
Heading for Personalized rTMS in Tinnitus: Reliability of Individualized Stimulation Protocols in Behavioral and Electrophysiological Responses

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Test Session Procedure
2.3. Repetitive Transcranial Magnetic Stimulation (rTMS)
2.4. Electroencephalography
2.4.1. Data Acquisition and Preprocessing
2.4.2. Power Spectra
2.5. Statistical Analysis
2.5.1. Reliability Analysis of TMS-Induced Tinnitus Loudness Changes and Discomfort Evaluation
2.5.2. Reliability Analysis of TMS-Induced Changes in Oscillatory Brain Activity
2.5.3. rTMS Individualization via Responder Identification Using Behavioral and Electrophysiological Data
3. Results
3.1. Sample Characteristics
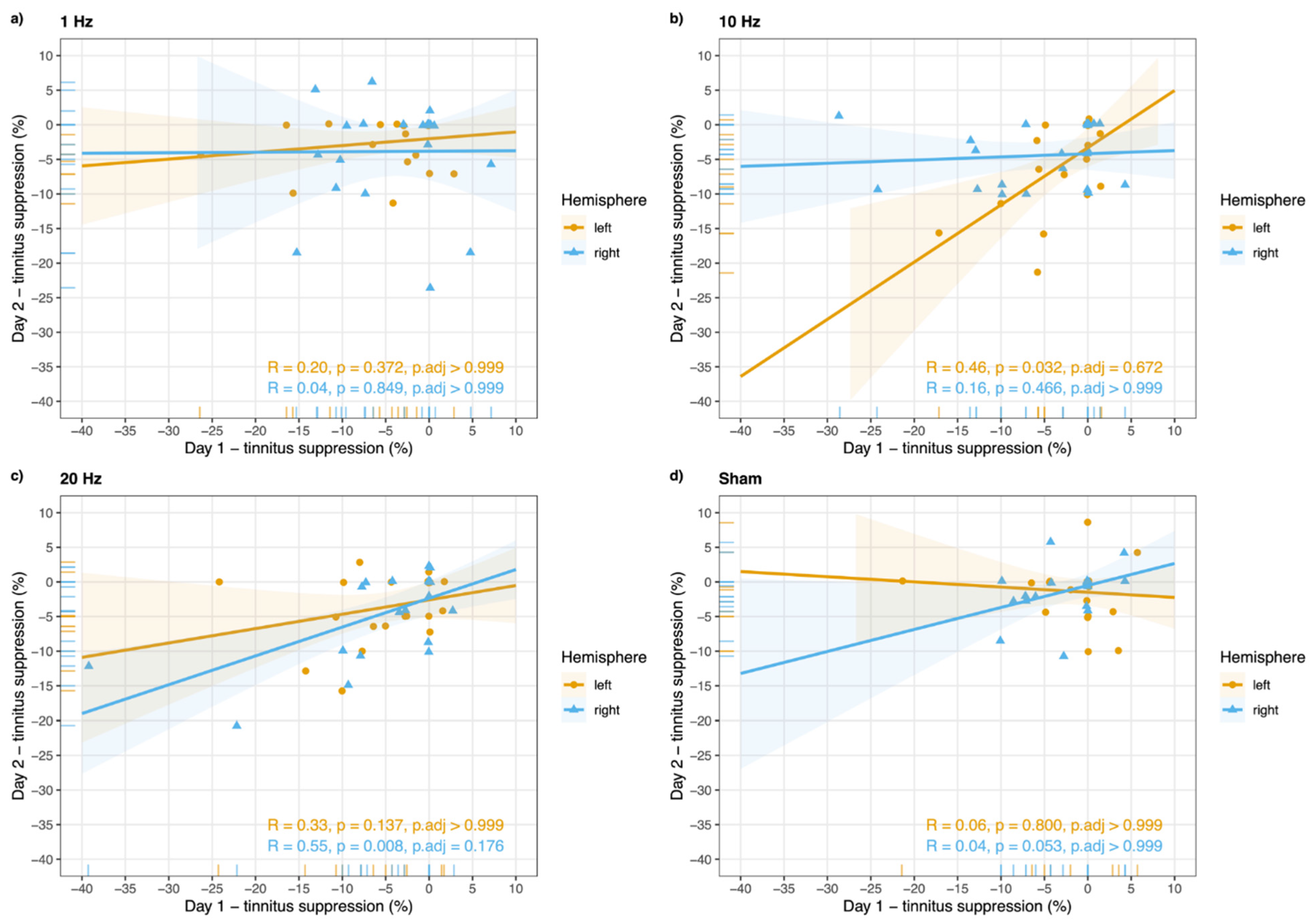
3.2. Test–Retest Reliability of TMS-Induced Changes in Tinnitus Loudness and Oscillatory Brain Activity
3.3. rTMS Individualization Using Behavioral and Electrophysiological Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Baguley, D.; McFerran, D.; Hall, D. Tinnitus. Lancet 2013, 382, 1600–1607. [Google Scholar] [CrossRef] [Green Version]
- Langguth, B.; Kreuzer, P.M.; Kleinjung, T.; De Ridder, D. Tinnitus: Causes and clinical management. Lancet Neurol. 2013, 12, 920–930. [Google Scholar] [CrossRef]
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear. Res. 2016, 337, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, J.J. Pathophysiology of tinnitus. Prog. Brain Res. 2007, 166, 19–543. [Google Scholar] [CrossRef]
- Eggermont, J.J.; Roberts, L.E. The Neuroscience of Tinnitus: Understanding Abnormal and Normal Auditory Perception. Front. Syst. Neurosci. 2012, 6, 53. [Google Scholar] [CrossRef] [Green Version]
- Eggermont, J.J.; Tass, P. Maladaptive Neural Synchrony in Tinnitus: Origin and Restoration. Front. Neurol. 2015, 6, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, J.A.; Roberts, L.E.; Caspary, D.M.; Theodoroff, S.M.; Salvi, R.J. Underlying Mechanisms of Tinnitus: Review and Clinical Implications. J. Am. Acad. Audiol. 2014, 25, 005–022. [Google Scholar] [CrossRef]
- Roberts, L.E.; Eggermont, J.J.; Caspary, D.M.; Shore, S.E.; Melcher, J.R.; Kaltenbach, J.A. Ringing Ears: The Neuroscience of Tinnitus. J. Neurosci. 2010, 30, 14972–14979. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B. Non-Invasive Neuromodulation for Tinnitus. J. Audiol. Otol. 2020, 24, 113–118. [Google Scholar] [CrossRef]
- Hallett, M. Transcranial Magnetic Stimulation: A Primer. Neuron 2007, 55, 187–199. [Google Scholar] [CrossRef] [Green Version]
- Hoogendam, J.M.; Ramakers, G.M.; Di Lazzaro, V. Physiology of repetitive transcranial magnetic stimulation of the human brain. Brain Stimul. 2010, 3, 95–118. [Google Scholar] [CrossRef]
- Siebner, H.R.; Rothwell, J. Transcranial magnetic stimulation: New insights into representational cortical plasticity. Exp. Brain Res. 2003, 148, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, P.B. Intensity-dependent effects of 1 Hz rTMS on human corticospinal excitability. Clin. Neurophysiol. 2002, 113, 1136–1141. [Google Scholar] [CrossRef]
- Fitzgerald, P.B.; Fountain, S.; Daskalakis, Z.J. A comprehensive review of the effects of rTMS on motor cortical excitability and inhibition. Clin. Neurophysiol. 2006, 117, 2584–2596. [Google Scholar] [CrossRef]
- Klomjai, W.; Katz, R.; Lackmy-Vallée, A. Basic principles of transcranial magnetic stimulation (TMS) and repetitive TMS (rTMS). Ann. Phys. Rehabilitation Med. 2015, 58, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Rossini, P.; Burke, D.; Chen, R.; Cohen, L.; Daskalakis, Z.; Di Iorio, R.; Di Lazzaro, V.; Ferreri, F.; Fitzgerald, P.; George, M.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin. Neurophysiol. 2015, 126, 1071–1107. [Google Scholar] [CrossRef]
- Eichhammer, P.; Langguth, B.; Marienhagen, J.; Kleinjung, T.; Hajak, G. Neuronavigated repetitive transcranial magnetic stimulation in patients with tinnitus: A short case series. Biol. Psychiatry 2003, 54, 862–865. [Google Scholar] [CrossRef]
- Langguth, B.; Eichhammer, P.; Wiegand, R.; Marienhegen, J.; Maenner, P.; Jacob, P.; Hajak, G. Neuronavigated rTMS in a patient with chronic tinnitus. Effects of 4 weeks treatment. NeuroReport 2003, 14, 980–997. [Google Scholar] [CrossRef]
- Schoisswohl, S.; Agrawal, K.; Simoes, J.; Neff, P.; Schlee, W.; Langguth, B.; Schecklmann, M. RTMS parameters in tinnitus trials: A systematic review. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef]
- Lehner, A.; Schecklmann, M.; Greenlee, M.W.; Rupprecht, R.; Langguth, B. Triple-site rTMS for the treatment of chronic tinnitus: A randomized controlled trial. Sci. Rep. 2016, 6, 22302. [Google Scholar] [CrossRef] [Green Version]
- Lehner, A.; Schecklmann, M.; Poeppl, T.B.; Kreuzer, P.M.; Vielsmeier, V.; Rupprecht, R.; Landgrebe, M.; Langguth, B. Multisite rTMS for the Treatment of Chronic Tinnitus: Stimulation of the Cortical Tinnitus Network—A Pilot Study. Brain Topogr. 2012, 26, 501–510. [Google Scholar] [CrossRef]
- De Ridder, D.; Song, J.-J.; Vanneste, S. Frontal Cortex TMS for Tinnitus. Brain Stimul. 2013, 6, 355–362. [Google Scholar] [CrossRef]
- Noh, T.S.; Kyong, J.S.; Chang, M.Y.; Park, M.K.; Lee, J.H.; Oh, S.H.; Kim, J.S.; Chung, C.K.; Suh, M.W. Comparison of Treatment Outcomes Following Either Prefrontal Cortical-only or Dual-site Repetitive Transcranial Magnetic Stimulation in Chronic Tinnitus Patients: A Double-blind Randomized Study. Otol. Neurotol. 2017, 38, 296–303. [Google Scholar]
- Vanneste, S.; De Ridder, D. Differences between a single session and repeated sessions of 1 Hz TMS by double-cone coil prefrontal stimulation for the improvement of tinnitus. Brain Stimul. 2013, 6, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Forogh, B.; Yazdi-Bahri, S.-M.; Ahadi, T.; Fereshtehnejad, S.-M.; Raissi, G.R. Comparison of two protocols of transcranial magnetic stimulation for treatment of chronic tinnitus: A randomized controlled clinical trial of burst repetitive versus high-frequency repetitive transcranial magnetic stimulation. Neurol. Sci. 2014, 35, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E.M.; Abo-Elfetoh, N.; Rothwell, J.C.; El-Atar, A.; Sayed, E.; Khalifa, H. Contralateral versus ipsilateral rTMS of temporoparietal cortex for the treatment of chronic unilateral tinnitus: Comparative study. Eur. J. Neurol. 2010, 17, 976–983. [Google Scholar] [CrossRef]
- Khedr, E.M.; Rothwell, J.C.; Ahmed, M.A.; El-Atar, A. Effect of daily repetitive transcranial magnetic stimulation for treatment of tinnitus: Comparison of different stimulus frequencies. J. Neurol. Neurosurg. Psychiatry 2008, 79, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Plewnia, C.; Vonthein, R.; Wasserka, B.; Arfeller, C.; Naumann, A.; Schraven, S.P.; Plontke, S.K. Treatment of chronic tinnitus with theta burst stimulation: A randomized controlled trial. Neurology 2012, 78, 1628–1634. [Google Scholar] [CrossRef]
- Schecklmann, M.; Giani, A.; Tupak, S.; Langguth, B.; Raab, V.; Polak, T.; Várallyay, C.; Großmann, W.; Herrmann, M.J.; Fallgatter, A.J. Neuronavigated left temporal continuous theta burst stimulation in chronic tinnitus. Restor. Neurol. Neurosci. 2016, 34, 165–175. [Google Scholar] [CrossRef]
- Dong, C.; Chen, C.; Wang, T.; Gao, C.; Wang, Y.; Guan, X.; Dong, X. Low-Frequency Repetitive Transcranial Magnetic Stimulation for the Treatment of Chronic Tinnitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. BioMed. Res. Int. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Zenner, H.-P.; Delb, W.; Kröner-Herwig, B.; Jäger, B.; Peroz, I.; Hesse, G.; Mazurek, B.; Goebel, G.; Gerloff, C.; Trollmann, R.; et al. A multidisciplinary systematic review of the treatment for chronic idiopathic tinnitus. Eur. Arch. Otorhinolaryngol. 2017, 274, 2079–2091. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; André-Obadia, N.; Antal, A.; Ayache, S.S.; Baeken, C.; Benninger, D.H.; Cantello, R.M.; Cincotta, M.; De Carvalho, M.; De Ridder, D.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin. Neurophysiol. 2014, 125, 2150–2206. [Google Scholar] [CrossRef] [PubMed]
- Londero, A.; Bonfils, P.; Lefaucheur, J. Transcranial magnetic stimulation and subjective tinnitus. A review of the literature, 2014–2016. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2018, 135, 51–58. [Google Scholar] [CrossRef]
- Lefebvre-Demers, M.; Doyon, N.; Fecteau, S. Non-invasive neuromodulation for tinnitus: A meta-analysis and modeling studies. Brain Stimul. 2021, 14, 113–128. [Google Scholar] [CrossRef] [PubMed]
- Guerra, A.; López-Alonso, V.; Cheeran, B.; Suppa, A. Variability in non-invasive brain stimulation studies: Reasons and results. Neurosci. Lett. 2020, 719, 133330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Alonso, V.; Cheeran, B.; Río-Rodríguez, D.; Fernández-Del-Olmo, M. Inter-individual Variability in Response to Non-invasive Brain Stimulation Paradigms. Brain Stimul. 2014, 7, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Polanía, R.; Nitsche, M.A.; Ruff, C.C. Studying and modifying brain function with non-invasive brain stimulation. Nat. Neurosci. 2018, 21, 174–187. [Google Scholar] [CrossRef]
- Terranova, C.; Rizzo, V.; Cacciola, A.; Chillemi, G.; Calamuneri, A.; Milardi, D.; Quartarone, A. Is There a Future for Non-invasive Brain Stimulation as a Therapeutic Tool? Front. Neurol. 2019, 9, 1146. [Google Scholar] [CrossRef] [PubMed]
- Cocchi, L.; Zalesky, A. Personalized Transcranial Magnetic Stimulation in Psychiatry. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Garnaat, S.L.; Fukuda, A.M.; Yuan, S.; Carpenter, L.L. Identification of clinical features and biomarkers that may inform a personalized approach to rTMS for depression. Pers. Med. Psychiatry 2019, 17–18, 4–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folmer, R.L.; Carroll, J.R.; Rahim, A.; Shi, Y.; Martin, W.H. Effects of repetitive transcranial magnetic stimulation (rTMS) on chronic tinnitus. Acta Otolaryngol. 2006, 126, 96–101. [Google Scholar] [CrossRef]
- Fregni, F.; Marcondes, R.; Boggio, P.; Marcolin, M.A.; Rigonatti, S.P.; Sanchez, T.G.; Nitsche, M.A.; Pascual-Leone, A. Transient tinnitus suppression induced by repetitive transcranial magnetic stimulation and transcranial direct current stimulation. Eur. J. Neurol. 2006, 13, 996–1001. [Google Scholar] [CrossRef]
- Lorenz, I.; Müller, N.; Schlee, W.; Langguth, B.; Weisz, N. Short-Term Effects of Single Repetitive TMS Sessions on Auditory Evoked Activity in Patients With Chronic Tinnitus. J. Neurophysiol. 2010, 104, 1497–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meeus, O.; Blaivie, C.; Ost, J.; De Ridder, D.; Van de Heyning, P. Influence of Tonic and Burst Transcranial Magnetic Stimulation Characteristics on Acute Inhibition of Subjective Tinnitus. Otol. Neurotol. 2009, 30, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Plewnia, C.; Bartels, M.; Gerloff, C. Transient suppression of tinnitus by transcranial magnetic stimulation. Ann. Neurol. 2003, 53, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Müller, N.; Lorenz, I.; Langguth, B.; Weisz, N. rTMS Induced Tinnitus Relief Is Related to an Increase in Auditory Cortical Alpha Activity. PLoS ONE 2013, 8, e55557. [Google Scholar] [CrossRef] [PubMed]
- Kreuzer, P.M.; Poeppl, T.B.; Rupprecht, R.; Vielsmeier, V.; Lehner, A.; Langguth, B.; Schecklmann, M. Individualized Repetitive Transcranial Magnetic Stimulation Treatment in Chronic Tinnitus? Front. Neurol. 2017, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoisswohl, S.; Langguth, B.; Schecklmann, M. Short-Term Tinnitus Suppression With Electric-Field Guided rTMS for Individualizing rTMS Treatment: A Technical Feasibility Report. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef]
- Ridder, D.E.; Evanneste, S.; Elangguth, B.; Ellinas, R. Thalamocortical Dysrhythmia: A Theoretical Update in Tinnitus. Front. Neurol. 2015, 6, 124. [Google Scholar] [CrossRef]
- Llinás, R.; Urbano, F.J.; Leznik, E.; Ramírez, R.R.; van Marle, H.J. Rhythmic and dysrhythmic thalamocortical dynamics: GABA systems and the edge effect. Trends Neurosci. 2005, 28, 325–333. [Google Scholar] [CrossRef]
- Llinás, R.R.; Ribary, U.; Jeanmonod, D.; Kronberg, E.; Mitra, P.P. Thalamocortical dysrhythmia: A neurological and neuropsychiatric syndrome characterized by magnetoencephalography. Proc. Natl. Acad. Sci. USA 1999, 96, 15222–15227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisz, N.; Dohrmann, K.; Elbert, T. The relevance of spontaneous activity for the coding of the tinnitus sensation. Prog. Brain Res. 2007, 166, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Adjamian, P.; Sereda, M.; Zobay, O.; Hall, D.A.; Palmer, A.R. Neuromagnetic Indicators of Tinnitus and Tinnitus Masking in Patients with and without Hearing Loss. J. Assoc. Res. Otolaryngol. 2012, 13, 715–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balkenhol, T.; Wallhäusser-Franke, E.; Delb, W. Psychoacoustic Tinnitus Loudness and Tinnitus-Related Distress Show Different Associations with Oscillatory Brain Activity. PLoS ONE 2013, 8, e53180. [Google Scholar] [CrossRef] [PubMed]
- Moazami-Goudarzi, M.; Michels, L.; Weisz, N.; Jeanmonod, D. Temporo-insular enhancement of EEG low and high frequencies in patients with chronic tinnitus. QEEG study of chronic tinnitus patients. BMC Neurosci. 2010, 11, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlee, W.; Schecklmann, M.; Lehner, A.; Kreuzer, P.M.; Vielsmeier, V.; Poeppl, T.B.; Langguth, B. Reduced Variability of Auditory Alpha Activity in Chronic Tinnitus. Neural Plast. 2014, 2014, 1–9. [Google Scholar] [CrossRef]
- Weisz, N.; Müller, S.; Schlee, W.; Dohrmann, K.; Hartmann, T.; Elbert, T. The Neural Code of Auditory Phantom Perception. J. Neurosci. 2007, 27, 1479–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisz, N.; Moratti, S.; Meinzer, M.; Dohrmann, K.; Elbert, T. Tinnitus Perception and Distress Is Related to Abnormal Spontaneous Brain Activity as Measured by Magnetoencephalography. PLoS Med. 2005, 2, e153. [Google Scholar] [CrossRef]
- De Ridder, D.; Congedo, M.; Vanneste, S. The neural correlates of subjectively perceived and passively matched loudness perception in auditory phantom perception. Brain Behav. 2015, 5, e00331. [Google Scholar] [CrossRef]
- Van Der Loo, E.; Gais, S.; Congedo, M.; Vanneste, S.; Plazier, M.; Menovsky, T.; Van De Heyning, P.; De Ridder, D. Tinnitus Intensity Dependent Gamma Oscillations of the Contralateral Auditory Cortex. PLoS ONE 2009, 4, e7396. [Google Scholar] [CrossRef] [Green Version]
- Noda, Y. Toward the establishment of neurophysiological indicators for neuropsychiatric disorders using transcranial magnetic stimulation-evoked potentials: A systematic review. Psychiatry Clin. Neurosci. 2020, 74, 12–34. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Wang, S.; Yi, W.; Zhang, C.; He, H. The lasting effects of 1Hz repetitive transcranial magnetic stimulation on resting state EEG in healthy subjects. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; Volume 2019, pp. 5918–5922. [Google Scholar]
- Thut, G.; Pascual-Leone, A. A Review of Combined TMS-EEG Studies to Characterize Lasting Effects of Repetitive TMS and Assess Their Usefulness in Cognitive and Clinical Neuroscience. Brain Topogr. 2009, 22, 219–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, J.; Tremblay, S.; Daskalakis, Z.J. The Current and Future Potential of Transcranial Magnetic Stimulation with Electroencephalography in Psychiatry. Clin. Pharmacol. Ther. 2019, 106, 734–746. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, S.; Rogasch, N.C.; Premoli, I.; Blumberger, D.M.; Casarotto, S.; Chen, R.; Di Lazzaro, V.; Farzan, F.; Ferrarelli, F.; Fitzgerald, P.B.; et al. Clinical utility and prospective of TMS–EEG. Clin. Neurophysiol. 2019, 130, 802–844. [Google Scholar] [CrossRef]
- Eschecklmann, M.; Elehner, A.; Egollmitzer, J.; Eschmidt, E.; Eschlee, W.; Elangguth, B. Repetitive transcranial magnetic stimulation induces oscillatory power changes in chronic tinnitus. Front. Cell. Neurosci. 2015, 9, 421. [Google Scholar] [CrossRef] [Green Version]
- Langguth, B.; Landgrebe, M.; Frank, E.; Schecklmann, M.; Sand, P.; Vielsmeier, V.; Hajak, G.; Kleinjung, T. Efficacy of different protocols of transcranial magnetic stimulation for the treatment of tinnitus: Pooled analysis of two randomized controlled studies. World J. Biol. Psychiatry 2012, 15, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Schecklmann, M.; Landgrebe, M.; Kleinjung, T.; Frank, E.; Sand, P.G.; Rupprecht, R.; Eichhammer, P.; Hajak, G.; Langguth, B. Changes in motor cortex excitability associated with temporal repetitive transcranial magnetic stimulation in tinnitus: Hints for cross-modal plasticity? BMC Neurosci. 2014, 15, 71. [Google Scholar] [CrossRef] [Green Version]
- Kleinjung, T.; Fischer, B.; Langguth, B.; Sand, P.; Hajak, G.; Dvořáková, J.; Eichhammer, P. Validierung einer deutschsprachigen Version des “Tinnitus Handicap Inventory”. Psychiatr. Prax. 2007, 34, 140–142. [Google Scholar] [CrossRef]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch. Otolaryngol. Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef]
- Langguth, B.; Goodey, R.; Azevedo, A.; Bjorne, A.; Cacace, A.; Crocetti, A.; Del Bo, L.; De Ridder, D.; Diges, I.; Elbert, T.; et al. Consensus for tinnitus patient assessment and treatment outcome measurement: Tinnitus Research Initiative meeting, Regensburg, July 2006. Neural Regen. 2007, 166, 525–536. [Google Scholar] [CrossRef] [Green Version]
- Genitsaridi, E.; Partyka, M.; Gallus, S.; Lopez-Escamez, J.A.; Schecklmann, M.; Mielczarek, M.; Trpchevska, N.; Santacruz, J.L.; Schoisswohl, S.; Riha, C.; et al. Standardised profiling for tinnitus research: The European School for Interdisciplinary Tinnitus Research Screening Questionnaire (ESIT-SQ). Hear. Res. 2019, 377, 353–359. [Google Scholar] [CrossRef]
- Chen, R.; Classen, J.; Gerloff, C.; Celnik, P.; Wassermann, E.M.; Hallett, M.; Cohen, L.G. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology 1997, 48, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Kumru, H.; Albu, S.; Rothwell, J.; Leon, D.; Flores, C.; Opisso, E.; Tormos, J.M.; Valls-Sole, J. Modulation of motor cortex excitability by paired peripheral and transcranial magnetic stimulation. Clin. Neurophysiol. 2017, 128, 2043–2047. [Google Scholar] [CrossRef] [Green Version]
- Delorme, A.; Makeig, S. EEGLAB: An Open Source Toolbox for Analysis of Single-Trial EEG Dynamics Including Independent Component Analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Perrin, F.; Pernier, J.; Bertrand, O.; Echallier, J. Spherical splines for scalp potential and current density mapping. Electroencephalogr. Clin. Neurophysiol. 1989, 72, 184–187. [Google Scholar] [CrossRef]
- Oostenveld, R.; Fries, P.; Maris, E.; Schoffelen, J.-M. FieldTrip: Open Source Software for Advanced Analysis of MEG, EEG, and Invasive Electrophysiological Data. Comput. Intell. Neurosci. 2010, 2011, 1–9. [Google Scholar] [CrossRef]
- Vanneste, S.; Van De Heyning, P.; De Ridder, D. The neural network of phantom sound changes over time: A comparison between recent-onset and chronic tinnitus patients. Eur. J. Neurosci. 2011, 34, 718–731. [Google Scholar] [CrossRef]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Siebner, H.R.; Lang, N.; Rizzo, V.; Nitsche, M.A.; Paulus, W.; Lemon, R.N.; Rothwell, J.C. Preconditioning of Low-Frequency Repetitive Transcranial Magnetic Stimulation with Transcranial Direct Current Stimulation: Evidence for Homeostatic Plasticity in the Human Motor Cortex. J. Neurosci. 2004, 24, 3379–3385. [Google Scholar] [CrossRef] [PubMed]
- Maeda, F.; Keenan, J.P.; Tormos, J.M.; Topka, H.; Pascual-Leone, A. Interindividual variability of the modulatory effects of repetitive transcranial magnetic stimulation on cortical excitability. Exp. Brain Res. 2000, 133, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Nettekoven, C.; Volz, L.J.; Leimbach, M.; Pool, E.-M.; Rehme, A.K.; Eickhoff, S.B.; Fink, G.R.; Grefkes, C. Inter-individual variability in cortical excitability and motor network connectivity following multiple blocks of rTMS. NeuroImage 2015, 118, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sommer, M.; Wu, T.; Tergau, F.; Paulus, W. Intra- and interindividual variability of motor responses to repetitive transcranial magnetic stimulation. Clin. Neurophysiol. 2002, 113, 265–269. [Google Scholar] [CrossRef]
- Soleimani, R.; Jalali, M.M.; Hasandokht, T. Therapeutic impact of repetitive transcranial magnetic stimulation (rTMS) on tinnitus: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2015, 273, 1663–1675. [Google Scholar] [CrossRef] [PubMed]
- Lehner, A.; Schecklmann, M.; Poeppl, T.B.; Kreuzer, P.M.; Peytard, J.; Frank, E.; Langguth, B. Efficacy and Safety of Repeated Courses of rTMS Treatment in Patients with Chronic Subjective Tinnitus. BioMed. Res. Int. 2015, 2015, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rachid, F. Maintenance repetitive transcranial magnetic stimulation (rTMS) for relapse prevention in with depression: A review. Psychiatry Res. 2018, 262, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Silvanto, J.; Pascual-Leone, A. State-Dependency of Transcranial Magnetic Stimulation. Brain Topogr. 2008, 21, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Weisz, N.; Lüchinger, C.; Thut, G.; Müller, N. Effects of individual alpha rTMS applied to the auditory cortex and its implications for the treatment of chronic tinnitus. Hum. Brain Mapp. 2014, 35, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Weisz, N.; Steidle, L.; Lorenz, I. Formerly known as inhibitory: Effects of 1-Hz rTMS on auditory cortex are state-dependent: Formerly known as inhibitory. Eur. J. Neurosci. 2012, 36, 2077–2087. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Verstraeten, E.; Van der Kelen, K.; De Mulder, G.; Sunaert, S.; Verlooy, J.; Van de Heyning, P.; Moller, A. Transcranial Magnetic Stimulation for Tinnitus: Influence of Tinnitus Duration on Stimulation Parameter Choice and Maximal Tinnitus Suppression. Otol. Neurotol. 2005, 26, 616–619. [Google Scholar] [CrossRef]
- King, R.O.C.; Shekhawat, G.S.; King, C.; Chan, E.; Kobayashi, K.; Searchfield, G.D. The Effect of Auditory Residual Inhibition on Tinnitus and the Electroencephalogram. Ear Hear. 2021, 42, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Thut, G.; Veniero, D.; Romei, V.; Miniussi, C.; Schyns, P.; Gross, J. Rhythmic TMS Causes Local Entrainment of Natural Oscillatory Signatures. Curr. Biol. 2011, 21, 1176–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, J.; Makeig, S.; Hoopes, D.; Gola, M. Can Oscillatory Alpha-Gamma Phase-Amplitude Coupling be Used to Understand and Enhance TMS Effects? Front. Hum. Neurosci. 2019, 13, 263. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (female) | 22 (5) | |||
| Handedness (left/right/both) (4 missing) | 0/14/4 | |||
| Tinnitus laterality (left/right/both/inside head) (4 missing) | 1/1/14/2 | |||
| Tinnitus loudness fluctuation (yes/no) (4 missing) | 14/4 | |||
| M ± SD | Md | Min | Max | |
| Age (years) | 57.05 ± 6.79 | 57.50 | 43.00 | 69.00 |
| Tinnitus duration (months) (2 missing) | 131.65 ± 116.79 | 102.00 | 5.00 | 420.00 |
| Hearing loss left (dB) (8 missing) | 23.42 ± 9.72 | 22.22 | 7.22 | 41.67 |
| Hearing loss right (dB) (8 missing) | 27.87 ± 14.29 | 23.06 | 7.78 | 61.88 |
| THI score (0–100) | 58.49 ± 19.55 | 58.00 | 30.00 | 90.00 |
| Tinnitus loudness (%) (6 missing) | 70.31 ± 19.87 | 80.00 | 30.00 | 90.00 |
| RMT (%) | 33.95 ± 5.33 | 33.00 | 25.00 | 46.00 |
| RMT (%) + EEG cap | 41.91 ± 9.65 | 41.00 | 30.00 | 66.00 |
| Electrical field (V/m) | 54.47 ± 13.90 | 52.50 | 27.00 | 86.00 |
| Electrical field (V/m) + EEG cap | 66.66 ± 15.38 | 66.25 | 44.00 | 99.00 |
| Subject | Behavioral Responder | Alpha (8–12.5 Hz)/Gamma (30.5–44 Hz) | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | 12.86 | - | - | Left | - | ↓ γ | ↑ α ↓ γ | |
| Right | 17.15 | - | - | Right | - | ↓ γ | - | |
| 2 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | ↑ α ↓ γ | ↑ α ↓ γ | - | |||||
| Right | - | - | - | |||||
| 3 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | 3.98 | - | 3.71 | Left | ↑ α ↓ γ | ↑ α | - | |
| Right | - | - | - | Right | ↓ γ | - | - | |
| 4 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | - | 10.35 | - | Left | ↑ α ↓ γ | - | - | |
| Right | - | 9.28 | 25.71 | Right | - | - | - | |
| 5 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | - | 16.42 | - | Left | ↑ α | ↓ γ | ↑ α | |
| Right | 10 | 16.79 | 21.42 | Right | - | - | - | |
| 6 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | - | 10.71 | - | Left | ↑ α | - | ↑ α | |
| Right | - | - | - | Right | - | ↑ α ↓ γ | - | |
| 7 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | - | ↑ α | - | |||||
| Right | - | ↑ α | ↑ α ↓ γ | |||||
| 8 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | - | 6.07 | 8.93 | Left | - | ↑ α ↓ γ | ↓ γ | |
| Right | - | 4.64 | 9.28 | Right | - | ↑ α | - | |
| 9 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | - | - | 3.93 | Left | ↑ α ↓ γ | ↑ α ↓ γ | ↑ α ↓ γ | |
| Right | 7.55 | - | - | Right | ↓ γ | - | - | |
| 10 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | 15.36 | - | 5.71 | Left | ↓ γ | ↑ α | ↓ γ | |
| Right | - | - | - | Right | - | ↓ γ | ↑ α ↓ γ | |
| 11 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | ↑ α | - | - | |||||
| Right | ↓ γ | ↑ α ↓ γ | ↑ α | |||||
| 12 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | - | - | - | |||||
| Right | - | ↑ α | ↓ γ | |||||
| 13 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | ↓ γ | ↑ α ↓ γ | - | |||||
| Right | ↑ α ↓ γ | ↓ γ | - | |||||
| 14 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | ↑ α | ↓ γ | ↑ α ↓ γ | |||||
| Right | ↓ γ | - | ↑ α | |||||
| 15 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | ↓ γ | ↑ α | - | |||||
| Right | ↓ γ | - | - | |||||
| 16 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | - | 5 | 12.85 | Left | - | ↑ α ↓ γ | - | |
| Right | - | - | 10 | Right | - | ↑ α | ↓ γ | |
| 17 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | - | ↓ γ | - | |||||
| Right | ↑ α | ↓ γ | ↑ α ↓ γ | |||||
| 18 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | ↓ γ | ↓ γ | ↑ α ↓ γ | |||||
| Right | ↑ α ↓ γ | ↑ α | - | |||||
| 19 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | - | 13.57 | 13.57 | Left | ↑ α | ↓ γ | - | |
| Right | - | - | - | Right | ↑ α | ↓ γ | ↑ α | |
| 20 | - | 1 Hz | 10 Hz | 20 Hz | ||||
| Left | ↓ γ | ↓ γ | - | |||||
| Right | - | - | - | |||||
| 21 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | - | - | - | Left | - | - | ↓ γ | |
| Right | 7.14 | - | 3.93 | Right | ↓ γ | ↓ γ | ↓ γ | |
| 22 | 1 Hz | 10 Hz | 20 Hz | 1 Hz | 10 Hz | 20 Hz | ||
| Left | - | - | 7.85 | Left | ↓ γ | ↑ α ↓ γ | - | |
| Right | - | - | - | Right | - | - | - | |
| Behavioral Responder | ↑ Alpha | ↓ Gamma | |
|---|---|---|---|
| Total number of responders (N) | 12 | 20 | 22 |
| Number of responders per protocol (N) | |||
| Left 1 Hz | 3 | 9 | 10 |
| Right 1 Hz | 4 | 4 | 8 |
| Left 10 Hz | 6 | 10 | 13 |
| Right 10 Hz | 3 | 7 | 8 |
| Left 20 Hz | 7 | 6 | 7 |
| Right 20 Hz | 5 | 6 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoisswohl, S.; Langguth, B.; Hebel, T.; Abdelnaim, M.A.; Volberg, G.; Schecklmann, M. Heading for Personalized rTMS in Tinnitus: Reliability of Individualized Stimulation Protocols in Behavioral and Electrophysiological Responses. J. Pers. Med. 2021, 11, 536. https://doi.org/10.3390/jpm11060536
Schoisswohl S, Langguth B, Hebel T, Abdelnaim MA, Volberg G, Schecklmann M. Heading for Personalized rTMS in Tinnitus: Reliability of Individualized Stimulation Protocols in Behavioral and Electrophysiological Responses. Journal of Personalized Medicine. 2021; 11(6):536. https://doi.org/10.3390/jpm11060536
Chicago/Turabian StyleSchoisswohl, Stefan, Berthold Langguth, Tobias Hebel, Mohamed A. Abdelnaim, Gregor Volberg, and Martin Schecklmann. 2021. "Heading for Personalized rTMS in Tinnitus: Reliability of Individualized Stimulation Protocols in Behavioral and Electrophysiological Responses" Journal of Personalized Medicine 11, no. 6: 536. https://doi.org/10.3390/jpm11060536
APA StyleSchoisswohl, S., Langguth, B., Hebel, T., Abdelnaim, M. A., Volberg, G., & Schecklmann, M. (2021). Heading for Personalized rTMS in Tinnitus: Reliability of Individualized Stimulation Protocols in Behavioral and Electrophysiological Responses. Journal of Personalized Medicine, 11(6), 536. https://doi.org/10.3390/jpm11060536