
Enhanced Risk of Osteoporotic Fracture in Patients with Sarcopenia: A National Population-Based Study in Taiwan

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
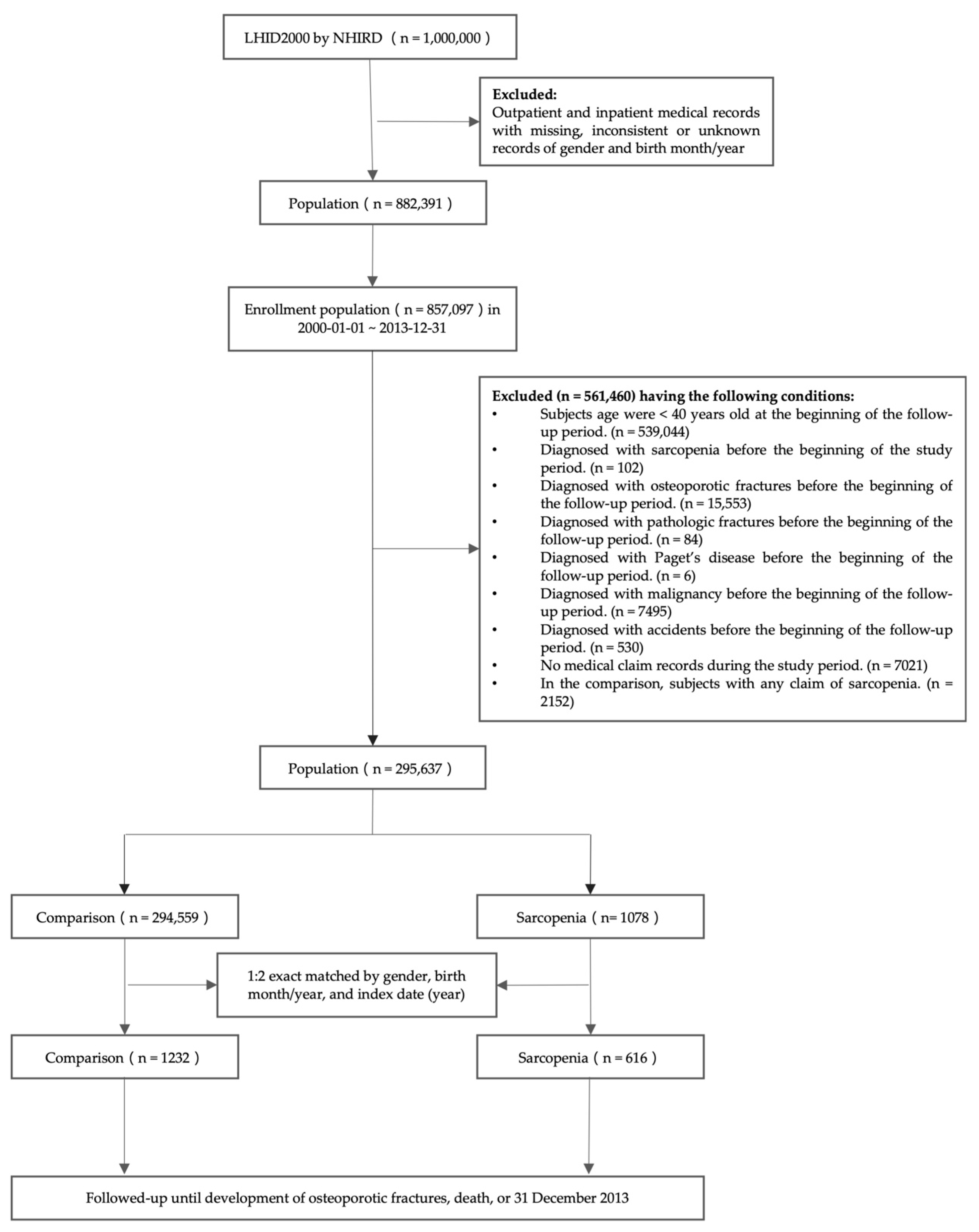
2.2. Study Design and Population
2.3. Selection and Length of Exposure
2.4. Definition of the Frequency of Osteoporotic Fracture
2.5. Potential Confounding Factors
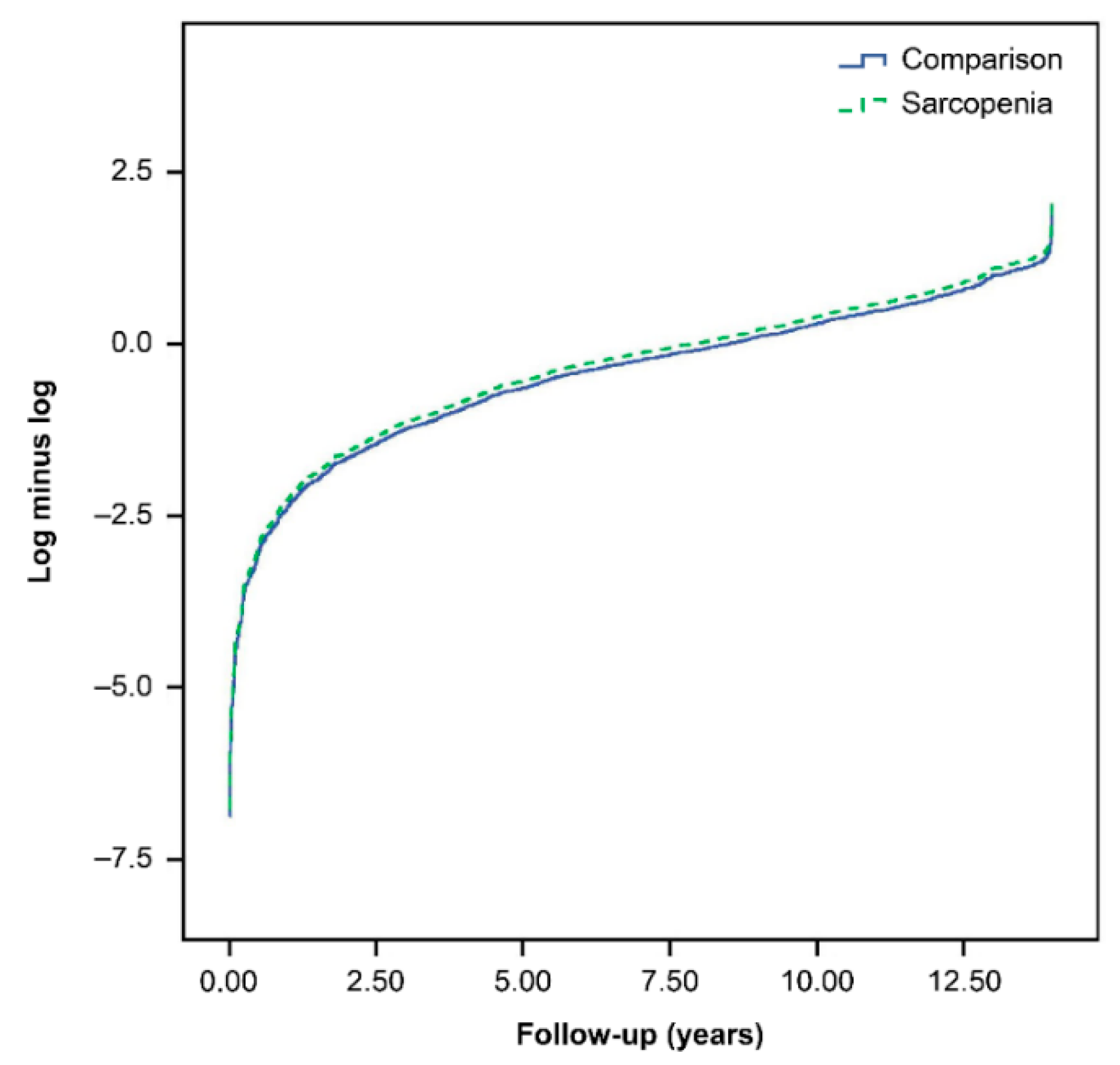
2.6. Statistical Analysis
3. Results
3.1. Clinical Details of the Study Population
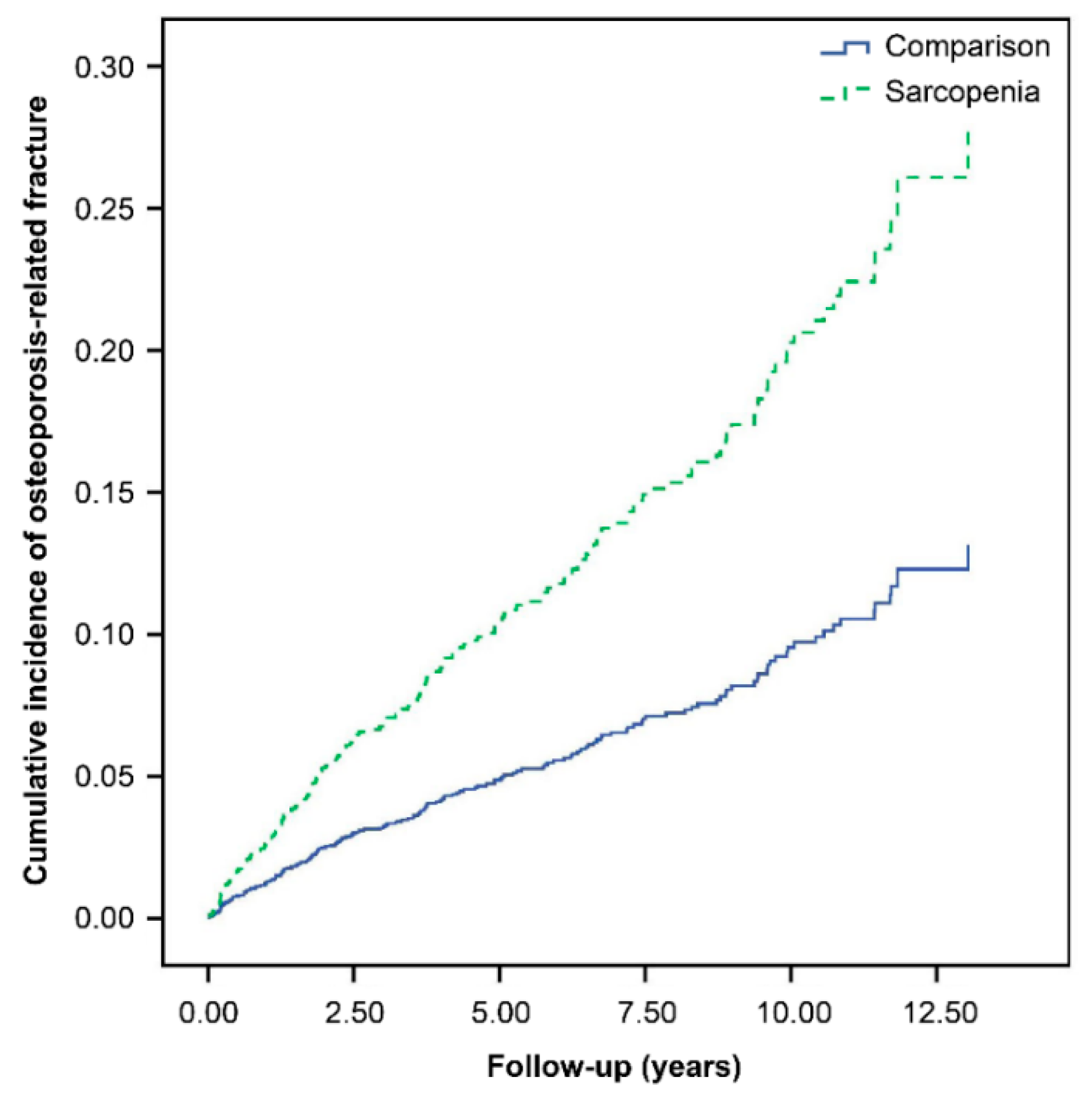
3.2. Associations between Sarcopenia and Osteoporosis-Related Fracture
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Hao, Q.; Hai, S.; Wang, H.; Cao, L.; Dong, B. Sarcopenia as a predictor of all-cause mortality among community-dwelling older people: A systematic review and meta-analysis. Maturitas 2017, 103, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, M.H.; Kuo, Y.J.; Chen, Y.P. The Association Between Sarcopenia and Postoperative Outcomes Among Older Adults With Hip Fracture: A Systematic Review. J. Appl. Gerontol. 2021, 40, 1903–1913. [Google Scholar] [CrossRef]
- Pisano, C.; Polisano, D.; Balistreri, C.R.; Altieri, C.; Nardi, P.; Bertoldo, F.; Trombetti, D.; Asta, L.; Ferrante, M.S.; Buioni, D.; et al. Role of Cachexia and Fragility in the Patient Candidate for Cardiac Surgery. Nutrients 2021, 13, 517. [Google Scholar] [CrossRef]
- Aibar-Almazán, A.; Martínez-Amat, A.; Cruz-Díaz, D.; Jiménez-García, J.D.; Achalandabaso, A.; Sánchez-Montesinos, I.; de la Torre-Cruz, M.; Hita-Contreras, F. Sarcopenia and sarcopenic obesity in Spanish community-dwelling middle-aged and older women: Association with balance confidence, fear of falling and fall risk. Maturitas 2018, 107, 26–32. [Google Scholar] [CrossRef]
- Benichou, O.; Lord, S.R. Rationale for Strengthening Muscle to Prevent Falls and Fractures: A Review of the Evidence. Calcif. Tissue Tissue Int. 2016, 98, 531–545. [Google Scholar] [CrossRef]
- He, H.; Liu, Y.; Tian, Q.; Papasian, C.J.; Hu, T.; Deng, H.W. Relationship of sarcopenia and body composition with osteoporosis. Osteoporos Int. 2016, 27, 473–482. [Google Scholar] [CrossRef]
- Inoue, T.; Maeda, K.; Nagano, A.; Shimizu, A.; Ueshima, J.; Murotani, K.; Sato, K.; Hotta, K.; Morishita, S.; Tsubaki, A. Related Factors and Clinical Outcomes of Osteosarcopenia: A Narrative Review. Nutrients 2021, 13, 291. [Google Scholar] [CrossRef]
- Oliveira, A.; Vaz, C. The role of sarcopenia in the risk of osteoporotic hip fracture. Clin. Rheumatol. 2015, 34, 1673–1680. [Google Scholar] [CrossRef]
- (NHIRD). N.H.I.R.D. Introduction to the National Health Insurance Research Database. Available online: http://nhird.nhri.org.tw/en/index.html (accessed on 1 April 2022).
- Sherman, R.E.; Anderson, S.A.; Dal Pan, G.J.; Gray, G.W.; Gross, T.; Hunter, N.L.; LaVange, L.; Marinac-Dabic, D.; Marks, P.W.; Robb, M.A.; et al. Real-World Evidence—What Is It and What Can It Tell Us? N. Engl. J. Med. 2016, 375, 2293–2297. [Google Scholar] [CrossRef] [Green Version]
- Anker, S.D.; Morley, J.E.; von Haehling, S. Welcome to the ICD-10 code for sarcopenia. J. Cachexia Sarcopenia Muscle 2016, 7, 512–514. [Google Scholar] [CrossRef]
- Lin, M.-H.; Chiu, S.-Y.; Chang, P.-H.; Lai, Y.-L.; Chen, P.-C.; Ho, W.-C. Hyperlipidemia and Statins Use for the Risk of New Diagnosed Sarcopenia in Patients with Chronic Kidney: A Population-Based Study. Int J. Environ. Res. Public Health 2020, 17, 1494. [Google Scholar] [CrossRef] [Green Version]
- Bishwakarma, R.; Zhang, W.; Lin, Y.L.; Kuo, Y.F.; Cardenas, V.J.; Sharma, G. Metformin use and health care utilization in patients with coexisting chronic obstructive pulmonary disease and diabetes mellitus. Int. J. Chronic Obstruct. Pulmon. Dis. 2018, 13, 793–800. [Google Scholar] [CrossRef] [Green Version]
- Pacifico, J.; Geerlings, M.A.J.; Reijnierse, E.M.; Phassouliotis, C.; Lim, W.K.; Maier, A.B. Prevalence of sarcopenia as a comorbid disease: A systematic review and meta-analysis. Exp. Gerontol. 2020, 131, 110801. [Google Scholar] [CrossRef]
- Dennison, E.M.; Sayer, A.A.; Cooper, C. Epidemiology of sarcopenia and insight into possible therapeutic targets. Nat. Rev. Rheumatol. 2017, 13, 340–347. [Google Scholar] [CrossRef] [Green Version]
- Watson, K.B.; Carlson, S.A.; Gunn, J.P.; Galuska, D.A.; O’Connor, A.; Greenlund, K.J.; Fulton, J.E. Physical inactivity among adults aged 50 years and older—United States, 2014. Morb. Mortal. Wkly. Rep. 2016, 65, 954–958. [Google Scholar] [CrossRef]
- Bekfani, T.; Pellicori, P.; Morris, D.A.; Ebner, N.; Valentova, M.; Steinbeck, L.; Wachter, R.; Elsner, S.; Sliziuk, V.; Schefold, J.C. Sarcopenia in patients with heart failure with preserved ejection fraction: Impact on muscle strength, exercise capacity and quality of life. Int. J. Cardiol. 2016, 222, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Group, L.P.A.S.W. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Chaicharn Pothirat, M.; Chaiwong, W.; Phetsuk, N.; Liwsrisakun, C.; Bumroongkit, C.; Deesomchok, A.; Theerakittikul, T.; Limsukon, A. The relationship between body composition and clinical parameters in chronic obstructive pulmonary disease. J. Med. Assoc. Thai 2016, 99, 386–393. [Google Scholar]
- Dalle, S.; Rossmeislova, L.; Koppo, K. The Role of Inflammation in Age-Related Sarcopenia. Front. Physiol. 2017, 8, 1045. [Google Scholar] [CrossRef] [Green Version]
- Fávaro-Moreira, N.C.; Krausch-Hofmann, S.; Matthys, C.; Vereecken, C.; Vanhauwaert, E.; Declercq, A.; Bekkering, G.E.; Duyck, J. Risk factors for malnutrition in older adults: A systematic review of the literature based on longitudinal data. Adv. Nutr. 2016, 7, 507–522. [Google Scholar] [CrossRef]
- Sieber, C.C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef]
- Waters, D.L.; Hale, L.; Grant, A.M.; Herbison, P.; Goulding, A. Osteoporosis and gait and balance disturbances in older sarcopenic obese New Zealanders. Osteoporos. Int. 2010, 21, 351–357. [Google Scholar] [CrossRef]
- Reiss, J.; Iglseder, B.; Alzner, R.; Mayr-Pirker, B.; Pirich, C.; Kässmann, H.; Kreutzer, M.; Dovjak, P.; Reiter, R. Sarcopenia and osteoporosis are interrelated in geriatric inpatients. Z. Gerontol. Geriatr. 2019, 52, 688–693. [Google Scholar] [CrossRef] [Green Version]
- Muir, S.W.; Berg, K.; Chesworth, B.; Klar, N.; Speechley, M. Quantifying the magnitude of risk for balance impairment on falls in community-dwelling older adults: A systematic review and meta-analysis. J. Clin. Epidemiol. 2010, 63, 389–406. [Google Scholar] [CrossRef]
- Bijlsma, A.Y.; Pasma, J.H.; Lambers, D.; Stijntjes, M.; Blauw, G.J.; Meskers, C.G.; Maier, A.B. Muscle strength rather than muscle mass is associated with standing balance in elderly outpatients. J. Am. Medical. Dir. Assoc. 2013, 14, 493–498. [Google Scholar] [CrossRef]
- Ochi, M.; Tabara, Y.; Kido, T.; Uetani, E.; Ochi, N.; Igase, M.; Miki, T.; Kohara, K. Quadriceps sarcopenia and visceral obesity are risk factors for postural instability in the middle-aged to elderly population. Geriatr. Gerontol. Int. 2010, 10, 233–243. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef] [Green Version]
- Patel, H.P.; Syddall, H.E.; Jameson, K.; Robinson, S.; Denison, H.; Roberts, H.C.; Edwards, M.; Dennison, E.; Cooper, C.; Aihie Sayer, A. Prevalence of sarcopenia in community-dwelling older people in the UK using the European Working Group on Sarcopenia in Older People (EWGSOP) definition: Findings from the Hertfordshire Cohort Study (HCS). Age Ageing 2013, 42, 378–384. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.P.; Wong, P.K.; Tsai, M.J.; Chang, W.C.; Hsieh, T.S.; Leu, T.H.; Jeff Lin, C.F.; Lee, C.H.; Kuo, Y.J.; Lin, C.Y. The high prevalence of sarcopenia and its associated outcomes following hip surgery in Taiwanese geriatric patients with a hip fracture. J. Formos Med. Assoc. 2020, 119, 1807–1816. [Google Scholar] [CrossRef]
- Edwards, M.H.; Dennison, E.M.; Aihie Sayer, A.; Fielding, R.; Cooper, C. Osteoporosis and sarcopenia in older age. Bone 2015, 80, 126–130. [Google Scholar] [CrossRef] [Green Version]
- Frost, H.M. Bone’s mechanostat: A 2003 update. Anat Rec. A Discov. Mol. Cell Evol. Biol. 2003, 275, 1081–1101. [Google Scholar] [CrossRef]
- Messier, V.; Rabasa-Lhoret, R.; Barbat-Artigas, S.; Elisha, B.; Karelis, A.D.; Aubertin-Leheudre, M. Menopause and sarcopenia: A potential role for sex hormones. Maturitas 2011, 68, 331–336. [Google Scholar] [CrossRef]
- Frisoli, A., Jr.; Martin, F.G.; Carvalho, A.C.C.; Borges, J.; Paes, A.T.; Ingham, S.J.M. Sex effects on the association between sarcopenia EWGSOP and osteoporosis in outpatient older adults: Data from the SARCOS study. Arch. Endocrinol. Metab. 2018, 62, 615–622. [Google Scholar] [CrossRef] [Green Version]
- Scott, D.; Seibel, M.; Cumming, R.; Naganathan, V.; Blyth, F.; Le Couteur, D.G.; Handelsman, D.J.; Waite, L.M.; Hirani, V. Sarcopenic Obesity and Its Temporal Associations With Changes in Bone Mineral Density, Incident Falls, and Fractures in Older Men: The Concord Health and Ageing in Men Project. J. Bone Miner. Res. 2017, 32, 575–583. [Google Scholar] [CrossRef]
- Hars, M.; Biver, E.; Chevalley, T.; Herrmann, F.; Rizzoli, R.; Ferrari, S.; Trombetti, A. Low Lean Mass Predicts Incident Fractures Independently From FRAX: A Prospective Cohort Study of Recent Retirees. J. Bone Miner. Res. 2016, 31, 2048–2056. [Google Scholar] [CrossRef]
- Chalhoub, D.; Cawthon, P.M.; Ensrud, K.E.; Stefanick, M.L.; Kado, D.M.; Boudreau, R.; Greenspan, S.; Newman, A.B.; Zmuda, J.; Orwoll, E.S.; et al. Risk of Nonspine Fractures in Older Adults with Sarcopenia, Low Bone Mass, or Both. J. Am. Geriatr. Soc. 2015, 63, 1733–1740. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) | p-Value | |
|---|---|---|---|
| Comparison Cohort (n = 1232) | Sarcopenia Cohort (n = 616) | ||
| Age, years | 0.950 | ||
| Mean ± SD | 60.37 ± 12.00 | 60.41 ± 12.00 | |
| Sex | Matched | ||
| Male | 622 (50.49) | 311 (50.49) | |
| Urbanization level a | <0.001 | ||
| 1 (highest) | 605 (49.11) | 334 (54.22) | |
| 2 | 370 (30.03) | 146 (23.70) | |
| 3 | 90 (7.31) | 25 (4.06) | |
| 4 (lowest) | 14 (1.14) | 3 (0.49) | |
| Unknown | 153 (12.42) | 108 (17.53) | |
| Insurance amount b, NT$ | 0.498 | ||
| Financially dependent | 13 (1.06) | 7 (1.14) | |
| 1–19,999 | 567 (46.02) | 262 (42.53) | |
| 20,000–39,999 | 400 (32.47) | 202 (32.79) | |
| ≥40,000 | 152 (12.34) | 92 (14.94) | |
| Unknown | 100 (8.12) | 53 (8.60) | |
| Confounding factors c | |||
| Rheumatoid arthritis | 12 (0.97) | 26 (4.22) | <0.001 |
| Smoking habit | 78 (6.33) | 98 (15.91) | 0.014 |
| Alcohol use | 26 (2.11) | 26 (4.22) | 0.700 |
| Hypertension | 327 (26.54) | 197 (31.98) | 0.012 |
| Diabetes | 253 (20.54) | 243 (39.45) | <0.001 |
| Dyslipidemia | 159 (12.91) | 265 (43.02) | <0.001 |
| Obesity | 2 (0.16) | 8 (1.30) | 0.005 |
| Coronary heart disease | 199 (16.15) | 235 (38.15) | <0.001 |
| Stroke | 184 (14.94) | 234 (37.99) | <0.001 |
| Chronic obstructive pulmonary disease | 163 (13.23) | 281 (45.62) | <0.001 |
| Depression | 29 (2.35) | 23 (3.73) | 0.102 |
| Cognitive dysfunction | 51 (4.14) | 85 (13.80) | <0.001 |
| Parkinson’s disease | 26 (2.11) | 50 (8.12) | <0.001 |
| Use of glucocorticoids | 174 (14.12) | 267 (43.34) | <0.001 |
| Population # | Study Group | Osteoporosis-Related Fracture | PY | Rate a | Crude HR (95% CI) | Adjusted HR b (95% CI) |
|---|---|---|---|---|---|---|
| Total | Comparison (n = 1232) | 111 | 7599 | 14.61 | 1 (reference) | 1 (reference) |
| Sarcopenia (n = 616) | 65 | 3585 | 18.13 | 1.23 (0.90, 1.67) | 2.11 (1.47, 3.04) ‡ | |
| Female | Comparison (n = 610) | 64 | 3894 | 16.44 | 1 (reference) | 1 (reference) |
| Sarcopenia (n = 305) | 45 | 1804 | 24.95 | 1.50 (1.02, 2.20) * | 2.40 (1.51, 3.81) ‡ | |
| Male | Comparison (n = 622) | 47 | 3705 | 12.69 | 1 (reference) | 1 (reference) |
| Sarcopenia (n = 311) | 20 | 1781 | 11.23 | 0.88 (0.52, 1.48) | 1.53 (0.83, 2.82) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.-W.; Tsai, Z.-R.; Chen, K.-T.; Hsu, S.-L.; Kuo, Y.-J.; Lin, Y.-C.; Huang, S.-W.; Chen, Y.-P.; Peng, H.-C.; Tsai, J.J.P.; et al. Enhanced Risk of Osteoporotic Fracture in Patients with Sarcopenia: A National Population-Based Study in Taiwan. J. Pers. Med. 2022, 12, 791. https://doi.org/10.3390/jpm12050791
Zhang H-W, Tsai Z-R, Chen K-T, Hsu S-L, Kuo Y-J, Lin Y-C, Huang S-W, Chen Y-P, Peng H-C, Tsai JJP, et al. Enhanced Risk of Osteoporotic Fracture in Patients with Sarcopenia: A National Population-Based Study in Taiwan. Journal of Personalized Medicine. 2022; 12(5):791. https://doi.org/10.3390/jpm12050791
Chicago/Turabian StyleZhang, Han-Wei, Zhi-Ren Tsai, Ko-Ta Chen, Sheng-Lun Hsu, Yi-Jie Kuo, Ying-Chin Lin, Shu-Wei Huang, Yu-Pin Chen, Hsiao-Ching Peng, Jeffrey J. P. Tsai, and et al. 2022. "Enhanced Risk of Osteoporotic Fracture in Patients with Sarcopenia: A National Population-Based Study in Taiwan" Journal of Personalized Medicine 12, no. 5: 791. https://doi.org/10.3390/jpm12050791
APA StyleZhang, H. -W., Tsai, Z. -R., Chen, K. -T., Hsu, S. -L., Kuo, Y. -J., Lin, Y. -C., Huang, S. -W., Chen, Y. -P., Peng, H. -C., Tsai, J. J. P., & Hsu, C. Y. (2022). Enhanced Risk of Osteoporotic Fracture in Patients with Sarcopenia: A National Population-Based Study in Taiwan. Journal of Personalized Medicine, 12(5), 791. https://doi.org/10.3390/jpm12050791