
Development and Evaluation of a Machine Learning Prediction Model for Small-for-Gestational-Age Births in Women Exposed to Radiation before Pregnancy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Participants and Features
2.3. Study Design
2.4. ML Algorithms
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
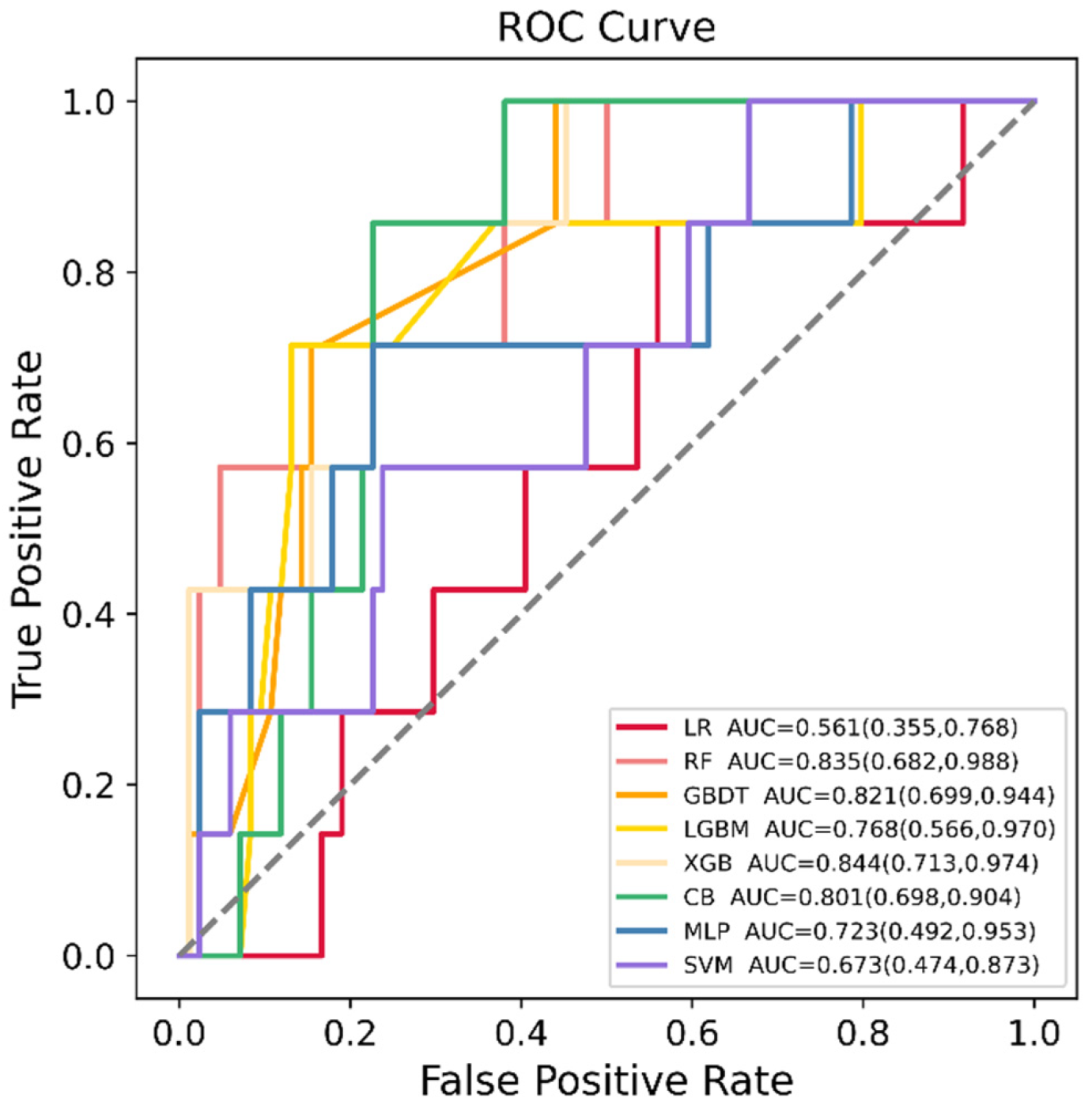
3.2. ML Algorithms’ Performance Comparison
3.3. Feature Selection and Final Prediction Model
3.4. Assessment of Variable Importance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCowan, L.M.; Figueras, F.; Anderson, N.H. Evidence-based national guidelines for the management of suspected fetal growth restriction: Comparison, consensus, and controversy. Am. J. Obstet. Gynecol. 2018, 218, S855–S868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindqvist, P.G.; Molin, J. Does antenatal identification of small-for-gestational age fetuses significantly improve their outcome? Ultrasound. Obstet. Gynecol. 2005, 25, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Frøen, J.F.; Gardosi, J.O.; Thurmann, A.; Francis, A.; Stray-Pedersen, B. Restricted fetal growth in sudden intrauterine unexplained death. Acta Obstet. Et. Gynecol. Scand. 2004, 83, 801–807. [Google Scholar] [CrossRef]
- Gardosi, J.; Madurasinghe, V.; Williams, M.; Malik, A.; Francis, A. Maternal and fetal risk factors for stillbirth: Population based study. BMJ 2013, 346, f108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugandzic, R.; Dodds, L.; Stieb, D.; Smith-Doiron, M. The association between low level exposures to ambient air pollution and term low birth weight: A retrospective cohort study. Environ. Health 2006, 5, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grazuleviciene, R.; Nieuwenhuijsen, M.J.; Vencloviene, J.; Kostopoulou-Karadanelli, M.; Krasner, S.W.; Danileviciute, A.; Balcius, G.; Kapustinskiene, V. Individual exposures to drinking water trihalomethanes, low birth weight and small for gestational age risk: A prospective Kaunas cohort study. Environ. Health 2011, 10, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morello-Frosch, R.; Jesdale, B.M.; Sadd, J.L.; Pastor, M. Ambient air pollution exposure and full-term birth weight in California. Environ. Health 2010, 9, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshimoto, Y.; Schull, W.J.; Kato, H.; Neel, J.V. Mortality among the offspring (F1) of atomic bomb survivors, 1946–1985. J. Radiat. Res. 1991, 32, 327–351. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.R.; Loke, W.K.; Khoo, B.C. Low-dose or low-dose-rate ionizing radiation-induced bioeffects in animal models. J. Radiat. Res. 2017, 58, 165–182. [Google Scholar] [CrossRef]
- Otake, M.; Fujikoshi, Y.; Funamoto, S.; Schull, W.J. Evidence of radiation-induced reduction of height and body weight from repeated measurements of adults exposed in childhood to the atomic bombs. Radiat. Res. 1994, 140, 112–122. [Google Scholar] [CrossRef]
- Hamilton, P.M.; Roney, P.L.; Keppel, K.G.; Placek, P.J. Radiation procedures performed on U.S. women during pregnancy: Findings from two 1980 surveys. Public Health Rep. 1984, 99, 146–151. [Google Scholar] [PubMed]
- Goldberg, M.S.; Mayo, N.E.; Levy, A.R.; Scott, S.C.; Poîtras, B. Adverse reproductive outcomes among women exposed to low levels of ionizing radiation from diagnostic radiography for adolescent idiopathic scoliosis. Epidemiology 1998, 9, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Hudson, M.M. Reproductive outcomes for survivors of childhood cancer. Obstet. Gynecol. 2010, 116, 1171–1183. [Google Scholar] [CrossRef] [PubMed]
- Hujoel, P.P.; Bollen, A.M.; Noonan, C.J.; del Aguila, M.A. Antepartum dental radiography and infant low birth weight. JAMA 2004, 291, 1987–1993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shouval, R.; Bondi, O.; Mishan, H.; Shimoni, A.; Unger, R.; Nagler, A. Application of machine learning algorithms for clinical predictive modeling: A data-mining approach in SCT. Bone Marrow Transplant. 2014, 49, 332–337. [Google Scholar] [CrossRef]
- Wu, Q.; Nasoz, F.; Jung, J.; Bhattarai, B.; Han, M.V. Machine Learning Approaches for Fracture Risk Assessment: A Comparative Analysis of Genomic and Phenotypic Data in 5130 Older Men. Calcif. Tissue Int. 2020, 107, 353–361. [Google Scholar] [CrossRef]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [Green Version]
- Kuhle, S.; Maguire, B.; Zhang, H.; Hamilton, D.; Allen, A.C.; Joseph, K.S.; Allen, V.M. Comparison of logistic regression with machine learning methods for the prediction of fetal growth abnormalities: A retrospective cohort study. BMC Pregnancy Childbirth 2018, 18, 333. [Google Scholar] [CrossRef]
- Papastefanou, I.; Wright, D.; Nicolaides, K.H. Competing-risks model for prediction of small-for-gestational-age neonate from maternal characteristics and medical history. Ultrasound Obstet. Gynecol. 2020, 56, 196–205. [Google Scholar] [CrossRef]
- Saw, S.N.; Biswas, A.; Mattar, C.N.Z.; Lee, H.K.; Yap, C.H. Machine learning improves early prediction of small-for-gestational-age births and reveals nuchal fold thickness as unexpected predictor. Prenat. Diagn. 2021, 41, 505–516. [Google Scholar] [CrossRef]
- Shah, P.S. Paternal factors and low birthweight, preterm, and small for gestational age births: A systematic review. Am. J. Obstet. Gynecol. 2010, 202, 103–123. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, G.D.; Bushnik, T.; Sheppard, A.J.; Kramer, M.S.; Kaufman, J.S.; Yang, S. Paternal education and adverse birth outcomes in Canada. J. Epidemiol. Community Health 2017, 71, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Kloog, I.; Melly, S.J.; Ridgway, W.L.; Coull, B.A.; Schwartz, J. Using new satellite based exposure methods to study the association between pregnancy PM₂.₅ exposure, premature birth and birth weight in Massachusetts. Environ. Health 2012, 11, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, Y.; Zhang, S.; Wang, Q.; Shen, H.; Zhang, Y.; Li, Y.; Yan, D.; Sun, L. Investigating the association between prepregnancy body mass index and adverse pregnancy outcomes: A large cohort study of 536 098 Chinese pregnant women in rural China. BMJ Open 2016, 6, e011227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.Y.; Li, Q.; Guo, Y.; Zhou, H.; Wang, X.; Wang, Q.; Shen, H.; Zhang, Y.; Yan, D.; Zhang, Y.; et al. Association of Long-term Exposure to Airborne Particulate Matter of 1 μm or Less With Preterm Birth in China. JAMA Pediatr. 2018, 172, e174872. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Wang, Q.; Shen, H. Design of the National Free Preconception Health Examination Project in China. Natl. Med. J. China 2015, 95, 162–165. [Google Scholar]
- Xiao, Q.; Chang, H.H.; Geng, G.; Liu, Y. An Ensemble Machine-Learning Model To Predict Historical PM(2.5) Concentrations in China from Satellite Data. Environ. Sci. Technol. 2018, 52, 13260–13269. [Google Scholar] [CrossRef]
- Zhu, L.; Zhang, R.; Zhang, S.; Shi, W.; Yan, W.; Wang, X.; Lyu, Q.; Liu, L.; Zhou, Q.; Qiu, Q.; et al. Chinese neonatal birth weight curve for different gestational age. Zhonghua Er Ke Za Zhi 2015, 53, 97–103. [Google Scholar]
- Gong, J.; Bao, X.; Wang, T.; Liu, J.; Peng, W.; Shi, J.; Wu, F.; Gu, Y. A short-term follow-up CT based radiomics approach to predict response to immunotherapy in advanced non-small-cell lung cancer. Oncoimmunology 2022, 11, 2028962. [Google Scholar] [CrossRef]
- Lim, L.J.; Lim, A.J.W.; Ooi, B.N.S.; Tan, J.W.L.; Koh, E.T.; Chong, S.S.; Khor, C.C.; Tucker-Kellogg, L.; Lee, C.G.; Leong, K.P. Machine Learning using Genetic and Clinical Data Identifies a Signature that Robustly Predicts Methotrexate Response in Rheumatoid Arthritis. Rheumatology 2022. [Google Scholar] [CrossRef]
- Lu, C.; Song, J.; Li, H.; Yu, W.; Hao, Y.; Xu, K.; Xu, P. Predicting Venous Thrombosis in Osteoarthritis Using a Machine Learning Algorithm: A Population-Based Cohort Study. J. Pers. Med. 2022, 12, 114. [Google Scholar] [CrossRef] [PubMed]
- Bloch, L.; Friedrich, C.M. Data analysis with Shapley values for automatic subject selection in Alzheimer’s disease data sets using interpretable machine learning. Alzheimer’s. Res. Ther. 2021, 13, 155. [Google Scholar] [CrossRef] [PubMed]
- Le Cessie, S.; Van Houwelingen, J.C. Ridge estimators in logistic regression. Appl. Stat. 1992, 41, 191–201. [Google Scholar] [CrossRef]
- Kulkarni, V.Y.; Sinha, P.K.; Petare, M.C. Weighted hybrid decision tree model for random forest classifier. J. Inst. Eng. Ser. B. 2016, 97, 209–217. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Jung, C. GBDT-MO: Gradient-Boosted Decision Trees for Multiple Outputs. IEEE. Trans. Neural Netw. Learn. Syst. 2021, 32, 3156–3167. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Yoshida, K. Quantitative structure-property relationships for the calculation of the soil adsorption coefficient using machine learning algorithms with calculated chemical properties from open-source software. Environ. Res. 2021, 196, 110363. [Google Scholar] [CrossRef]
- Hancock, J.T.; Khoshgoftaar, T.M. CatBoost for big data: An interdisciplinary review. J. Big Data 2020, 7, 94. [Google Scholar] [CrossRef]
- Li, Y.; Li, M.; Li, C.; Liu, Z. Forest aboveground biomass estimation using Landsat 8 and Sentinel-1A data with machine learning algorithms. Sci. Rep. 2020, 10, 9952. [Google Scholar] [CrossRef]
- Huang, S.; Cai, N.; Pacheco, P.P.; Narrandes, S.; Wang, Y.; Xu, W. Applications of Support Vector Machine (SVM) Learning in Cancer Genomics. Cancer Genom. Proteom. 2018, 15, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Long, Z.; Jing, B.; Yan, H.; Dong, J.; Liu, H.; Mo, X.; Han, Y.; Li, H. A support vector machine-based method to identify mild cognitive impairment with multi-level characteristics of magnetic resonance imaging. Neuroscience 2016, 331, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Prout, T.A.; Zilcha-Mano, S.; Aafjes-van Doorn, K.; Békés, V.; Christman-Cohen, I.; Whistler, K.; Kui, T.; Di Giuseppe, M. Identifying Predictors of Psychological Distress During COVID-19: A Machine Learning Approach. Front. Psychol. 2020, 11, 586202. [Google Scholar] [CrossRef] [PubMed]
- Reulen, R.C.; Zeegers, M.P.; Wallace, W.H.; Frobisher, C.; Taylor, A.J.; Lancashire, E.R.; Winter, D.L.; Hawkins, M.M. Pregnancy outcomes among adult survivors of childhood cancer in the British Childhood Cancer Survivor Study. Cancer Epidemiol. Prev. Biomark. 2009, 18, 2239–2247. [Google Scholar] [CrossRef] [Green Version]
- Green, D.M.; Whitton, J.A.; Stovall, M.; Mertens, A.C.; Donaldson, S.S.; Ruymann, F.B.; Pendergrass, T.W.; Robison, L.L. Pregnancy outcome of female survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Am. J. Obstet. Gynecol. 2002, 187, 1070–1080. [Google Scholar] [CrossRef] [PubMed]
- Signorello, L.B.; Cohen, S.S.; Bosetti, C.; Stovall, M.; Kasper, C.E.; Weathers, R.E.; Whitton, J.A.; Green, D.M.; Donaldson, S.S.; Mertens, A.C.; et al. Female survivors of childhood cancer: Preterm birth and low birth weight among their children. J. Natl. Cancer Inst. 2006, 98, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Scherb, H.; Hayashi, K. Spatiotemporal association of low birth weight with Cs-137 deposition at the prefecture level in Japan after the Fukushima nuclear power plant accidents: An analytical-ecologic epidemiological study. Environ. Health 2020, 19, 82. [Google Scholar] [CrossRef]
- Dasgupta, S.; Goldberg, Y.; Kosorok, M.R. Feature elimination in kernel machines in moderately high dimensions. Ann. Stat. 2019, 47, 497–526. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.J.W.; Lim, L.J.; Ooi, B.N.S.; Koh, E.T.; Tan, J.W.L.; Chong, S.S.; Khor, C.C.; Tucker-Kellogg, L.; Leong, K.P.; Lee, C.G. Functional coding haplotypes and machine-learning feature elimination identifies predictors of Methotrexate Response in Rheumatoid Arthritis patients. EBioMedicine 2022, 75, 103800. [Google Scholar] [CrossRef]
- Ntakolia, C.; Kokkotis, C.; Moustakidis, S.; Tsaopoulos, D. Identification of most important features based on a fuzzy ensemble technique: Evaluation on joint space narrowing progression in knee osteoarthritis patients. Int. J. Med. Inform. 2021, 156, 104614. [Google Scholar] [CrossRef] [PubMed]
- Ntakolia, C.; Kokkotis, C.; Moustakidis, S.; Tsaopoulos, D. Prediction of Joint Space Narrowing Progression in Knee Osteoarthritis Patients. Diagnostics 2021, 11, 285. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Suarez, D.F.; Kim, Y.; Villablanca, P.; Gupta, T.; Wiley, J.; Nieves-Rodriguez, B.G.; Rodriguez-Maldonado, J.; Feliu Maldonado, R.; da Luz Sant’Ana, I.; Sanina, C.; et al. Machine Learning Prediction Models for In-Hospital Mortality After Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2019, 12, 1328–1338. [Google Scholar] [CrossRef] [PubMed]
- Miletić, T.; Stoini, E.; Mikulandra, F.; Tadin, I.; Roje, D.; Milić, N. Effect of parental anthropometric parameters on neonatal birth weight and birth length. Coll. Antropol. 2007, 31, 993–997. [Google Scholar] [PubMed]
- Myklestad, K.; Vatten, L.J.; Magnussen, E.B.; Salvesen, K.; Romundstad, P.R. Do parental heights influence pregnancy length?: A population-based prospective study, HUNT 2. BMC Pregnancy Childbirth 2013, 13, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, Y.; Groth, S.W. Fathers Count: The Impact of Paternal Risk Factors on Birth Outcomes. Matern. Child. Health J. 2018, 22, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Harville, E.W.; Chen, W.; Bazzano, L.; Oikonen, M.; Hutri-Kähönen, N.; Raitakari, O. Indicators of fetal growth and adult liver enzymes: The Bogalusa Heart Study and the Cardiovascular Risk in Young Finns Study. J. Dev. Orig. Health Dis. 2017, 8, 226–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larroca, S.G.; Arevalo-Serrano, J.; Abad, V.O.; Recarte, P.P.; Carreras, A.G.; Pastor, G.N.; Hernandez, C.R.; Pacheco, R.P.; Luis, J.L. Platelet Count in First Trimester of Pregnancy as a Predictor of Perinatal Outcome. Maced. J. Med. Sci. 2017, 5, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Heumann, C.L.; Quilter, L.A.; Eastment, M.C.; Heffron, R.; Hawes, S.E. Adverse Birth Outcomes and Maternal Neisseria gonorrhoeae Infection: A Population-Based Cohort Study in Washington State. Sex. Transm. Dis. 2017, 44, 266–271. [Google Scholar] [CrossRef] [Green Version]
- Johnson, H.L.; Ghanem, K.G.; Zenilman, J.M.; Erbelding, E.J. Sexually transmitted infections and adverse pregnancy outcomes among women attending inner city public sexually transmitted diseases clinics. Sex. Transm. Dis. 2011, 38, 167–171. [Google Scholar] [CrossRef]
- Leng, J.; Hay, J.; Liu, G.; Zhang, J.; Wang, J.; Liu, H.; Yang, X.; Liu, J. Small-for-gestational age and its association with maternal blood glucose, body mass index and stature: A perinatal cohort study among Chinese women. BMJ Open 2016, 6, e010984. [Google Scholar] [CrossRef]
- Siega-Riz, A.M.; Viswanathan, M.; Moos, M.K.; Deierlein, A.; Mumford, S.; Knaack, J.; Thieda, P.; Lux, L.J.; Lohr, K.N. A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention. Am. J. Obstet. Gynecol. 2009, 201, 339.e1–339.e14. [Google Scholar] [CrossRef]
- Lederman, S.A. Pregnancy weight gain and postpartum loss: Avoiding obesity while optimizing the growth and development of the fetus. J. Am. Med. Women’s Assoc. 2001, 56, 53–58. [Google Scholar]
- Nadi, S.; Elahi, M.; Moradi, S.; Banaei, A.; Ataei, G.; Abedi-Firouzjah, R. Radioprotective Effect of Arbutin in Megavoltage Therapeutic X-irradiated Mice using Liver Enzymes Assessment. J. Biomed. Phys. Eng. 2019, 9, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.K.; Seed, T.M. A review of radiation countermeasures focusing on injury-specific medicinals and regulatory approval status: Part I. Radiation sub-syndromes, animal models and FDA-approved countermeasures. Int. J. Radiat. Biol. 2017, 93, 851–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Z.B.; Zou, J.F.; Bai, J.; Yu, G.C.; Zhang, X.X.; Ma, H.H.; Cheng, Q.M.; Wang, S.P.; Ji, F.L.; Yu, W.L. The occupational and procreation health of immigrant female workers in electron factory. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2011, 29, 661–664. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Alsubaie, Y.; Almubarak, Z.; Almutawa, H.; AlQasem, Y.; Hasanato, R.M. Association of Exposure to Radio-Frequency Electromagnetic Field Radiation (RF-EMFR) Generated by Mobile Phone Base Stations with Glycated Hemoglobin (HbA1c) and Risk of Type 2 Diabetes Mellitus. Int. J. Environ. Res. Public Health 2015, 12, 14519–14528. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Overall (n = 455) | Not SGA (n = 395) | SGA (n = 60) | p Value |
|---|---|---|---|---|
| Gestational at birth, week | 40.0 (39.0–40.0) | 40.0 (39.0–40.0) | 40.0 (39.0–40.0) | 0.013 |
| Birth weight, kg | 3.3 (3.0–3.6) | 3.4 (3.1–3.6) | 2.6 (2.2–2.8) | <0.001 |
| Maternal age, year | 24.0 (23.0–27.0) | 24.0 (23.0–27.0) | 24.5 (22.0–26.0) | 0.184 |
| Maternal height, cm | 160.0 (156.0–163.0) | 160.0 (157.0–163.0) | 158.0 (155.0–160.0) | 0.014 |
| Maternal BMI, kg/m2 | 20.2 (18.8–22.0) | 20.2 (18.8–22.0) | 20.0 (18.6–22.2) | 0.332 |
| Maternal education level | ||||
| Below junior high school | 168 (36.9%) | 149 (37.7%) | 19 (31.7%) | 0.635 |
| Senior high school | 146 (32.1%) | 126 (31.9%) | 20 (33.3%) | |
| Bachelor’s degrees and above | 141 (31.0%) | 120 (30.4%) | 21 (35.0%) | |
| Mother adnexitis before pregnancy | 23 (5.1%) | 14 (3.5%) | 9 (15.0%) | 0.001 |
| Number of previous pregnancies | 0.0 (0.0–1.0) | 0.0 (0.0–1.0) | 1.0 (0.0–1.0) | 0.003 |
| Paternal age, year | 26.0 (24.0–29.0) | 26.0 (24.0–28.0) | 26.0 (24.0–29.0) | 0.328 |
| Paternal height, cm | 171.4 ± 5.3 | 171.6 ± 5.2 | 170.2 ± 5.6 | 0.055 |
| Paternal education level | ||||
| Below junior high school | 174 (38.2%) | 153 (38.7%) | 21 (35.0%) | 0.810 |
| Senior high school | 151 (33.2%) | 131 (33.2%) | 20 (33.3%) | |
| Bachelor’s degrees and above | 130 (28.6%) | 111 (28.1%) | 19 (31.7%) | |
| Father anemia before pregnancy | 10 (2.2%) | 5 (1.3%) | 5 (8.3%) | 0.003 |
| Model | AUC Training | AUC Testing | Sensitivity | Specificity | PPV | NPV | MCC | Kappa |
|---|---|---|---|---|---|---|---|---|
| LR | 0.620 | 0.561 | 0.857 | 0.440 | 0.113 | 0.974 | 0.161 | 0.074 |
| RF | 0.897 | 0.835 | 0.714 | 0.845 | 0.278 | 0.973 | 0.374 | 0.325 |
| GBDT | 0.850 | 0.821 | 0.714 | 0.845 | 0.278 | 0.973 | 0.374 | 0.325 |
| XGBoost | 0.958 | 0.844 | 0.857 | 0.774 | 0.240 | 0.985 | 0.377 | 0.290 |
| LGBM | 0.844 | 0.768 | 0.714 | 0.869 | 0.312 | 0.973 | 0.408 | 0.367 |
| CatBoost | 0.853 | 0.801 | 0.857 | 0.774 | 0.240 | 0.985 | 0.377 | 0.290 |
| SVM | 0.836 | 0.673 | 1.000 | 0.333 | 0.111 | 1.000 | 0.192 | 0.071 |
| MLP | 0.902 | 0.723 | 0.714 | 0.774 | 0.208 | 0.970 | 0.295 | 0.231 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, X.; Zhou, Z.; Luo, Y.; Yang, H.; Zhu, H.; Chen, S.; Pan, H. Development and Evaluation of a Machine Learning Prediction Model for Small-for-Gestational-Age Births in Women Exposed to Radiation before Pregnancy. J. Pers. Med. 2022, 12, 550. https://doi.org/10.3390/jpm12040550
Bai X, Zhou Z, Luo Y, Yang H, Zhu H, Chen S, Pan H. Development and Evaluation of a Machine Learning Prediction Model for Small-for-Gestational-Age Births in Women Exposed to Radiation before Pregnancy. Journal of Personalized Medicine. 2022; 12(4):550. https://doi.org/10.3390/jpm12040550
Chicago/Turabian StyleBai, Xi, Zhibo Zhou, Yunyun Luo, Hongbo Yang, Huijuan Zhu, Shi Chen, and Hui Pan. 2022. "Development and Evaluation of a Machine Learning Prediction Model for Small-for-Gestational-Age Births in Women Exposed to Radiation before Pregnancy" Journal of Personalized Medicine 12, no. 4: 550. https://doi.org/10.3390/jpm12040550
APA StyleBai, X., Zhou, Z., Luo, Y., Yang, H., Zhu, H., Chen, S., & Pan, H. (2022). Development and Evaluation of a Machine Learning Prediction Model for Small-for-Gestational-Age Births in Women Exposed to Radiation before Pregnancy. Journal of Personalized Medicine, 12(4), 550. https://doi.org/10.3390/jpm12040550