
Predictive Assessment of Quantitative Ultra-Widefield Angiographic Features for Future Need for Anti-VEGF Therapy in Diabetic Eye Disease

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
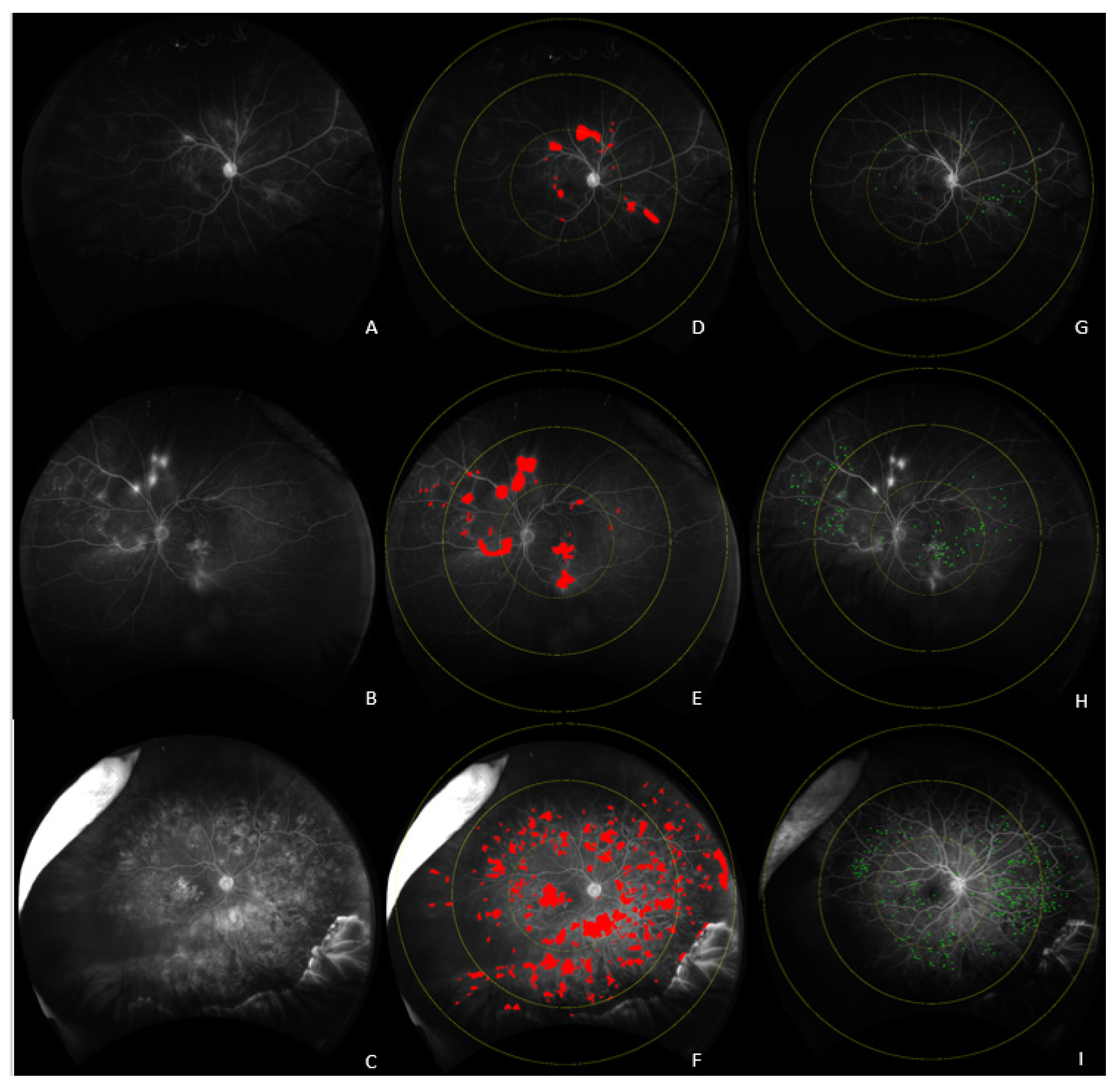
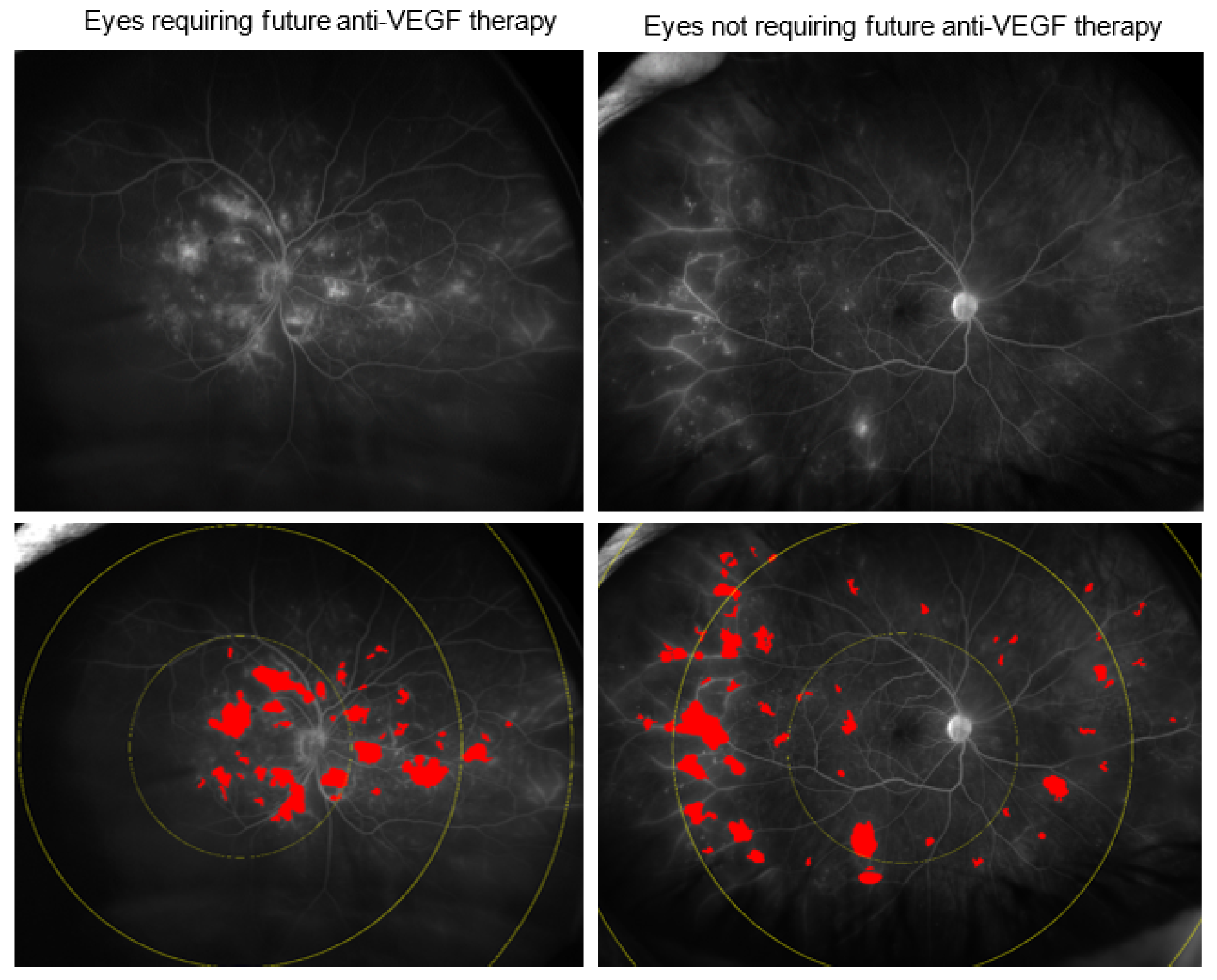
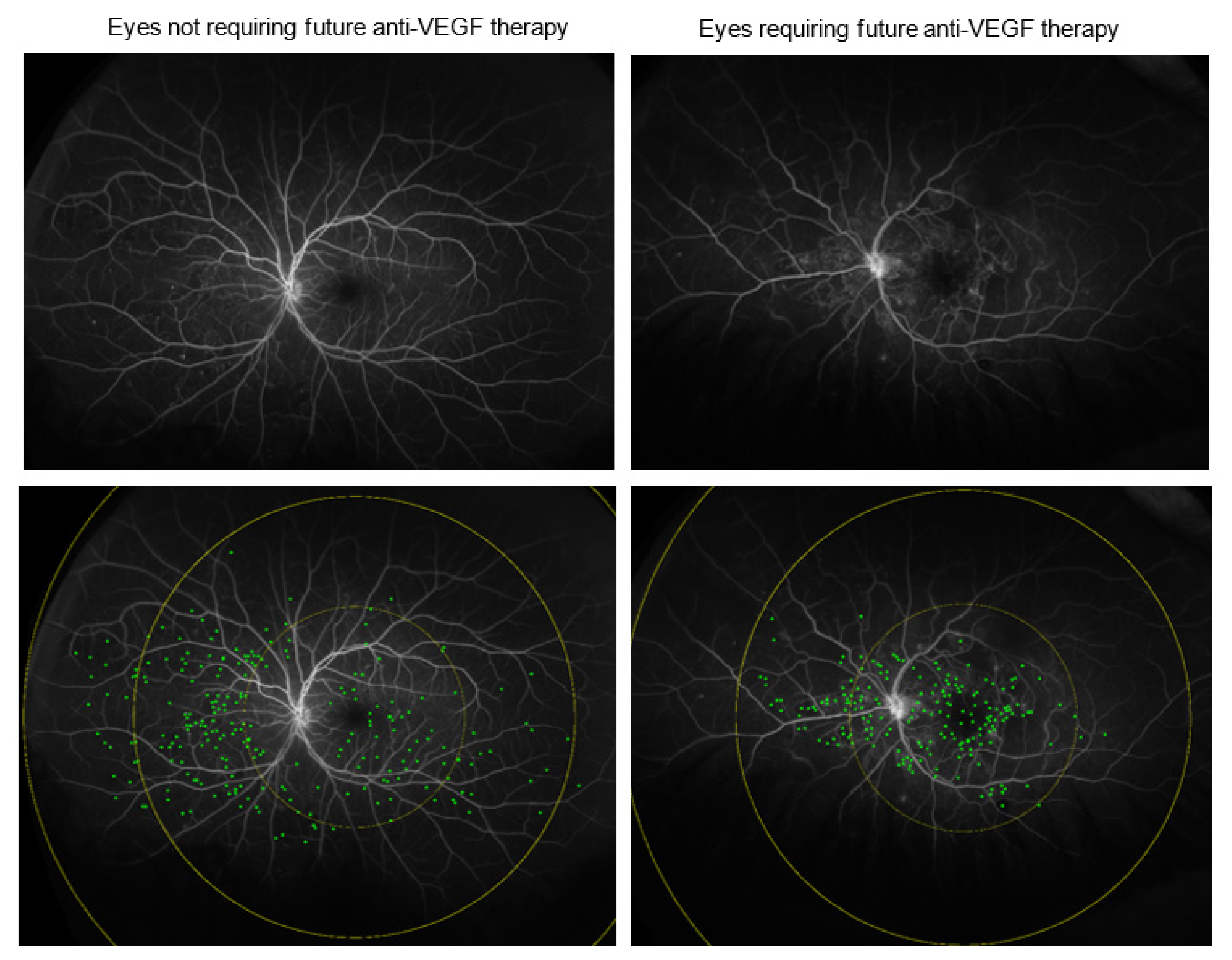
2.1. UWFA Image Analysis
2.2. Statistical Analysis
3. Results
3.1. Early Anti-VEGF Intervention Requirement
3.2. Delayed Anti-VEGF Treatment Requirement
3.3. Comparative Assessment of Eyes Requiring Early vs. Deferred Anti-VEGF Treatment
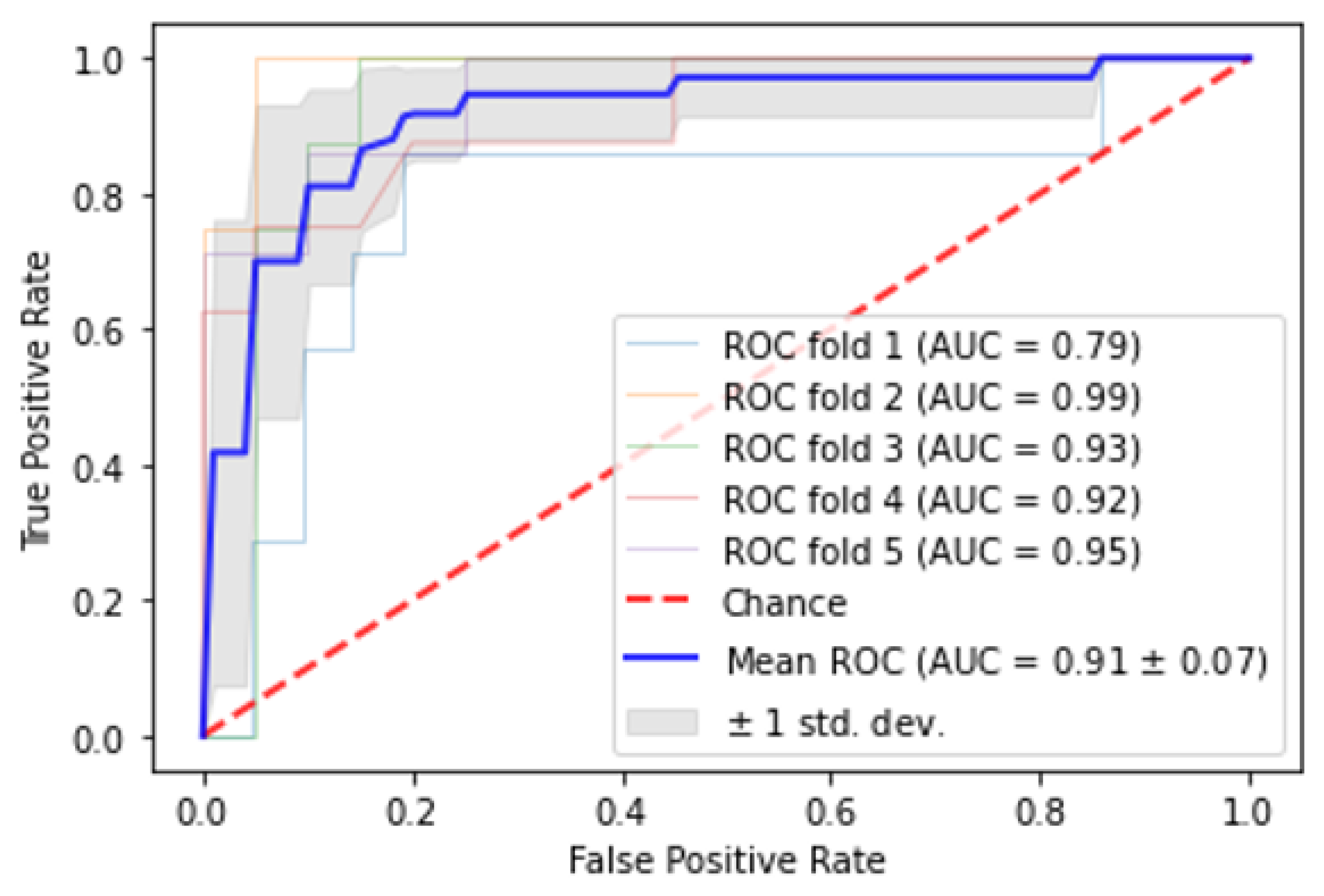
3.4. Automated Classification of Eyes Based on Need for Early or Late Anti-VEGF Therapy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bresnick, G.H. Diabetic Macular Edema: A Review. Ophthalmology 1986, 93, 989–997. [Google Scholar] [CrossRef]
- Photocoagulation For Diabetic Macular Edema: Early Treatment Diabetic Retinopathy Study Report Number 1 Early Treatment Diabetic Retinopathy Study Research Group. Arch. Ophthalmol. 1985, 103, 1796–1806. [CrossRef]
- Jiang, S.; Barner, J.C.; Park, C.; Ling, Y.-L. Treatment Patterns of Anti-Vascular Endothelial Growth Factor and Laser Therapy Among Patients with Diabetic Macular Edema. J. Manag. Care Spec. Pharm. 2015, 21, 735–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, P.; Bandello, F.; Schmidt-Erfurth, U.; Lang, G.E.; Massin, P.; Schlingemann, R.O.; Sutter, F.; Simader, C.; Burian, G.; Gerstner, O.; et al. The RESTORE Study: Ranibizumab Monotherapy or Combined with Laser versus Laser Monotherapy for Diabetic Macular Edema. Ophthalmology 2011, 118, 615–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, J.A.; Glassman, A.R.; Ayala, A.R.; Jampol, L.M.; Bressler, N.M.; Bressler, S.B.; Brucker, A.J.; Ferris, F.L.; Hampton, G.R.; Jhaveri, C.; et al. Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema: Two-Year Results from a Comparative Effectiveness Randomized Clinical Trial. Ophthalmology 2016, 123, 1351–1359. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, Q.D.; Brown, D.M.; Marcus, D.M.; Boyer, D.S.; Patel, S.; Feiner, L.; Gibson, A.; Sy, J.; Rundle, A.C.; Hopkins, J.J.; et al. Ranibizumab for Diabetic Macular Edema: Results from 2 Phase III Randomized Trials: RISE and RIDE. Ophthalmology 2012, 119, 789–801. [Google Scholar] [CrossRef]
- Levin, A.M.; Rusu, I.; Orlin, A.; Gupta, M.P.; Coombs, P.; D’Amico, D.J.; Kiss, S. Retinal Reperfusion in Diabetic Retinopathy Following Treatment with Anti-VEGF Intravitreal Injections. Clin. Ophthalmol. 2017, 11, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Silva, P.S.; Dela Cruz, A.J.; Ledesma, M.G.; van Hemert, J.; Radwan, A.; Cavallerano, J.D.; Aiello, L.M.P.; Sun, J.K.; Aiello, L.M.P. Diabetic Retinopathy Severity and Peripheral Lesions Are Associated with Nonperfusion on Ultrawide Field Angiography. Ophthalmology 2015, 122, 2465–2472. [Google Scholar] [CrossRef]
- Wessel, M.M.; Nair, N.; Aaker, G.D.; Ehrlich, J.R.; D’Amico, D.J.; Kiss, S. Peripheral Retinal Ischaemia, as Evaluated by Ultra-Widefield Fluorescein Angiography, Is Associated with Diabetic Macular Oedema. Br. J. Ophthalmol. 2012, 96, 694–698. [Google Scholar] [CrossRef]
- Ehlers, J.P.; Jiang, A.C.; Boss, J.D.; Hu, M.; Figueiredo, N.; Babiuch, A.; Talcott, K.; Sharma, S.; Hach, J.; Le, T.; et al. Quantitative Ultra-Widefield Angiography and Diabetic Retinopathy Severity. Ophthalmology 2019, 126, 1527–1532. [Google Scholar] [CrossRef]
- Croft, D.E.; van Hemert, J.; Wykoff, C.C.; Clifton, D.; Verhoek, M.; Fleming, A.; Brown, D.M. Precise Montaging and Metric Quantification of Retinal Surface Area from Ultra-Widefield Fundus Photography and Fluorescein Angiography. Ophthalmic Surg. Lasers Imaging Retina 2014, 45, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Wykoff, C.C.; Nittala, M.G.; Zhou, B.; Fan, W.; Velaga, S.B.; Lampen, S.I.R.; Rusakevich, A.M.; Ehlers, J.P.; Babiuch, A.; Brown, D.M.; et al. Intravitreal Aflibercept for Retinal Non-Perfusion in Proliferative Diabetic Retinopathy: Outcomes from the RECOVERY Randomized Trial. Ophthalmol. Retin. 2019, 3, 1076–1086. [Google Scholar] [CrossRef] [PubMed]
- Automated Quantitative Characterisation of Retinal Vascular Leakage and Microaneurysms in Ultra-Widefield Fluorescein Angiography|Enhanced Reader. Available online: Chrome-extension://dagcmkpagjlhakfdhnbomgmjdpkdklff/enhanced-reader.html?openApp&pdf=https%3A%2F%2Fbjo.bmj.com%2Fcontent%2Fbjophthalmol%2F101%2F6%2F696.full.pdf (accessed on 20 May 2021).
- Damla Sevgi, D.; Scott, A.W.; Martin, A.; Mugnaini, C.; Patel, S.; Linz, M.O.; Nti, A.A.; Reese, J.; Ehlers, J.P. Longitudinal Assessment of Quantitative Ultra-Widefield Ischaemic and Vascular Parameters in Sickle Cell Retinopathy. Br. J. Ophthalmol. 2022, 106, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Automated Quality Optimized Phase Selection in Ultra-Widefield Angiography Using Retinal Vessel Segmentation with Deep Neural Networks|IOVS|ARVO Journals. Available online: https://iovs.arvojournals.org/article.aspx?articleid=2770382 (accessed on 20 May 2021).
- Longitudinal Precision of Vasculature Parameter Assessment on Ultra-Widefield Fluorescein Angiography Using a Deep-Learning Model for Vascular Segmentation in Eyes without Vascular Pathology|IOVS|ARVO Journals. Available online: https://iovs.arvojournals.org/article.aspx?articleid=2769705 (accessed on 20 May 2021).
- Bonnin, S.; Dupas, B.; Lavia, C.; Erginay, A.; Dhundass, M.; Couturier, A.; Gaudric, A.; Tadayoni, R. Anti–vascular endothelial growth factor therapy can improve diabetic retinopathy score without change in retinal perfusion. Retina 2019, 39, 426–434. [Google Scholar] [CrossRef]
- Heier, J.S.; Korobelnik, J.F.; Brown, D.M.; Schmidt-Erfurth, U.; Do, D.V.; Midena, E.; Boyer, D.S.; Terasaki, H.; Kaiser, P.K.; Marcus, D.M.; et al. Intravitreal Aflibercept for Diabetic Macular Edema: 148-Week Results from the VISTA and VIVID Studies. Ophthalmology 2016, 123, 2376–2385. [Google Scholar]
- Nunes, S.; Pires, I.; Rosa, A.; Duarte, L.; Bernardes, R.; Cunha-Vaz, J. Microaneurysm Turnover Is a Biomarker for Diabetic Retinopathy Progression to Clinically Significant Macular Edema: Findings for Type 2 Diabetics with Nonproliferative Retinopathy. Ophthalmologica 2009, 223, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Najeeb, B.H.; Simader, C.; Deak, G.; Vass, C.; Gamper, J.; Montuoro, A.; Gerendas, B.S.; Schmidt-Erfurth, U. The Distribution of Leakage on Fluorescein Angiography in Diabetic Macular Edema: A New Approach to Its Etiology. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3986–3990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allingham, M.J.; Mukherjee, D.; Lally, E.B.; Rabbani, H.; Mettu, P.S.; Cousins, S.W.; Farsiu, S. A Quantitative Approach to Predict Differential Effects of Anti-VEGF Treatment on Diffuse and Focal Leakage in Patients with Diabetic Macular Edema: A Pilot Study. Transl. Vis. Sci. Technol. 2017, 6, 7. [Google Scholar] [CrossRef] [Green Version]
- Couturier, A.; Rey, P.-A.; Erginay, A.; Lavia, C.; Bonnin, S.; Dupas, B.; Gaudric, A.; Tadayoni, R. Widefield OCT-Angiography and Fluorescein Angiography Assessments of Nonperfusion in Diabetic Retinopathy and Edema Treated with Anti–Vascular Endothelial Growth Factor. Ophthalmology 2019, 126, 1685–1694. [Google Scholar] [CrossRef]
- Sevgi, D.D.; Srivastava, S.K.; Whitney, J.; O’Connell, M.; Kar, S.S.; Hu, M.; Reese, J.; Madabhushi, A.; Ehlers, J.P. Characterization of Ultra-Widefield Angiographic Vascular Features in Diabetic Retinopathy with Automated Severity Classification. Ophthalmol. Sci. 2021, 1, 100049. [Google Scholar] [CrossRef]
- Moshfeghi, A.; Garmo, V.; Sheinson, D.; Ghanekar, A.; Abbass, I. Five-Year Patterns of Diabetic Retinopathy Progression in Us Clinical Practice. Clin. Ophthalmol. 2020, 14, 3651–3659. [Google Scholar] [CrossRef]
- Sim, D.A.; Keane, P.A.; Rajendram, R.; Karampelas, M.; Selvam, S.; Powner, M.B.; Fruttiger, M.; Tufail, A.; Egan, C.A. Patterns of Peripheral Retinal and Central Macula Ischemia in Diabetic Retinopathy as Evaluated by Ultra-Widefield Fluorescein Angiography. Am. J. Ophthalmol. 2014, 158, 144–153.e1. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.D.; Messner, L.V.; Teitelbaum, B.; Michel, K.A.; Hariprasad, S.M. Characterization of Ischemic Index Using Ultra-Widefield Fluorescein Angiography in Patients with Focal and Diffuse Recalcitrant Diabetic Macular Edema. Am. J. Ophthalmol. 2013, 155, 1038–1044.e2. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, N.; Srivastava, S.K.; Singh, R.P.; Babiuch, A.; Sharma, S.; Rachitskaya, A.; Talcott, K.; Reese, J.; Hu, M.; Ehlers, J.P. Longitudinal Panretinal Leakage and Ischemic Indices in Retinal Vascular Disease Following Aflibercept Therapy: The PERMEATE Study; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Calvo, C.M.; Sridhar, J.; Shahlaee, A.; Ho, A.C. Reduction of Diabetic Macular Edema in the Untreated Fellow Eye Following Intravitreal Injection of Aflibercept. Ophthalmic Surg. Lasers Imaging Retin. 2016, 47, 474–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isildak, H.; Schwartz, S.G.; Flynn, H.W. Therapeutic Effect of Anti-VEGF for Age-Related Macular Degeneration in the Untreated Fellow Eye. Case Rep. Ophthalmol. Med. 2018, 2018, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.S.; Ong, J.M.; Ooi, J.L. Re: “Fellow Eye Effect of Unilateral Intravitreal Bevacizumab Injection in Eyes with Diabetic Macular Edema”. Eye 2015, 29, 291–292. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Not Requiring Treatment (n = 101) | Anti-VEGF Injection within 3 Months (n = 38) | Anti-VEGF Injection after 3 Months (n = 34) | |
|---|---|---|---|
| Age | 63 ± 13 | 66 ± 13 | 62 ± 13 |
| Gender | |||
| Female | 48 | 20 | 17 |
| Male | 53 | 18 | 17 |
| Follow-up time (months) | 21.6 ± 8.3 | 21.0 ± 10.3 | 25.7 ± 10.8 |
| Systolic Blood Pressure | 134.6 ± 15.6 | 139.5 ± 19.8 | 144.6 ± 20.2 |
| Hypertension | 97.0% | 100% | 97.1% |
| Presence of DME on OCT * | 27% | 92% | 65% |
| HbA1c | 8.0 ± 1.8 | 8.4 ± 2.3 | 8.4 ± 2.3 |
| Visual acuity * | 20/25 | 20/80 | 20/50 |
| CST (µm) * | 263 ± 57 | 415 ± 134 | 314 ± 112 |
| Panretinal LI (%) * | 2.0 ± 2.8 | 4.1 ± 3.4 | 4.4 ± 3.7 |
| Macular LI (%) * | 4.3 ± 5.0 | 11.5 ± 7.6 | 12.9 ± 11.3 |
| Panretinal ischemia index (%) | 2.1 ± 1.4 | 3.1 ± 4.1 | 4.7 ± 4.8 |
| Panretinal MA count | 161 ± 131 | 260 ± 385 | 156 ± 125 |
| Macular MA count * | 51 ± 46 | 88 ± 64 | 57 ± 46 |
| Peripheral MA Count * | 108 ± 102 | 167 ± 320 | 97 ± 93 |
| Panretinal vessel area (mm2) | 86.2 ± 19.8 | 92.2 ± 25.3 | 90.6 ± 25.0 |
| Macular vessel area (mm2) * | 16.5 ± 2.1 | 17.1 ± 2.4 | 15.5 ± 2.9 |
| Median vessel density (%) * | 15.1 ± 2.5 | 16.6 ± 2.7 | 16.1 ± 2.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, A.C.; Sevgi, D.D.; Mugnaini, C.; Whitney, J.; Srivastava, S.K.; Talcott, K.E.; Hu, M.; Reese, J.L.; Ehlers, J.P. Predictive Assessment of Quantitative Ultra-Widefield Angiographic Features for Future Need for Anti-VEGF Therapy in Diabetic Eye Disease. J. Pers. Med. 2022, 12, 608. https://doi.org/10.3390/jpm12040608
Jiang AC, Sevgi DD, Mugnaini C, Whitney J, Srivastava SK, Talcott KE, Hu M, Reese JL, Ehlers JP. Predictive Assessment of Quantitative Ultra-Widefield Angiographic Features for Future Need for Anti-VEGF Therapy in Diabetic Eye Disease. Journal of Personalized Medicine. 2022; 12(4):608. https://doi.org/10.3390/jpm12040608
Chicago/Turabian StyleJiang, Alice C., Duriye Damla Sevgi, Christopher Mugnaini, Jon Whitney, Sunil K. Srivastava, Katherine E. Talcott, Ming Hu, Jamie L. Reese, and Justis P. Ehlers. 2022. "Predictive Assessment of Quantitative Ultra-Widefield Angiographic Features for Future Need for Anti-VEGF Therapy in Diabetic Eye Disease" Journal of Personalized Medicine 12, no. 4: 608. https://doi.org/10.3390/jpm12040608
APA StyleJiang, A. C., Sevgi, D. D., Mugnaini, C., Whitney, J., Srivastava, S. K., Talcott, K. E., Hu, M., Reese, J. L., & Ehlers, J. P. (2022). Predictive Assessment of Quantitative Ultra-Widefield Angiographic Features for Future Need for Anti-VEGF Therapy in Diabetic Eye Disease. Journal of Personalized Medicine, 12(4), 608. https://doi.org/10.3390/jpm12040608