
Randomized Clinical Trial Comparing Concomitant and Tailored Therapy for Eradication of Helicobacter pylori Infection

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
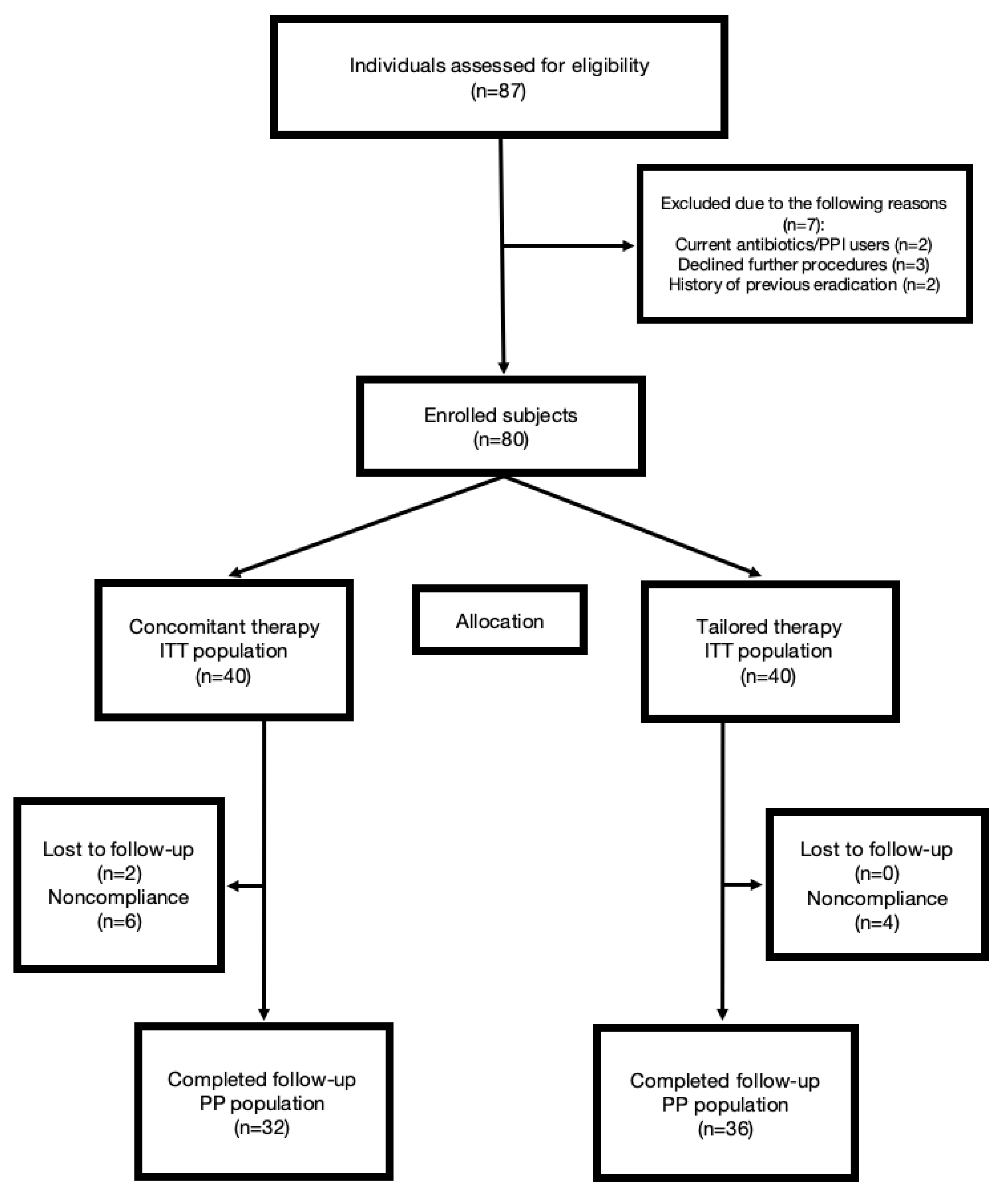
2.1. Design Overview
2.2. Biopsy Sampling and Microbiology Tests
2.3. Patient Follow-Up
2.4. Therapy
2.5. Statistical Analysis
2.5.1. Sample Size Calculation
2.5.2. Statistical Analysis
3. Results
3.1. Study Group Characteristics
3.2. Outcomes
3.2.1. Eradication and Antimicrobial Resistance Rate
3.2.2. Compliance and Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fock, K.M.; Graham, D.Y.; Malfertheiner, P. Helicobacter pylori research: Historical insights and future directions. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Fischbach, L. Helicobacter pylori treatment in the era of increasing of antibiotic resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global Cancer Statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plummer, M.; Franceschi, S.; Vignat, J.; Forman, D.; de Martel, C. Global burden of gastric cancer attributable to Helicobacter pylori. Int. J. Cancer 2015, 136, 487–490. [Google Scholar] [CrossRef]
- Wojciech, J.; Lech, C.; Wiktor, Ł.; Maciej, S. Alcohol dehydrogenase (ADH) isoenzymes activity in the sera of patients with Helicobacter pylori infection. Dig. Dis. Sci. 2007, 52, 1513–1516. [Google Scholar]
- Wojciech, J.; Magdalena, Ł.; Anna, S.; Maciej, S. The alcohol dehydrogenase isoenzyme alcohol dehydrogenase IV as a candidate marker of Helicobacter pylori infection. Arch. Med. Sci. 2014, 10, 951–955. [Google Scholar]
- Sugano, K.; Tack, J.; Kuipers, E.J.; Graham, D.Y.; El-Omar, E.M.; Miura, S.; Malfertheiner, P. Kyoto global consensus report on Helicobacter pylori gastritis. Gut 2015, 64, 1353–1367. [Google Scholar] [CrossRef] [Green Version]
- Graham, D.Y. Transitioning of Helicobacter pylori Therapy from Trial and Error to Antimicrobial Stewardship. Antibiotics 2020, 9, 671. [Google Scholar] [CrossRef] [PubMed]
- Wüppenhorst, N.; Draeger, S.; Stüger, H.P.; Hobmaier, B.; Vorreiter, J.; Kist, M.; ResiNet Study Group. Prospective multicentre study on antimicrobial resistance of Helicobacter pylori in Germany. J. Antimicrob. Chemother. 2014, 69, 3127–3133. [Google Scholar] [CrossRef] [Green Version]
- Tonkic, A.; Tonkic, M.; Brnic, D.; Novak, A.; Puljiz, Z.; Simunic, M. Time trends of primary antibiotic resistance of Helicobacter pylori isolates in Southern Croatia. J. Chemother. 2012, 24, 182–184. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Kim, J.I.; Cheung, D.Y.; Kim, T.H.; Jun, E.J.; Oh, J.H.; Kim, J.K. Eradication of Helicobacter pylori according to 23S ribosomal RNA point mutations associated with clarithromycin resistance. J. Infect. Dis. 2013, 208, 1123–1130. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Zhang, J.; Song, Z.; He, L.; Li, Y.; Qian, J.; Lin, S. Tailored versus triple plus bismuth or concomitant therapy as initial Helicobacter pylori treatment: A randomized trial. Helicobacter 2015, 21, 91–99. [Google Scholar] [CrossRef]
- Lee, J.Y.; Choi, Y.J.; Yoon, K.; Nam, R.H.; Suh, J.H.; Lee, J.W.; Lee, D.H. Comparison of the efficacy of culture-based tailored therapy for Helicobacter pylori eradication with that of the traditional second-line rescue therapy in Korean patients: A prospective single tertiary center study. Scand. J. Gastroenterol. 2016, 51, 270–276. [Google Scholar]
- Megraud, F.; Coenen, S.; Versporten, A.; Kist, M.; Lopez-Brea, M.; Hirschl, A.M.; Glupczynski, Y. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut 2012, 62, 34–42. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Calvet, X. Review article: Non-bismuth quadruple (concomitant) therapy for Helicobacter pylori eradication. Aliment Pharmacol. There 2011, 34, 604–617. [Google Scholar] [CrossRef]
- Mestrovic, A.; Perkovic, N.; Bozic, J.; Ivelja, M.P.; Vukovic, J.; Kardum, G.; Puljiz, Z.; Tonkic, A. Randomised clinical trial comparing concomitant and hybrid therapy for eradication of Helicobacter pylori infection. PLoS ONE 2020, 15, e0244500. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Kim, J.I.; Lee, J.S.; Jun, E.J.; Oh, J.H.; Cheung, D.Y.; Kim, S.S. Concomitant therapy achieved the best eradication rate for Helicobacter pylori among various treatment strategies. World J. Gastroen. 2015, 21, 351–359. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Calvet, X. Update on non-bismuth quadruple (concomitant) therapy for eradication of Helicobacter pylori. Clin. Exp. Gastroenterol. 2012, 5, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolinar, U.; Plut, S.; Štabuc, B.; Homan, M.; Tepeš, B.; Jeverica, S. Primary and secondary resistance of Helicobacter pylori in Slovenia, 2011–2014. In Proceedings of the 25th European Congress of Clinical Microbiology and Infectious Diseases, Copenhagen, Denmark, 25–28 April 2015; Available online: https://www.escmid.org/escmid_publications/escmid_elibrary/ (accessed on 25 April 2021).
- Megraud, F.; Lehours, P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin. Microbiol. Rev. 2007, 20, 280–322. [Google Scholar] [CrossRef] [Green Version]
- Romano, M.; Iovene, M.R.; Montella, F.; Vitale, L.M.; De Simone, T.; Del Vecchio Blanco, C. Pretreatment antimicrobial-susceptibility testing in the eradication of H. pylori infection. Am. J. Gastroenterol. 2000, 95, 3317–3318. [Google Scholar] [CrossRef] [PubMed]
- Tonkić, M.; Tonkić, A.; Goić-Barisić, I.; Jukić, I.; Simunić, M.; Punda-Polić, V. Primary resistance and antibiotic minimum inhibitory concentrations for Helicobacter pylori strains, in Split, Croatia. J. Chemother. 2006, 18, 437–439. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.; Gisbert, J.; Kuipers, E.; Axon, A.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.; et al. Management ofHelicobacter pyloriinfection—the Maastricht V/Florence Consensus Report. Gut 2016, 66, 6–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Atherton, J.; Axon, A.T.; Bazzoli, F.; European Helicobacter Study Group. Management of Helicobacter pylori infection--the Maastricht IV/ Florence Consensus Report. Gut 2012, 61, 646–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Essa, A.S.; Kramer, J.R.; Graham, D.Y.; Treiber, G. Meta-analysis: Four-drug, three-antibiotic, non-bismuth-containing “concomitant therapy” versus triple therapy for Helicobacter pylori eradication. Helicobacter 2009, 14, 109–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Marshall, J.K. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology 2016, 151, 51–69.e14. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.C.; Hsu, P.I.; Wu, J.Y.; Opekun, A.R.; Kuo, C.H.; Wu, I.C.; Wang, S.S.; Chen, A.; Hung, W.C.; Graham, D.Y. Sequential and concomitant therapy with 4 drugs are equally effective for H. pylori infection. Clin. Gastroenterol. Hepatol. 2010, 8, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Liou, J.M.; Chen, C.C.; Chang, C.Y.; Chen, M.J.; Chen, C.C.; Fang, Y.J.; Wu, M.S. Sequential therapy for 10 days versus triple therapy for 14 days in the eradication of Helicobacter pylori in the community and hospital populations: A randomised trial. Gut 2016, 65, 784–1792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuta, T.; Graham, D.Y. Pharmacologic aspects of eradication therapy for Helicobacter pylori infection. Gastroenterol. Clin. N. Am. 2010, 39, 465–480. [Google Scholar] [CrossRef] [PubMed]
- Tepeš, B.; Štabuc, B. Slovenian society for gastroenterology and hepatology guidelines on the management of Helicobacter pylori infection. Zdrav. Vestn. 2011, 80, 647–656. [Google Scholar]
- Chen, L.; Xu, W.; Lee, A. The impact of Helicobacter pylori infection, eradication therapy and probiotic supplementation on gut microenvironment homeostasis: An open-label, randomized clinical trial. EBioMedicine 2018, 35, 87–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenzhen, Y.; Yumin, L.; Quanlin, G.; Kehu, Y.; Lei, J.; Donghai, W.; Lijuan, Y. Is Antimicrobial Susceptibility Testing Necessary Before First-line Treatment for Helicobacter pylori Infection? Meta-analysis of Randomized Controlled Trials-. Intern. Med. 2010, 49, 1103–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuta, T.; Shirai, N.; Kodaira, M.; Sugimoto, M.; Nogaki, A.; Kuriyama, S.; Iwaizumi, M.; Yamade, M.; Terakawa, I.; Ohashi, K.; et al. Pharmacogenomics-based Tailored Versus Standard Therapeutic Regimen for Eradication of H. pylori. Clin. Pharmacol. Ther. 2007, 81, 521–528. [Google Scholar] [CrossRef]
- Cosme, A.; Montes, M.; Martos, M.; Gil, I.; Mendarte, U.; Salicio, Y.; Piñeiro, L.; Recasens, M.T.; Ibarra, B.; Sarasqueta, C.; et al. Usefulness of antimicrobial susceptibility in the eradication of Helicobacter pylori. Clin. Microbiol. Infect. 2013, 19, 379–383. [Google Scholar] [CrossRef] [Green Version]
- Park, C.S.; Lee, S.M.; Park, C.H.; Koh, H.R.; Jun, C.H.; Park, S.Y.; Rew, J.S. Pretreatment antimicrobial susceptibility-guided vs. clarithromycin-based triple therapy for Helicobacter pylori eradication in a region with high rates of multiple drug resistance. Am. J. Gastroenterol. 2014, 109, 1595–1602. [Google Scholar] [CrossRef] [PubMed]
- López-Góngora, S.; Puig, I.; Calvet, X.; Villoria, A.; Baylina, M.; Munoz, N.; Gisbert, J.P. Systematic review and meta-analysis: Susceptibility-guided versus empirical antibiotic treatment for Helicobacter pylori infection. J. Antimicrob. Chemother. 2015, 70, 2447–2455. [Google Scholar] [CrossRef] [Green Version]
- Breuer, T.; Graham, D.Y. Costs of diagnosis and treatment of Helicobacter pylori infection: When does choosing the treatment regimen based on susceptibility testing become cost effective? Am. J. Gastroenterol. 1999, 94, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.; Marmo, R.; Cuomo, A.; De Simone, T.; Mucherino, C.; Iovene, M.R.; Nardone, G. Pretreatment antimicrobial susceptibility testing is cost saving in the eradication of Helicobacter pylori. Clin. Gastroen. Hepat. 2003, 1, 273–278. [Google Scholar] [CrossRef]
- Graham, D.Y. Avoiding unethical Helicobacter pylori clinical trials: Susceptibility-based studies and probiotics as adjuvants. Helicobacter 2015, 20, 321–325. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Parameter | Concomitant Therapy (N = 40) | Tailored Therapy (N = 40) | p * |
|---|---|---|---|
| Male gender (N, %) | 21 (52.5) | 17 (42.5) | 0.373 * |
| Age (years) | 61.9 ± 12.7 | 60.4 ± 13.4 | 0.628 † |
| Smoking (N, %) | 7 (17.5) | 11 (27.5) | 0.287 * |
| Alcohol consumption (N, %) | 8 (20.0) | 5 (12.5) | 0.546 ‡ |
| Endoscopic findings | |||
| Gastritis | 32 (80.0) | 33 (82.5) | 0.503 ‡ |
| Gastric ulcer | 5 (12.5) | 5 (12.5) | |
| Duodenal ulcer | 2 (5.0) | 0 (0.0) | |
| Duodenitis | 1 (2.5) | 2 (5.0) |
| Parameter | Concomitant Therapy (N = 40, %) | Tailored Therapy (N = 40, %) | p * |
|---|---|---|---|
| Eradication rate: | |||
| Intention-to-treat (%; 95% CI) | 28/40 (70.0; 55.8–84.2) | 37/40 (92.5; 85.0–100.0) | 0.010 |
| Per-protocol (%; 95% CI) | 28/32 (87.5; 76.1–98.9) | 36/36 (100.0; /) | 0.030 |
| Compliance >80% | 34/40 (85.0) | 36/40 (90.0) | 0.502 |
| Adverse effects | 13/40 (32.5) | 3/40 (7.5) | 0.006 † |
| Antimicrobial Agent | Strains Tested (N) | Primary Antibiotic Resistance n (%) |
|---|---|---|
| Clarithromycin | 40 | 15 (37.5) |
| Metronidazole | 40 | 7 (17.5) |
| Levofloxacin | 40 | 2 (5) |
| Amoxicillin | 40 | 0 (0) |
| Dual resistance | ||
| Clarithromycin, Metronidazole | 40 | 4 (10) |
| Clarithromycin, Levofloxacin | 40 | 2 (5) |
| Parameter | Concomitant Therapy 1 (N = 40) | Tailored Therapy 1 (N = 40) | p * |
|---|---|---|---|
| Nausea | 7 (17.5) | 3 (7.5) | 0.311 |
| Stomach pain | 1 (2.5) | 0 (0.0) | 0.998 |
| Skin rash | 2 (5.0) | 0 (0.0) | 0.493 |
| Metallic taste | 2 (5.0) | 0 (0.0) | 0.493 |
| Headache | 1 (2.5) | 0 (0.0) | 0.998 |
| Diarrhea | 1 (2.5) | 0 (0.0) | 0.998 |
| Tongue deposits | 1 (2.5) | 0 (0.0) | 0.998 |
| Adverse effect † | Concomitant Therapy 1 (N = 40) | Tailored Therapy 1 (N = 40) | p * |
|---|---|---|---|
| None | 27 (67.5) | 37 (92.5) | 0.019 |
| Mild | 10 (25.0) | 2 (5.0) | |
| Moderate | 3 (7.5) | 1 (2.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perkovic, N.; Mestrovic, A.; Bozic, J.; Ivelja, M.P.; Vukovic, J.; Kardum, G.; Sundov, Z.; Tonkic, M.; Puljiz, Z.; Vukojevic, K.; et al. Randomized Clinical Trial Comparing Concomitant and Tailored Therapy for Eradication of Helicobacter pylori Infection. J. Pers. Med. 2021, 11, 534. https://doi.org/10.3390/jpm11060534
Perkovic N, Mestrovic A, Bozic J, Ivelja MP, Vukovic J, Kardum G, Sundov Z, Tonkic M, Puljiz Z, Vukojevic K, et al. Randomized Clinical Trial Comparing Concomitant and Tailored Therapy for Eradication of Helicobacter pylori Infection. Journal of Personalized Medicine. 2021; 11(6):534. https://doi.org/10.3390/jpm11060534
Chicago/Turabian StylePerkovic, Nikola, Antonio Mestrovic, Josko Bozic, Mirela Pavicic Ivelja, Jonatan Vukovic, Goran Kardum, Zeljko Sundov, Marija Tonkic, Zeljko Puljiz, Katarina Vukojevic, and et al. 2021. "Randomized Clinical Trial Comparing Concomitant and Tailored Therapy for Eradication of Helicobacter pylori Infection" Journal of Personalized Medicine 11, no. 6: 534. https://doi.org/10.3390/jpm11060534
APA StylePerkovic, N., Mestrovic, A., Bozic, J., Ivelja, M. P., Vukovic, J., Kardum, G., Sundov, Z., Tonkic, M., Puljiz, Z., Vukojevic, K., & Tonkic, A. (2021). Randomized Clinical Trial Comparing Concomitant and Tailored Therapy for Eradication of Helicobacter pylori Infection. Journal of Personalized Medicine, 11(6), 534. https://doi.org/10.3390/jpm11060534