
Prognostic Value of C-Reactive Protein to Lymphocyte Ratio (CLR) in Emergency Department Patients with SARS-CoV-2 Infection

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
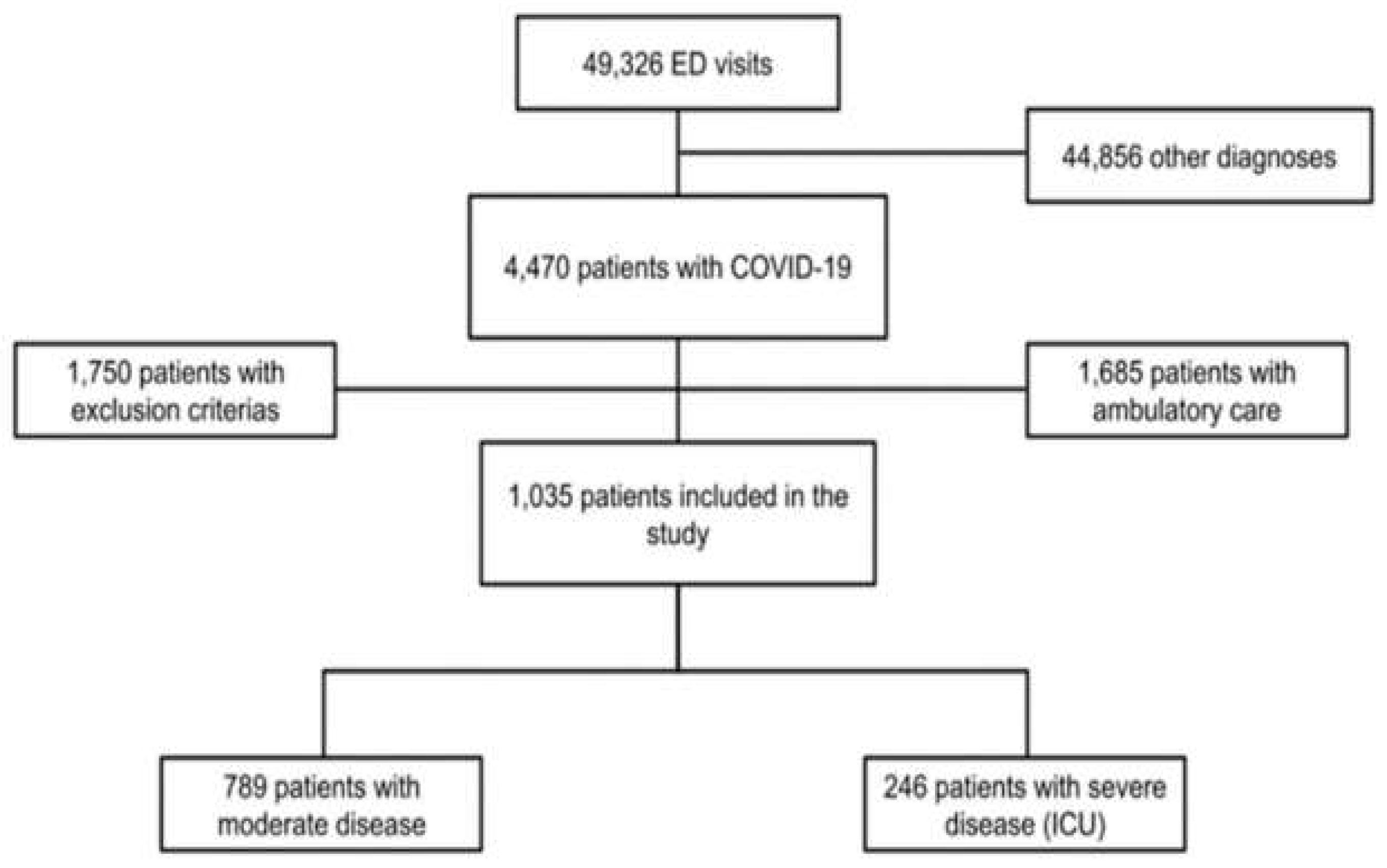
2.1. Study Population and Settings
2.2. Data Collection
2.3. Ethics
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Biochemical Factors Associated COVID-19 Severity
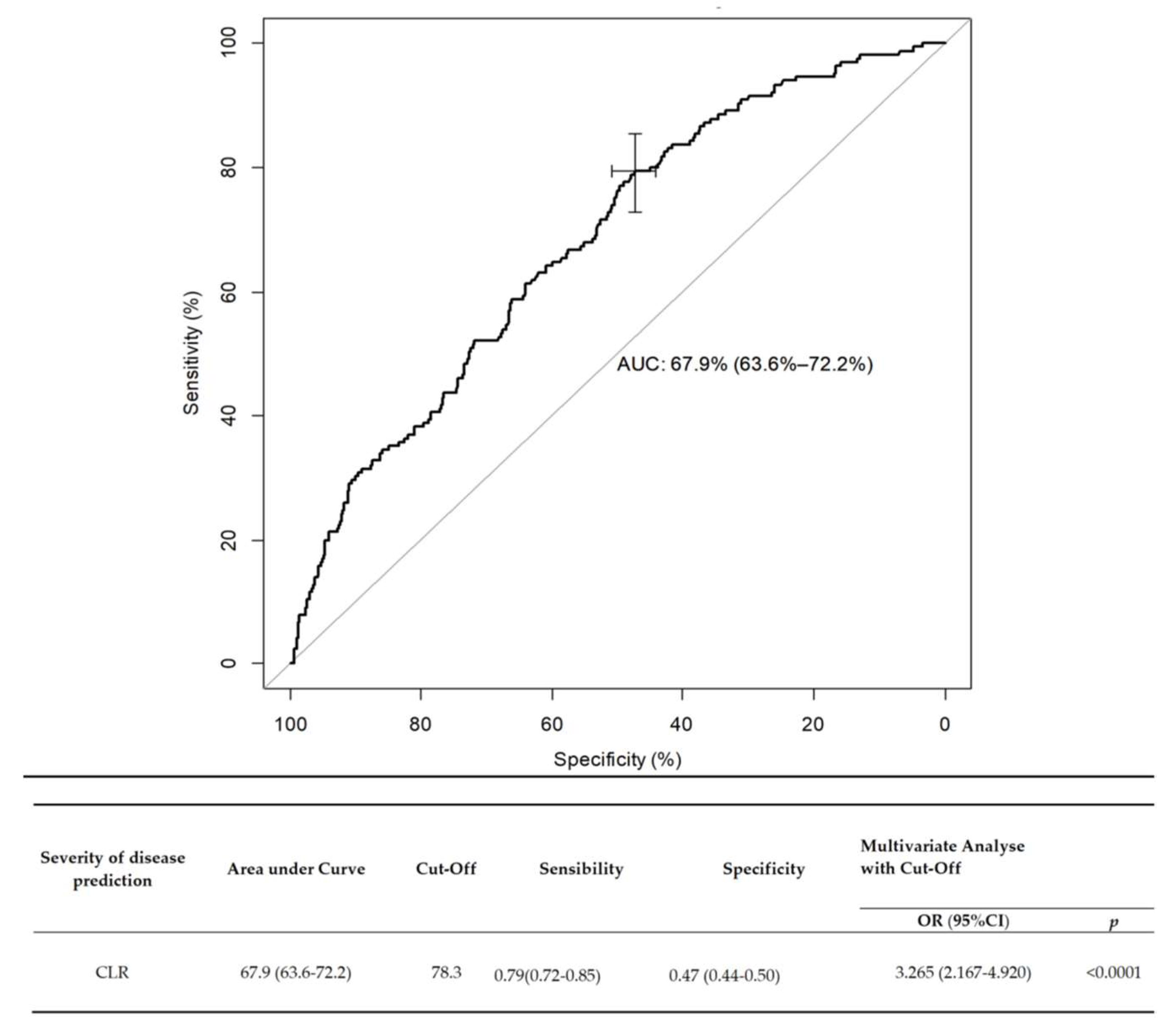
3.3. Factors Predicting COVID-19 Severity
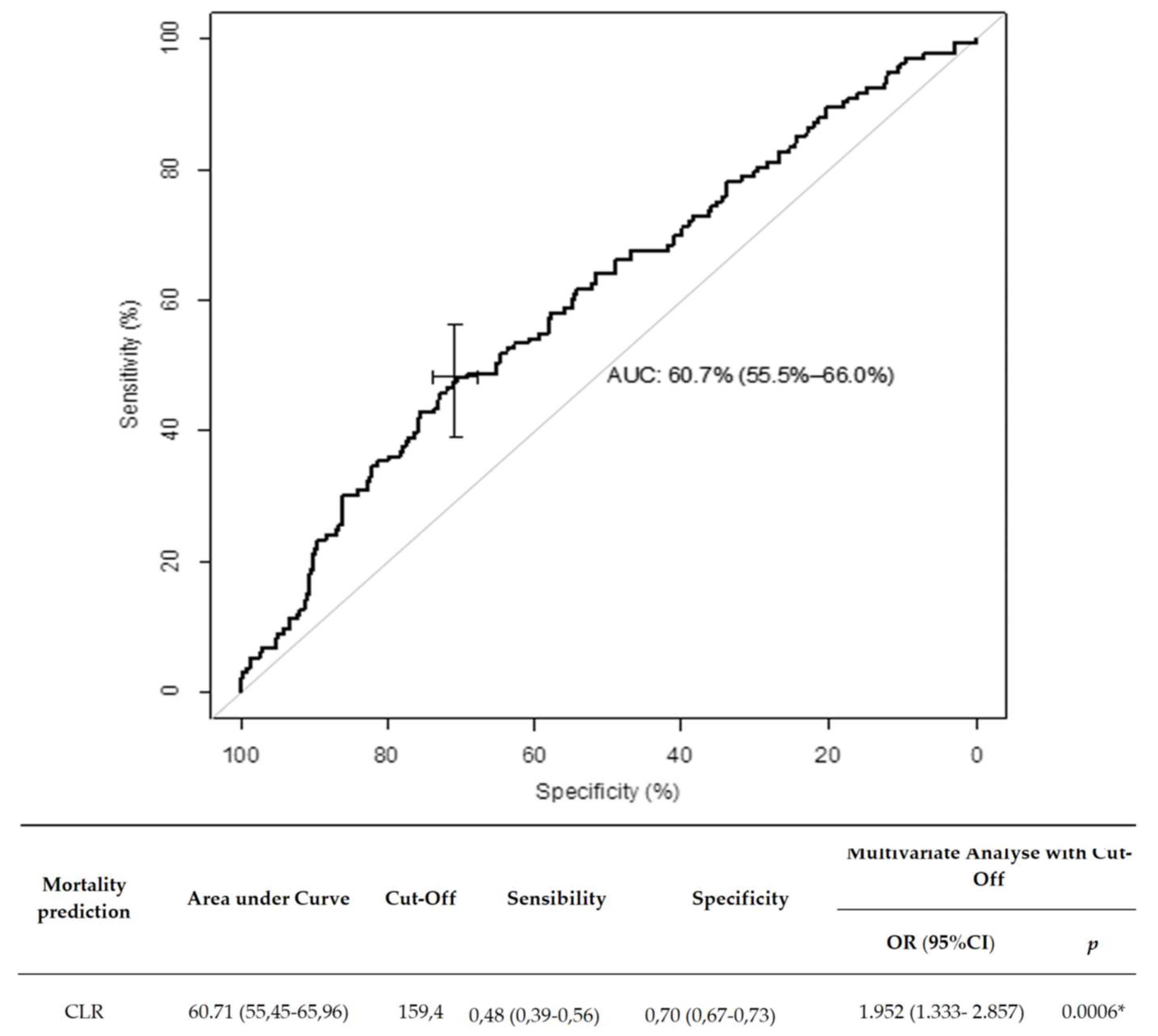
3.4. Biochemical Factors Associated with COVID-19 Mortality
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mulchandani, R.; Lyngdoh, T.; Kakkar, A.K. Deciphering the COVID-19 cytokine storm: Systematic review and meta-analysis. Eur. J. Clin. Investig. 2021, 51, e13429. [Google Scholar] [CrossRef]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Plebani, M. Laboratory abnormalities in patients with COVID-2019 infection. Clin. Chem. Lab. Med. CCLM 2020, 58, 1131–1134. [Google Scholar] [CrossRef] [Green Version]
- Gong, J.; Dong, H.; Xia, Q.-S.; Huang, Z.-Y.; Wang, D.-K.; Zhao, Y.; Liu, W.-H.; Tu, S.-H.; Zhang, M.-M.; Wang, Q.; et al. Correlation Analysis Between Disease Severity and Inflammation-related Parameters in Patients with COVID-19 Pneumonia. BMC Infect. Dis. 2020, 20, 936. [Google Scholar] [CrossRef]
- Hong, L.-Z.; Shou, Z.-X.; Zheng, D.-M.; Jin, X. The most important biomarker associated with coagulation and inflammation among COVID-19 patients. Mol. Cell. Biochem. 2021, 476, 2877–2885. [Google Scholar] [CrossRef] [PubMed]
- Tjendra, Y.; Al Mana, A.F.; Espejo, A.P.; Akgun, Y.; Millan, N.C.; Gomez-Fernandez, C.; Cray, C. Predicting Disease Severity and Outcome in COVID-19 Patients: A Review of Multiple Biomarkers. Arch. Pathol. Lab. Med. 2020, 144, 1465–1474. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Li, C.K.; Li, K.; Hon, K.L.E.; Ng, M.H.L.; Chan, P.K.S.; Fok, T.F. Hematological findings in SARS patients and possible mechanisms (Review). Int. J. Mol. Med. 2004, 14, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.-L.; Chen, K.-T.; Lai, S.-K.; Kuo, H.-W.; Su, I.-J.; Lin, R.S.; Sung, F.-C. Hematological and Biochemical Factors Predicting SARS Fatality in Taiwan. J. Formos. Med. Assoc. 2006, 105, 439–450. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.-T.; Sheng, W.-H.; Fang, C.-T.; Chen, Y.-C.; Wang, J.-L.; Yu, C.-J.; Chang, S.-C.; Yang, P.-C. Clinical Manifestations, Laboratory Findings, and Treatment Outcomes of SARS Patients. Emerg. Infect. Dis. 2004, 10, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-J.; Dong, X.; Cao, Y.-Y.; Yuan, Y.-D.; Yang, Y.-B.; Yan, Y.-Q.; Akdis, C.A.; Gao, Y.-D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Han, T.; Chen, J.; Hou, C.; Hua, L.; He, S.; Guo, Y.; Zhang, S.; Wang, Y.; Yuan, J.; et al. Clinical and Autoimmune Characteristics of Severe and Critical Cases of COVID-19. Clin. Transl. Sci. 2020, 13, 1077–1086. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Yu, H.; Chen, H.; Qi, W.; Chen, L.; Chen, G.; Yan, W.; Chen, T.; Ning, Q.; Han, M.; et al. Longitudinal changes of inflammatory parameters and their correlation with disease severity and outcomes in patients with COVID-19 from Wuhan, China. Crit. Care 2020, 24, 525. [Google Scholar] [CrossRef]
- Yang, M.; Chen, X.; Xu, Y. A Retrospective Study of the C-Reactive Protein to Lymphocyte Ratio and Disease Severity in 108 Patients with Early COVID-19 Pneumonia from January to March 2020 in Wuhan, China. Med. Sci. Monit. 2020, 26, e926393. [Google Scholar] [CrossRef] [PubMed]
- L’Institut National d’Excellence en Santé et en Services Sociaux (INESSS). COVID-19, Anomalies et Analyses de Laboratoire Chez l’adulte. Available online: https://www.inesss.qc.ca/fileadmin/doc/INESSS/COVID-19/COVID-19_INESSS_Analyses_laboratoires.pdf (accessed on 26 November 2021).
- Cheng, L.; Li, H.; Li, L.; Liu, C.; Yan, S.; Chen, H.; Li, Y. Ferritin in the coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. J. Clin. Lab. Anal. 2020, 34, e23618. [Google Scholar] [CrossRef]
- Quel Est le Rôle de l’Interleukine 1 bêta au Sein de l’immunité? MonSystèmeImmunitaire. Available online: https://www.monsystemeimmunitaire.fr/quel-est-le-role-de-linterleukine-1-beta-au-sein-de-limmunite/ (accessed on 26 November 2021).
- d’Alessandro, M.; Cameli, P.; Refini, R.M.; Bergantini, L.; Alonzi, V.; Lanzarone, N.; Bennett, D.; Rana, G.D.; Montagnani, F.; Scolletta, S.; et al. Serum KL-6 concentrations as a novel biomarker of severe COVID-19. J. Med. Virol. 2020, 92, 2216–2220. [Google Scholar] [CrossRef]
- Ou, W.; Zhou, C.; Zhu, X.; Lin, L.; Xu, Q. Prognostic Significance of Preoperative Lymphocyte-to-C-Reactive Protein Ratio in Patients with Non-Metastatic Colorectal Cancer. OncoTargets Ther. 2021, 14, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Koyuncu, S.; Ismail, O. The role of C-reactive protein to lymphocyte ratio in the differentiation of acute and perforated appendicitis. Ulus. Travma Acil Cerrahi Derg. 2020, 26, 760–764. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Allenbach, Y.; Saadoun, D.; Maalouf, G.; Vieira, M.; Hellio, A.; Boddaert, J.; Gros, H.; Salem, J.E.; Rigon, M.R.; Menyssa, C.; et al. Development of a multivariate prediction model of intensive care unit transfer or death: A French prospective cohort study of hospitalized COVID-19 patients. PLoS ONE 2020, 15, e0240711. [Google Scholar] [CrossRef]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.-Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal Transduct. Target 2020, 5, 33. [Google Scholar] [CrossRef]
- Nahon, M. COVID-19: Mise au Point. Urgences-Online. Available online: https://urgences-serveur.fr/covid-19-mise-au-point.html (accessed on 26 November 2021).
- Turan, D.; Çınarka, H.; Çörtük, M.; Tanrıverdi, E.; Chousein, E.G.U.; Yıldırım, B.Z.; Arslan, M.A.; Sezen, C.B.; Çetinkaya, E. La relation entre les valeurs SII, PLR, LCR, MPV/PLT et le pronostic COVID-19. South. Clin. Ist. Euras. 2021, 32, 109–115. [Google Scholar]
- Ullah, W.; Basyal, B.; Tariq, S.; Almas, T.; Saeed, R.; Roomi, S.; Haq, S.; Madara, J.; Boigon, M.; Haas, D.C.; et al. Lymphocyte-to-C-Reactive Protein Ratio: A Novel Predictor of Adverse Outcomes in COVID-19. J. Clin. Med. Res. 2020, 12, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Cai, X.; Wang, H.; He, G.; Lin, Y.; Lu, B.; Chen, C.; Pan, Y.; Hu, X. Abnormalities of peripheral blood system in patients with COVID-19 in Wenzhou, China. Clin. Chim. Acta 2020, 507, 174–180. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Fantuzzi, G.; Dinarello, C.A. The inflammatory response in interleukin-1β-deficient mice: Comparison with other cytokine-related knock-out mice. J. Leukoc. Biol. 1996, 59, 489–493. [Google Scholar] [CrossRef]
- Gemcioglu, E.; Davutoglu, M.; Catalbas, R.; Karabuga, B.; Kaptan, E.; Aypak, A.; Kalem, A.K.; Özdemir, M.; Yeşilova, N.Y.; Kalkan, E.A.; et al. Predictive values of biochemical markers as early indicators for severe COVID-19 cases in admission. Future Virol. 2021. [Google Scholar] [CrossRef]
- López-Escobar, A.; Madurga, R.; Castellano, J.M.; Velázquez, S.; Suárez Del Villar, R.; Menéndez, J.; Peixoto, A.; Jimeno, S.; Sol Ventura, P.; Ruiz de Aguiar, S. Risk Score for Predicting In-Hospital Mortality in COVID-19 (RIM Score). Diagnostics 2021, 11, 596. [Google Scholar] [CrossRef] [PubMed]
- Painuli, D.; Mishra, D.; Bhardwaj, S.; Aggarwal, M. Forecast and prediction of COVID-19 using machine learning. In Data Science for COVID-19; Academic Press: New York, NY, USA, 2021; pp. 381–397. [Google Scholar]
- Álvarez-Mon, M.; Ortega, M.A.; Gasulla, Ó.; Fortuny-Profitós, J.; Mazaira-Font, F.A.; Saurina, P.; Monserrat, J.; Plana, M.N.; Troncoso, D.; Sanz Morento, J.; et al. A Predictive Model and Risk Factors for Case Fatality of COVID-19. J. Pers. Med. 2021, 11, 36. [Google Scholar] [CrossRef]
- Albarrán-Sánchez, A.; González-Ríos, R.D.; Alberti-Minutti, P.; Noyola-García, M.E.; Contreras-García, C.E.; Anda-Garay, J.C.; Martínez-Ascencio, L.E.; Castillo-López, D.J.; Reyes-Naranjo, L.A.; Guízar-García, L.A.; et al. Association of neutrophil-to-lymphocyte and lymphocyte-to-C-reactive protein ratios with COVID-19-related mortality. GAC Med. Mex. 2020, 156, 553–558. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients n = 1035 | Moderate COVID-19 n = 789 | Severe COVID-19 n = 246 | p | |
|---|---|---|---|---|
| Characteristics | ||||
| Age (years) | 69 (58–79) | 70 (58–81) | 66 (57.3–72) | <0.001 * |
| Gender male | 609 (58.8) | 433 (54.9) | 176 (71.5) | <0.001 * |
| Obesity | 281 (36.9) | 193 (35.0) | 88 (41.9) | 0.076 |
| Comorbidities | ||||
| Hypertension | 587 (56.7) | 453 (57.4) | 134 (54.5) | 0.416 |
| Diabetes mellitus | 275 (26.7) | 202 (25.6) | 73 (26.6) | 0.207 |
| CKD | 237 (23.2) | 199 (25.5) | 38 (15.8) | 0.002 * |
| Cardiovascular disease | 357 (34.5) | 291 (36.9) | 66 (26.8) | 0.004 * |
| Total autonomy | 796 (77.2) | 569 (72.4) | 227 (92.7) | <0.001 * |
| Respiratory disease | 203 (19.6) | 151 (19.1) | 52 (21.1) | 0.490 |
| Laboratory Findings | ||||
| CRP (mg/L) | 81 (39–142.3) | 68 (33–128) | 124 (76–192) | <0.001 * |
| Lymphocyte (×109/L) | 870 (630–1200) | 900 (640–1220) | 780 (590–1122) | 0.003 * |
| CLR | 97.0 (39.3–189.5) | 83.0 (33.3–173.5) | 163.9 (83.8–310) | <0.0001* |
| Outcome | ||||
| Hospital stay (days) | 10 (7–17.3) | 8 (6–12) | 24 (17–38) | <0.001 * |
| Intra-hospital mortality | 139 (13.6) | 82 (10.4) | 57 (24.1) | <0.001 * |
| All | Moderate | Severe | % Missing Data | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|---|---|
| Analysis | Analysis | |||||||
| OR (95% CI) | p | OR (95% CI) | p | |||||
| Lymphocytes (×109/L) | 870 (620–1200) | 890 (630–1210) | 870 (620–1200) | 1.5 | 0.864 (0.618–1.209) | 0.3950 | 1.951 (1.024–3.717) | 0.0422 * |
| CRP (mg/L) | 81 (39–142) | 71 (35–131) | 129.0 (76.0–195.0) | 0.7 | 1.008 (1.006–1.010) | <0.0001 * | 1.009 (1.007–1.011) | <0.0001 * |
| CLR | 97 (39.3–189.5) | 83 (33.3–173.5) | 163.9 (83.8–310.0) | 1.002 (1.001–1.003) | <0.0001 * | 1.001 (1.000–1.002) | 0.0120 * | |
| Alive n = 884 | Died n = 139 | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |||
| Lymphocytes (×109/L) | 0.89 (0.65–1.22) | 0.72 (0.50–1.00) | 0.524 (0.336–0.815) | 0.0042 * | 2.308 (1.286–4.141) | 0.0051 * |
| CRP (mg/L) | 78.5 (37.0–139.0) | 100.0 (56.0–158.0) | 1.003 (1.001–1.005) | 0.0065 * | 1.000 (0.997–1.004) | 0.814 |
| CLR | 90.5 (36.0–177.3) | 136.4 (54.4–259.6) | 1.002 (1.001–1.002) | 0.0001 * | 1.001 (1.000–1.003) | 0.090 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tonduangu, N.; Le Borgne, P.; Lefebvre, F.; Alame, K.; Bérard, L.; Gottwalles, Y.; Cipolat, L.; Gennai, S.; Bilbault, P.; Lavoignet, C.-E.; et al. Prognostic Value of C-Reactive Protein to Lymphocyte Ratio (CLR) in Emergency Department Patients with SARS-CoV-2 Infection. J. Pers. Med. 2021, 11, 1274. https://doi.org/10.3390/jpm11121274
Tonduangu N, Le Borgne P, Lefebvre F, Alame K, Bérard L, Gottwalles Y, Cipolat L, Gennai S, Bilbault P, Lavoignet C-E, et al. Prognostic Value of C-Reactive Protein to Lymphocyte Ratio (CLR) in Emergency Department Patients with SARS-CoV-2 Infection. Journal of Personalized Medicine. 2021; 11(12):1274. https://doi.org/10.3390/jpm11121274
Chicago/Turabian StyleTonduangu, Ndenga, Pierrick Le Borgne, François Lefebvre, Karine Alame, Lise Bérard, Yannick Gottwalles, Lauriane Cipolat, Stéphane Gennai, Pascal Bilbault, Charles-Eric Lavoignet, and et al. 2021. "Prognostic Value of C-Reactive Protein to Lymphocyte Ratio (CLR) in Emergency Department Patients with SARS-CoV-2 Infection" Journal of Personalized Medicine 11, no. 12: 1274. https://doi.org/10.3390/jpm11121274
APA StyleTonduangu, N., Le Borgne, P., Lefebvre, F., Alame, K., Bérard, L., Gottwalles, Y., Cipolat, L., Gennai, S., Bilbault, P., Lavoignet, C.-E., Abensur Vuillaume, L., & on behalf of CREMS Network (Clinical Research in Emergency Medicine and Sepsis) (CLR). (2021). Prognostic Value of C-Reactive Protein to Lymphocyte Ratio (CLR) in Emergency Department Patients with SARS-CoV-2 Infection. Journal of Personalized Medicine, 11(12), 1274. https://doi.org/10.3390/jpm11121274