
Exposure to Proton Pump Inhibitors and the Risk of Incident Asthma in Patients with Coronary Artery Diseases: A Population-Based Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
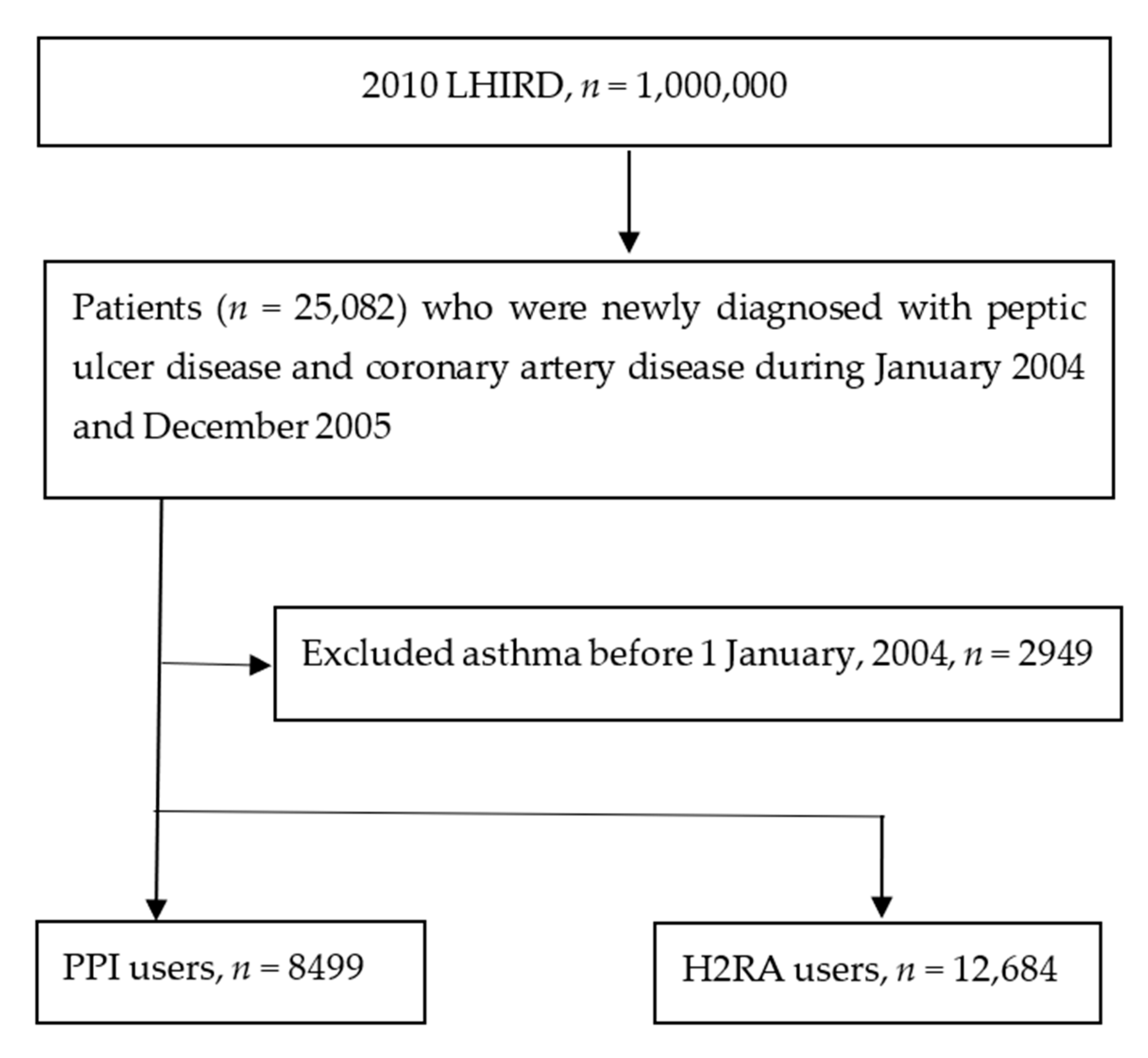
2.1. Study Design and Setting
2.2. Study Outcome
2.3. Study Variables
2.4. Data Analysis
3. Results
3.1. Characteristics of the Study Participants
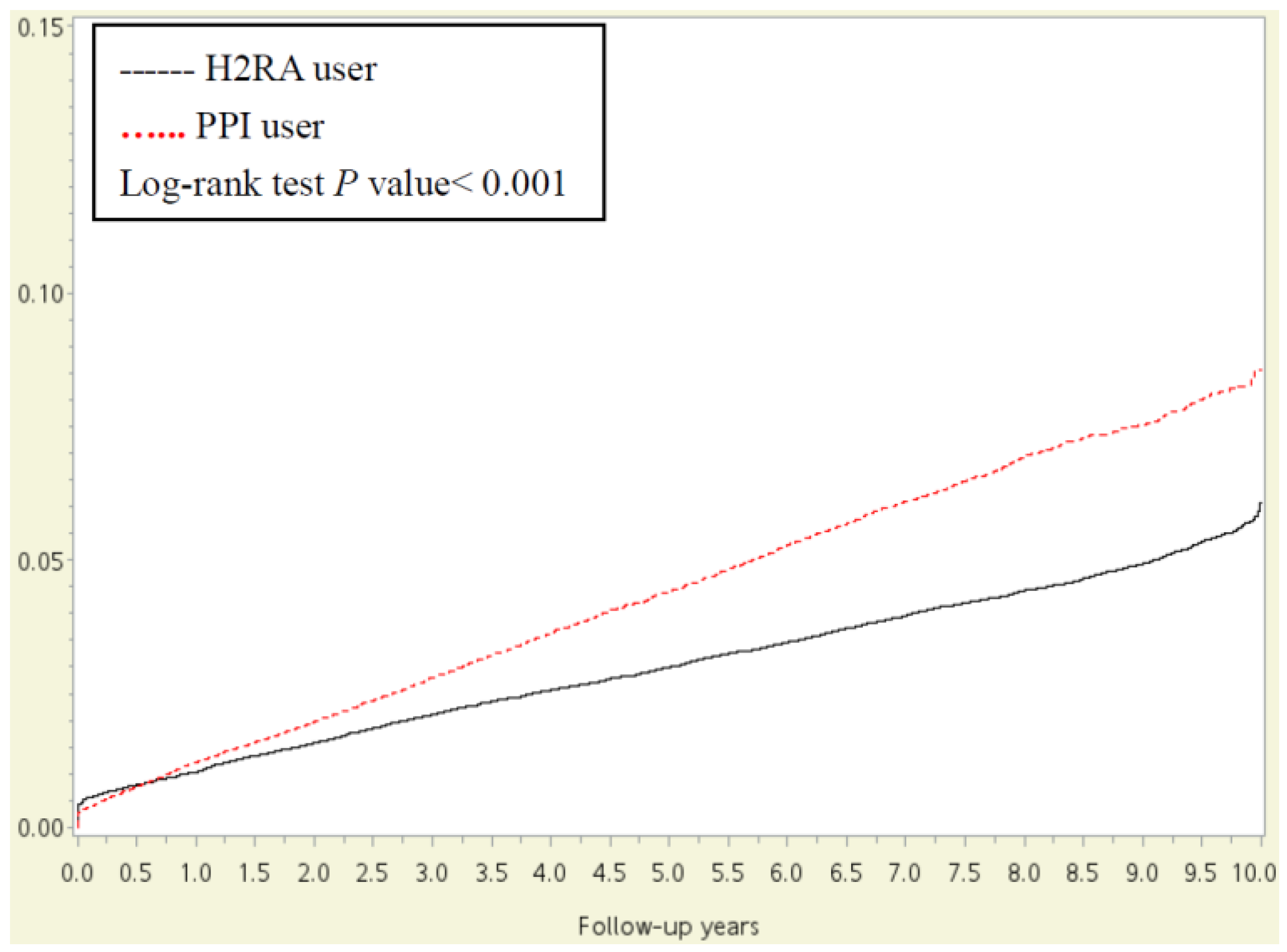
3.2. Association between PPI User and Asthma
3.3. Sensitivity and Subgroup Analyses
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Prevalence, Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 328 Diseases and Injuries for 195 Countries, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Lanas, A.; Gargallo, C.J. Management of Low-Dose Aspirin and Clopidogrel in Clinical Practice: A Gastrointestinal Perspective. J. Gastroenterol. 2015, 50, 626–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, W.W.; Chiou, E.; Obstein, K.L.; Tignor, A.S.; Whitlock, T.L. The Efficacy of Proton Pump Inhibitors for the Treatment of Asthma in Adults: A Meta-Analysis. Arch. Intern. Med. 2011, 171, 620–629. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Bidirectional Association between GERD and Asthma: Two Longitudinal Follow-up Studies Using a National Sample Cohort. J. Allergy Clin. Immunol. Pract. 2020, 8, 1005–1013.e9. [Google Scholar] [CrossRef] [PubMed]
- Kiljander, T.O.; Junghard, O.; Beckman, O.; Lind, T. Effect of Esomeprazole 40 MG Once or Twice Daily on Asthma: A Randomized, Placebo-Controlled Study. Am. J. Respir. Crit. Care Med. 2010, 181, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Luo, Y.; Li, J.; Gao, J. Randomised Trials of Proton Pump Inhibitors for Gastro-Oesophageal Reflux Disease in Patients with Asthma: An Updated Systematic Review and Meta-Analysis. BMJ. Open 2021, 11, e043860. [Google Scholar] [CrossRef]
- Kiljander, T.O.; Harding, S.M.; Field, S.K.; Stein, M.R.; Nelson, H.S.; Ekelund, J.; Illueca, M.; Beckman, O.; Sostek, M.B. Effects of Esomeprazole 40 mg Twice Daily on Asthma: A Randomized Placebo-Controlled Trial. Am. J. Respir. Crit. Care Med. 2006, 73, 1091–1097. [Google Scholar] [CrossRef]
- Yagoubi, A.; Laid, Y.; Smati, L.; Nafissa Benhalla, K.; Benhassine, F. Does Omeprazole Improve Asthma-Control in Poorly-Controlled Asthmatic Children with Gastro-Esophageal Reflux. J. Asthma 2021, 5, 1–8. [Google Scholar] [CrossRef]
- Holbrook, J.T.; Wise, R.A.; Gold, B.D.; Blake, K.; Brown, E.D.; Castro, M.; Dozor, A.J.; Lima, J.J.; Mastronarde, J.G.; et al.; Writing Committee for the American Lung Association Asthma Clinical Research Centers Lansoprazole for Children with Poorly Controlled Asthma: A Randomized Controlled Trial. JAMA. 2012, 307, 373–381. [Google Scholar]
- dos Santos, L.H.; Ribeiro, I.O.; Sánchez, P.G.; Hetzel, J.L.; Felicetti, J.C.; Cardoso, P.F. Evaluation of Pantoprazol Treatment Response of Patients with Asthma and Gastroesophageal Reflux: A Randomized Prospective Double-Blind Placebo-Controlled Study. J. Bras. Pneumol. 2007, 3, 119–127. [Google Scholar]
- Wang, Y.T.; Tsai, M.C.; Wang, Y.H.; Wei, J.C. Association between Proton Pump Inhibitors and Asthma: A Population-Based Cohort Study. Front. Pharmacol. 2020, 11, 607. [Google Scholar] [CrossRef] [PubMed]
- Hak, E.; Mulder, B.; Schuiling-Veninga, C.C.; de Vries, T.W.; Jick, S.S. Use of Acid Suppressive Drugs in Pregnancy and the Risk of Childhood Asthma: Bidirectional Crossover Study Using the General Practice Research Database. Drug Saf. 2013, 36, 1097–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulder, B.; Schuiling-Veninga, C.C.; Bos, H.J.; De Vries, T.W.; Jick, S.S.; Hak, E. Prenatal Exposure to Acid-Suppressive Drugs and the Risk of Allergic Diseases in the Offspring: A Cohort Study. Clin. Exp. Allergy 2014, 44, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.H.; Wintzell, V.; Ludvigsson, J.F.; Svanström, H.; Pasternak, B. Association between Proton Pump Inhibitor Use and Risk of Asthma in Children. JAMA Pediatr. 2021, 175, 394–403. [Google Scholar] [CrossRef]
- Dehlink, E.; Yen, E.; Leichtner, A.M.; Hait, E.J.; Fiebiger, E. First Evidence of a Possible Association between Gastric Acid Suppression during Pregnancy and Childhood Asthma: A Population-Based Register Study. Clin. Exp. Allergy 2009, 39, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Pali-Schöll, I.; Untersmayr, E.; Klems, M.; Jensen-Jarolim, E. The Effect of Digestion and Digestibility on Allergenicity of Food. Nutrients 2018, 10, 1129. [Google Scholar] [CrossRef] [Green Version]
- Bornehag, C.G.; Nanberg, E. Phthalate Exposure and Asthma in Children. Int. J. Androl. 2010, 33, 333–345. [Google Scholar] [CrossRef]
- Yepuri, G.; Sukhovershin, R.; Nazari-Shafti, T.Z.; Petrascheck, M.; Ghebre, Y.T.; Cooke, J.P. Proton Pump Inhibitors Accelerate Endothelial Senescence. Circ. Res. 2016, 118, e36–e42. [Google Scholar] [CrossRef] [Green Version]
- Ruigómez, A.; Rodríguez, L.A.; Wallander, M.A.; Johansson, S.; Thomas, M.; Price, D. Gastroesophageal Reflux Disease and Asthma: A Longitudinal Study in UK General Practice. Chest 2005, 128, 85–93. [Google Scholar] [CrossRef]
- Drug, V.L.; Antoniu, S.; Oana, B.B.; Arghir, O.C.; Bancila, I.; Bataga, S.; Brisc, C.; Cijevschi-Prelipcean, C.; Ciocîrlan, M.; Ciortescu, I.; et al. Romanian Guidelines for the Diagnosis and Treatment of GERD-Induced Respiratory Manifestations. J. Gastrointestin. Liver Dis. 2022, 31, 119–142. [Google Scholar] [CrossRef]
- Jaspersen, D.; Nocon, M.; Labenz, J.; Leodolter, A.; Richter, K.; Stolte, M.; Vieth, M.; Lind, T.; Willich, S.N.; Malfertheiner, P. Clinical Course of Laryngo-Respiratory Symptoms in Gastro-Oesophageal Reflux Disease during Routine Care—A 5-Year Follow-up. Aliment. Pharmacol. Ther. 2009, 29, 1172–1178. [Google Scholar] [CrossRef] [PubMed]
- Havemann, B.D.; Henderson, C.A.; El-Serag, H.B. The Association between Gastro-Oesophageal Reflux Disease and Asthma: A Systematic Review. Gut 2007, 56, 1654–1664. [Google Scholar] [CrossRef] [Green Version]
- Fortuna, L.A.; Pawloski, P.A.; Parker, E.D.; Trower, N.K.; Kottke, T.E. Proton Pump Inhibitor Use by Aspirin-Treated Coronary Artery Disease Patients Is Not Associated with Increased Risk of Cardiovascular Events. Eur. Heart J. Cardiovasc. Pharmacother. 2016, 2, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pello Lázaro, A.M.; Cristóbal, C.; Franco-Peláez, J.A.; Tarín, N.; Aceña, Á.; Carda, R.; Huelmos, A.; Martín-Mariscal, M.L.; Fuentes-Antras, J.; Martínez-Millá, J.; et al. Use of Proton-Pump Inhibitors Predicts Heart Failure and Death in Patients with Coronary Artery Disease. PLoS ONE 2017, 12, e0169826. [Google Scholar] [CrossRef] [PubMed]
- Krill, T.; Brown, G.; Weideman, R.A.; Cipher, D.J.; Spechler, S.J.; Brilakis, E.; Feagins, L.A. Patients with Cirrhosis Who Have Coronary Artery Disease Treated with Cardiac Stents Have High Rates of Gastrointestinal Bleeding, but No Increased Mortality. Aliment. Pharmacol. Ther. 2017, 46, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Kurth, T.; Barr, R.G.; Gaziano, J.M.; Buring, J.E. Randomised Aspirin Assignment and Risk of Adult-Onset Asthma in the Women’s Health Study. Thorax 2008, 63, 514–518. [Google Scholar] [CrossRef] [Green Version]
- Barr, R.G.; Kurth, T.; Stampfer, M.J.; Burin, J.E.; Hennekens, C.H.; Gaziano, J.M. Aspirin and Decreased Adult-Onset Asthma: Randomized Comparisons from the Physicians’ Health Study. Am. J. Respir. Crit. Care Med. 2007, 175, 120–125. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| H2RA n = 12,684 | PPI n = 8499 | p-Value | |
|---|---|---|---|
| Sex | <0.001 | ||
| Female | 7013 (55.29%) | 3537 (41.62%) | |
| Male | 5671 (44.71%) | 4962 (58.38%) | |
| Age | <0.001 | ||
| <20 | 483 (3.81%) | 133 (1.56%) | |
| 20–45 | 4724 (37.24%) | 3061 (36.02%) | |
| 45–60 | 4004 (31.57%) | 2858 (33.63%) | |
| 60–75 | 2466 (19.44%) | 1567 (18.44%) | |
| >= 75 | 1007 (7.94%) | 880 (10.35%) | |
| Urbanization | 0.0736 | ||
| Urban | 7359 (58.02%) | 5060 (59.54%) | |
| Sub-urban | 3827 (30.17%) | 2593 (30.51%) | |
| Rural | 1498 (11.81%) | 846 (9.95%) | |
| Low income | 88 (0.65%) | 49 (0.58%) | 0.4904 |
| Comorbidity | |||
| Hypertension | 3170 (24.99%) | 2303 (27.10%) | 0.0229 |
| Diabetes mellitus | 1353 (10.67%) | 1186 (13.95%) | <0.001 |
| Hyperlipidemia | 1896 (14.95%) | 1254 (14.75%) | 0.6901 |
| Stroke | 662 (5.22%) | 712 (8.38%) | <0.001 |
| Allergic rhinitis | 1508 (11.89%) | 835 (9.82%) | <0.0001 |
| Pneumonia | 264 (2.08%) | 380 (4.47%) | <0.001 |
| Cancer | 444 (3.50%) | 525 (6.18%) | <0.001 |
| Depression | 2306 (18.18%) | 1462 (17.20%) | 0.0912 |
| Concurrent medication | |||
| NSAIDs Aspirins Statins | 3567 (28.12%) 5959 (46.98%) 4830 (38.08%) | 3723 (43.81%) 4086 (48.08%) 3639 (42.82%) | <0.001 0.0597 <0.001 |
| Beta- blockers | 2395 (18.88%) | 2506 (29.48%) | <0.001 |
| CCBs | 3119 (24.59%) | 3127 (36.79%) | <0.001 |
| ACEIs | 10,351 (8.16%) | 1315 (15.47%) | <0.001 |
| ARBs | 1853 (14.61%) | 2416 (28.43%) | <0.001 |
| H2RA n = 12,684 | PPI n = 8499 | |
|---|---|---|
| Follow up person months | 1,127,352 | 719,322 |
| Event of asthma | 1002 | 885 |
| Incidence rate * (95% C.I.) | 8.89 (7.32–10.78) | 12.31 (9.95–15.23) |
| Crude HR (95% C.I.) | Reference | 1.38 (1.01–1.86) |
| aHR (95% C.I.) | Reference | 1.41 (1.04–1.89) |
| Model | HR (95% CI) | p-Value |
|---|---|---|
| IPTW 1 | 1.40 (1.03–1.88) | 0.0109 |
| Propensity score matching | 1.37 (1.04–1.81) | 0.0019 |
| Incidence Rate of Asthma | |||
|---|---|---|---|
| H2RA | PPI | aHR (95% CI) | |
| Hypertension | p for interaction = 0.2992 | ||
| Without | 4.49 (4.07–4.95) | 4.13 (3.62–4.70) | 0.92 (0.78–1.10) |
| With | 8.49 (7.49–9.62) | 10.30 (8.97–11.84) | 1.21 (1.05–1.46) |
| Diabetes mellitus | p for interaction = 0.5962 | ||
| Without | 5.06 (4.64–5.50) | 4.94 (4.42–5.52) | 0.98 (0.83–1.14) |
| With | 8.84 (7.3–10.71) | 8.63 (6.87–10.84) | 0.98 (0.67–1.23) |
| Hyperlipidemia | p for interaction = 0.4678 | ||
| Without | 5.21 (4.79–5.66) | 4.95 (4.42–5.54) | 0.98 (0.85–1.13) |
| With | 7.25 (6.10–8.62) | 7.89 (6.36–9.78) | 1.09 (0.82–1.44) |
| Stroke | p for interaction = 0.5355 | ||
| Without | 5.17 (4.77–5.6) | 4.84 (4.34–5.39) | 0.94 (0.82–1.15) |
| With | 12.07 (9.45–15.42) | 13.43 (10.45–17.26) | 1.09 (0.76–1.57) |
| Allergic rhinitis | p for interaction = 0.9168 | ||
| Without | 5.02 (4.61–5.47) | 5.00 (4.48–5.57) | 1.00 (0.87–1.15) |
| With | 8.67 (7.28–10.33) | 8.79 (6.88–11.24) | 1.01 (0.74–1.33) |
| Pneumonia | p for interaction = 0.7532 | ||
| Without | 5.29 (4.88–5.71) | 5.08 (4.57–5.63) | 0.96 (0.83–1.11) |
| With | 14.21 (10.01–20.10) | 16.12 (11.4–22.8) | 0.95 (0.55–1.58) |
| Cancer | p for interaction = 0.1361 | ||
| Without | 5.41 (5.00–5.85) | 5.41 (4.89–5.99) | 1.02 (0.89–1.16) |
| With | 7.72 (5.22–11.36) | 4.70 (2.83–7.80) | 0.60 (0.30–1.21) |
| Depression | p for interaction = 0.4483 | ||
| Without | 5.11 (4.65–5.54) | 4.95 (4.42–5.55) | 0.97 (0.81–1.11) |
| With | 7.31 (6.25–8.55) | 7.44 (6.07–9.13) | 1.08 (0.84–1.41) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, T.-K.; Tsai, C.-F.; Huang, J.-Y.; Pan, L.-F.; Jong, G.-P. Exposure to Proton Pump Inhibitors and the Risk of Incident Asthma in Patients with Coronary Artery Diseases: A Population-Based Cohort Study. J. Pers. Med. 2022, 12, 824. https://doi.org/10.3390/jpm12050824
Lin T-K, Tsai C-F, Huang J-Y, Pan L-F, Jong G-P. Exposure to Proton Pump Inhibitors and the Risk of Incident Asthma in Patients with Coronary Artery Diseases: A Population-Based Cohort Study. Journal of Personalized Medicine. 2022; 12(5):824. https://doi.org/10.3390/jpm12050824
Chicago/Turabian StyleLin, Tsung-Kun, Chin-Feng Tsai, Jing-Yang Huang, Lung-Fa Pan, and Gwo-Ping Jong. 2022. "Exposure to Proton Pump Inhibitors and the Risk of Incident Asthma in Patients with Coronary Artery Diseases: A Population-Based Cohort Study" Journal of Personalized Medicine 12, no. 5: 824. https://doi.org/10.3390/jpm12050824
APA StyleLin, T. -K., Tsai, C. -F., Huang, J. -Y., Pan, L. -F., & Jong, G. -P. (2022). Exposure to Proton Pump Inhibitors and the Risk of Incident Asthma in Patients with Coronary Artery Diseases: A Population-Based Cohort Study. Journal of Personalized Medicine, 12(5), 824. https://doi.org/10.3390/jpm12050824