
Clinical and Radiological Outcomes after Knee Arthroplasty with Patient-Specific versus Off-the-Shelf Knee Implants: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Quality Assessment
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
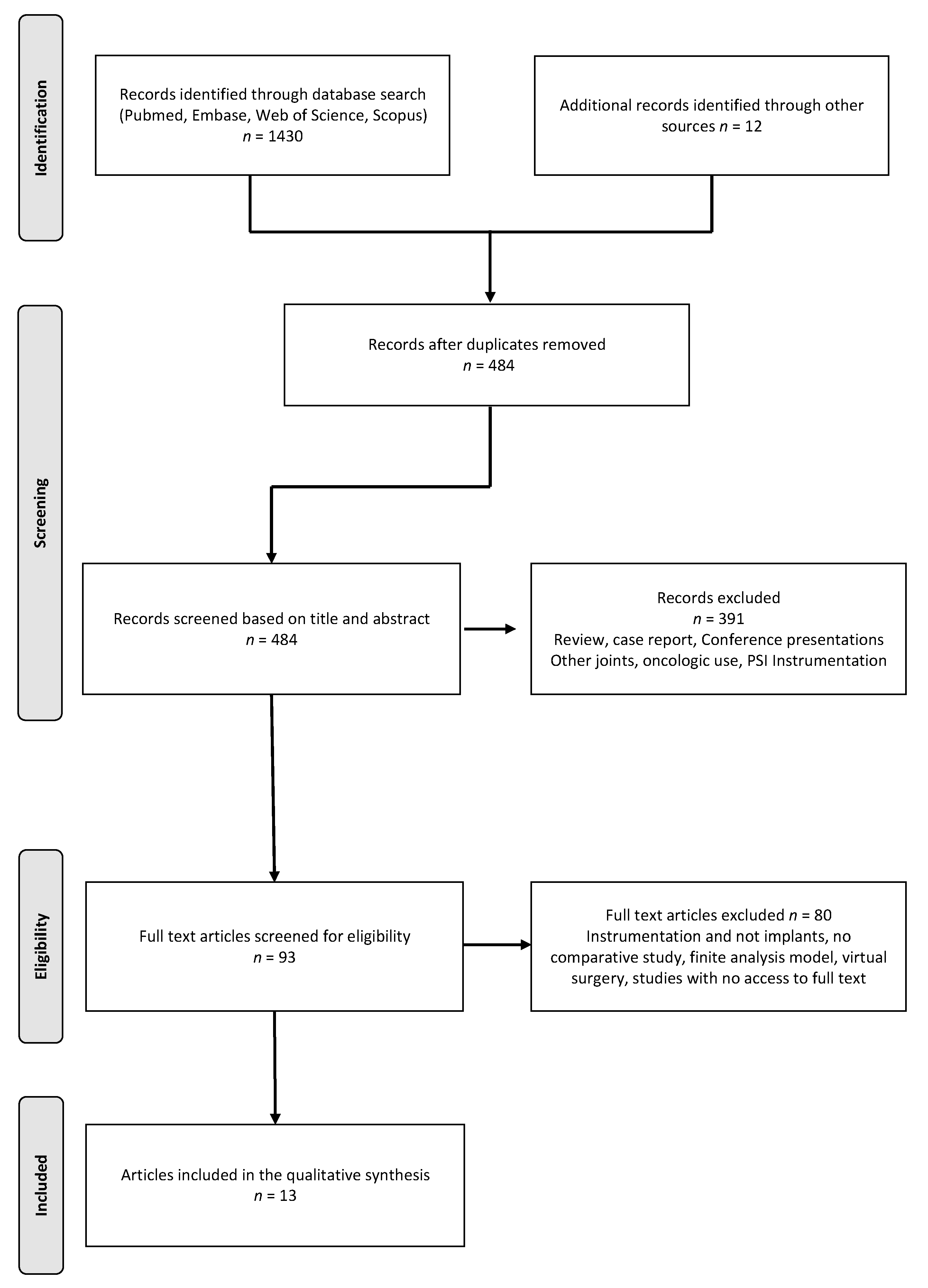
3.1. Search Results and Characteristics of Included Studies
3.2. Patient Characteristics
3.3. Implant Types
3.4. Clinical Outcome
3.5. Revisions and Reoperations
3.6. Radiological Outcomes
3.7. Procedure-Related Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lutzner, J.; Hubel, U.; Kirschner, S.; Gunther, K.P.; Krummenauer, F. Long-term results in total knee arthroplasty. A meta-analysis of revision rates and functional outcome. Chirurg 2011, 82, 618–624. [Google Scholar]
- Callahan, C.M.; Drake, B.G.; A Heck, D.; Dittus, R.S. Patient outcomes following tricompartmental total knee replacement. A meta-analysis. JAMA 1994, 271, 1349–1357. [Google Scholar] [CrossRef]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; A Salomon, J.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Hofmann, S.; Seitlinger, G.; Djahani, O.; Pietsch, M. The painful knee after TKA: A diagnostic algorithm for failure analysis. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1442–1452. [Google Scholar] [CrossRef]
- Mandalia, V.; Eyres, K.; Schranz, P.; Toms, A.D. Evaluation of patients with a painful total knee replacement. J. Bone Jt. Surg. Br. Vol. 2008, 90, 265–271. [Google Scholar] [CrossRef]
- Toms, A.D.; Mandalia, V.; Haigh, R.; Hopwood, B.; Toms, A.D.; Mandalia, V.; Haigh, R.; Hopwood, B. The management of patients with painful total knee replacement. J. Bone Jt. Surg. Br. Vol. 2009, 91, 143–150. [Google Scholar] [CrossRef]
- Beswick, A.D.; Wylde, V.; Gooberman-Hill, R.; Blom, A.W.; Dieppe, P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open 2012, 2, e000435. [Google Scholar] [CrossRef]
- Baker, P.N.; van der Meulen, J.H.; Lewsey, J.; Gregg, P.J.; National Joint Registry for England and Wales. The role of pain and function in determining patient satisfaction after total knee replacement. Data from the National Joint Registry for England and Wales. J. Bone Jt. Surg. Br. 2007, 89, 893–900. [Google Scholar] [CrossRef]
- Vince, K.G.; Abdeen, A.; Sugimori, T. The unstable total knee arthroplasty: Causes and cures. J. Arthroplast. 2006, 21, 44–49. [Google Scholar] [CrossRef]
- Sharkey, P.F.; Hozack, W.J.; Rothman, R.H.; Shastri, S.; Jacoby, S.M. Why Are Total Knee Arthroplasties Failing Today? Clin. Orthop. Relat. Res. 2002, 404, 7–13. [Google Scholar] [CrossRef]
- Sharkey, P.F.; Lichstein, P.M.; Shen, C.; Tokarski, A.T.; Parvizi, J. Why Are Total Knee Arthroplasties Failing Today—Has Anything Changed After 10 Years? J. Arthroplast. 2014, 29, 1774–1778. [Google Scholar] [CrossRef]
- Budhiparama, N.C.; Lumban-Gaol, I.; Ifran, N.N.; De Groot, P.C.; Nelissen, R.G. Anthropometric Measurement of Caucasian and Asian Knees, Mismatch with Knee Systems? Orthop. J. Sports Med. 2020, 8, 8. [Google Scholar] [CrossRef]
- Noble, P.C.; Scuderi, G.R.; Brekke, A.C.; Sikorskii, A.; Benjamin, J.B.; Lonner, J.H.; Chadha, P.; Daylamani, D.A.; Scott, N.W.; Bourne, R.B. Development of a New Knee Society Scoring System. Clin. Orthop. Relat. Res. 2012, 470, 20–32. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological Index for Non-Randomized Studies (MINORS): Development and Validation of a New Instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Arbab, D.; Reimann, P.; Brucker, M.; Bouillon, B.; Lüring, C. Alignment in total knee arthroplasty—A comparison of patient-specific implants with the conventional technique. Knee 2018, 25, 882–887. [Google Scholar] [CrossRef]
- Buch, R.; Schroeder, L.; Buch, R.; Eberle, R. Does Implant Design Affect Hospital Metrics and Patient Outcomes? TKA Utilizing a “Fast-Track” Protocol. Reconstr. Rev. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Culler, S.D.; Martin, G.M.; Swearingen, A. Comparison of adverse events rates and hospital cost between customized individually made implants and standard off-the-shelf implants for total knee arthroplasty. Arthroplast. Today 2017, 3, 257–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivie, C.B.; Probst, P.J.; Bal, A.K.; Stannard, J.T.; Crist, B.D.; Bal, B.S. Improved Radiographic Outcomes With Patient-Specific Total Knee Arthroplasty. J. Arthroplast. 2014, 29, 2100–2103. [Google Scholar] [CrossRef] [PubMed]
- Meheux, C.J.; Park, K.J.; Clyburn, T.A. A Retrospective Study Comparing a Patient-specific Design Total Knee Arthroplasty With an Off-the-Shelf Design: Unexpected Catastrophic Failure Seen in the Early Patient-specific Design. JAAOS Glob. Res. Rev. 2019, 3, e19.00143. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.I.; Blau, B.E. The Economic Value of Customized versus Off-the-Shelf Knee Implants in Medicare Fee-for-Service Beneficiaries. Am. Health Drug Benefits 2019, 12, 66–73. [Google Scholar] [PubMed]
- Reimann, P.; Brucker, M.; Arbab, D.; Lüring, C. Patient satisfaction—A comparison between patient-specific implants and conventional total knee arthroplasty. J. Orthop. 2019, 16, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, L.; Martin, G. In Vivo Tibial Fit and Rotational Analysis of a Customized, Patient-Specific TKA versus Off-the-Shelf TKA. J. Knee Surg. 2018, 32, 499–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzkopf, R.; Brodsky, M.; Garcia, G.A.; Gomoll, A.H. Surgical and Functional Outcomes in Patients Undergoing Total Knee Replacement With Patient-Specific Implants Compared With “Off-the-Shelf” Implants. Orthop. J. Sports Med. 2015, 3. [Google Scholar] [CrossRef]
- Wheatley, B.; Nappo, K.; Fisch, J.; Rego, L.; Shay, M.; Cannova, C. Early outcomes of patient-specific posterior stabilized total knee arthroplasty implants. J. Orthop. 2019, 16, 14–18. [Google Scholar] [CrossRef]
- White, P.B.; Ranawat, A.S. Patient-Specific Total Knees Demonstrate a Higher Manipulation Rate Compared to “Off-the-Shelf Implants”. J. Arthroplast. 2016, 31, 107–111. [Google Scholar] [CrossRef]
- Demange, M.K.; Von Keudell, A.; Probst, C.; Yoshioka, H.; Gomoll, A.H. Patient-specific implants for lateral unicompartmental knee arthroplasty. Int. Orthop. 2015, 39, 1519–1526. [Google Scholar] [CrossRef]
- Mayer, C.; Bittersohl, B.; Haversath, M.; Franz, A.; Krauspe, R.; Jäger, M.; Zilkens, C. The learning curve of patient-specific unikondylar arthroplasty may be advantageous to off-the-shelf implants: A preliminary study. J. Orthop. 2020, 22, 256–260. [Google Scholar] [CrossRef]
- Steinert, A.F.; Sefrin, L.; Jansen, B.; Schröder, L.; Holzapfel, B.M.; Arnholdt, J.; Rudert, M. Patient-specific cruciate-retaining total knee replacement with individualized implants and instruments (iTotal™ CR G2). Oper. Orthop. Traumatol. 2021, 33, 170–180. [Google Scholar] [CrossRef]
- Neginhal, V.; Kurtz, W.; Schroeder, L. Patient Satisfaction, Functional Outcomes, and Survivorship in Patients with a Customized Posterior-Stabilized Total Knee Replacement. JBJS Rev. 2020, 8, e19.00104. [Google Scholar] [CrossRef] [PubMed]
- Huber, B.; Tait, R.; Kurtz, W.; Burkhardt, J.; Swanson, T.; Clyburn, T. Outcomes after Customized Individually Made Total Knee Arthroplasty. In Proceedings of the ICJR Pan Pacific Congress 2016, Waikoloa, HI, USA, 10–13 August 2016. [Google Scholar]
- Kaelin, R.; Vogel, N.; Arnold, M.P. Clinical and Patient-Reported Short-Term Results after Customized Individually Made Total Knee Arthroplasty. Swiss Med. Wkly. 2019, 149, 62s. [Google Scholar]
- Zeller, I.M.; Sharma, A.; Kurtz, W.B.; Anderle, M.R.; Komistek, R.D. Customized versus Patient-Sized Cruciate-Retaining Total Knee Arthroplasty: An InVivo Kinematics Study Using Mobile Fluoroscopy. J. Arthroplast. 2017, 32, 1344–1350. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Bunn, A.; Bugbee, W.D.; Colwell, C.W.; D’Lima, D.D. Patient-specific implants with custom cutting blocks better approximate natural knee kinematics than standard TKA without custom cutting blocks. Knee 2015, 22, 624–629. [Google Scholar] [CrossRef]
- Katthagen, B.-D.; Chatziandreou, I. Comparison of Hospital Metrics and Patient Reported Outcomes for Patients with Customized, Individually Made Vs. Conventional TKA. In Proceedings of the 2015 World Arthroplasty Congress (WAC), Paris, France, 16–18 April 2015. [Google Scholar]
- Kay, A.B.; Kurtz, W.B.; Martin, G.M.; Huber, B.M.; Tait, R.J.; A Clyburn, T. Manipulation Rate Is Not Increased After Customized Total Knee Arthroplasty. Reconstr. Rev. 2018, 8, 8. [Google Scholar] [CrossRef] [Green Version]
- Ritter, M.A.; Davis, K.E.; Meding, J.B.; Pierson, J.L.; Berend, M.E.; Malinzak, R.A. The Effect of Alignment and BMI on Failure of Total Knee Replacement. J. Bone Jt. Surg. Am. Vol. 2011, 93, 1588–1596. [Google Scholar] [CrossRef]
- Fang, D.M.; Ritter, M.A.; Davis, K.E. Coronal Alignment in Total Knee Arthroplasty Just How Important is it? J. Arthroplast. 2009, 24, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Levengood, G.A.; Dupee, J. Accuracy of Coronal Plane Mechanical Alignment in a Customized, Individually Made Total Knee Replacement with Patient-Specific Instrumentation. J. Knee Surg. 2018, 31, 792–796. [Google Scholar] [CrossRef] [Green Version]
- Arnholdt, J.; Kamawal, Y.; Holzapfel, B.M.; Ripp, A.; Rudert, M.; Steinert, A.F. Evaluation of implant fit and frontal plane alignment after bi-compartmental knee arthroplasty using patient-specific instruments and implants. Arch. Med Sci. 2018, 14, 1424–1431. [Google Scholar] [CrossRef]
- Thienpont, E.; Schwab, P.E.; Fennema, P. Efficacy of Patient-Specific Instruments in Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. J. Bone Jt. Surg. Am. 2017, 99, 521–530. [Google Scholar] [CrossRef]
- Abdel, M.P.; Ollivier, M.; Parratte, S.; Trousdale, R.T.; Berry, D.J.; Pagnano, M.W. Effect of Postoperative Mechanical Axis Alignment on Survival and Functional Outcomes of Modern Total Knee Arthroplasties with Cement A Concise Follow-up at 20 Years. J. Bone Jt. Surg. Am Vol. 2018, 100, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Howell, S.M.; Shelton, T.J.; Hull, M.L. Implant Survival and Function Ten Years After Kinematically Aligned Total Knee Arthroplasty. J. Arthroplast. 2018, 33, 3678–3684. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, M.P.; Beckers, L.; Leon, A.; Chauveau, J.; Muller, J.H.; Tibesku, C.O.; Ait-Si-Selmi, T. Custom total knee arthroplasty facilitates restoration of constitutional coronal alignment. Knee Surg. Sports Traumatol. Arthrosc. 2020. Online ahead of print. [Google Scholar] [CrossRef]
- Panni, A.S.; Ascione, F.; Rossini, M.; Braile, A.; Corona, K.; Vasso, M.; Hirschmann, M.T. Tibial internal rotation negatively affects clinical outcomes in total knee arthroplasty: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 1636–1644. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, D.; Rowley, D.I. Internal rotational error of the tibial component is a major cause of pain after total knee replacement. J. Bone Jt. Surg. Br. Vol. 2010, 92, 1238–1244. [Google Scholar] [CrossRef]
- Carpenter, D.P.; Holmberg, R.R.; Quartulli, M.J.; Barnes, C.L. Tibial Plateau Coverage in UKA: A Comparison of Patient Specific and Off-The-Shelf Implants. J. Arthroplast. 2014, 29, 1694–1698. [Google Scholar] [CrossRef]
- Mahoney, O.M.; Kinsey, T. Overhang of the Femoral Component in Total Knee Arthroplasty: Risk Factors and Clinical Consequences. J. Bone Jt. Surg. Am. Vol. 2010, 92, 1115–1121. [Google Scholar] [CrossRef]
- Kim, T.K.; Phillips, M.; Bhandari, M.; Watson, J.; Malhotra, R. What Differences in Morphologic Features of the Knee Exist Among Patients of Various Races? A Systematic Review. Clin. Orthop. Relat. Res. 2017, 475, 170–182. [Google Scholar] [CrossRef] [Green Version]
- Yue, B.; Varadarajan, K.M.; Ai, S.; Tang, T.; Rubash, H.E.; Li, G. Differences of Knee Anthropometry Between Chinese and White Men and Women. J. Arthroplast. 2011, 26, 124–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, M.; Zingde, S.; Steinert, A.; Kurtz, W.; Koeck, F.; Beckmann, J. What Is the Possible Impact of High Variability of Distal Femoral Geometry on TKA? A CT Data Analysis of 24,042 Knees. Clin. Orthop. Relat. Res. 2019, 477, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, A.A.; Bachus, K.N.; Wyatt, R.W. Effect of the tibial cut on subsidence following total knee arthroplasty. Clin. Orthop. Relat. Res. 1991, 269, 63–69. [Google Scholar] [CrossRef]
- Namin, A.T.; Jalali, M.S.; Vahdat, V.; Bedair, H.S.; O’Connor, M.I.; Kamarthi, S.; Isaacs, J.A. Adoption of New Medical Technologies: The Case of Customized Individually Made Knee Implants. Value Health 2019, 22, 423–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author (Year) | Implant Type | Outcome Measurements | Study Design | Studied Implants | Level of Evidence | Minors Score | |
|---|---|---|---|---|---|---|---|
| OTS | PSI | ||||||
| Demange (2015) [27] | UKA | Clinical and radiological (coverage, alignment) | Retrospective cohort study | Miller-Galante (Zimmer Biomet) | iUni® G1 (ConforMIS) | III | 16 |
| Mayer (2020) [28] | UKA | Procedure-associated parameters, radiological (alignment), and revision rate | Retrospective cohort study | Oxford® MB (Zimmer Biomet) | iUni® FB (ConforMIS) | III | 20 |
| Arbab (2018) [16] | TKA | Radiological (alignment) | Retrospective cohort study | Triathlon® (Stryker) | iTotal® G2 CR (ConforMIS) | III | 19 |
| Buch (2019) [17] | TKA | Procedure-associated parameters, clinical, MUA, revision rate | Prospective cohort study | Columbus® (B. Braun) or Vanguard® (Zimmer Biomet) | iTotal® G2 CR (ConforMIS) | II | 20 |
| Culler (2017) [18] | TKA | Procedure-related parameters, costs | Prospective cohort study | N/A | N/A | II | 18 |
| Ivie (2014) [19] | TKA | Radiological (alignment) | Retrospective cohort study | NK II® PS (Zimmer Biomet) | iTotal® G2 CR (ConforMIS) | III | 18 |
| Meheux (2019) [20] | TKA | Clinical, revision rate, radiological, procedure-associated parameters | Retrospective cohort study | GENESIS II PS (Smith&Nephew) | iTotal® G2 CR (ConforMIS) and iTotal® G2 plus CR (ConforMIS) | III | 17 |
| O’Connor (2019) [21] | TKA | Procedure parameters | Retrospective cohort study | N/A | iTotal® (ConforMIS) | III | 20 |
| Reimann (2019) [22] | TKA | Clinical | Retrospective cohort study | Triathlon® CR (Stryker) | iTotal® G2 CR (ConforMIS) | III | 16 |
| Schroeder (2019) [23] | TKA | Radiological | Prospective cohort study | NexGen® (Zimmer Biomet) or Vanguard® (Zimmer Biomet) or SIGMA® (DePuy Synthes) | iTotal® CR (ConforMIS) | II | 14 |
| Schwarzkopf (2015) [24] | TKA | Clinical, procedure parameters | Retrospective cohort study | GENESIS II PS (Smith&Nephew) or SIGMA® (DePuy Synthes) or P.F.C.™ SIGMA® (DePuy Synthes) | iTotal® G2 CR (ConforMIS) | III | 15 |
| Wheatley (2019) [25] | TKA | Clinical | Retrospective cohort study | Persona® PS (Zimmer Biomet) | iTotal® PS (ConforMIS) | III | 18 |
| White and Ranawat (2016) [26] | TKA | Clinical radiological | Retrospective cohort study | P.F.C.™ SIGMA® PS FB cem (DePuy Synthes) or P.F.C.™ SIGMA® CR RP non-cem (DePuy Synthes) | iTotal® CR (ConforMIS) | III | 19 |
| Author (Year) | Implant System | Number of Knees | Mean Age, Years (Range) or (SD) | Gender, Female (%) | Mean BMI, kg/m2, (Range) or (SD) | Mean Follow-Up Time, Months (SD) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Demange (2015) [27] | OTS | 20 | 56 (6.9) | ns | 52.6 | 32.7 (7.2) | 75 (20) | |||
| PSI | 33 | 59 (10.9) | 65.6 | 28.7 (5.3) | 37 (8.6) | |||||
| Mayer (2020) [28] | OTS | 20 | 61.4 (8.4) | 45 | 31.3 (5.5) | 18 | ||||
| PSI | 20 | 62.9 (9.2) | 45 | 29.7 (5.6) | 18 | |||||
| Arbab (2018) [16] | OTS | 88 | ||||||||
| PSI | 113 | |||||||||
| Buch (2019) [17] | OTS | 30 | 57.2 (34–67) | ns | 53 | ns | 31 (22–38) | ns | 28 | |
| PSI | 32 | 57.3 (42–72) | 41 | 33.4 (24–53) | 28 | |||||
| Culler (2017) [18] | OTS | 122 | 68.3 (9.5) | ns | 43.9 | ns | 32.3 (7.8) | ns | ||
| PSI | 126 | 69.7 (8.4) | 41.9 | 30.8 (6.5) | ||||||
| Ivie (2014) [19] | OTS | 100 | ||||||||
| PSI | 100 | |||||||||
| Meheux (2019) [20] | OTS | 41 | 63 (10.1) | 34.4 (7.1) | ** | 37.2 (18) | ||||
| PSI 1 | 77 | 62.7 (8.3) | 30.3 (4.5) | 37.2 (18) | ||||||
| PSI 1 | 36 | 62.8 (6.7) | 28.9 (5.2) | 37.2 (18) | ||||||
| O’Connor (2019) [21] | OTS | 3695 | ||||||||
| PSI | 739 | |||||||||
| Reimann (2019) [22] | OTS | 103 | 70.9 (7.1) | *** | 68.4 | ns | 31.4 (5.5) | ns | 33 (7.6) | *** |
| PSI | 125 | 65.5 (9.3) | 63.1 | 30.5 (5.2) | 27.5 (5.7) | |||||
| Schroeder (2019) [23] | PSI | 44 | 70.5 (57–87) | 40.9 | ns | 30.7 (22–49.1) | ||||
| Schwarzkopf (2015) [24] | OTS | 314 | 65 | ns | 65 | 32.11 | ns | |||
| PSI | 307 | 61.4 | 60.2 | 30.85 | ||||||
| Wheatley (2019) [25] | OTS | 124 | 70 (8.5) | * | 64.6 | ns | 30.3 (8.5) | 3 | ||
| PSI | 47 | 66.9 (7.7) | 61.7 | 30.3 (8.5) | 3 | |||||
| White and Ranawat (2016) [26] | OTS, CR | 42 | 59.8 (6.7) | ns | 66.7 | ns | 31.8 (5.5) | ns | 31.2 (8.4) | ns |
| OTS, PS | 11 | 53.9 (6.0) | * | 9.1 | ** | 34.4 (6.5) | ** | 27.6 (4.8) | ||
| PSI, CR | 21 | 59.1 (7.4) | 66.7 | 28.7 (4.8) | 28.8 (4.8) | |||||
| Author (Year) | Implant System | Revision n (%) | Mean ROM (SD) | MUA n (%) | Mean KSS (SD) Preoperative | Mean KSS (SD) 1 Postoperative | FJS 1 | WOMAC Preoperative | WOMAC 1 Postoperative | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Demange (2015) [27] | OTS | 3 (15) | pre: 122° (±9.5°) post: 127° (±7.5°) | |||||||||||
| PSI | 2 (6.1) | pre: 125° (±8.5°) post: 125° (±6.2°) | KS: 48 (16.2) | KS: 94 (7.6) | ||||||||||
| * | ||||||||||||||
| Mayer (2020) [28] | OTS | 2 (10) | ||||||||||||
| PSI | 1 (5) | |||||||||||||
| Buch (2019) [17] | OTS | 2 (6.7) | post: 144° | *** | 1 (3.3) | ns | ||||||||
| PSI | 1 (3.1) | post: 122° | 2 (6.3) | |||||||||||
| Meheux (2019) [20] | OTS | 1 (2.4) | post: 122.7° (±8.2°) | ns | KS: 53.7 (10.1) | ns | KS: 91.9 (11.9) | ns | ||||||
| PSI 1 | 18 (23) | post: 124.2° (±6.0°) | KS: 55.5 (8.3) | KS: 94.6 (7.6) | ||||||||||
| PSI 2 | 0 (0) | post: 123.8° (±7.4°) | KS: 54.2 (6.7) | KS: 95.3 (13.3) | ||||||||||
| Reimann (2019) [22] | OTS | 1 (1.8) | pre: 110° (±13.8°) ns post: 105° (±9.2°) | ns | KS: 78.3 (13.8) FS: 68.0 (18.7) | |||||||||
| PSI | 1 (1.2) | pre: 110° (±15°) ns post: 105° (±9.9°) | KS: 82.4 (13.1) FS: 82.4 (13.1) | ns ** | ||||||||||
| Schwarzkopf (2015) [24] | OTS | |||||||||||||
| PSI | ||||||||||||||
| Wheatley (2019) [25] | OTS | 1 (0.8) | pre: 109.4° (±9.6°) post: 119.3° (±6.1°) | 2 (1.6) | ns | KS: 52.7 (10.8) FS: 56.3 (16.3) | ns | KS: 91.7 (10.2) FS: 77.6 (19.4) | ns | 62.1 (25.7) | ns | |||
| PSI | 1 (2.1) | pre: 109.3° (±9.1°) post: 118.8° (±11.0°) | ns | 1 (2.1) | KS: 55.1 (12.5) FS: 51.8 (16) | KS: 91.1 (9.6) FS: 81.4 (15.3) | 56.0 (26.9) | |||||||
| White and Ranawat (2016) [26] | OTS, CR | 0 (0) | pre: 111° (12°) post: 118° (8°) | ** | 0 | KS: 45.7 (9) FS: 51.1 (10.4) | KS: 95.5 (7.1) FS: 88.9 (13.8) | ns | TS: 52.4 (12.8) PS: 11.1 (2.8) SS: 5.1 (1.4) FS: 36.2 (9.7) | TS: 7.8 (8.4) * PS: 1.2 (2.5) SS: 1.3 (2.1) FS: 5.2 (5.8) | ||||
| OTS, PS | 0 (0) | pre: 114° (10°) post: 120° (4°) | 0 | KS: 45.2 (9) FS: 54.1 (13.2) | KS: 97.3 (3.9) FS: 96.4 (5) | * | TS: 41.3 (9.6) PS: 7.8 (1.9) SS: 3.4 (1.6) FS: 30.1 (7.36) | TS:15.4 (18.3) PS:2.8 (4) SS: 2.2 (2.3) FS: 10.4 (12.9) | ||||||
| PSI, CR | 1 (4.8) | pre: 120° (12°) post: 115° (10°) | ns | 6 (28.6) | KS: 53.6 (8.3) FS: 54 (12.2) | ** ns | KS: 85.4 (15.5) FS: 86 (14.8) | ** | TS: 51.4 (17) PS: 11.5 (3.9) SS: 4.6 (2.5) FS: 35.3 (12.3) | TS: 23.4 (23.1) * PS: 4.8 (5.3) SS: 3 (2.4) FS: 15.2 (16.3) | ||||
| Author (Year) | Implant System | Mean FFC (SD) | Mean FTC (SD) | Mean Tibial Slope (SD) | Mean HKA 1 (SD) or (Range) | > ±3° HKA Outliers | Femorotibial Angle 1 | Optimal Tibial Fit a Resp. Relative Undercoverage b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Op | Post-Op | Pre-Op | Post-Op | |||||||||||||||
| Demange (2015) [27] | OTS | 21.1% a | ||||||||||||||||
| PSI | 3.3° (4.9°) (−5.4°–+8.5°) | −0.9° (3.8°) (−8.0°–3.4°) | 75.8% a | |||||||||||||||
| Arbab (2018) [16] | OTS, CR | 8.2° (−18.2°–+15.7°) median 5.6° | 2.3° (−10.1°–+12.5°) median 1.7° | 26% | ||||||||||||||
| PSI, CR | 9.0° (−27.3°–+18.9) median 5.7° | 3.2° (−7.6°–+8.4°) median 0.7° | 16% | |||||||||||||||
| Ivie (2014) [19] | OTS | 88.32° (1.51°) | * | 87.81 (1.54) | ns | 87.12° (1.73°) | ns | 1.68° (3.65°) | ** | 43.1% | ||||||||
| PSI | 87.37° (3.87°) | 87.71° (1.44°) | 86.42° (2.61°) | −0.47° (3.15°) | 29.6% | |||||||||||||
| Meheux (2019) [20] | OTS | 88.54° (1.5°) | 4.00° (2.5°) | −3.32° (5.2°) | ns | −3.32° (5.2°) | ns | 2.29° (3.8°) | ||||||||||
| PSI 1 | 91.08° (1.9°) | 6.40° (2.9°) | −3.97° (3.5°) | −1.34° (4.6°) | 4.09° (2.7°) | |||||||||||||
| PSI 2 | 89.89° (1.0°) | 5.53° (3.9°) | −3.89° (3.46°) | −0.35° (1.8°) | 4.1° (3°) | |||||||||||||
| Schroeder (2019) [23] | OTS 1 | 23% a + b | *** | |||||||||||||||
| OTS 2 | 25% a + b | |||||||||||||||||
| OTS 3 | 34% a + b | |||||||||||||||||
| PSI | 80% a + b | |||||||||||||||||
| White and Ranawat (2016) [26] | OTS, CR | 5° (1°) | −4° (3°) | ns | 2° | ns | ||||||||||||
| OTS, PS | 4° (1°) | −1° (7°) | 2° | |||||||||||||||
| PSI, CR | 5° (1°) | −3° (4°) | 2° | |||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moret, C.S.; Schelker, B.L.; Hirschmann, M.T. Clinical and Radiological Outcomes after Knee Arthroplasty with Patient-Specific versus Off-the-Shelf Knee Implants: A Systematic Review. J. Pers. Med. 2021, 11, 590. https://doi.org/10.3390/jpm11070590
Moret CS, Schelker BL, Hirschmann MT. Clinical and Radiological Outcomes after Knee Arthroplasty with Patient-Specific versus Off-the-Shelf Knee Implants: A Systematic Review. Journal of Personalized Medicine. 2021; 11(7):590. https://doi.org/10.3390/jpm11070590
Chicago/Turabian StyleMoret, Céline Saphena, Benjamin Luca Schelker, and Michael Tobias Hirschmann. 2021. "Clinical and Radiological Outcomes after Knee Arthroplasty with Patient-Specific versus Off-the-Shelf Knee Implants: A Systematic Review" Journal of Personalized Medicine 11, no. 7: 590. https://doi.org/10.3390/jpm11070590
APA StyleMoret, C. S., Schelker, B. L., & Hirschmann, M. T. (2021). Clinical and Radiological Outcomes after Knee Arthroplasty with Patient-Specific versus Off-the-Shelf Knee Implants: A Systematic Review. Journal of Personalized Medicine, 11(7), 590. https://doi.org/10.3390/jpm11070590