5. Data Analysis
3. Results
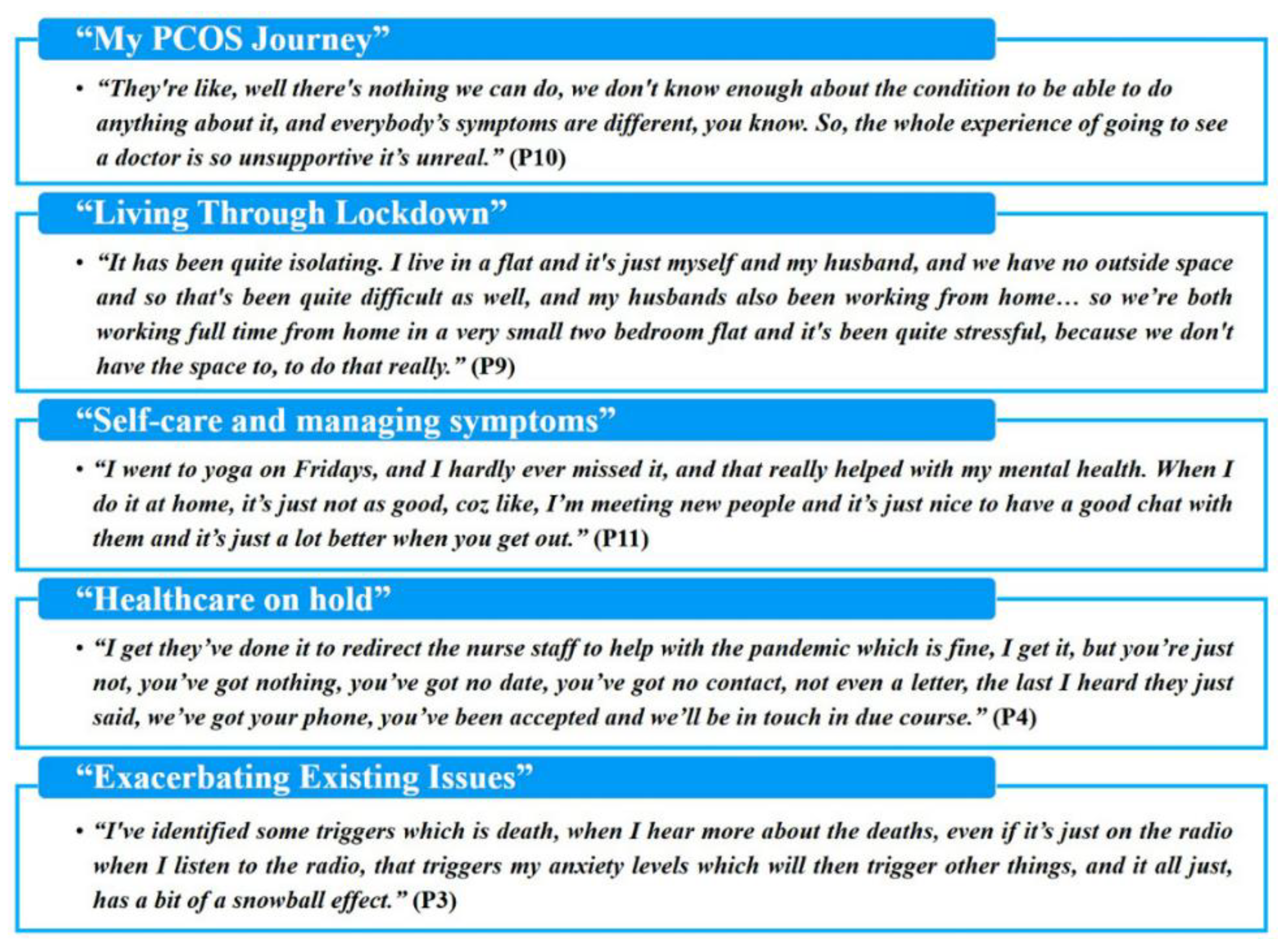
3.1. My PCOS Journey
“when I found out that I only ovulated from one ovary I sat and cried…I was terrified.”(P8)
“No one’s offered me an endocrinologist or a dermatologist I’ve just been told it’s not bad enough. And I was like well who are you to say it’s not bad enough? It’s bad enough for me.”(P5)
“the last couple of years I’ve spoken to a lot of other women, become a lot more knowledgeable I suppose, self-educated about it, probably more so in the last year… I was also trying to change my diet a bit during that time as well, I looked into supplements and things like that so probably since about August/September I’d start making some gradual changes in that respect as well, just sort of educating myself a bit more in the absence of any doctors.”(P2)
“I’ve done bootcamps, I’ve done the meal replacement diets, with varying success. Ten years ago, I managed to lose 8 stone because I didn’t eat any food other than the meal replacement packs for about six months. And it was fine, and it worked brilliantly, it was fantastic and there was a lot of symptoms cleared up and it was fab. They do really work and I’m trying it again actually and I lost 5 pounds last week, but its balance, you know sometimes I just want to be normal.”(P9)
“if it’s not the acne it’s the scars…and if it’s not that, it’s my weight and if it’s not that it’s the hair. If it’s not that it’s my mood, do you know what I mean, it’s like this spider web of things and you can’t sort find your way out of it.”(P10)
3.2. Self-Care and Managing Symptoms
3.2.1. Access to Supplies and Services
“when you’ve got access to shops, and chemists if you’re relying on long term medication, or if you’re struggling with certain menstrual problems accessing things like sanitary pads and stronger painkillers that’s been quite difficult, that’s been quite a challenge… if Tesco’s don’t have them in stock or if you’re not in an area where the pharmacy is going to deliver to you, that kinda thing, that’s been quite difficult.”(P11)
“to begin with, food was like, it was hard to get hold of, do you know what I mean? You just sort of, bought what you could to keep you going and that included a lot of things that were, processed do you know I mean, like sausage rolls and all the bits in the cupboard.”(P10)
“I would say not being able to do as much exercise. So, for example I can’t go to the gym, so that affects my weight as well as my mood. Not being able to go out as much affects my mood.”(P7)
“I just didn’t want to go backwards in my weight loss plans and worsen my PCOS symptoms.”(P1)
“I have gained three quarters of a stone since lockdown started, which is incredibly frustrating.”(P5)
“I would say, yeah it’s made me want to comfort eat more if I’m honest. It just makes me want to comfort eat more, I think with me anyway, growing up with PCOS I found it really difficult in terms of some of the symptoms, especially the excess hair and I feel like as a coping mechanism I would comfort eat. And I stopped doing that, but now it’s coming back again because of the pandemic, and the anxiety around how life is changing in all these different ways. So I feel like I’m going back to using unhealthy coping strategies again. Sometimes you just don’t feel like making an effort with your appearance, coz you’re not going out either.”(P7)
“And in terms of the, just like emotions being able to get out and have a breather. Being able to talk to my friends and my family about these issues I can’t really do that, like see them face to face I can’t do that, go out and do that.”(P7)
3.2.2. Freedom from Usual Pressures
“at the start you had kinda less access to certain foods, a lot less access to shops so that’s helped a bit this managing my health and wellbeing a bit. You’ve got to make more kinda smarter choices about what you’re eating I suppose. Walking everywhere as well instead of being able to use public transport so easily, so that’s helped a bit.”(P11)
“I had like a couple of days where I’ve been really stressed and I’ve had like a bit of bleeding, but I’m alright because you know I can change like every hour. But when I’m at work or whatever I can’t and I need to have days off work. But when I’m at home I’m okay, well I think I am!”(P6)
“I know I have been looking at diets and things more and trying to consider, like after all of this has happened, and I’m in a better state of mind to think about how I’m gonna consume food more... And I don’t know that if before all of this, I would have really sat and thought about it. For so much time.”(P8)
“it’s given me a drive to actually lose weight, which is always good. And maybe speak to people more when I’m struggling.”(P12)
“If anything, I think it’s been quite good in the sense that I’ve been a little bit less paranoid about having to do things like hair removal and that kind of stuff, because I’m not going out as much. So, it’s removed some of that social anxiety regarding it.”(P5)
3.3. Living through Lockdown
“I’ve got no choice really but to stay indoors more, so I think that’s… it’s frustrating. I think that emotionally can take a toll on you, sometimes I feel like socialising with, say like family members like my mum or dad and I don’t get to see them which makes me feel a bit isolated. And its little things like going to the shops and things because you feel more anxious about the time going, I just feel very anxious. And I think that can, and when you feel anxious and you are changing the way you live it makes me feel a bit like low mood as well. So yeah I think that’s it.”(P7)
3.4. Healthcare on Hold
“I had a period this week and because it was quite heavy and painful, I had phoned the GP surgery and I’d said if I could be given something like tranexamic acid even, just to make things a bit more manageable, but to actually get that help, you have to fill out an online form for the surgery, who then discuss it with the doctor, and then the doctor tells the receptionist what to do, then the receptionist phones me back, but they said that process could take up to three to four weeks, so that, yeah you feel that you can’t get the advice you would normally get at all.”(P11)
“I’m not able to be in touch with my doctor as much as I’d like, because she gives me some really good advice on things that she thinks will help, and obviously everybody is like drowning into the doctor’s system, so it’s really difficult to see anyone. And I absolutely adore my doctor she’s been amazing to me.”(P8)
“We’re waiting on an appointment for [fertility] treatment …, just before it happened and now everything’s put on hold… When you ring up to find out anything it’s just automated message that says we’ll come back to you, and it’s really hard coz we’ve already waited two and a half years to get to this point in March, and it’s just been pulled from under our feet again.”(P4)
“I thought about things like, if in the future I needed IVF because maybe I might find it difficult to get pregnant, in the future maybe because of my PCOS because I know these things can change. How would that work out, in terms of me being able to do that? It made me think about accessing, for example accessing like GP support really around my PCOS, I can’t just go to the doctor and see someone face to face.”(P7)
3.5. Exacerbating Existing Issues
“at home it is not really somewhere I can relax and I’m very tense and very anxious and a lot of that is to do with my mood and my depression that I get with my PCOS symptoms. So obviously spending all of my time at home and not being able escape and to go the gym or several dog walks a day or whatever I was finding it really hard, and I was kind of going backwards in a lot of things.”(P1)
“with me having so much time on my hands to think. There are times, you know over the last three months where I’ve had to sort of have a word with myself, do you know what I mean and sort of turn myself off and tell myself to calm down, sort of talk myself out of it, you know because that, that panic is just bubbling underneath, just there you know, and it’s like, the bars only gotta be shortened a little bit before it explodes, you know so it’s very hard.”(P10)
“I am really worried about catching it, like cos I haven’t seen a lot of things, you know like regarding PCOS and the virus so I would like to have seen a bit more things about it, because obviously there is quite a few women with it, they wouldn’t have seen as well which is really worrying like, am I gonna get it. I know you can’t tell if you’re going to get it really bad, but are we in that category where it could be really bad?”(P6)
“I think in that sense, the pandemic in some ways is easier to cope [with] because you’re sort of used to that level of restriction on your life anyway, but in other ways, I think it can be much more frightening as well because you realise that you’re probably one of those people who’s going to be a bit more vulnerable to that virus, and more vulnerable to not being able to access healthcare so easily as well, so I think it’s yes, there’s both kind of a positive side of having the sort of long term health issue, it can have a positive influence on how you cope with this kind of situation, but it has quite a negative one as well, it’s kind of pretty mixed.”(P11)
“we may try and socially distantly see my parents in the next few weeks. But we’ve not seen them at all, they’re over in Yorkshire so we would have had to drive to see them so it wasn’t an option anyway until recently, and we’ve sort of held back on that a bit longer. But yeah certainly keeping in touch with everyone, I just think that “I know my friends aren’t seeing each other separately anyway” we’re all sort of spread out and things, so I don’t feel that I’m missing out on things that, that my friends are doing, same with my family. So yeah, it’s always been fine really yeah, I’ve had days where I’ve felt a little bit down. I suppose, you just get a bit cabin fever.”(P2)
“I think I’ve been out four times since lockdown began, which has impacted my mental health quite a bit.”(P8)
4. Discussion
5. Conclusions and Implications for Practice
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- WHO. Coronavirus Disease 2019 (COVID-19): Situation Report, 51. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 12 June 2021).
- Bohn, M.K.; Hall, A.; Sepiashvili, L.; Jung, B.; Steele, S.; Adeli, K. Pathophysiology of COVID-19: Mechanisms Underlying Disease Severity and Progression. Physiology 2020, 35, 288–301. [Google Scholar] [CrossRef]
- Osuchowski, M.F.; Winkler, S.M.; Skirecki, T.; Cajander, S.; Shankar-Hari, M.; Lachmann, G.; Monneret, G.; Venet, F.; Bauer, M.; Brunkhorst, M.F. The COVID-19 puzzle: Deciphering pathophysiology and phenotypes of a new disease entity. Lancet Respir. Med. 2021, 9, 622–642. [Google Scholar] [CrossRef]
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.I.; Chapman, A.; Persad, E.; Klerings, I.; Wagner, G.; Sieber, U.; Christof, C.; Zachariah, C. Quarantine alone or in combination with other public health measures to control COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 9. [Google Scholar] [CrossRef]
- Girum, T.; Lentiro, K.; Geremew, M.; Migora, B.; Shewamare, S. Global strategies and effectiveness for COVID-19 prevention through contact tracing, screening, quarantine, and isolation: A systematic review. Trop. Med. Health 2020, 48, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Caristia, S.; Ferranti, M.; Skrami, E.; Raffetti, E.; Pierannunzio, D.; Palladino, R.; Ancona, C. Effect of national and local lockdowns on the control of COVID-19 pandemic: A rapid review. Epidemiol. Prev. 2020, 44, 60–68. [Google Scholar] [PubMed]
- Du, P.; Li, D.; Wang, A.; Shen, S.; Ma, Z.; Li, X. A Systematic Review and Meta-Analysis of Risk Factors Associated with Severity and Death in COVID-19 Patients. Can. J. Infect. Dis. Med. Microbiol. 2021, 2021, 6660930. [Google Scholar] [CrossRef]
- Wingert, A.; Wingert, A.; Pillay, J.; Gates, M.; Guitard, S.; Rahman, S.; Beck, A.; Hartling, L. Risk factors for severity of COVID-19: A rapid review to inform vaccine prioritisation in Canada. BMJ Open 2021, 11, e044684. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Gale, C.R.; Kivimäki, M.; Batty, G.D. Overweight, obesity, and risk of hospitalization for COVID-19: A community-based cohort study of adults in the United Kingdom. Proc. Natl. Acad. Sci. USA 2020, 117, 21011–21013. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Reed, A.B.; Ponzo, S.; Yassaee, A.; Aral, M.; Plans, D.; Mohan, D. Population risk factors for severe disease and mortality in COVID-19: A global systematic review and meta-analysis. PLoS ONE 2021, 16, e0247461. [Google Scholar] [CrossRef]
- Schlesinger, S.; Neuenschwander, M.; Lang, A.; Pafili, K.; Kuss, O.; Herder, C.; Roden, M. Risk phenotypes of diabetes and association with COVID-19 severity and death: A living systematic review and meta-analysis. Diabetologia 2021, 64, 1480–1491. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Zhou, N.; Zha, W.; Lv, Y. Hypertension is a clinically important risk factor for critical illness and mortality in COVID-19: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 745–755. [Google Scholar] [CrossRef]
- Shah, H.; Khan, M.S.H.; Dhurandhar, N.V.; Hegde, V. The triumvirate: Why hypertension, obesity, and diabetes are risk factors for adverse effects in patients with COVID-19. Acta Diabetol. 2021, 831–843. [Google Scholar] [CrossRef]
- Kyritsi, E.M.; Dimitriadis, G.K.; Kyrou, I.; Kaltsas, G.; Randeva, H.S. PCOS remains a diagnosis of exclusion: A concise review of key endocrinopathies to exclude. Clin. Endocrinol. 2017, 86, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyrou, I.; Weickert, M.O.; Randeva, H.S. Diagnosis and Management of Polycystic Ovary Syndrome (PCOS). In Endocrinology and Diabetes: Case Studies, Questions and Commentaries; Ajjan, R., Orme, S.M., Eds.; Springer: London, UK, 2015; pp. 99–113. [Google Scholar]
- Kyrou, I.; Karteris, E.; Robbins, T.; Chatha, K.; Drenos, F.; Randeva, H.S. Polycystic ovary syndrome (PCOS) and COVID-19: An overlooked female patient population at potentially higher risk during the COVID-19 pandemic. BMC Med. 2020, 18, 1–10. [Google Scholar] [CrossRef]
- The Rotterdam ESHRE; ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar]
- Kakoly, N.S.; Khomami, M.B.; Joham, A.E.; Cooray, S.D.; Misso, M.L.; Norman, R.J.; Moran, L.J. Ethnicity, obesity and the prevalence of impaired glucose tolerance and type 2 diabetes in PCOS: A systematic review and meta-regression. Hum. Reprod. Update 2018, 24, 455–467. [Google Scholar] [CrossRef]
- Kahal, H.; Kyrou, I.; Uthman, O.A.; Brown, A.; Johnson, S.; Wall, P.D.; Randeva, H.S. The prevalence of obstructive sleep apnoea in women with polycystic ovary syndrome: A systematic review and meta-analysis. Sleep Breath. 2020, 24, 339–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Norman, R.J. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [Green Version]
- Dokras, A.; Saini, S.; Gibson-Helm, M.; Schulkin, J.; Cooney, L.; Teede, H. Gaps in knowledge among physicians regarding diagnostic criteria and management of polycystic ovary syndrome. Fertil. Steril. 2017, 107, 1380–1386. [Google Scholar] [CrossRef] [Green Version]
- Gibson-Helm, M.; Dokras, A.; Karro, H.; Piltonen, T.; Teede, H.J. Knowledge and Practices Regarding Polycystic Ovary Syndrome among Physicians in Europe, North America, and Internationally: An Online Questionnaire-Based Study. Semin. Reprod. Med. 2018, 36, 19–27. [Google Scholar] [CrossRef]
- Moin, A.S.M.; Sathyapalan, T.; Butler, A.E.; Atkin, S.L. Vitamin D Association With Macrophage-Derived Cytokines in Polycystic Ovary Syndrome: An Enhanced Risk of COVID-19 Infection? Front. Endocrinol. 2021, 12, 638621. [Google Scholar] [CrossRef]
- Subramanian, A.; Anand, A.; Adderley, N.J.; Okoth, K.; Toulis, K.A.; Gokhale, K.; Nirantharakumar, K. Increased COVID-19 infections in women with polycystic ovary syndrome: A population-based study. Eur. J. Endocrinol. 2021, 184, 637–645. [Google Scholar] [CrossRef]
- Snyder, B.S. The lived experience of women diagnosed with polycystic ovary syndrome. J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Kitzinger, C.; Willmott, J. ‘The thief of womanhood’: Women’s experience of polycystic ovarian syndrome. Soc. Sci. Med. 2002, 54, 349–361. [Google Scholar] [CrossRef]
- Hillman, S.C.; Bryce, C.; Caleyachetty, R.; Dale, J. Women’s experiences of diagnosis and management of polycystic ovary syndrome: A mixed-methods study in general practice. Br. J. Gen. Pract. 2020, 70, e322–e329. [Google Scholar] [CrossRef] [PubMed]
- Hadjiconstantinou, M.; Mani, H.; Patel, N.; Levy, M.; Davies, M.; Khunti, K.; Stone, M. Understanding and supporting women with polycystic ovary syndrome: A qualitative study in an ethnically diverse UK sample. Endocr. Connect. 2017, 6, 323–330. [Google Scholar] [CrossRef]
- Crete, J.; Adamshick, P. Managing Polycystic Ovary Syndrome: What Our Patients Are Telling Us. J. Holist. Nurs. 2011, 29, 256–266. [Google Scholar] [CrossRef]
- Kite, C.; Atkinson, L.; McGregor, G.; Clark, C.C.; Brown, J.E.; Kyrou, I.; Randeva, H.S. Sleep disruption and depression, stress and anxiety levels in women with polycystic ovary syndrome (PCOS) during the lockdown measures for COVID-19 in the UK. Front. Glob. Women’s Health 2021, 2. [Google Scholar] [CrossRef]
- Pfaff, K.A.; Baxter, P.E.; Jack, S.M.; Ploeg, J. Exploring new graduate nurse confidence in interprofessional collaboration: A mixed methods study. Int. J. Nurs. Stud. 2014, 51, 1142–1152. [Google Scholar] [CrossRef]
- Musselwhite, K.; Cuff, L.; McGregor, L.; King, K.M. The telephone interview is an effective method of data collection in clinical nursing research: A discussion paper. Int. J. Nurs. Stud. 2007, 44, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Groarke, J.M.; Berry, E.; Graham-Wisener, L.; McKenna-Plumley, P.E.; McGlinchey, E.; Armour, C. Loneliness in the UK during the COVID-19 pandemic: Cross-sectional results from the COVID-19 Psychological Wellbeing Study. PLoS ONE 2020, 15, e0239698. [Google Scholar] [CrossRef]
- Williams, S.N.; Armitage, C.J.; Tampe, T.; Dienes, K. Public perceptions and experiences of social distancing and social isolation during the COVID-19 pandemic: A UK-based focus group study. BMJ Open 2020, 10, e039334. [Google Scholar] [CrossRef] [PubMed]
- Grey, E.; Solomon-Moore, E.; Lambert, J.; Gillison, F.; Townsend, N.; Griffin, T. Lockdown lifestyles: A mixed methods study exploring the impact of COVID-19 prevention measures on diet, physical activity and mental health in the UK adult population. In Proceedings of the Annual General Meeting of the UK Society of Behavioural Medicine (Virtual), Online, 13–14 January 2021. [Google Scholar]
- Tay, C.T.; Teede, H.J.; Hill, B.; Loxton, D.; Joham, A.E. Increased prevalence of eating disorders, low self-esteem, and psychological distress in women with polycystic ovary syndrome: A community-based cohort study. Fertil. Steril. 2019, 112, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Smith, C.A.; Costello, M.F.; MacMillan, F.; Moran, L.; Ee, C. Barriers and facilitators to weight management in overweight and obese women living in Australia with PCOS: A qualitative study. BMC Endocr. Disord. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Institute, M.G. The Future of Work after COVID-19. 2021. Available online: https://www.mckinsey.com/featured-insights/future-of-work/the-future-of-work-after-covid-19 (accessed on 15 July 2021).
- Wood, S.J.; Michaelides, G.; Inceoglu, I.; Hurren, E.T.; Daniels, K.; Niven, K. Homeworking, well-being and the Covid-19 pandemic: A diary study. Int. J. Environ. Res. Public Health 2021, 18, 7575. [Google Scholar] [CrossRef]
- Damone, A.L.; Joham, A.E.; Loxton, D.; Earnest, A.; Teede, H.J.; Moran, L.J. Depression, anxiety and perceived stress in women with and without PCOS: A community-based study. Psychol. Med. 2019, 49, 1510–1520. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W. Northwell COVID-19 Research Consortium. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Tomlinson, J.; Pinkney, J.; Adams, L.; Stenhouse, E.; Bendall, A.; Corrigan, O.; Letherby, G. The diagnosis and lived experience of polycystic ovary syndrome: A qualitative study. J. Adv. Nurs. 2017, 73, 2318–2326. [Google Scholar] [CrossRef]
- Tippett, A. Life on pause: An. analysis of UK fertility patients’ coping mechanisms after the cancellation of fertility treatment due to COVID-19. J. Health Psychol. 2021. [Google Scholar] [CrossRef]
- Grabowski, D.; Overgaard, M.; Meldgaard, J.; Johansen, L.B.; Willaing, I. Disrupted Self-Management and Adaption to New Diabetes Routines: A Qualitative Study of How People with Diabetes Managed Their Illness during the COVID-19 Lockdown. Diabetology 2021, 2, 1–15. [Google Scholar] [CrossRef]
- Grannell, A.; le Roux, C.W.; McGillicuddy, D. “I am terrified of something happening to me” The lived experience of people with obesity during the COVID-19 pandemic. Clin. Obes. 2020, 10, e12406. [Google Scholar] [CrossRef]
- Gillard, S.; Dare, C.; Hardy, J.; Nyikavarand, P.; Rowan, O.R.; Shah, P.; BirkeN, M.; Foye, U.; Ocloo, J.; Pearce, E.; et al. Experiences of living with mental health problems during the COVID-19 pandemic in the UK: A coproduced, participatory qualitative interview study. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 1–11. [Google Scholar] [CrossRef]
- Burton, A.; McKinlay, A.; Aughterson, H.; Fancourt, D. Impact of the Covid-19 pandemic on the mental health and wellbeing of adults with mental health conditions in the UK: A qualitative interview study. medRxiv 2020. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, U.C.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atkinson, L.; Kite, C.; McGregor, G.; James, T.; Clark, C.C.T.; Randeva, H.S.; Kyrou, I. Uncertainty, Anxiety and Isolation: Experiencing the COVID-19 Pandemic and Lockdown as a Woman with Polycystic Ovary Syndrome (PCOS). J. Pers. Med. 2021, 11, 952. https://doi.org/10.3390/jpm11100952
Atkinson L, Kite C, McGregor G, James T, Clark CCT, Randeva HS, Kyrou I. Uncertainty, Anxiety and Isolation: Experiencing the COVID-19 Pandemic and Lockdown as a Woman with Polycystic Ovary Syndrome (PCOS). Journal of Personalized Medicine. 2021; 11(10):952. https://doi.org/10.3390/jpm11100952
Chicago/Turabian StyleAtkinson, Lou, Chris Kite, Gordon McGregor, Tamsin James, Cain C. T. Clark, Harpal S. Randeva, and Ioannis Kyrou. 2021. "Uncertainty, Anxiety and Isolation: Experiencing the COVID-19 Pandemic and Lockdown as a Woman with Polycystic Ovary Syndrome (PCOS)" Journal of Personalized Medicine 11, no. 10: 952. https://doi.org/10.3390/jpm11100952
APA StyleAtkinson, L., Kite, C., McGregor, G., James, T., Clark, C. C. T., Randeva, H. S., & Kyrou, I. (2021). Uncertainty, Anxiety and Isolation: Experiencing the COVID-19 Pandemic and Lockdown as a Woman with Polycystic Ovary Syndrome (PCOS). Journal of Personalized Medicine, 11(10), 952. https://doi.org/10.3390/jpm11100952