
Diet, Obesity, and Depression: A Systematic Review

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
1.1. Diet and Depression
1.2. Depression and Obesity
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
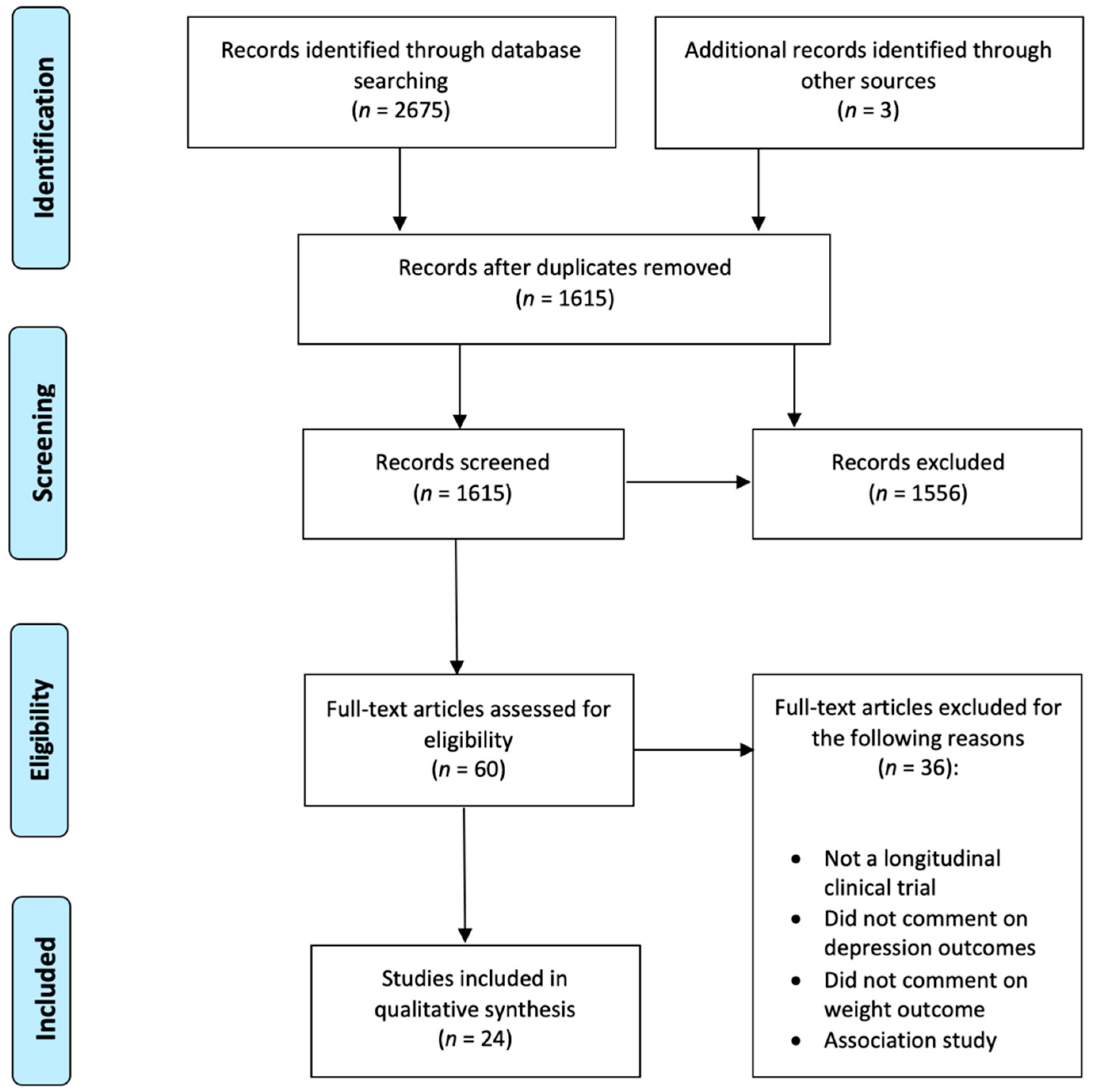
2.3. Study Selection
3. Results
3.1. Characteristics of Included Studies

{kind=link}
| Study | Disease | Sample Size (Recruited) | Excluded Due to Nonadherence to Intervention | Excluded or Withdrawn for Other Reasons | Completed | Diet Intervention | Energy Restricted Diet | Nondieting Control Group | Depression Scale | Gender (M) | Age (Mean ± SD) | Summary | Quality Assessment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bot et al. [30] | Obesity | 1025 | 779 | Multinutrient supplementation + FRBA | No | No | MINI, PHQ-9 | 772 (253) | 46.6 | No significant effect of supplements or FRBA on PHQ scores. | Good | ||
| Breymeyer et al. [28] | Overweight/ Obese vs. healthy | 82 | 82 | Isocaloric HGL and LGL (crossover) | No | No | POMS, CES-D | 41 (41) | Mood disturbance was higher on HGL diet. Significant effect of diet on CES-D score with higher depression score associated with HGL diet. | Good | |||
| Brinkwork, Buckley at al. [31] | Overweight/ Obesity | 106 | 4 | 66 | Energy restricted LCHF vs. HCLF | Yes | No | POMS, BDI | 50 ± 0.8 | Both diet groups achieved significant reduction in weight and depression scores. However, LC group rebounded to baseline levels over time whereas LF group depression scores remained low. | Good | ||
| Brinkworth, Luscombe-Marsh et al. [39] | Obesity + diabetes | 115 | 6 | 32 | 77 | Energy restricted LCHF vs. HCLF | Yes | No | POMS, BDI | 58.5 ± 7.1 | Both diet groups achieved significant decrease in weight, POMS, and BDI scores. | Good | |
| Canheta et al. [47] | Obesity | 149 | 36 | 113 | Brazilian diet vs. extra virgin olive oil vs. both | Yes | Yes | HADS | 109 (20) | 38.9 ± 8.7 | All diet groups achieved significant reduction in depression scores. | Good | |
| Coates et al. [46] | Overweight/ Obese | 151 | 2 | 20 | 128 | Isocaloric AED vs. NF | No | No | POMS | 78 (70) | 65 ± 8 | No reduction in weight or depression scores. | Good |
| Crerand et al. [43] | Obesity | 123 | Meal replacement or balanced deficit diet vs. control (nondieting group) | Yes | Yes | BDI | 123 (0) | Diet group lost significantly more weight and reported significantly greater reduction in depressive symptoms. | Good | ||||
| Fuller et al. [40] | Obesity | 70 | 60 | Diet + exercise (Korean vs. Western hypocaloric) | Yes | No | BDI-II | 44 (36) | 45.5 ± 11.1 | Significant decrease for both groups in weight and BDI scores at end of intervention. | Good | ||
| Galletly et al. [29] | Overweight + PCOS | 25 | LPHC vs. HPLC | Yes | No | HADS | 25 (0) | HPLC: 33 ± 1.2 LPHC: 32 ± 1.2 | HPLC diet resulted in significant reduction in depression scores. No difference in weight loss between diet groups. | Good | |||
| Hadi et al. [49] | Overweight/ Obese | 60 | 0 | 1 | 59 | Synbiotics vs. placebo | No | N/A | DASS-21 | 20 (40) | Synbiotic: 34.5 ± 6 Placebo: 36.6 ± 7.3 | Both groups showed decreased weight and depression scores, however, synbiotic group showed greater improvement compared to placebo. | Good |
| Halyburton et al. [44] | Overweight/ Obese | 121 | 5 | 21 | 95 | Energy restricted LCHF vs. HCLF | Yes | No | POMS, BDI | 95 (0) | LCHF: 50.6 ± 1.1 HCLF: 49.8 ± 1.3 | LCHF significantly greater weight loss than HCLF. Significant reduction in POMS and BDI scores for both diet groups. | Very good |
| Hariri et al. [33] | Overweight/ Obesity | 62 | 62 | Energy restricted diet plus sumac supplement vs. energy restricted diet + placebo | Yes | No | BDI-II | 62 (0) | S: 42 ± 8.44 C: 44 ± 11.8 | Significant reduction in weight and depression in both groups. Sumac supplement group showed significantly more reduction in weight. | Good | ||
| Lutze et al. [41] | Obesity | 117 | 8 | 43 | 66 | Isocaloric HP vs. HCLF | Yes | No | POMS, SF-36 mental health summary | 0 (66) | 49.6 ± 9.2 | No effect of HP vs. HC diet. Both diets resulted in reduced weight and reduced POMS and SF-36 scores. | Good |
| Pedersen et al. [48] | Overweight/ Obesity | 70 | 55 | AIT vs. LED | Yes | No | HADS | 12 (43) | LED mean weight loss: 9.9kg, AIT mean weight loss: 1.6%. No significant change in HADS. | Good | |||
| Raman et al. [34] | Obesity | 80 | 80 | BWL vs. BWL + CRT-O | No | N/A | DASS-21 | 69 (11) | CRT-O: 40.6 ± 7.0 C: 42.2 ± 8.8 | BWL + CRT-O resulted in significantly more weight loss at 3-month follow-up but had no effect on depression scores | Good | ||
| Rodriguez-Lozada et al. [32] | Overweight/ Obese | 305 | 305 | MHP vs. LF | Yes | No | BDI | 213 (92) | 45.3 | Both energy intake restricted diets resulted in reduced weight and depression scores. LF diet had more pronounced effects on depression scores in women. | Good | ||
| Ruusunen et al. [35] | Overweight/ Obese + impaired glucose tolerance | 140 | 140 | Counselling on weight reduction + physical activity | No | N/A | BDI | 81 (59) | 57.7 ± 6.4 | Both groups achieved reductions in weight and depression scores. With participants showing the greatest reduction in weight also showing greater decreases in depression scores. | Good | ||
| Sanchez et al. [45] | Obesity | 105 | 104 | Moderate energy restriction + probiotic | Yes | No | BDI | 60 (45) | 35 ± 10 | Significant decrease in BDI scores in probiotic group compared to placebo. | Good | ||
| Tan et al. [50] | Overweight/ Obesity + insomnia | 73 | 2 | 6 | 49 | Energy restricted diet vs. control | Yes | Yes | Rimon’s brief depression scale | 0 (49) | D: 51 C: 52.6 | Diet group improved sleep time and depression scores. However, depression scores reduced in both groups. | Good |
| Uemura et al. [36] | Obesity | 44 | 44 | Counselling on gut microbiota | No | N/A | CES-D | 44 (0) | I: 62 ± 8.7 C: 63.3 ± 9.1 | BMI, body weight, and CES-D scores decreased significantly after intervention. | Good | ||
| Vaghef-Mehrabany et al. [25] | Obesity + MDD | 62 | 6 | 11 | 45 | 25% weight loss diet + probiotic vs. placebo | Yes | No | BDI-II, HDRS | 62 (0) | Regardless of supplementation group, patients who achieved >1.9kg reduction in weight, showed reduction in HDRS and borderline reduction in BDI-II. Prebiotic supplementation had no effect on depressive symptoms. | Good | |
| Vigna et al. [37] | Overweight/ Obese | 77 | 77 | LCD: Hericium erinaceus vs. control | Yes | No | Zung’s depression scale, SCL-90 | 65 (12) | 53.2 ± 0.7 | H. erinaceus supplementation decreased depression scores. | Very good | ||
| Webber et al. [38] | Overweight/ Obese | 49 | 49 | BWL vs. EBT | No | N/A | CES-D | 41 (8) | 45 ± 7.9 | Both groups showed improvements in BMI and depression scores. | Good | ||
| Wing et al. [42] | Obesity + diabetes | 33 | 2 | 31 | VLCD vs. balanced diet | Yes | No | BDI | 25 (18) | Both weight and BDI scores decreased significantly after intervention. VLCD group had more weight loss. | Fair |
3.2. Study Findings
3.2.1. Effects of Diet Interventions on Obesity and Clinically Diagnosed Depression
3.2.2. Effects of Diet Interventions on Obesity and Depressive Symptoms
Studies of Energy Restricted Diets
Studies on Energy Restricted Diets Plus Pre/Probiotic Supplementation
Studies on Diet Combined with Exercise Intervention
Studies on Counselling (Not Explicitly Calorie Restricted)
4. Discussion
4.1. Summary of the Main Findings
4.2. Possible Mechanisms for Improved Mood after Weight Loss
4.2.1. Physiological Mechanisms
4.2.2. Psychosocial Mechanisms
4.3. Clinical Implications
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agha, M.; Agha, R. The rising prevalence of obesity. Int. J. Surg. Oncol. 2017, 2, e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Q.; He, H.; Yang, J.; Feng, X.; Zhao, F.; Lyu, J. Changes in the global burden of depression from 1990 to 2017: Findings from the Global Burden of Disease study. J. Psychiatr. Res. 2020, 126, 134–140. [Google Scholar] [CrossRef]
- Kotsis, V.; Tsioufis, K.; Antza, C.; Seravalle, G.; Coca, A.; Sierra, C.; Lurbe, E.; Stabouli, S.; Jelakovic, B.; Redon, J.; et al. Obesity and cardiovascular risk: A call for action from the European Society of Hypertension Working Group of Obesity, Diabetes and the High-risk Patient and European Association for the Study of Obesity: Part B: Obesity-induced cardiovascular disease, early prevention strategies and future research directions. J. Hypertens. 2018, 36, 1441–1455. [Google Scholar]
- Penninx, B.W.J.H.; Beekman, A.T.F.; Honig, A.; Deeg, D.J.H.; Schoevers, R.A.; Van Eijk, J.T.M.; van Tilburg, W. Depression and cardiac mortality: Results from a community-based longitudinal study. Arch. Gen. Psychiatry 2001, 58, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Pereira-Miranda, E.; Costa, P.R.F.; Queiroz, V.A.O.; Pereira-Santos, M.; Santana, M.L.P. Overweight and Obesity Associated with Higher Depression Prevalence in Adults: A Systematic Review and Meta-Analysis. J. Am. Coll. Nutr. 2017, 36, 223–233. [Google Scholar] [CrossRef]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.J.H.; Zitman, F.G. Overweight, Obesity, and Depression. Arch. Gen. Psychiatry 2010, 67, 220. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, S.R.; Schuppenies, A.; Wong, M.L.; Licinio, J. Approaching the shared biology of obesity and depression: The stress axis as the locus of gene-environment interactions. Mol. Psychiatry 2006, 11, 892–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hryhorczuk, C.; Sharma, S. Metabolic disturbances connecting obesity and depression. Front. Neurosci. 2013, 7, 177. [Google Scholar] [CrossRef] [Green Version]
- Minkwitz, J.; Scheipl, F.; Cartwright, L.; Campbell, I.C.; Chittka, T.; Thormann, J.; Hegerl, U.; Sander, C.; Himmerich, H. Why some obese people become depressed whilst others do not: Exploring links between cognitive reactivity, depression and obesity. Psychol. Health Med. 2019, 24, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Thormann, J.; Chittka, T.; Minkwitz, J.; Kluge, M.; Himmerich, H. Obesity and depression: An overview on the complex interactions of two diseases. Fortschr. Neurol. Psychiatr. 2013, 81, 145–153. [Google Scholar] [PubMed]
- Nicolaou, M.; Colpo, M.; Vermeulen, E.; Elstgeest, L.E.M.; Cabout, M.; Gibson-Smith, D.; Knuppel, A.; Sini, G.; Schoenaker, D.A.J.M.; Mishra, G.D.; et al. Association of a priori dietary patterns with depressive symptoms: A harmonised meta-analysis of observational studies. Psychol. Med. 2020, 50, 1872–1883. [Google Scholar] [CrossRef] [Green Version]
- Himmerich, H.; Kohls, E.; Hegerl, U.; Rummel-Kluge, C. Predictive factors of depression and its therapy. Nervenarzt 2014, 85, 1249–1254. [Google Scholar] [CrossRef]
- Azzi, A.; Gysin, R.; Kempná, P.; Munteanu, A.; Villacorta, L.; Visarius, T.; Zingg, J.M. Regulation of gene expression by α-tocopherol. Biol. Chem. 2004, 385, 585–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kornman, K.S.; Martha, P.M.; Duff, G.W. Genetic variations and inflammation: A practical nutrigenomics opportunity. Nutrition 2004, 20, 44–49. [Google Scholar] [CrossRef]
- Lamers, F.; Beekman, A.T.F.; Van Hemert, A.M.; Schoevers, R.A.; Penninx, B.W.J.H. Six-year longitudinal course and outcomes of subtypes of depression. Br. J. Psychiatry 2016, 208, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Stunkard, A.J.; Faith, M.S.; Allison, K.C. Depression and obesity. Biol. Psychiatry 2003, 54, 330–337. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Lichtblau, N.; Minkwitz, J.; Chittka, T.; Thormann, J.; Kirkby, K.C.; Sander, C.; Mergl, R.; Faßhauer, M.; Stumvoll, M.; et al. Cytokine levels in depressed and non-depressed subjects, and masking effects of obesity. J. Psychiatr. Res. 2014, 55, 29–34. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Weschenfelder, J.; Sander, C.; Minkwitz, J.; Thormann, J.; Chittka, T.; Mergl, R.; Kirkby, K.C.; Faßhauer, M.; Stumvoll, M.; et al. Inflammatory Cytokines in General and Central Obesity and Modulating Effects of Physical Activity. PLoS ONE 2015, 10, e0121971. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Mergl, R.; Minkwitz, J.; Holdt, L.M.; Teupser, D.; Hegerl, U.; Himmerich, H.; Sander, C. Is There an Association or Not?—Investigating the Association of Depressiveness, Physical Activity, Body Composition and Sleep with Mediators of Inflammation. Front. Psychiatry 2020, 11, 563. [Google Scholar] [CrossRef]
- Sander, C.; Ueck, P.; Mergl, R.; Gordon, G.; Hegerl, U.; Himmerich, H. Physical activity in depressed and non-depressed patients with obesity. Eat. Weight Disord. 2018, 23, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Zorena, K.; Jachimowicz-Duda, O.; Ślęzak, D.; Robakowska, M.; Mrugacz, M. Adipokines and Obesity. Potential Link to Metabolic Disorders and Chronic Complications. Int. J. Mol. Sci. 2020, 21, 3570. [Google Scholar] [CrossRef] [PubMed]
- Waters, G.S.; Pories, W.J.; Swanson, M.S.; Meelheim, H.D.; Flickinger, E.G.; May, H.J. Long-term studies of mental health after the greenville gastric bypass operation for morbid obesity. Am. J. Surg. 1991, 161, 154–158. [Google Scholar] [CrossRef]
- Dymek, M.P.; Le Grange, D.; Neven, K.; Alverdy, J. Quality of life and psychosocial adjustment in patients after Roux-en-Y gastric Bypass: A brief report. Obes. Surg. 2001, 11, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Emery, C.F.; Fondow, M.D.M.; Schneider, C.M.; Christofi, F.L.; Hunt, C.; Busby, A.K.; Needleman, B.J.; Melvin, W.S.; Elsayed-Awad, H.M. Gastric bypass surgery is associated with reduced inflammation and less depression: A preliminary investigation. Obes. Surg. 2007, 17, 759–763. [Google Scholar] [CrossRef]
- Vaghef-Mehrabany, E.; Ranjbar, F.; Asghari-Jafarabadi, M.; Hosseinpour-Arjmand, S. Calorie restriction in combination with prebiotic supplementation in obese women with depression: Effects on metabolic and clinical response. Nutr. Neurosci. 2019, 25, 1–15. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- National Heart, Lung, and Blood Institute (NHLBI). Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 27 December 2020).
- Breymeyer, K.L.; Lampe, J.W.; McGregor, B.A.; Neuhouser, M.L. Subjective mood and energy levels of healthy weight and overweight/obese healthy adults on high-and low-glycemic load experimental diets. Appetite 2016, 107, 253–359. [Google Scholar] [CrossRef] [Green Version]
- Galletly, C.; Moran, L.; Noakes, M.; Clifton, P.; Tomlinson, L.; Norman, R. Psychological benefits of a high-protein, low-carbohydrate diet in obese women with polycystic ovary syndrome-A pilot study. Appetite 2007, 49, 590–593. [Google Scholar] [CrossRef]
- Bot, M.; Brouwer, I.A.; Roca, M.; Kohls, E.; Penninx, B.W.J.H.; Watkins, E.; van Grootheest, G.; Cabout, M.; Hegerl, U.; Gili, M.; et al. MooDFOOD Prevention Trial Investigators. Effect of Multinutrient Supplementation and Food-Related Behavioral Activation Therapy on Prevention of Major Depressive Disorder Among Overweight or Obese Adults With Subsyndromal Depressive Symptoms. JAMA 2019, 321, 858. [Google Scholar] [CrossRef] [Green Version]
- Brinkworth, G.D.; Buckley, J.D.; Noakes, M.; Clifton, P.M.; Wilson, C.J. Long-term effects of a very low-carbohydrate diet and a low-fat diet on mood and cognitive function. Arch. Int. Med. 2009, 169, 1873–1880. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Lozada, C.; Cuervo, M.; Cuevas-Sierra, A.; Goni, L.; Riezu-Boj, J.I.; Navas-Carretero, S.; Milagro, F.I.; Martinez, J.A. Changes in anxiety and depression traits induced by energy restriction: Predictive value of the baseline status. Nutrients 2019, 11, 1206. [Google Scholar] [CrossRef] [PubMed]
- Hariri, N.; Ghahroudi, S.D.; Jahangiri, S.; Borumandnia, N.; Narmaki, E.; Saidpour, A. The beneficial effects of sumac (Rhus coriaria L.) supplementation along with restricted calorie diet on anthropometric indices, oxidative stress, and inflammation in overweight or obese women with depression: A randomized clinical trial. Phyther. Res. 2020, 34, 3041–3051. [Google Scholar] [CrossRef] [PubMed]
- Raman, J.; Hay, P.; Tchanturia, K.; Smith, E. A randomised controlled trial of manualized cognitive remediation therapy in adult obesity. Appetite 2018, 123, 269–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruusunen, A.; Voutilainen, S.; Karhunen, L.; Lehto, S.M.; Tolmunen, T.; Keinänen-Kiukaanniemi, S.; Eriksson, J.; Tuomilehto, J.; Uusitupa, M.; Lindström, J. How does lifestyle intervention affect depressive symptoms? Results from the Finnish Diabetes Prevention Study. Diabet. Med. 2012, 29, e126–e132. [Google Scholar] [CrossRef] [PubMed]
- Uemura, M.; Hayashi, F.; Ishioka, K.; Ihara, K.; Yasuda, K.; Okazaki, K.; Omata, J.; Suzutani, T.; Hirakawa, Y.; Chiang, C.; et al. Obesity and mental health improvement following nutritional education focusing on gut microbiota composition in Japanese women: A randomised controlled trial. Eur. J. Nutr. 2019, 58, 3291–3302. [Google Scholar] [CrossRef]
- Vigna, L.; Morelli, F.; Agnelli, G.M.; Napolitano, F.; Ratto, D.; Occhinegro, A.; Di Iorio, C.; Savino, E.; Girometta, C.; Brandalise, F.; et al. Hericium erinaceus Improves Mood and Sleep Disorders in Patients Affected by Overweight or Obesity: Could Circulating Pro-BDNF and BDNF Be Potential Biomarkers? Evid. Based Complement. Alternat. Med. 2019, 2019, 7861297. [Google Scholar] [CrossRef] [Green Version]
- Webber, K.H.; Casey, E.M.; Mayes, L.; Katsumata, Y.; Mellin, L. A comparison of a behavioral weight loss program to a stress management program: A pilot randomized controlled trial. Nutrition 2016, 32, 904–909. [Google Scholar] [CrossRef] [Green Version]
- Brinkworth, G.D.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G. Long-term effects of very low-carbohydrate and high-carbohydrate weight-loss diets on psychological health in obese adults with type 2 diabetes: Randomized controlled trial. J. Int. Med. 2016, 280, 388–397. [Google Scholar] [CrossRef]
- Fuller, N.R.; Burns, J.; Sainsbury, A.; Horsfield, S.; da Luz, F.; Zhang, S.; Denyer, G.; Markovic, T.P.; Caterson, I.D. Examining the association between depression and obesity during a weight management programme. Clin. Obes. 2017, 7, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Lutze, J.; Taylor, P.; Brinkworth, G.D.; Wyld, B.; Syrette, J.; Wilson, C.J.; Clifton, P.M.; Noakes, M. Psychological well-being response to high protein and high carbohydrate weight loss diets in overweight and obese men: A randomised trial. ESPEN J. 2013, 8, e235–e240. [Google Scholar] [CrossRef]
- Wing, R.R.; Marcus, M.D.; Blair, E.H.; Burton, L.R. Psychological responses of obese type II diabetic subjects to very-low-calorie diet. Diabetes Care 1991, 14, 596–599. [Google Scholar] [CrossRef] [PubMed]
- Crerand, C.E.; Wadden, T.A.; Foster, G.D.; Sarwer, D.B.; Paster, L.M.; Berkowitz, R.I. Changes in Obesity-related Attitudes in Women Seeking Weight Reduction. Obesity 2007, 15, 740–747. [Google Scholar] [CrossRef] [Green Version]
- Halyburton, A.K.; Brinkworth, G.D.; Wilson, C.J.; Noakes, M.; Buckley, J.D.; Keogh, J.B.; Clifton, P.M. Low- and high-carbohydrate weight-loss diets have similar effects on mood but not cognitive performance. Am. J. Clin. Nutr. 2007, 86, 580–587. [Google Scholar] [CrossRef]
- Sanchez, M.; Darimont, C.; Panahi, S.; Drapeau, V.; Marette, A.; Taylor, V.H.; Doré, J.; Tremblay, A. Effects of a Diet-Based Weight-Reducing Program with Probiotic Supplementation on Satiety Efficiency, Eating Behaviour Traits, and Psychosocial Behaviours in Obese Individuals. Nutrients 2017, 9, 284. [Google Scholar] [CrossRef] [PubMed]
- Coates, A.M.; Morgillo, S.; Yandell, C.; Scholey, A.; Buckley, J.D.; Dyer, K.A.; Alison, M.H. Effect of a 12-Week Almond-Enriched Diet on Biomarkers of Cognitive Performance, Mood, and Cardiometabolic Health in Older Overweight Adults. Nutrients 2020, 12, 1180. [Google Scholar] [CrossRef] [Green Version]
- Canheta, A.; Santos, A.S.; Souza, J.; Silveira, E.A. Traditional Brazilian diet and extra virgin olive oil reduce symptoms of anxiety and depression in individuals with severe obesity: Randomized clinical trial. Clin. Nutr. 2020, 40, 404–411. [Google Scholar] [CrossRef]
- Pedersen, L.R.; Olsen, R.H.; Jurs, A.; Astrup, A.; Chabanova, E.; Simonsen, L.; Wisløff, U.; Haugaard, S.B.; Prescott, E. A randomised trial comparing weight loss with aerobic exercise in overweight individuals with coronary artery disease: The CUT-IT trial. Eur. J. Prev. Cardiol. 2015, 22, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Hadi, A.; Sepandi, M.; Marx, W.; Moradi, S. Clinical and psychological responses to synbiotic supplementation in obese or overweight adults: A randomized clinical trial. Complement. Ther. Med. 2019, 47, 102216. [Google Scholar] [CrossRef]
- Tan, X.; Alén, M.; Wang, K.; Tenhunen, J.; Wiklund, P.; Partinen, M.; Cheng, S. Effect of Six-Month Diet Intervention on Sleep among Overweight and Obese Men with Chronic Insomnia Symptoms: A Randomized Controlled Trial. Nutrients 2016, 8, 751. [Google Scholar] [CrossRef]
- Carey, M.; Small, H.; Yoong, S.L.; Boyes, A.; Bisquera, A.; Sanson-Fisher, R. Prevalence of comorbid depression and obesity in general practice: A cross-sectional survey. Br. J. Gen. Pract. 2014, 64, e122. [Google Scholar] [CrossRef]
- Levitan, R.D.; Davis, C.; Kaplan, A.S.; Arenovich, T.; Phillips, D.I.W.; Ravindran, A.V. Obesity Comorbidity in Unipolar Major Depressive Disorder. J. Clin. Psychiatry 2012, 73, 1119–1124. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Steen, S.N.; Wingate, B.J.; Foster, G.D. Psychosocial consequences of weight reduction: How much weight loss is enough? Am. J. Clin. Nutr. 1996, 63 (Suppl. 3), 461–465. [Google Scholar] [CrossRef] [Green Version]
- Quinn, D.M.; Puhl, R.M.; Reinka, M.A. Trying again (and again): Weight cycling and depressive symptoms in U.S. adults. PLoS ONE 2020, 15, e0239004. [Google Scholar] [CrossRef]
- Brownell, K.D.; Puhl, R.M.; Schwartz, M.B.; Rudd, L. Weight Bias: Nature, Consequences, and Remedies; Guilford Publications: New York, NY, USA, 2005. [Google Scholar]
- Kasen, S.; Cohen, P.; Chen, H.; Must, A. Obesity and psychopathology in women: A three decade prospective study. Int. J. Obes. 2008, 32, 558–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, R.; Deleger, S.; Strawbridge, W.J.; Kaplan, G.A. Prospective association between obesity and depression: Evidence from the Alameda County Study. Int. J. Obes. 2003, 27, 514–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wise, L.A.; Adams-Campbell, L.L.; Palmer, J.R.; Rosenberg, L. Leisure time physical activity in relation to depressive symptoms in the Black Women’s Health Study. Ann. Behav. Med. 2006, 32, 68–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliver, G.; Wardle, J. Perceived effects of stress on food choice. Physiol. Behav. 1999, 66, 511–515. [Google Scholar] [CrossRef]
- Dallman, M.F.; Pecoraro, N.C.; La Fleur, S.E. Chronic stress and comfort foods: Self-medication and abdominal obesity. Brain Behav. Immun. 2005, 19, 275–280. [Google Scholar] [CrossRef]
- Himmerich, H.; Minkwitz, J.; Kirkby, K.C. Weight Gain and Metabolic Changes During Treatment with Antipsychotics and Antidepressants. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 252–260. [Google Scholar] [CrossRef]
- Serretti, A.; Mandelli, L. Antidepressants and Body Weight. J. Clin. Psychiatry 2010, 71, 1259–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellegrin, K.L.; O’Neil, P.M.; Stellefson, E.J.; Fossey, M.D.; Ballenger, J.C.; Cochrane, C.E.; Currey, H.S. Average daily nutrient intake and mood among obese women. Nutr. Res. 1998, 18, 1103–1112. [Google Scholar] [CrossRef]
- de Castro, J.M. Macronutrient relationships with meal patterns and mood in the spontaneous feeding behavior of humans. Physiol. Behav. 1987, 39, 561–569. [Google Scholar] [CrossRef]
- Muñoz, M.A.; Fíto, M.; Marrugat, J.; Covas, M.I.; Schröder, H. Adherence to the Mediterranean diet is associated with better mental and physical health. Br. J. Nutr. 2009, 101, 1821–1827. [Google Scholar] [CrossRef] [Green Version]
- Akbaraly, T.N.; Brunner, E.J.; Ferrie, J.E.; Marmot, M.G.; Kivimaki, M.; Singh-Manoux, A. Dietary pattern and depressive symptoms in middle age. Br. J. Psychiatry 2009, 195, 408–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacka, F.N.; Pasco, J.A.; Mykletun, A.; Williams, L.J.; Hodge, A.M.; O’Reilly, S.L.; Nicholson, G.C.; Kotowicz, M.A.; Berk, M. Association of western and traditional diets with depression and anxiety in women. Am. J. Psychiatry 2010, 167, 305–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiecolt-Glaser, J.K. Stress, food, and inflammation: Psychoneuroimmunology and nutrition at the cutting edge. Psychosom. Med. 2010, 72, 365–369. [Google Scholar] [CrossRef] [Green Version]
- Shelton, R.C.; Miller, A.H. Eating ourselves to death (and despair): The contribution of adiposity and inflammation to depression. Prog. Neurobiol. 2010, 91, 275–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raison, C.; Miller, A. Is depression an inflammatory disorder? Curr. Psychiatry Rep. 2011, 13, 467–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milaneschi, Y.; Simmons, W.K.; van Rossum, E.F.C.; Penninx, B.W.J.H. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef] [PubMed]
- De Bellis, M.D.; Gold, P.W.; Geracioti, T.D.; Listwak, S.J.; Kling, M.A. Association of fluoxetine treatment with reductions in CSF concentrations of corticotropin-releasing hormone and arginine vasopressin in patients with major depression. Am. J. Psychiatry 1993, 150, 656–657. [Google Scholar] [PubMed]
- De Mello, A.F.; De Mello, M.F.; Carpenter, L.L.; Price, L.H. Update on stress and depression: The role of the hypothalamic-pituitary-adrenal (HPA) axis. Braz. J. Psychiatry 2003, 25, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Gibbons, J.L.; McHugh, P.R. Plasma cortisol in depressive illness. J. Psychiatr. Res. 1962, 1, 162–171. [Google Scholar] [CrossRef]
- Sachar, E.J.; Hellman, L.; Fukushima, D.K.; Gallagher, T.F. Cortisol Production in Depressive Illness: A Clinical and Biochemical Clarification. Arch. Gen. Psychiatry 1970, 23, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S.; Shargill, N.S.; Spiegelman, B.M. Adipose expression of tumor necrosis factor-α: Direct role in obesity-linked insulin resistance. Science 1993, 259, 87–91. [Google Scholar] [CrossRef]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Makki, K.; Froguel, P.; Wolowczuk, I. Adipose Tissue in Obesity-Related Inflammation and Insulin Resistance: Cells, Cytokines, and Chemokines. ISRN Inflamm. 2013, 2013, 139239. [Google Scholar] [CrossRef] [Green Version]
- Kanda, H.; Tateya, S.; Tamori, Y.; Kotani, K.; Hiasa, K.I.; Kitazawa, R.; Kitazawa, S.; Miyachi, H.; Maeda, S.; Egashira, K.; et al. MCP–1 contributes to macrophage infiltration into adipose tissue, insulin resistance, and hepatic steatosis in obesity. J. Clin. Investig. 2006, 116, 1494–1505. [Google Scholar] [CrossRef] [PubMed]
- Kamei, N.; Tobe, K.; Suzuki, R.; Ohsugi, M.; Watanabe, T.; Kubota, N.; Ohtsuka-Kowatari, N.; Kumagai, K.; Sakamoto, K.; Kobayashi, M.; et al. Overexpression of monocyte chemoattractant protein-1 in adipose tissues causes macrophage recruitment and insulin resistance. J. Biol. Chem. 2006, 281, 26602–26614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capuron, L.; Ravaud, A.; Neveu, P.J.; Miller, A.H.; Maes, M.; Dantzer, R. Association between decreased serum tryptophan concentrations and depressive symptoms in cancer patients undergoing cytokine therapy. Mol. Psychiatry 2002, 7, 468–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wohleb, E.S.; McKim, D.B.; Sheridan, J.F.; Godbout, J.P. Monocyte trafficking to the brain with stress and inflammation: A novel axis of immune-to-brain communication that influences mood and behavior. Front. Neurosci. 2015, 8, 447. [Google Scholar] [CrossRef]
- Ataka, K.; Asakawa, A.; Nagaishi, K.; Kaimoto, K.; Sawada, A.; Sawada, A.; Hayakawa, Y.; Tatezawa, R.; Inui, A.; Fujimiya, M. Bone Marrow-Derived Microglia Infiltrate into the Paraventricular Nucleus of Chronic Psychological Stress-Loaded Mice. Harrison JK, editor. PLoS ONE 2013, 8, e81744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraus, T.; Haack, M.; Schuld, A.; Hinze-Selch, D.; Pollmächer, T. Low leptin levels but normal body mass indices in patients with depression or schizophrenia. Neuroendocrinology 2001, 73, 243–247. [Google Scholar] [CrossRef]
- Jow, G.M.; Yang, T.T.; Chen, C.L. Leptin and cholesterol levels are low in major depressive disorder, but high in schizophrenia. J. Affect. Disord. 2006, 90, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Maffei, M.; Halaas, J.; Ravussin, E.; Pratley, R.; Lee, G.H.; Zhang, Y.; Fei, H.; Kim, S.; Lallone, R.; Ranganathan, S.; et al. Leptin levels in human and rodent: Measurement of plasma leptin and ob RNA in obese and weight-reduced subjects. Nat. Med. 1997, 1, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Silha, J.V.; Krsek, M.; Skrha, J.V.; Sucharda, P.; Nyomba, L.G.; Murphy, L.J. Plasma resistin, adiponectin and leptin levels in lean and obese subjects: Correlations with insulin resistance. Eur. J. Endocrinol. 2003, 149, 331–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Münzberg, H.; Björnholm, M.; Bates, S.H.; Myers, M.G. Leptin receptor action and mechanisms of leptin resistance. Cell. Mol. Life Sci. 2005, 62, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Münzberg, H.; Myers, M.G. Molecular and anatomical determinants of central leptin resistance. Nat. Neurosci. 2005, 8, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Licinio, J.; Mantzoros, C.; Negrao, A.B.; Cizza, G.; Wong, M.L.; Bongiorno, P.B.; Chrousos, G.P.; Karp, B.; Allen, C.; Flier, J.S.; et al. Human leptin levels are pulsatile and inversely related to pituitary–ardenal function. Nat. Med. 1997, 3, 575–579. [Google Scholar] [CrossRef]
- Chen, H.; Charlat, O.; Tartaglia, L.A.; Woolf, E.A.; Weng, X.; Ellis, S.J.; Lakey, N.D.; Culpepper, J.; Moore, K.J.; Breitbart, R.E.; et al. Evidence that the diabetes gene encodes the leptin receptor: Identification of a mutation in the leptin receptor gene in db/db mice. Cell 1996, 84, 491–495. [Google Scholar] [CrossRef] [Green Version]
- Calapai, G.; Corica, F.; Corsonello, A.; Sautebin, L.; Di Rosa, M.; Campo, G.M.; Buemi, M.; Mauro, V.N.; Caputi, A.P. Leptin increases serotonin turnover by inhibition of brain nitric oxide synthesis. J. Clin. Investig. 1999, 104, 975–982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulton, S.; Pissios, P.; Manchon, R.P.; Stiles, L.; Frank, L.; Pothos, E.N.; Maratos-Flier, E.; Flier, J.S. Leptin Regulation of the Mesoaccumbens Dopamine Pathway. Neuron 2006, 51, 811–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, S.E.; Kirschbaum, C.; Steptoe, A. Perceived weight discrimination and chronic biochemical stress: A population-based study using cortisol in scalp hair. Obesity 2016, 24, 2515–2521. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Mickelson, K.D.; Williams, D.R. The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. J. Health Soc. Behav. 1999, 40, 208–230. [Google Scholar] [CrossRef] [PubMed]
- Carr, D.; Friedman, M.A. Is obesity stigmatizing? Body weight, perceived discrimination, and psychological well-being in the United States. J. Health. Soc. Behav. 2005, 46, 244–259. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, M.B.; Chambliss, H.O.N.; Brownell, K.D.; Blair, S.N.; Billington, C. Weight Bias among Health Professionals Specializing in Obesity. Obes. Res. 2003, 11, 1033–1039. [Google Scholar] [CrossRef]
- Friedman, M.A.; Brownell, K.D. Psychological Correlates of Obesity: Moving to the Next Research Generation. Psychol. Bull. 1995, 117, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Friedman, K.E.; Reichmann, S.K.; Costanzo, P.R.; Musante, G.J. Body image partially mediates the relationship between obesity and psychological distress. Obes. Res. 2002, 10, 33–41. [Google Scholar] [CrossRef]
- Markowitz, S.; Friedman, M.A.; Arent, S.M. Understanding the Relation Between Obesity and Depression: Causal Mechanisms and Implications for Treatment. Clin. Psychol. Sci. Pract. 2008, 15, 1–20. [Google Scholar] [CrossRef]
- Wing, R.R.; Epstein, L.H.; Marcus, M.D.; Kupfer, D.J. Mood changes in behavioral weight loss programs. J. Psychosom. Res. 1984, 28, 189–196. [Google Scholar] [CrossRef]
- Karlsson, J.; Hallgren, P.; Kral, J.; Lindroos, A.K.; Sjöström, L.; Sullivan, M. Predictors and effects of long-term dieting on mental well-being and weight loss in obese women. Appetite 1994, 23, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Bryan, J.; Tiggemann, M. The effect of weight-loss dieting on cognitive performance and psychological well-being in overweight women. Appetite 2001, 36, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Nauta, H.; Hospers, H.; Jansen, A. One-year follow-up effects of two obesity treatments on psychological well-being and weight. Br. J. Health Psychol. 2001, 6, 271–284. [Google Scholar] [CrossRef] [PubMed]
- Kraft, A.M. Weight loss and depression. Am. J. Psychiatry 1991, 148, 947–948. [Google Scholar]
- Junig, J.T.; Lehrmann, J.A. A psychotic episode associated with the Atkins Diet in a patient with bipolar disorder. Bipolar. Disord. 2005, 7, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Drapeau, V.; Jacob, R.; Panahi, S.; Tremblay, A. Effect of energy restriction on eating behavior traits and psychobehavioral factors in the low satiety phenotype. Nutrients 2019, 11, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacka, F.N.; O’Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M.L.; et al. A randomised controlled trial of dietary improvement for adults with major depression (the “SMILES” trial). BMC Med. 2017, 15, 23. [Google Scholar] [CrossRef] [Green Version]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutr. Neurosci. 2019, 22, 474–487. [Google Scholar] [CrossRef] [Green Version]

| Study | Weight kg (Mean ± SD) | BMI kg/m2 (Mean ± SD) | Depression | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post | p-Value | Baseline | Post | p-Value | Baseline | Post | p-Value | |
| Bot et al. [30] | P: 31.4 P + FRBA: 31.2 S: 31.3 S + FRBA: 31.7 | P: 7.3 (4.1) P + FRBA: 7.4 (4.4) S: 7.9 (4.4) S + FRBA: 7.1 (4) | |||||||
| Breymeyer et al. [28] | HGL: 2.80 LGL: 2.03 | p = 0.002 | |||||||
| Brinkworth, Buckley et al. [31] | LCHF: 96 ± 1.6 HCLF: 97.6 ± 1.6 | LCHF: 82.3 ± 2.1 HCLF: 83.9 ± 1.9 | BDI: p = 0.05 POMS: p = 0.05 | ||||||
| Brinkworth, Luscombe-Marsh et al. [39] | LC: 101.8 ± 2 HCLF: 101.1 ± 2 | LC: 92.6 ± 2 HCLF: 91 ± 2 | |||||||
| Canheta et al. [47] | 46.3 ± 6.5 | p < 0.001 | |||||||
| Coates et al. [46] | AED: 84.4 ± 12 NF: 85.4 ± 14 | AED: 84.8 ± 1.38 NF: 85.6 ± 1.36 | p > 0.05 | AED: 30.2 ± 0.44 NF: 30.6 ± 0.43 | AED: 30.5 ± 0.44 NF: 30.3 ± 0.43 | p > 0.05 | AED: 0.89 ± 1.9 NF: –3.74 ± 1.88 | AED: 1.11 ± 2.2 NF: –2.22 ± 2.17 | POMS: p > 0.05 |
| Crerand et al. [43] | D: 97.8 ± 13.5 C: 96.1 ± 12.1 | D: 36.2 ± 4.5 C: 35.3 ± 4.3 | D vs. C: p < 0.001 | D: 7.7 ± 5.5 C: 7.4 ± 5.9 | p < 0.001 | ||||
| Fuller et al. [40] | D: 90.9 ± 12.2 C: 93.8 ± 12.7 | D: –7.9 ± 2.1 C: 0.1 | D: 34.1 ± 4.3 C: 35.2 ± 4.8 | D: 22.1 ± 8.1 C: 23.7 ± 11.1 | D: 19.3 ± 6 C: 25.3 ± 12.7 | POMS: time x group p < 0.001 | |||
| Galletly et al. [29] | HPLC: 104.2 ± 5.3 LPHC: 98.6 ± 4.6 | HPLC: –6.9 ± 0.8 LPHC: –8.5 ± 6.3 | HPLC: 37.6 ± 6.4 LPHC: 37.2 ± 6.9 | HPLC: 34.5 ± 5.7 LPHC: 34.5 ± 6.3 | HPLC: 5.6 ± 3.2 LPHC: 4.8 ± 3.4 | HPLC: 3.6 ± 2.8 LPHC: 3.4 ± 3.3 | HPLC: p < 0.001 LPHC: NS | ||
| Hadi et al. [49] | 89.4 ± 16.1 | –5.2% ± 4.3% | p < 0.001 | 31.1 ± 3.9 | 5 ± 4.6 | 2 ± 4.1 | p < 0.001 | ||
| Halyburton et al. [44] | LCHF: 93.6 ± 2.1 HCLF: 97 ± 2.1 | LCHF: 33.3 ± 0.6 HCLF: 33.8 ± 0.6 | p < 0.001 | ||||||
| Hariri et al. [33] | Su: 84.3 ± 11.7 P: 79.3 ± 11.4 | Su: 78.96 ± 10.84 P: 76.89 ± 11.35 | p < 0.001 | Su: 32.4 ± 3.73 P: 31.2 ± 3.87 | S: 30.4 ± 3.55 P: 30.3 ± 3.89 | p < 0.001 | Su: 25.4 ± 9.42 P: 26.17 ± 11.21 | Su: 25.4 ± 9.42 P: 26.17 ± 11.21 | p < 0.001 |
| Lutze et al. [41] | HP: 100.5 ± 1.8 HC: 102.6 ± 1.8 | HP: –12.3 ± 1.4 HC: –10.9 ± 1.4 | HP: 23.4 ± 1.09 HC: 23.04 ± 1.05 | HP: 20.77 ± 0.97 HC: 20.19 ± 0.94 | POMS: p < 0.001 SF-36 subscales vitality and mental health: p < 0.001 | ||||
| Pedersen et al. [48] | Median: 92.8 | LED: p < 0.001 | Median: 31.4 | ||||||
| Raman et al. [34] | CRT-O: 40.3 ± 7.8 C: 39.2 ± 7.4 | CRT-O: 38.9 ± 7.6 C: 39.7 ± 8.4 | CRT-O:19.1 ± 11.2 C: 13.3 ± 12.2 | CRT-O: 4.5 ± 5.1 C: 15.4 ± 12.2 | |||||
| Rodriguez-Lozada et al. [32] | 87.7 | –8.6 | p < 0.001 | 31.6 | –3.1 | p < 0.001 | 6.6 | –2.7 | p < 0.001 |
| Ruusunen et al. [35] | –3.14 ± 4.5 | 30.5 ± 3.4 | –1.16 ± 1.74 | I vs. C: p = 0.024 | I: 6.8 ± 5.6 | I: –0.9 ± 4.5 | I: p = 0.03 | ||
| Sanchez et al. [45] | Pro: 95.1 ± 13.9 | Pro: –5.3 ± 4.3 | Pro: 33.8 ± 3.3 | Pro: 4.4 ± 4.1 | Pro: –1.5 ± 3 | p < 0.05 | |||
| Uemura et al. [36] | I: 66.3 ± 8.74 | I: 64.6 ± 8.07 | p < 0.001 | I: 27.8 ± 3.1 | I: 27.1 ± 2.82 | p < 0.001 | I: 17.64 ± 13.58 | I: 10.05 ± 7.4 | p < 0.001 |
| Tan et al. [50] | D: 93.8 C: 93.1 | D: 92.7 C: 94.4 | D: p < 0.05 | D: 29.4 C: 29.2 | D: 5.0 C: 4.0 | D: 4.0 C: 3.0 | p < 0.05 | ||
| Vaghef-Mehrabany et al. [25] | For >1.9kg weight loss: HDRS: 13.2 BDI: 19.5 | For >1.9kg weight loss: HDRS: 9.1 BDI: 14.7 | For >1.9kg weight loss: HDRS: p < 0.001 BDI: p = 0.006 | ||||||
| Vigna et al. [37] | HE: 33.1 ± 0.84 C: 33.4 ± 0.83 | HE: 32.01 ± 0.82 C: 32.08 ± 0.88 | HE: 48.8 ± 1.03 | HE: 43.2 ± 2.38 | HE: p < 0.05 | ||||
| Webber et al. [38] | BWL: 99 ± 16.7 EBT: 101 ± 10.8 | BWL: 36 ± 4.3 EBT: 37 ± 4.9 | BWL: –1.3 EBT: –0.6 | BWL: p < 0.001 EBT: p = 0.032 BWL vs. EBT: p < 0.03 | BWL: 7.5 ± 6.4 EBT: 10.4 ± 9.8 | BWL: –2.9 EBT: –3.1 | BWL: p = 0.012 EBT: p = 0.006 | ||
| Wing et al. [42] | 103.2 ± 16.9 | VLCD: 14.6 ± 9.4 BD: 11.4 ± 7.2 | VLCD: 5 ± 6.3 BD: 2.9 ± 2.8 | VLCD: p < 0.001 BD: p < 0.001 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patsalos, O.; Keeler, J.; Schmidt, U.; Penninx, B.W.J.H.; Young, A.H.; Himmerich, H. Diet, Obesity, and Depression: A Systematic Review. J. Pers. Med. 2021, 11, 176. https://doi.org/10.3390/jpm11030176
Patsalos O, Keeler J, Schmidt U, Penninx BWJH, Young AH, Himmerich H. Diet, Obesity, and Depression: A Systematic Review. Journal of Personalized Medicine. 2021; 11(3):176. https://doi.org/10.3390/jpm11030176
Chicago/Turabian StylePatsalos, Olivia, Johanna Keeler, Ulrike Schmidt, Brenda W. J. H. Penninx, Allan H. Young, and Hubertus Himmerich. 2021. "Diet, Obesity, and Depression: A Systematic Review" Journal of Personalized Medicine 11, no. 3: 176. https://doi.org/10.3390/jpm11030176
APA StylePatsalos, O., Keeler, J., Schmidt, U., Penninx, B. W. J. H., Young, A. H., & Himmerich, H. (2021). Diet, Obesity, and Depression: A Systematic Review. Journal of Personalized Medicine, 11(3), 176. https://doi.org/10.3390/jpm11030176