
The Assisi Think Tank Meeting Breast Large Database for Standardized Data Collection in Breast Cancer—ATTM.BLADE

 ,
,  ,
, 
 ,
,  , ,
, ,  ,
, 
 , and
, and 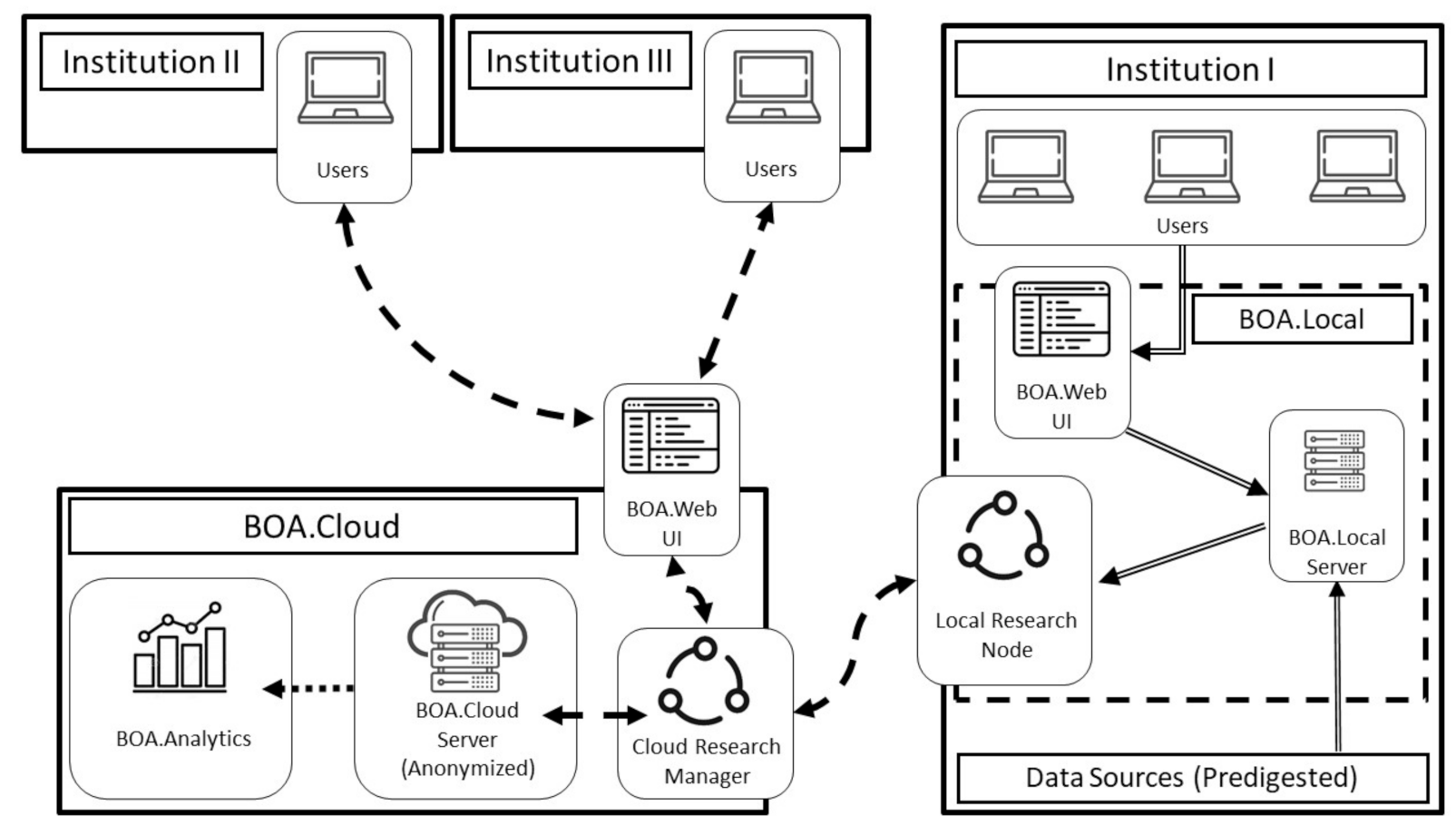{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
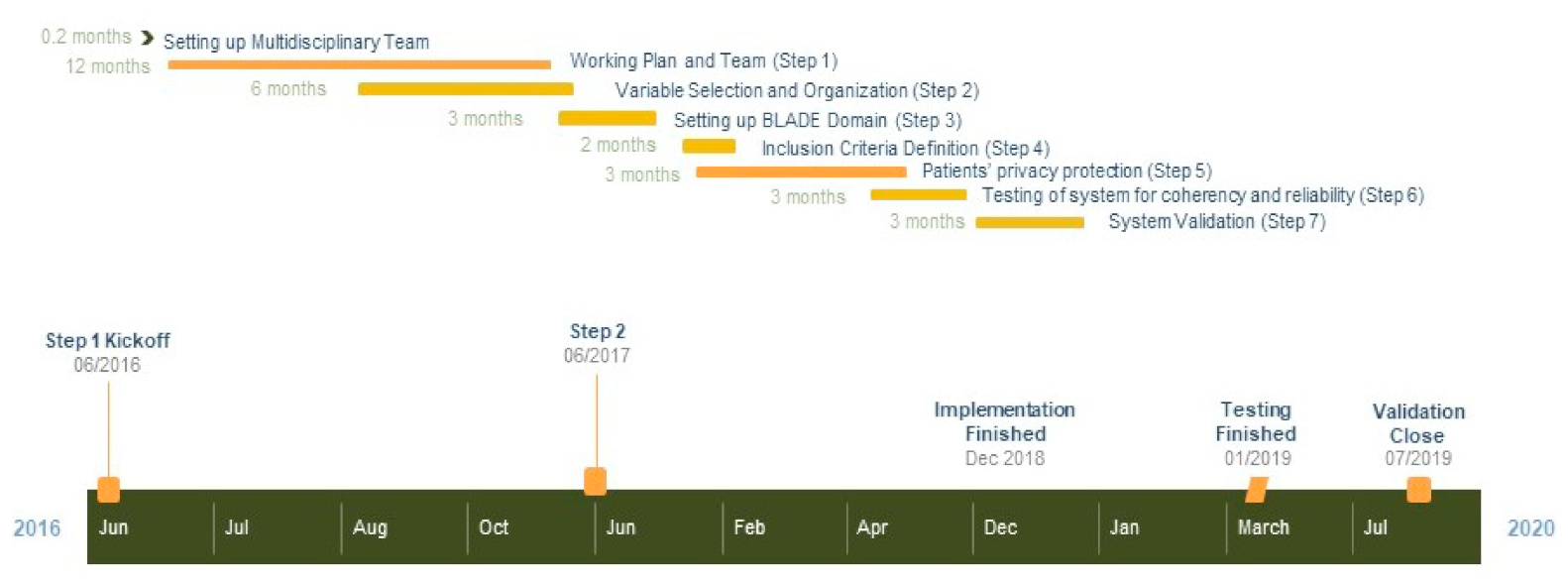
2. Materials and Methods
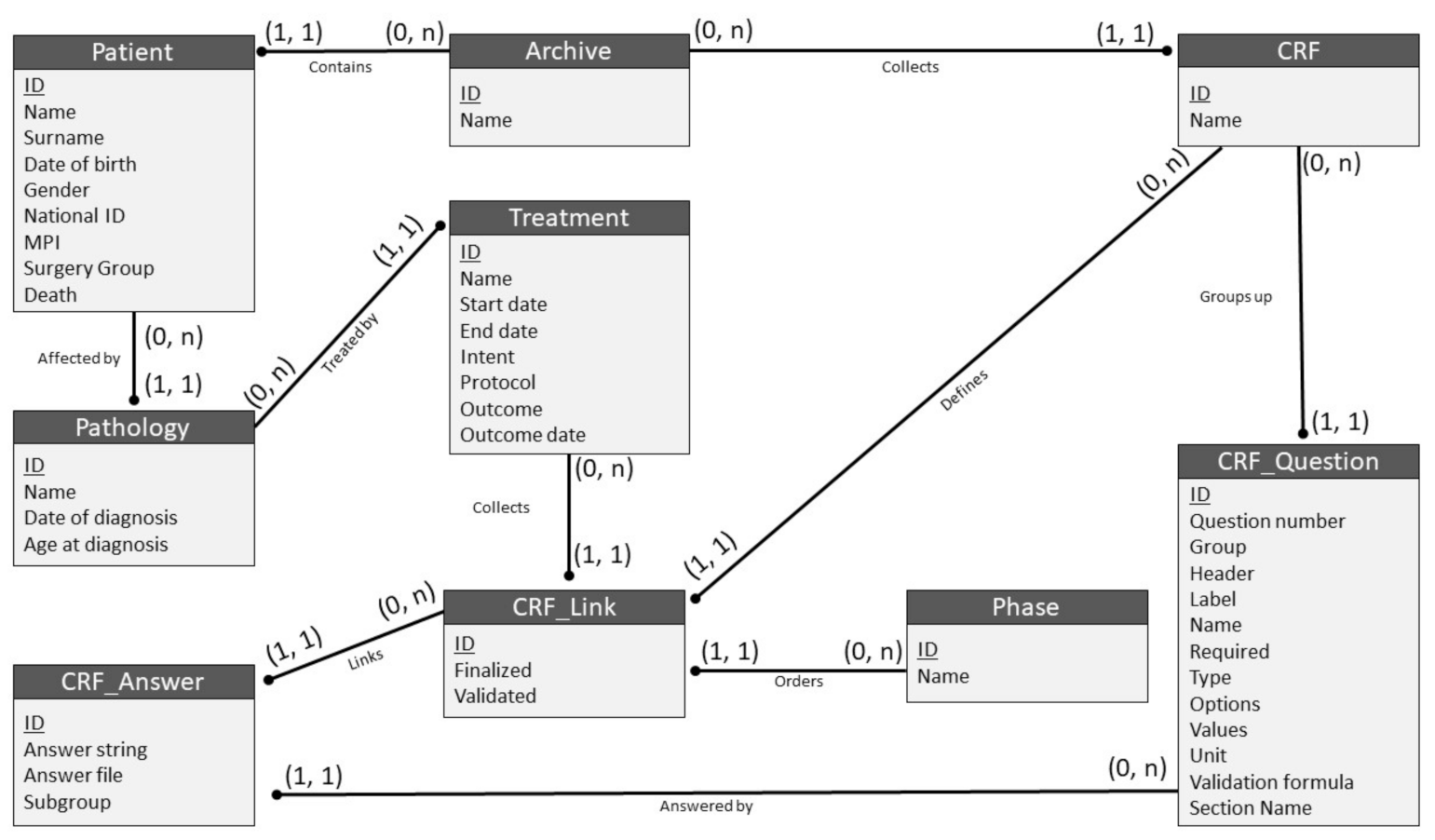
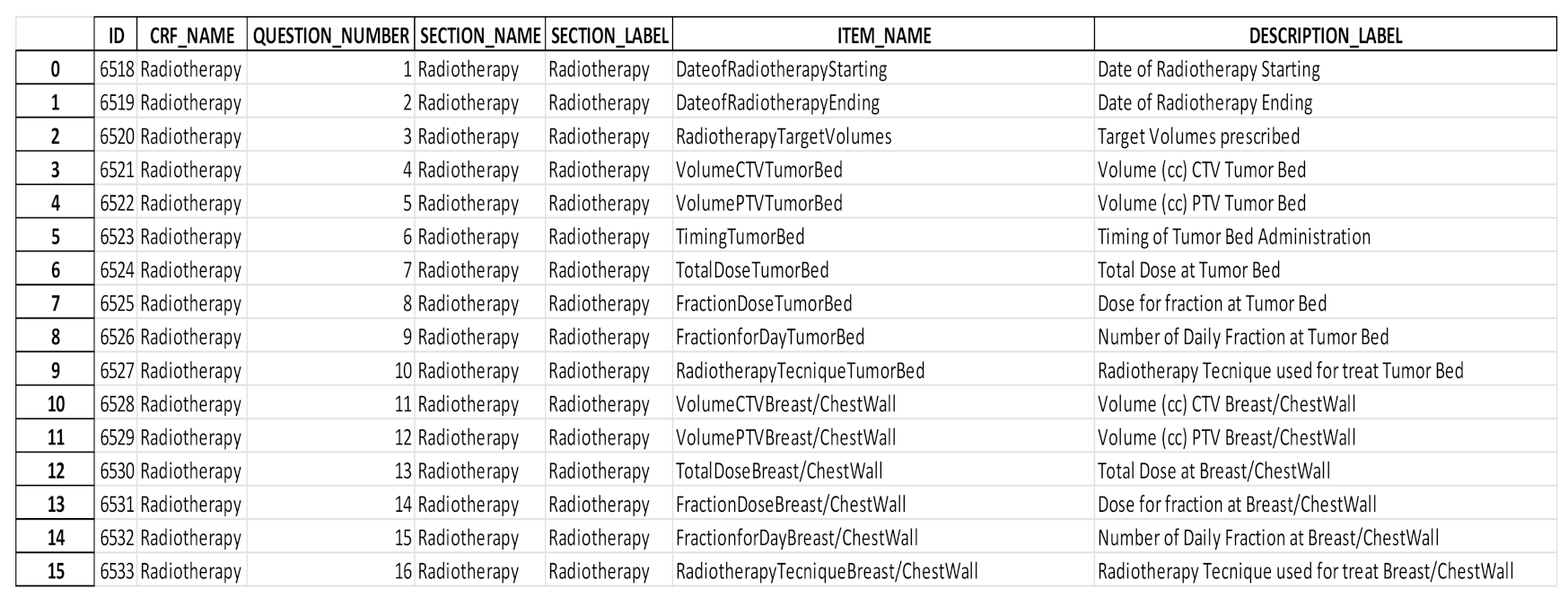
2.1. Data Collection Methodology
2.2. Testing the BLADE Domain for Coherency and Reliability (Step 6)
- −
- Data pseudo-anonymization and encryption;
- −
- Permanent assurance of confidentiality, integrity, availability, and resiliency of treatment systems and services;
- −
- Prompt restoration of availability and access to personal data in case of physical or technical accident;
- −
- Regular tests, verifications, and assessments of technical and organizational effectiveness measures to ensure data safety.
2.3. System Validation (Step 7)
- Clinical-, treatment-, and tumor-related data: age, date of diagnosis, primary systemic treatments, histological sub-type, receptor status, multi-focality, and clinical and pathological stages;
- Reconstruction data: type of reconstructive surgery, prosthesis material, time to prosthesis-related complication (TPC), time to prosthesis reoperation (TPR), and ratio of TPC/time from reconstructive surgery;
- Dosimetric data referring to the chest wall: prescribed dose, conformity index, homogeneity index, and V95% and V105%.
- −
- Uploading at least 80% of chart data by the data manager without physician assistance;
- −
- Physician correction of <20% of uploaded data;
- −
- Extraction of at least 80% of data for statistical analyses;
- −
- Joint physician and statistician correction of <20% of extracted data;
- −
- Performance of at least 80% of planned statistical analyses on RStudio©.
3. Results
3.1. Setting up BLADE (June 2016)
3.2. BLADE Data Safety Tests (January 2019)
3.3. Validation (February–July 2019)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Information to Join ATTM.BLADE Network and/or Propose Research Project
References
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer in Women: Burden and Trends. Cancer Epidemiol. Biomark. Prev. 2017, 26, 444–457. [Google Scholar] [CrossRef] [Green Version]
- Martin, E.; Pourtau, L.; Di Palma, M.; Delaloge, S. New oral targeted therapies for metastatic breast cancer disrupt the traditional patients’ management-A healthcare providers’ view. Eur. J. Cancer Care 2016, 26, e12624. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Hu, T.; Chen, Y. Small-arc volumetric-modulated arc therapy: A new approach that is superior to fixed-field IMRT in optimizing dosimetric and treatment-relevant parameters for patients undergoing whole-breast irradiation following breast-conserving surgery. Medicine 2016, 95, e4609. [Google Scholar] [CrossRef] [PubMed]
- Blaschke, S.-M.; Gough, K.C.; Chua, B.H.; Francis, P.A.; Cockerell, R.; Drosdowsky, A.F.; Sheeran, L.; Krishnasamy, M. Implementation of a Multidisciplinary Model of Care for Women with Metastatic Breast Cancer: Challenges and Lessons Learned. Clin. Breast Cancer 2019, 19, e327–e336. [Google Scholar] [CrossRef]
- Di Paolo, A.; Sarkozy, F.; Ryll, B.; Siebert, U. Personalized medicine in Europe: Not yet personal enough? BMC Health Serv. Res. 2017, 17, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burock, S.; Meunier, F.; Lacombe, D. How can innovative forms of clinical research contribute to deliver affordable cancer care in an evolving health care environment? Eur. J. Cancer 2013, 49, 2777–2783. [Google Scholar] [CrossRef]
- Duburs, G.; Neibecker, D.; Žarković, N. Chemistry and personalized medicine–the research and development future of Europe. Croat. Med. J. 2012, 53, 291–293. [Google Scholar] [CrossRef] [Green Version]
- Thall, P.F. Ethical issues in oncology biostatistics. Stat. Methods Med. Res. 2002, 11, 429–448. [Google Scholar] [CrossRef] [PubMed]
- Meldolesi, E.; Van Soest, J.; Damiani, A.; Dekker, A.; Alitto, A.R.; Campitelli, M.; DiNapoli, N.; Gatta, R.; Gambacorta, M.A.; Lanzotti, V.; et al. Standardized data collection to build prediction models in oncology: A prototype for rectal cancer. Future Oncol. 2016, 12, 119–136. [Google Scholar] [CrossRef] [Green Version]
- Lambin, P.; Roelofs, E.; Reymen, B.; Velazquez, E.R.; Buijsen, J.; Zegers, C.M.; Carvalho, S.; Leijenaar, R.T.; Nalbantov, G.; Oberije, C.; et al. ‘Rapid Learning health care in oncology’—An approach towards decision support systems enabling customised radiotherapy. Radiother. Oncol. 2013, 109, 159–164. [Google Scholar] [CrossRef]
- Lambin, P.; Zindler, J.; Vanneste, B.; Van De Voorde, L.; Jacobs, M.; Eekers, D.; Peerlings, J.; Reymen, B.; LaRue, R.T.H.M.; Deist, T.M.; et al. Modern clinical research: How rapid learning health care and cohort multiple randomised clinical trials complement traditional evidence based medicine. Acta Oncol. 2015, 54, 1289–1300. [Google Scholar] [CrossRef] [Green Version]
- Guihard, S.; Thariat, J.; Clavier, J.-B. Métadonnées et leurs applications possibles en radiothérapie. Bull. Cancer 2017, 104, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Aristei, C.; Kaidar-Person, O.; Arenas, M.; Coles, C.; Offersen, B.V.; Bourgier, C.; Frezza, G.; Leonardi, M.C.; Valentini, V.; Poortmans, P.M.P. The 2016 Assisi Think Tank Meeting on breast cancer: White paper. Breast Cancer Res. Treat. 2016, 160, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Meldolesi, E.; Van Soest, J.; DiNapoli, N.; Dekker, A.; Damiani, A.; Gambacorta, M.A.; Valentini, V. An umbrella protocol for standardized data collection (SDC) in rectal cancer: A prospective uniform naming and procedure convention to support personalized medicine. Radiother. Oncol. 2014, 112, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Meldolesi, E.; Van Soest, J.; Alitto, A.R.; Autorino, R.; DiNapoli, N.; Dekker, A.; Gambacorta, M.A.; Gatta, R.; Tagliaferri, L.; Damiani, A.; et al. VATE: VAlidation of high TEchnology based on large database analysis by learning machine. Colorectal Cancer 2014, 3, 435–450. [Google Scholar] [CrossRef] [Green Version]
- Alitto, A.R.; Gatta, R.; Vanneste, B.; Vallati, M.; Meldolesi, E.; Damiani, A.; Lanzotti, V.; Mattiucci, G.C.; Frascino, V.; Masciocchi, C.; et al. PRODIGE: PRediction models in prOstate cancer for personalized meDIcine challenGE. Futur. Oncol. 2017, 13, 2171–2181. [Google Scholar] [CrossRef]
- Wilson, G. Gantt charts: A centenary appreciation. Eur. J. Oper. Res. 2003, 149, 430–437. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Breast Cancer; NCCN: Plymouth Meeting, PA, USA, 2020. [Google Scholar]
- Smith, B.D.; Bellon, J.R.; Blitzblau, R.; Freedman, G.; Haffty, B.; Hahn, C.; Halberg, F.; Hoffman, K.; Horst, K.; Moran, J.; et al. Radiation therapy for the whole breast: Executive summary of an American Society for Radiation Oncology (ASTRO) evidence-based guideline. Pr. Radiat. Oncol. 2018, 8, 145–152. [Google Scholar] [CrossRef] [Green Version]
- GRUPPO DI COORDINAMENTO AIRO MAMMELLA Triennio 2017–2019, Best Clinical Practice Nella Radioterapia dei Tumori Della Mammella; Sede Legale: Milano, Italy, 2019. Available online: radioterapiaitalia.it (accessed on 1 February 2021).
- Baumann, B. Create and Modify Case Report Forms (CRFs). 24 March 2014. Available online: https://docs.openclinica.com/3.1/study-setup/build-study/create-case-report-forms-crfs (accessed on 10 June 2016).
- Guidelines 2/2019 on the Processing of Personal Data under Article 6(1)(b) GDPR in the Context of the Provision of Online Services to Data Subjects-Version Adopted after Public Consultation. Available online: https://edpb.europa.eu/our-work-tools/our-documents/guidelines/guidelines-22019-processing-personal-data-under-article-61b_en (accessed on 31 October 2018).
- Article 32, EU GDPR, “Security of Processing”. Available online: http://www.privacy-regulation.eu/en/32.htm (accessed on 31 October 2018).
- Liou, D.-M.; Chang, W.-P. Applying Data Mining for the Analysis of Breast Cancer Data. Methods Mol. Biol. 2014, 1246, 175–189. [Google Scholar] [CrossRef]
- Melo, M.T.D.; Gonçalves, V.H.L.; Costa, H.D.R.; Braga, D.S.; Gomide, L.B.; Alves, C.S.; Brasil, L.M. OntoMama: An Ontology Applied to Breast Cancer. Stud. Health Technol. Inform. 2015, 216, 1104. [Google Scholar]
- Zhu, Q.; Tao, C.; Shen, F.; Chute, C.G. Exploring the Pharmacogenomics Knowledge Base (Pharmgkb) for Repositioning Breast Cancer Drugs by Leveraging Web Ontology Language (Owl) and Cheminformatics Approaches. In Pac Symp Biocomputing; World Scientific: Singapore, 2013; pp. 172–182. [Google Scholar]
- Papatheodorou, I.; METABRIC Group; Crichton, C.; Morris, L.; Maccallum, P.; Davies, J.; Brenton, J.D.; Caldas, C. A metadata approach for clinical data management in translational genomics studies in breast cancer. BMC Med. Genom. 2009, 2, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abidi, S.R.; Abidi, S.S.; Hussain, S.; Shepherd, M. Ontology-based Modeling of Clinical Practice Guidelines: A Clinical Decision Support System for Breast Cancer Follow-up Interventions at Primary Care Settings. Stud. Health Technol. Inform. 2007, 129, 845–849. [Google Scholar] [PubMed]
- Wu, S.-G.; Li, H.; Tang, L.-Y.; Sun, J.-Y.; Zhang, W.-W.; Li, F.-Y.; Chen, Y.-X.; He, Z.-Y. The effect of distant metastases sites on survival in de novo stage-IV breast cancer: A SEER database analysis. Tumor Biol. 2017, 39, 101042831770508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murthy, V.; Pawar, S.; Chamberlain, R.S. Disease Severity, Presentation, and Clinical Outcomes Among Adolescents With Malignant Breast Neoplasms: A 20-Year Population-Based Outcomes Study From the SEER Database (1973–2009). Clin. Breast Cancer 2017, 17, 392–398. [Google Scholar] [CrossRef]
- Liu, J.; Su, M.; Hong, S.; Gao, H.; Zheng, X.; Wang, S. Nomogram predicts survival benefit from preoperative radiotherapy for non-metastatic breast cancer: A SEER-based study. Oncotarget 2017, 8, 49861–49868. [Google Scholar] [CrossRef] [Green Version]
- Plasilova, M.L.; Hayse, B.; Killelea, B.K.; Horowitz, N.R.; Chagpar, A.B.; Lannin, D.R. Features of triple-negative breast cancer. Medicine 2016, 95, e4614. [Google Scholar] [CrossRef]
- Diwanji, T.P.; Molitoris, J.K.; Chhabra, A.M.; Snider, J.W.; Bentzen, S.M.; Tkaczuk, K.H.; Rosenblatt, P.Y.; Kesmodel, S.B.; Bellavance, E.C.; Cohen, R.J.; et al. Utilization of hypofractionated whole-breast radiation therapy in patients receiving chemotherapy: A National Cancer Database analysis. Breast Cancer Res. Treat. 2017, 165, 445–453. [Google Scholar] [CrossRef]
- Marazzi, F.; Tagliaferri, L.; Masiello, V.; Moschella, F.; Colloca, G.F.; Corvari, B.; Sanchez, A.M.; Capocchiano, N.D.; Pastorino, R.; Iacomini, C.; et al. GENERATOR Breast DataMart—The Novel Breast Cancer Data Discovery System for Research and Monitoring: Preliminary Results and Future Perspectives. J. Pers. Med. 2021, 11, 65. [Google Scholar] [CrossRef] [PubMed]
- Montero-Luis, A.; Aristei, C.; Meattini, I.; Arenas, M.; Boersma, L.; Bourgier, C.; Coles, C.; Cutuli, B.; Falcinelli, L.; Kaidar-Person, O.; et al. The Assisi Think Tank Meeting Survey of post-mastectomy radiation therapy in ductal carcinoma in situ: Suggestions for routine practice. Crit. Rev. Oncol. 2019, 138, 207–213. [Google Scholar] [CrossRef]
- Arenas, M.; Selek, U.; Kaidar-Person, O.; Perrucci, E.; Luis, A.M.; Boersma, L.; Coles, C.; Offersen, B.; Meattini, I.; Bölükbaşı, Y.; et al. The 2018 assisi think tank meeting on breast cancer: International expert panel white paper. Crit. Rev. Oncol. 2020, 151, 102967. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marazzi, F.; Masiello, V.; Masciocchi, C.; Merluzzi, M.; Saldi, S.; Belli, P.; Boldrini, L.; Capocchiano, N.D.; Di Leone, A.; Magno, S.; et al. The Assisi Think Tank Meeting Breast Large Database for Standardized Data Collection in Breast Cancer—ATTM.BLADE. J. Pers. Med. 2021, 11, 143. https://doi.org/10.3390/jpm11020143
Marazzi F, Masiello V, Masciocchi C, Merluzzi M, Saldi S, Belli P, Boldrini L, Capocchiano ND, Di Leone A, Magno S, et al. The Assisi Think Tank Meeting Breast Large Database for Standardized Data Collection in Breast Cancer—ATTM.BLADE. Journal of Personalized Medicine. 2021; 11(2):143. https://doi.org/10.3390/jpm11020143
Chicago/Turabian StyleMarazzi, Fabio, Valeria Masiello, Carlotta Masciocchi, Mara Merluzzi, Simonetta Saldi, Paolo Belli, Luca Boldrini, Nikola Dino Capocchiano, Alba Di Leone, Stefano Magno, and et al. 2021. "The Assisi Think Tank Meeting Breast Large Database for Standardized Data Collection in Breast Cancer—ATTM.BLADE" Journal of Personalized Medicine 11, no. 2: 143. https://doi.org/10.3390/jpm11020143
APA StyleMarazzi, F., Masiello, V., Masciocchi, C., Merluzzi, M., Saldi, S., Belli, P., Boldrini, L., Capocchiano, N. D., Di Leone, A., Magno, S., Meldolesi, E., Moschella, F., Mulé, A., Smaniotto, D., Terribile, D. A., Tagliaferri, L., Franceschini, G., Gambacorta, M. A., Masetti, R., ... Aristei, C. (2021). The Assisi Think Tank Meeting Breast Large Database for Standardized Data Collection in Breast Cancer—ATTM.BLADE. Journal of Personalized Medicine, 11(2), 143. https://doi.org/10.3390/jpm11020143