
Comparison of 0.12% Chlorhexidine and a New Bone Bioactive Liquid, BBL, in Mouthwash for Oral Wound Healing: A Randomized, Double Blind Clinical Human Trial
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population: Inclusion and Exclusion Criteria
2.2. Removal of Patients from Therapy or Assessment
2.3. Study Design
2.4. Surgery Assessments
2.5. Post-Surgical Procedures
2.6. Wound Healing Measurement Procedures
2.7. Procedures for Measurement of Post-Surgical Pain, Safety, and Discomfort
2.8. Statistical and Analytical Methods
3. Results
3.1. BBL Mouthwash Dramatically Reduces VAS
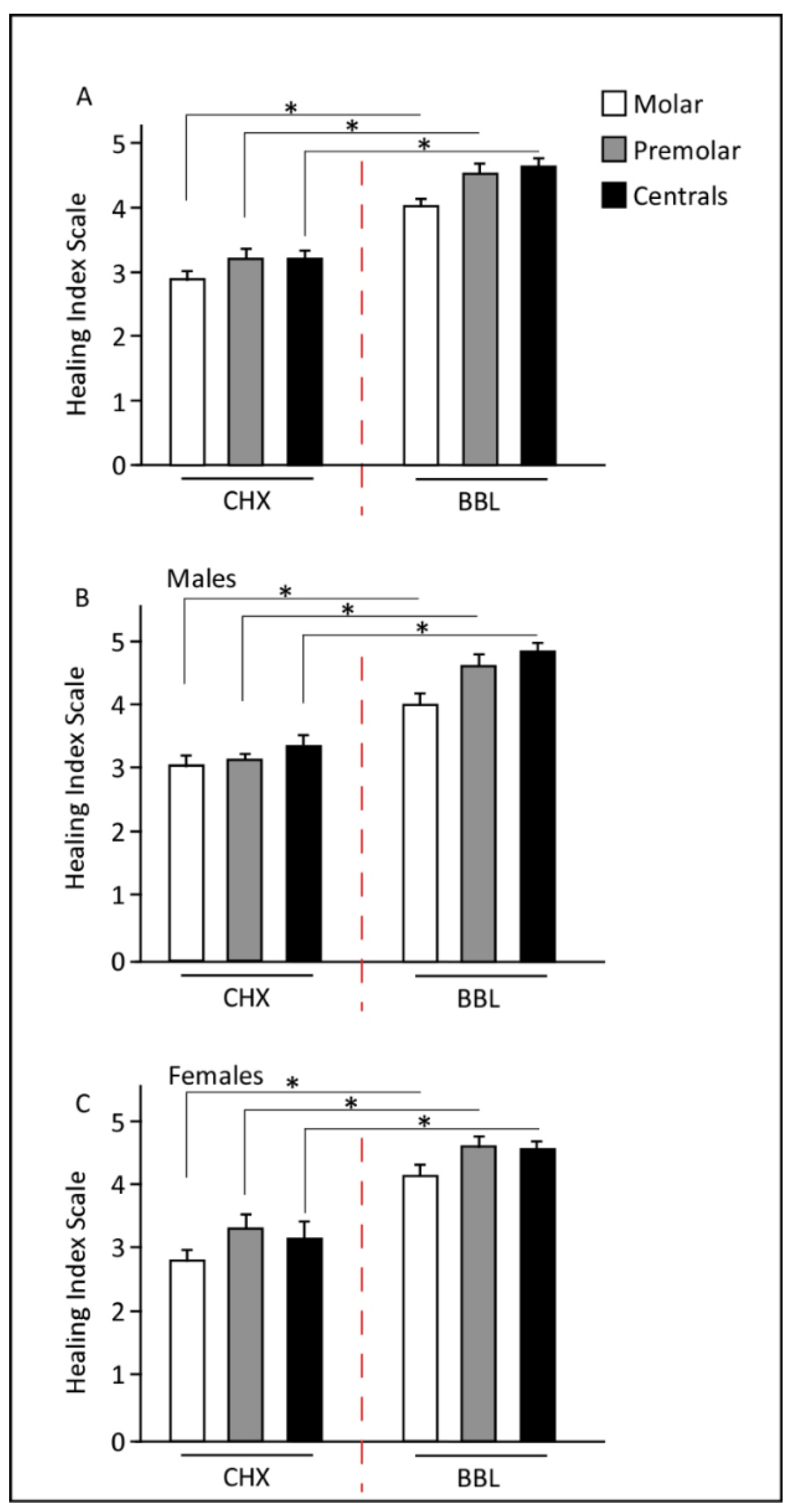
3.2. BBL Mouthwash Improves EHI
4. Discussion
5. Conclusions
6. Study Limitation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bielefeld, K.A.; Amini-Nik, S.; Alman, B.A. Cutaneous wound healing: Recruiting developmental pathways for regeneration. Cell. Mol. Life Sci. 2013, 70, 2059–2081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, V.W.; Gurtner, G.C.; Longaker, M.T. Wound healing: A paradigm for regeneration. Mayo. Clin. Proc. 2013, 88, 1022–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toma, A.I.; Fuller, J.M.; Willett, N.J.; Goudy, S.L. Oral wound healing models and emerging regenerative therapies. Transl. Res. 2021, 236, 17–34. [Google Scholar] [CrossRef] [PubMed]
- Discepoli, N.; Vignoletti, F.; Laino, L.; de Sanctis, M.; Munoz, F.; Sanz, M. Early healing of the alveolar process after tooth extraction: An experimental study in the beagle dog. J. Clin. Periodontol. 2013, 40, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Farina, R.; Marzola, A.; Bozzi, L.; Liljenberg, B.; Lindhe, J. Modeling and remodeling of human extraction sockets. J. Clin. Periodontol. 2008, 35, 630–639. [Google Scholar] [CrossRef]
- Pagni, G.; Pellegrini, G.; Giannobile, W.V.; Rasperini, G. Postextraction alveolar ridge preservation: Biological basis and treatments. Int. J. Dent. 2012, 2012, 151030. [Google Scholar] [CrossRef] [Green Version]
- Whetman, J.; Mealey, B.L. Effect of Healing Time on New Bone Formation After Tooth Extraction and Ridge Preservation with Demineralized Freeze-Dried Bone Allograft: A Randomized Controlled Clinical Trial. J. Periodontol. 2016, 87, 1022–1029. [Google Scholar] [CrossRef]
- Politis, C.; Schoenaers, J.; Jacobs, R.; Agbaje, J.O. Wound Healing Problems in the Mouth. Front. Physiol. 2016, 7, 507. [Google Scholar] [CrossRef] [Green Version]
- Glim, J.E.; van Egmond, M.; Niessen, F.B.; Everts, V.; Beelen, R.H. Detrimental dermal wound healing: What can we learn from the oral mucosa? Wound Repair Regen. 2013, 21, 648–660. [Google Scholar] [CrossRef]
- Ford, S.J. The importance and provision of oral hygiene in surgical patients. Int. J. Surg. 2008, 6, 418–419. [Google Scholar] [CrossRef]
- Goldenhart, A.L.; Nagy, H. Assisting Patients with Personal Hygiene; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Varoni, E.; Tarce, M.; Lodi, G.; Carrassi, A. Chlorhexidine (CHX) in dentistry: State of the art. Minerva Stomatol. 2012, 61, 399–419. [Google Scholar]
- Colombo, A.P.; Haffajee, A.D.; Dewhirst, F.E.; Paster, B.J.; Smith, C.M.; Cugini, M.A.; Socransky, S.S. Clinical and microbiological features of refractory periodontitis subjects. J. Clin. Periodontol. 1998, 25, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, S.; Addy, M.; Wade, W. The mechanism of action of chlorhexidine. A study of plaque growth on enamel inserts in vivo. J. Clin. Periodontol. 1988, 15, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Eick, S.; Seltmann, T.; Pfister, W. Efficacy of antibiotics to strains of periodontopathogenic bacteria within a single species biofilm—An in vitro study. J. Clin. Periodontol. 2004, 31, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Rajendiran, M.; Trivedi, H.M.; Chen, D.; Gajendrareddy, P.; Chen, L. Recent Development of Active Ingredients in Mouthwashes and Toothpastes for Periodontal Diseases. Molecules 2021, 26, 2001. [Google Scholar] [CrossRef]
- Ferrés-Amat, E.; Al Madhoun, A.; Ferrés-Amat, E.; Al Demour, S.; Ababneh, M.A.; Ferrés-Padró, E.; Marti, C.; Carrio, N.; Barajas, M.; Atari, M. Histologic and Histomorphometric Evaluation of a New Bioactive Liquid BBL on Implant Surface: A Preclinical Study in Foxhound Dogs. Materials 2021, 14, 6217. [Google Scholar] [CrossRef]
- Krishnankutty, B.; Bellary, S.; Kumar, N.B.; Moodahadu, L.S. Data management in clinical research: An overview. Indian J. Pharmacol. 2012, 44, 168–172. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- Fickl, S.; Fischer, K.R.; Jockel-Schneider, Y.; Stappert, C.F.; Schlagenhauf, U.; Kebschull, M. Early wound healing and patient morbidity after single-incision vs. trap-door graft harvesting from the palate—A clinical study. Clin. Oral Investig. 2014, 18, 2213–2219. [Google Scholar] [CrossRef]
- Landry, R.G. Effectiveness of Benzydamine HC1 in the Treatment of Periodontal Post-Surgical Patients. Doctoral Dissertation, Faculty of Dentistry, University of Toronto, Toronto, ON, Canada, 1985. [Google Scholar]
- Haefeli, M.; Elfering, A. Pain assessment. Eur. Spine J. 2006, 15 (Suppl. 1), S17–S24. [Google Scholar] [CrossRef] [PubMed]
- Chye, R.M.L.; Perrotti, V.; Piattelli, A.; Iaculli, F.; Quaranta, A. Effectiveness of Different Commercial Chlorhexidine-Based Mouthwashes After Periodontal and Implant Surgery: A Systematic Review. Implant Dent. 2019, 28, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Brookes, Z.L.S.; Bescos, R.; Belfield, L.A.; Ali, K.; Roberts, A. Current uses of chlorhexidine for management of oral disease: A narrative review. J. Dent. 2020, 103, 103497. [Google Scholar] [CrossRef] [PubMed]
- Flotra, L.; Gjermo, P.; Rolla, G.; Waerhaug, J. Side effects of chlorhexidine mouth washes. Scand. J. Dent. Res. 1971, 79, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Pemberton, M.N.; Gibson, J. Chlorhexidine and hypersensitivity reactions in dentistry. Br. Dent. J. 2012, 213, 547–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, P.; Parnell, C.; Whelton, H. The caries-preventive effect of chlorhexidine varnish in children and adolescents: A systematic review. Caries Res. 2010, 44, 333–340. [Google Scholar] [CrossRef]
- Berchier, C.E.; Slot, D.E.; Van der Weijden, G.A. The efficacy of 0.12% chlorhexidine mouthrinse compared with 0.2% on plaque accumulation and periodontal parameters: A systematic review. J. Clin. Periodontol. 2010, 37, 829–839. [Google Scholar] [CrossRef]
- Poppolo Deus, F.; Ouanounou, A. Chlorhexidine in Dentistry: Pharmacology, Uses, and Adverse Effects. Int. Dent. J. 2022, 72, 269–277. [Google Scholar] [CrossRef]
- Samanth, S.A.; Varghese, S.S. The Most Effective Concentration of Chlorhexidine as a Mouthwash-Systematic Review. J. Pharm. Sci. Res. 2017, 9, 233–236. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Criteria | Visit 1 | Phone Calls | Visit 2 | |
|---|---|---|---|---|
| (Surgery Day) | Day 2 | Day 4 | Day 7 | |
| Informed consent | X | |||
| Inclusion/exclusion criteria | X | |||
| Collection of clinical data | X | X | ||
| Oral examination | X | X | ||
| Patient diary: Pain VAS scale 0–10 | X | X | X | |
| Patient diary: clinical healing measurements | X | X | ||
| Tolerability and post-treatment side effects | X | |||
| EHI Score | Total of 171 Dental Extractions in Operations on 81 Patients | |
|---|---|---|
| BBL Treatment | 0.12% Chlorhexidine Treatment | |
| 1—very poor | 0 | 0 |
| 2—poor | 0 | 4 |
| 3—good | 5 | 64 |
| 4—very good | 49 | 9 |
| 5—excellent | 38 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrés-Amat, E.; Al Madhoun, A.; Ferrés-Amat, E.; Carrió, N.; Barajas, M.; Al-Madhoun, A.S.; Ferrés-Padró, E.; Marti, C.; Atari, M. Comparison of 0.12% Chlorhexidine and a New Bone Bioactive Liquid, BBL, in Mouthwash for Oral Wound Healing: A Randomized, Double Blind Clinical Human Trial. J. Pers. Med. 2022, 12, 1725. https://doi.org/10.3390/jpm12101725
Ferrés-Amat E, Al Madhoun A, Ferrés-Amat E, Carrió N, Barajas M, Al-Madhoun AS, Ferrés-Padró E, Marti C, Atari M. Comparison of 0.12% Chlorhexidine and a New Bone Bioactive Liquid, BBL, in Mouthwash for Oral Wound Healing: A Randomized, Double Blind Clinical Human Trial. Journal of Personalized Medicine. 2022; 12(10):1725. https://doi.org/10.3390/jpm12101725
Chicago/Turabian StyleFerrés-Amat, Eduard, Ashraf Al Madhoun, Elvira Ferrés-Amat, Neus Carrió, Miguel Barajas, Areej Said Al-Madhoun, Eduard Ferrés-Padró, Carles Marti, and Maher Atari. 2022. "Comparison of 0.12% Chlorhexidine and a New Bone Bioactive Liquid, BBL, in Mouthwash for Oral Wound Healing: A Randomized, Double Blind Clinical Human Trial" Journal of Personalized Medicine 12, no. 10: 1725. https://doi.org/10.3390/jpm12101725
APA StyleFerrés-Amat, E., Al Madhoun, A., Ferrés-Amat, E., Carrió, N., Barajas, M., Al-Madhoun, A. S., Ferrés-Padró, E., Marti, C., & Atari, M. (2022). Comparison of 0.12% Chlorhexidine and a New Bone Bioactive Liquid, BBL, in Mouthwash for Oral Wound Healing: A Randomized, Double Blind Clinical Human Trial. Journal of Personalized Medicine, 12(10), 1725. https://doi.org/10.3390/jpm12101725