
Association of Serum 25-Hydroxyvitamin D Concentration with Breast Cancer Risk in Postmenopausal Women in the US



Abstract
:1. Introduction
2. Methods
2.1. Description of NHANES
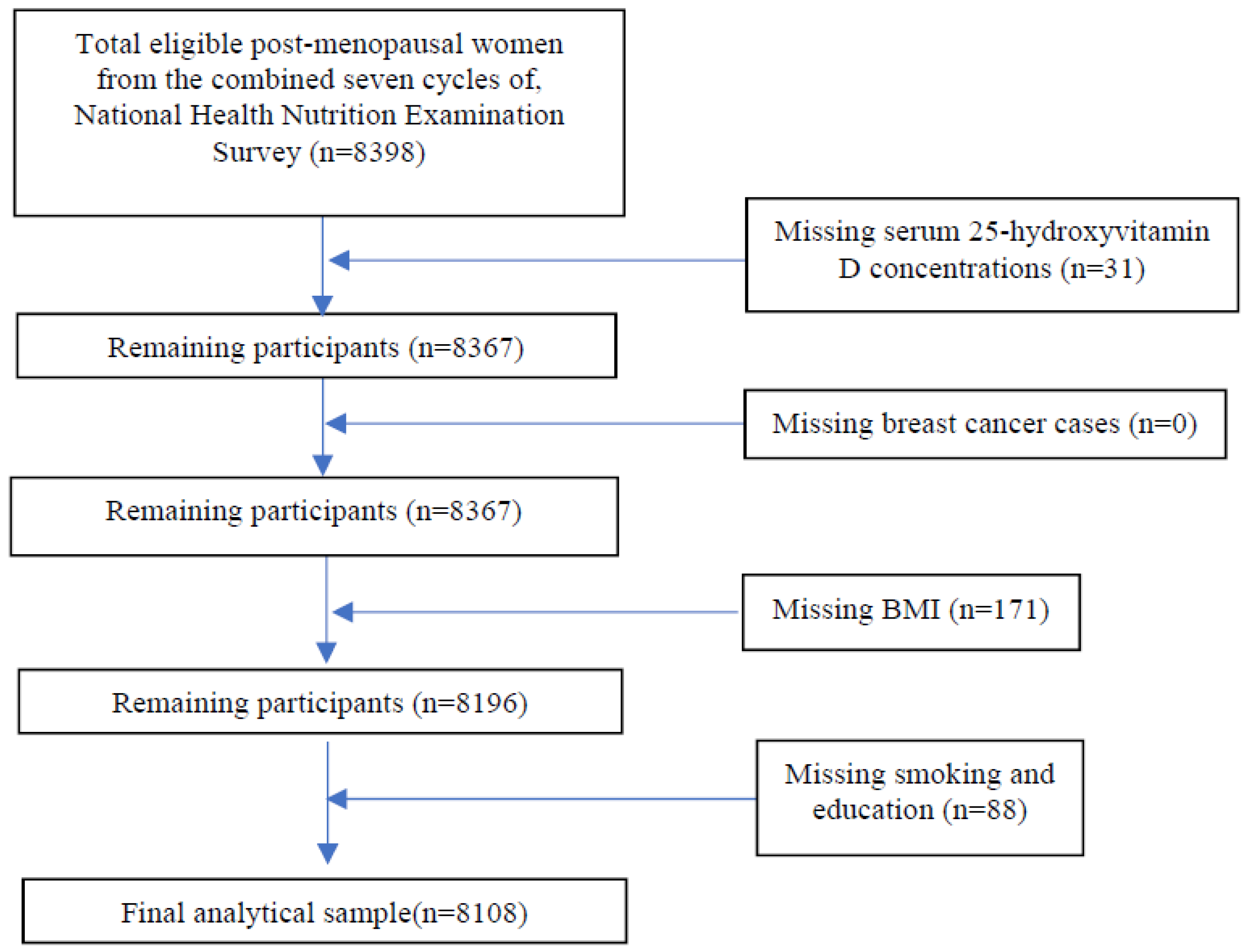
2.2. NHANES Study Design and Subject Selection
2.3. Measurement of Serum 25(OH)D Concentrations
2.4. Outcome Measure: Breast Cancer
2.5. Confounding Variables
2.6. Statistical Analyses
3. Results
3.1. Sample Derivation and Subject Characteristics
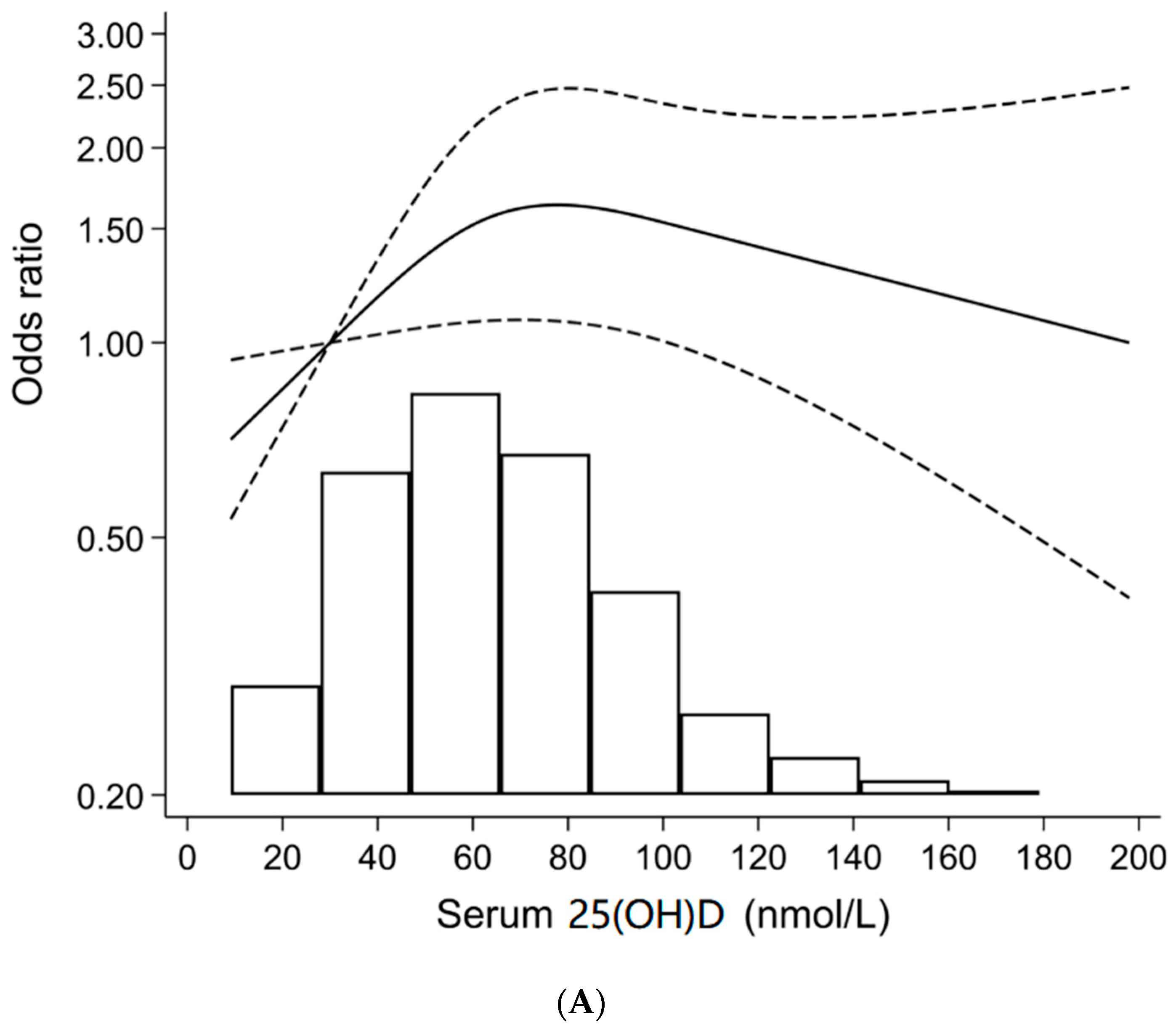
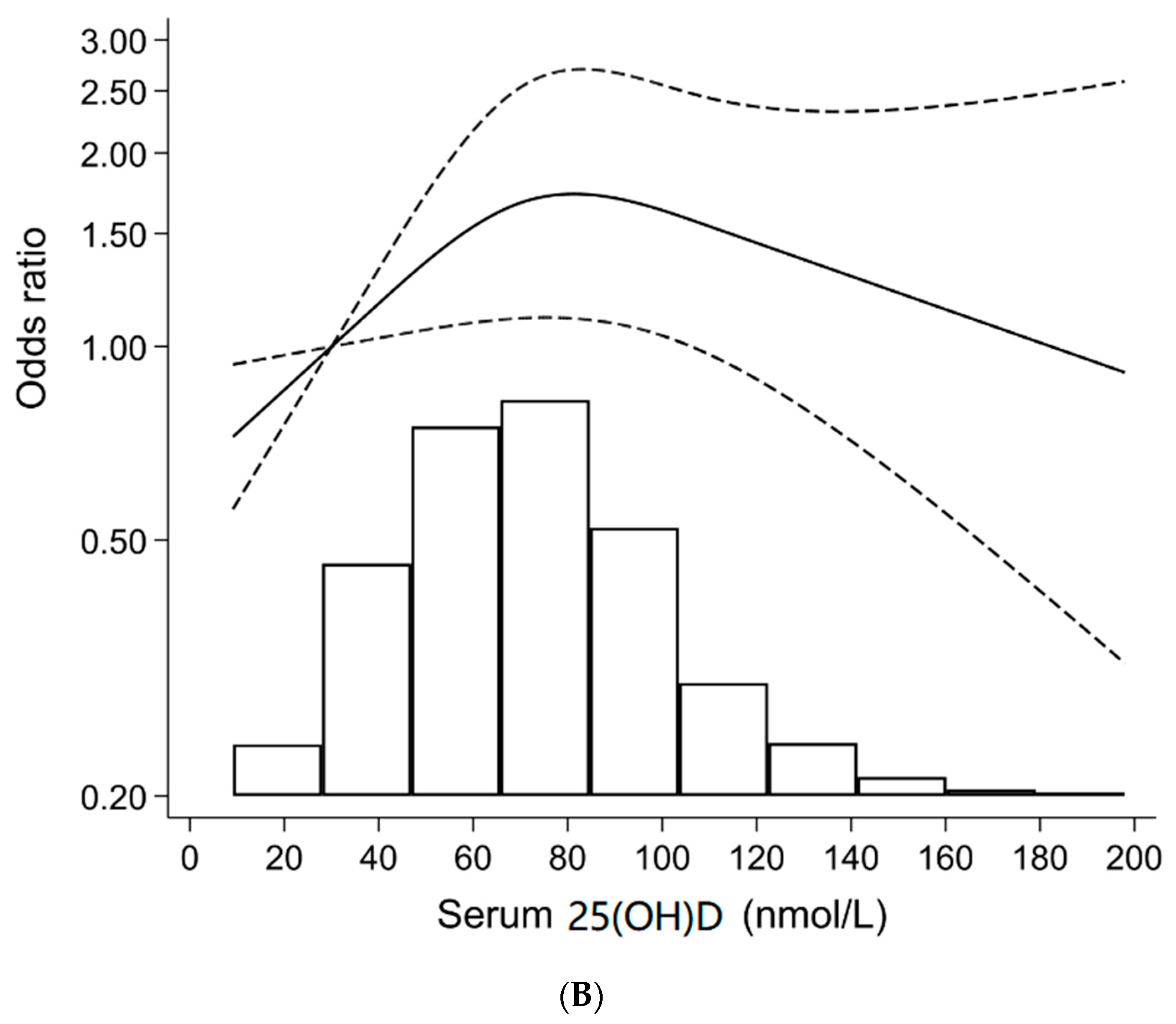
3.2. Association between Serum 25(OH)D Concentrations and Breast Cancer Prevalence
3.3. Association between Serum 25(OH)D Concentrations and Breast Cancer Prevalence by Race-Ethnicity, Supplement Use, and Season of Survey
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Reporting Guidelines
Abbreviations
| [1,25(OH)2D] | 1,25-dihydroxyvitamin D |
| CYP24A1 | 24-hydroxylase |
| [25(OH)D] | 25-hydroxyvitamin D |
| CYP27B1 | 25-hydroxyvitamin D 1-α hydroxylase |
| ES | Endocrine Society |
| HRT | hormone replacement therapy |
| IOM | Institute of Medicine |
| LC-TMS | Liquid Chromatography-Tandem Mass Spectrometry |
| MET | Metabolic Equivalent of Task |
| MA/H | Mexican American/Hispanic |
| MEC | Mobile Examination Centers |
| NHANES | National Health and Nutrition Examination Survey |
| NHB | non-Hispanic black |
| NCHS | National Center for Health Statistics |
| PIR | poverty income ratio |
| UV | Ultraviolet |
| US | United States |
| VDR | vitamin D receptors |
References
- Ganji, V.; Tangpricha, V.; Zhang, X. Serum Vitamin D Concentration >/=75 nmol/L Is Related to Decreased Cardiometabolic and Inflammatory Biomarkers, Metabolic Syndrome, and Diabetes; and Increased Cardiorespiratory Fitness in US Adults. Nutrients 2020, 12, 730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avestaei, A.H.; Yaghchiyan, M.; Ali-Hemmati, A.; Farhangi, M.A.; Mesgari-Abbasi, M.; Shahabi, P. Histological, metabolic, and inflammatory changes in the renal tissues of high-fat diet-induced obese rats after vitamin D supplementation. Nutr. Food Sci. 2020, 89, 143–151. [Google Scholar] [CrossRef]
- Ganji, V.; Milone, C.; Cody, M.M.; McCarty, F.; Wang, Y.T. Serum vitamin D concentrations are related to depression in young adult US population: The Third National Health and Nutrition Examination Survey. Int. Arch. Med. 2010, 3, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedirko, V.; Torres-Mejia, G.; Ortega-Olvera, C.; Biessy, C.; Angeles-Llerenas, A.; Lazcano-Ponce, E.; Saldana-Quiroz, V.A.; Romieu, I. Serum 25-hydroxyvitamin D and risk of breast cancer: Results of a large population-based case-control study in Mexican women. Cancer Causes Control 2012, 23, 1149–1162. [Google Scholar] [CrossRef]
- Wang, Q.; Ma, A.; Gao, T.; Liu, Y.; Ren, L.; Han, L.; Wei, B.; Liu, Q.; Dong, C.; Mu, Y.; et al. Poor Vitamin D Status in Active Pulmonary Tuberculosis Patients and Its Correlation with Leptin and TNF-alpha. J. Nutr. Sci. Vitam. 2019, 65, 390–398. [Google Scholar] [CrossRef] [Green Version]
- Farnik, H.; Bojunga, J.; Berger, A.; Allwinn, R.; Waidmann, O.; Kronenberger, B.; Keppler, O.T.; Zeuzem, S.; Sarrazin, C.; Lange, C.M. Low vitamin D serum concentration is associated with high levels of hepatitis B virus replication in chronically infected patients. Hepatology 2013, 58, 1270–1276. [Google Scholar] [CrossRef] [Green Version]
- Ganji, V.; Zhang, X.; Tangpricha, V. Serum 25-hydroxyvitamin D concentrations and prevalence estimates of hypovitaminosis D in the U.S. population based on assay-adjusted data. J. Nutr. 2012, 142, 498–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Looker, A.C.; Pfeiffer, C.M.; Lacher, D.A.; Schleicher, R.L.; Picciano, M.F.; Yetley, E.A. Serum 25-hydroxyvitamin D status of the US population: 1988–1994 compared with 2000–2004. Am. J. Clin. Nutr. 2008, 88, 1519–1527. [Google Scholar] [CrossRef]
- Agarwal, N.; Mithal, A.; Dhingra, V.; Kaur, P.; Godbole, M.M.; Shukla, M. Effect of two different doses of oral cholecalciferol supplementation on serum 25-hydroxy-vitamin D levels in healthy Indian postmenopausal women: A randomized controlled trial. Indian J. Endocrinol. Metab. 2013, 17, 883–889. [Google Scholar] [CrossRef]
- Bruyere, O.; Slomian, J.; Beaudart, C.; Buckinx, F.; Cavalier, E.; Gillain, S.; Petermans, J.; Reginster, J.Y. Prevalence of vitamin D inadequacy in European women aged over 80 years. Arch. Gerontol. Geriatr. 2014, 59, 78–82. [Google Scholar] [CrossRef]
- Li, S.; Ou, Y.; Zhang, H.; Zhang, Z.; Zhou, H.; Liu, L.; Sheng, Z.; Liao, E. Vitamin D status and its relationship with body composition, bone mineral density and fracture risk in urban central south Chinese postmenopausal women. Ann. Nutr. Metab. 2014, 64, 13–19. [Google Scholar] [CrossRef]
- Chlebowski, R.T.; Johnson, K.C.; Lane, D.; Pettinger, M.; Kooperberg, C.L.; Wactawski-Wende, J.; Rohan, T.; O’Sullivan, M.J.; Yasmeen, S.; Hiatt, R.A.; et al. 25-hydroxyvitamin D concentration, vitamin D intake and joint symptoms in postmenopausal women. Maturitas 2011, 68, 73–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanwar, G.; Sharma, N.; Shekhawat, M.; Sharma, P.; Hada, R.; Chandel, C.S. Comparison of vitamin D Levels in pre and postmenopausal type 2 diabetic females. J. Dent. Med. Sci. 2015, 14, 70–73. [Google Scholar]
- World Health Organization. Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 7 June 2020).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Song, D.; Deng, Y.; Liu, K.; Zhou, L.; Li, N.; Zheng, Y.; Hao, Q.; Yang, S.; Wu, Y.; Zhai, Z.; et al. Vitamin D intake, blood vitamin D levels, and the risk of breast cancer: A dose-response meta-analysis of observational studies. Aging 2019, 11, 12708–12732. [Google Scholar] [CrossRef]
- Yousef, F.M.; Jacobs, E.T.; Kang, P.T.; Hakim, I.A.; Going, S.; Yousef, J.M.; Al-Raddadi, R.M.; Kumosani, T.A.; Thomson, C.A. Vitamin D status and breast cancer in Saudi Arabian women: Case-control study. Am. J. Clin. Nutr. 2013, 98, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Vrieling, A.; Hein, R.; Abbas, S.; Schneeweiss, A.; Flesch-Janys, D.; Chang-Claude, J. Serum 25-hydroxyvitamin D and postmenopausal breast cancer survival: A prospective patient cohort study. Breast Cancer Res. 2011, 13, R74. [Google Scholar] [CrossRef] [Green Version]
- Abbas, S.; Linseisen, J.; Slanger, T.; Kropp, S.; Mutschelknauss, E.J.; Flesch-Janys, D.; Chang-Claude, J. Serum 25-hydroxyvitamin D and risk of post-menopausal breast cancer--results of a large case-control study. Carcinogenesis 2008, 29, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Cheney, C.P.; Thorand, B.; Huth, C.; Berger, K.; Peters, A.; Seifert-Klauss, V.; Kiechle, M.; Strauch, K.; Quante, A.S. The Association between Serum 25-Hydroxyvitamin D and Cancer Risk: Results from the Prospective KORA F4 Study. Oncol. Res. Treat. 2018, 41, 117–121. [Google Scholar] [CrossRef]
- Cheng, T.D.; Song, X.; Beresford, S.A.A.; Ho, G.Y.F.; Johnson, K.C.; Datta, M.; Chlebowski, R.T.; Wactawski-Wende, J.; Qi, L.; Neuhouser, M.L. Serum 25-hydroxyvitamin D concentrations and lung cancer risk in never-smoking postmenopausal women. Cancer Causes Control 2017, 28, 1053–1063. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. About the National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 19 June 2020).
- Centers for Disease Control and Prevention. NCHS Research Ethics Review Board (ERB) Approval. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 19 June 2020).
- Phipps, A.I.; Ichikawa, L.; Bowles, E.J.; Carney, P.A.; Kerlikowske, K.; Miglioretti, D.L.; Buist, D.S. Defining menopausal status in epidemiologic studies: A comparison of multiple approaches and their effects on breast cancer rates. Maturitas 2010, 67, 60–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. NHANES 2007–2008 Procedure Manuals. Available online: https://wwwn.cdc.gov/nchs/nhanes/ContinuousNhanes/manuals.aspx?BeginYear=2007 (accessed on 19 June 2020).
- Centers for Disease Control and Prevention. NHANES 2009–2010 Procedure Manuals. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/continuousnhanes/manuals.aspx?BeginYear=2009 (accessed on 19 June 2020).
- Centers for Disease Control and Prevention. NHANES 2011–2012 Procedure Manuals. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/manuals.aspx?BeginYear=2011 (accessed on 19 June 2020).
- Centers for Disease Control and Prevention. NHANES 2013–2014 Procedure Manuals. Available online: https://wwwn.cdc.gov/nchs/nhanes/ContinuousNhanes/Manuals.aspx?BeginYear=2013 (accessed on 19 June 2020).
- Centers for Disease Control and Prevention. Analytical Note for 25-Hydroxyvitamin D Data Analysis Using NHANES III (1988–1994), NHANES 2001–2006, and NHANES 2007–2010 (October 2015). Available online: https://wwwn.cdc.gov/nchs/nhanes/VitaminD/AnalyticalNote.aspx (accessed on 19 June 2020).
- Magro, G.; Salvatorelli, L.; Puzzo, L.; Piombino, E.; Bartoloni, G.; Broggi, G.; Vecchio, G.M. Practical approach to diagnosis of bland-looking spindle cell lesions of the breast. Pathologica. 2019, 111, 344–360. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Committee to Review Dietary Reference Intakes for calcium and Vitamin, D. The National Academies Collection: Reports funded by National Institutes of Health. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academy of Sciences: Washington, DC, USA, 2011. [Google Scholar]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Ordonez-Mena, J.M.; Schottker, B.; Fedirko, V.; Jenab, M.; Olsen, A.; Halkjaer, J.; Kampman, E.; de Groot, L.; Jansen, E.; Bueno-de-Mesquita, H.B.; et al. Pre-diagnostic vitamin D concentrations and cancer risks in older individuals: An analysis of cohorts participating in the CHANCES consortium. Eur. J. Epidemiol. 2016, 31, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Ordonez-Mena, J.M.; Schottker, B.; Haug, U.; Muller, H.; Kohrle, J.; Schomburg, L.; Holleczek, B.; Brenner, H. Serum 25-hydroxyvitamin d and cancer risk in older adults: Results from a large German prospective cohort study. Cancer Epidemiol. Biomark. Prev. 2013, 22, 905–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, M.L.; Stevens, V.L.; Patel, R.; Jacobs, E.J.; Bain, E.B.; Horst, R.L.; Gapstur, S.M.; Thun, M.J.; Calle, E.E. Serum 25-hydroxyvitamin D concentrations and postmenopausal breast cancer risk: A nested case control study in the Cancer Prevention Study-II Nutrition Cohort. Breast Cancer Res. 2009, 11, R64. [Google Scholar] [CrossRef] [Green Version]
- Freedman, D.M.; Chang, S.C.; Falk, R.T.; Purdue, M.P.; Huang, W.Y.; McCarty, C.A.; Hollis, B.W.; Graubard, B.I.; Berg, C.D.; Ziegler, R.G. Serum levels of vitamin D metabolites and breast cancer risk in the prostate, lung, colorectal, and ovarian cancer screening trial. Cancer Epidemiol. Biomark. Prev. 2008, 17, 889–894. [Google Scholar] [CrossRef] [Green Version]
- Eliassen, A.H.; Spiegelman, D.; Hollis, B.W.; Horst, R.L.; Willett, W.C.; Hankinson, S.E. Plasma 25-hydroxyvitamin D and risk of breast cancer in the Nurses’ Health Study II. Breast Cancer Res. 2011, 13, R50. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Eliassen, A.H.; Spiegelman, D.; Willett, W.C.; Hankinson, S.E. Plasma free 25-hydroxyvitamin D, vitamin D binding protein, and risk of breast cancer in the Nurses’ Health Study II. Cancer Causes Control 2014, 25, 819–827. [Google Scholar] [CrossRef] [Green Version]
- Amir, E.; Cecchini, R.S.; Ganz, P.A.; Costantino, J.P.; Beddows, S.; Hood, N.; Goodwin, P.J. 25-Hydroxy vitamin-D, obesity, and associated variables as predictors of breast cancer risk and tamoxifen benefit in NSABP-P1. Breast Cancer Res. Treat. 2012, 133, 1077–1088. [Google Scholar] [CrossRef] [Green Version]
- Scarmo, S.; Afanasyeva, Y.; Lenner, P.; Koenig, K.L.; Horst, R.L.; Clendenen, T.V.; Arslan, A.A.; Chen, Y.; Hallmans, G.; Lundin, E.; et al. Circulating levels of 25-hydroxyvitamin D and risk of breast cancer: A nested case-control study. Breast Cancer Res. 2013, 15, R15. [Google Scholar] [CrossRef] [PubMed]
- Bauer, S.R.; Hankinson, S.E.; Bertone-Johnson, E.R.; Ding, E.L. Plasma vitamin D levels, menopause, and risk of breast cancer: Dose-response meta-analysis of prospective studies. Medicine 2013, 92, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamshidinaeini, Y.; Akbari, M.E.; Abdollahi, M.; Ajami, M.; Davoodi, S.H. Vitamin D Status and Risk of Breast Cancer in Iranian Women: A Case-Control Study. J. Am. Coll. Nutr. 2016, 35, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Green, A.K.; Hankinson, S.E.; Bertone-Johnson, E.R.; Tamimi, R.M. Mammographic density, plasma vitamin D levels and risk of breast cancer in postmenopausal women. Int. J. Cancer 2010, 127, 667–674. [Google Scholar] [CrossRef]
- Forrest, K.Y.; Stuhldreher, W.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef]
- Chesney, R.W.; Rosen, J.F.; Hamstra, A.J.; Smith, C.; Mahaffey, K.; DeLuca, H.F. Absence of seasonal variation in serum concentrations of 1,25-dihydroxyvitamin D despite a rise in 25-hydroxyvitamin D in summer. J. Clin. Endocrinol. Metab. 1981, 53, 139–142. [Google Scholar] [CrossRef]
- Giammanco, M.; Di Majo, D.; La Guardia, M.; Aiello, S.; Crescimannno, M.; Flandina, C.; Tumminello, F.M.; Leto, G. Vitamin D in cancer chemoprevention. Pharm. Biol. 2015, 53, 1399–1434. [Google Scholar] [CrossRef] [Green Version]
- Wilson, E.N.; Bristol, M.L.; Di, X.; Maltese, W.A.; Koterba, K.; Beckman, M.J.; Gewirtz, D.A. A switch between cytoprotective and cytotoxic autophagy in the radiosensitization of breast tumor cells by chloroquine and vitamin D. Horm. Cancer 2011, 2, 272–285. [Google Scholar] [CrossRef] [Green Version]
- Fleet, J.C.; DeSmet, M.; Johnson, R.; Li, Y. Vitamin D and cancer: A review of molecular mechanisms. Biochem. J. 2012, 441, 61–76. [Google Scholar] [CrossRef] [Green Version]
- Stambolsky, P.; Tabach, Y.; Fontemaggi, G.; Weisz, L.; Maor-Aloni, R.; Siegfried, Z.; Shiff, I.; Kogan, I.; Shay, M.; Kalo, E.; et al. Modulation of the vitamin D3 response by cancer-associated mutant p53. Cancer Cell 2010, 17, 273–285. [Google Scholar] [CrossRef] [Green Version]
- Brozyna, A.A.; Jozwicki, W.; Jochymski, C.; Slominski, A.T. Decreased expression of CYP27B1 correlates with the increased aggressiveness of ovarian carcinomas. Oncol. Rep. 2015, 33, 599–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, N.; Sousa, B.; Martins, D.; Gomes, M.; Vieira, D.; Veronese, L.A.; Milanezi, F.; Paredes, J.; Costa, J.L.; Schmitt, F. Alterations in Vitamin D signalling and metabolic pathways in breast cancer progression: A study of VDR, CYP27B1 and CYP24A1 expression in benign and malignant breast lesions. BMC Cancer 2010, 10, 483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albertson, D.G.; Ylstra, B.; Segraves, R.; Collins, C.; Dairkee, S.H.; Kowbel, D.; Kuo, W.L.; Gray, J.W.; Pinkel, D. Quantitative mapping of amplicon structure by array CGH identifies CYP24 as a candidate oncogene. Nat Genet 2000, 25, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Townsend, K.; Banwell, C.M.; Guy, M.; Colston, K.W.; Mansi, J.L.; Stewart, P.M.; Campbell, M.J.; Hewison, M. Autocrine metabolism of vitamin D in normal and malignant breast tissue. Clin. Cancer Res. 2005, 11, 3579–3586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voutsadakis, I.A. Vitamin D baseline levels at diagnosis of breast cancer: A systematic review and meta-analysis. Hematol. Oncol. Stem Cell Ther. 2021, 14, 16–26. [Google Scholar] [CrossRef]
- Huss, L.; Butt, S.; Borgquist, S.; Almquist, M.; Malm, J.; Manjer, J. Serum levels of vitamin D, parathyroid hormone and calcium in relation to survival following breast cancer. Cancer Causes Control 2014, 25, 1131–1140. [Google Scholar] [CrossRef] [Green Version]
- Friedrich, M.; Axt-Fliedner, R.; Villena-Heinsen, C.; Tilgen, W.; Schmidt, W.; Reichrath, J. Analysis of vitamin D-receptor (VDR) and retinoid X-receptor alpha in breast cancer. Histochem. J. 2002, 34, 35–40. [Google Scholar] [CrossRef]
- Huss, L.; Butt, S.T.; Borgquist, S.; Elebro, K.; Sandsveden, M.; Rosendahl, A.; Manjer, J. Vitamin D receptor expression in invasive breast tumors and breast cancer survival. Breast Cancer Res. 2019, 21, 84. [Google Scholar] [CrossRef]
- Broggi, G.; Filetti, V.; Ieni, A.; Rapisarda, V.; Ledda, C.; Vitale, E.; Varricchio, S.; Russo, D.; Lombardo, C.; Tuccari, G.; et al. MacroH2A1 Immunoexpression in Breast Cancer. Front. Oncol. 2020, 10, 1519. [Google Scholar] [CrossRef]
- Kim, H.J.; Koh, B.S.; Yu, J.H.; Lee, J.W.; Son, B.H.; Kim, S.B.; Ahn, S.H. Changes in serum hydroxyvitamin D levels of breast cancer patients during tamoxifen treatment or chemotherapy in premenopausal breast cancer patients. Eur. J. Cancer 2014, 50, 1403–1411. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Serum 25(OH)D Concentrations 2 | ||||||
|---|---|---|---|---|---|---|
| <30 nmol/L | 30–<50 nmol/L | 50–<75 nmol/L | 75–<100 nmol/L | ≥100 nmol/L | p-Value 3 | |
| (n = 697) | (n = 1931) | (n = 2778) | (n = 1822) | (n = 880) | ||
| Serum 25(OH)D, nmol/L | 23.6 (4.6) | 40.4 (5.8) | 62.1 (7) | 85.8 (7.1) | 122.2 (22.8) | <0.001 |
| Age, y | 61.4 (12.5) | 62.1 (12.9) | 63 (12.9) | 64.1 (12.6) | 65.8 (12.4) | <0.001 |
| Race-ethnicity | <0.001 | |||||
| Non-Hispanic white, n (%) | 189 (27.1) | 744 (38.5) | 1496 (53.9) | 1223 (67.1) | 649 (73.8) | |
| Non-Hispanic black, n (%) | 327 (46.9) | 553 (28.6) | 417 (15) | 204 (11.2) | 98 (11.1) | |
| Mexican American/Hispanic, n (%) | 114 (16.4) | 389 (20.1) | 459 (16.5) | 159 (8.7) | 30 (3.4) | |
| Others, n (%) 4 | 67 (9.6) | 245 (12.7) | 406 (14.6) | 236 (13) | 103 (11.7) | |
| Smoking status | <0.001 | |||||
| Never, n (%) | 329 (47.2) | 1148 (59.5) | 1690 (60.8) | 1080 (59.3) | 514 (58.4) | |
| Former, n (%) | 176 (25.3) | 449 (23.3) | 695 (25) | 530 (29.1) | 263 (29.9) | |
| Current, n (%) | 192 (27.5) | 334 (17.3) | 393 (14.1) | 212 (11.6) | 103 (11.7) | |
| Alcohol drinking 5 | <0.001 | |||||
| No, n (%) | 216 (31) | 524 (27.1) | 687 (24.7) | 394 (21.6) | 191 (21.7) | |
| Yes, n (%) | 312 (44.8) | 883 (45.7) | 1405 (50.6) | 1033 (56.7) | 503 (57.2) | |
| Not reported, n (%) | 169 (24.2) | 524 (27.1) | 686 (24.7) | 395 (21.7) | 186 (21.1) | |
| Season of survey | <0.001 | |||||
| Winter, n (%) | 406 (58.2) | 1027 (53.2) | 1219 (43.9) | 691 (37.9) | 321 (36.5) | |
| Summer, n (%) | 291 (41.8) | 904 (46.8) | 1559 (56.1) | 1131 (62.1) | 559 (63.5) | |
| Body mass index, kg/m2 | 32.6 (8.3) | 31.2 (7.2) | 29.4 (6.7) | 28.4 (6.8) | 27.3 (5.9) | <0.001 |
| Physical activity (METs/week) 6 | <0.001 | |||||
| <600 (low), n (%) | 488 (70) | 1210 (62.7) | 1512 (54.4) | 891 (48.9) | 428 (48.6) | |
| 600–1199 (moderate), n (%) | 65 (9.3) | 229 (11.9) | 385 (13.9) | 256 (14.1) | 124 (14.1) | |
| ≥1200 (vigorous), n (%) | 144 (20.7) | 492 (25.5) | 881 (31.7) | 675 (37) | 328 (37.3) | |
| Poverty Income Ratio 7 | <0.001 | |||||
| <1.30 (low income), n (%) | 254 (36.4) | 621 (32.2) | 799 (28.8) | 429 (23.5) | 169 (19.2) | |
| 1.3–3.5 (moderate income), n (%) | 245 (35.2) | 728 (37.7) | 1034 (37.2) | 607 (33.3) | 326 (37) | |
| >3.5 (high income), n (%) | 132 (18.9) | 420 (21.8) | 730 (26.3) | 644 (35.3) | 324 (36.8) | |
| Not reported, n (%) | 66 (9.5) | 162 (8.4) | 215 (7.7) | 142 (7.8) | 61 (6.9) | |
| Education | <0.001 | |||||
| <11 grade, n (%) | 274 (39.3) | 681 (35.3) | 891 (32.1) | 399 (21.9) | 156 (17.7) | |
| High school, n (%) | 165 (23.7) | 482 (25) | 682 (24.6) | 509 (27.9) | 229 (26) | |
| Some college, n (%) | 179 (25.7) | 521 (27) | 748 (26.9) | 534 (29.3) | 255 (29) | |
| Higher than College, n (%) | 79 (11.3) | 247 (12.8) | 457 (16.5) | 380 (20.9) | 240 (27.3) | |
| Hormone replacement therapy, n (%) 8 | 106 (15.2) | 339 (17.6) | 582 (21) | 291 (16) | 63 (7.2) | <0.001 |
| Supplements intake 9 | <0.001 | |||||
| Yes, n (%) | 200 (28.7) | 861 (44.5) | 1902 (68.5) | 1488 (81.7) | 790 (89.8) | |
| No, n (%) | 497 (71.3) | 1070 (55.5) | 875 (31.5) | 334 (18.3) | 90 (10.2) | |
| Serum 25(OH)D Concentrations 2 | ||||||
|---|---|---|---|---|---|---|
| <30 nmol/L 3 (n = 697) | 30–<50 nmol/L (n = 1931) | 50–<75 nmol/L (n = 2778) | 75–<100 nmol/L (n = 1822) | ≥100 nmol/L (n = 880) | p for Trend 4 | |
| Breast cancer cases, n (%) | 23 (3.3) | 77 (4) | 128 (4.6) | 117 (6.4) | 61 (6.9) | <0.001 |
| Unadjusted | 1 | 1.7 (0.98–3) | 2 (1.2–3.4) 5 | 2.7 (1.6–4.5) 5 | 2.4 (1.4–4.2) 5 | <0.001 |
| Age-adjusted | 1 | 1.7 (0.95–2.9) | 1.9 (1.1–3.3) 5 | 2.5 (1.5–4.2) 5 | 2 (1.2–3.6) 5 | 0.005 |
| Race-ethnicity-adjusted | 1 | 1.7 (0.94–2.9) | 1.8 (1.1–3.1) 5 | 2.4 (1.4–4) 5 | 2.1 (1.2–3.7) 5 | 0.007 |
| Multivariate-adjusted 6 | 1 | 1.7 (0.9–3) | 1.9 (1.05–3.3) 5 | 2.4 (1.4–4.2) 5 | 1.94 (1.03–3.6) 5 | 0.031 |
| Serum 25(OH) D Concentrations 2 | ||||||
|---|---|---|---|---|---|---|
| <30 nmol/L 3 | 30–<50 nmol/L | 50–<75 nmol/L | 75–<100 nmol/L | ≥100 nmol/L | p for Trend 4 | |
| Non-Hispanic white (n = 4301) | ||||||
| Unadjusted | 1 | 3 (1.1–7.4) 5 | 3 (1.1–7.4) 5 | 3.7 (1.5–9.1) 5 | 3 (1.2–7.8) 5 | 0.049 |
| Age-adjusted | 1 | 3 (1.1–7.5) 5 | 3 (1.2–7.4) 5 | 3.8 (1.6–9.3) 5 | 3 (1.1–7.3) 5 | 0.1 |
| Multivariate-adjusted 6 | 1 | 3 (1.14–8) 5 | 3.14 (1.2–8.3) 5 | 4.1 (1.6–11) 5 | 3.2 (1.15–8.7) 5 | 0.07 |
| Non-Hispanic black (n = 1599) | ||||||
| Unadjusted | 1 | 0.6 (0.3–1.3) | 0.6 (0.3–1.4) | 1.6 (0.6–4.2) | 2.2 (0.8–6) | 0.11 |
| Age-adjusted | 1 | 0.6 (0.3–1.3) | 0.6 (0.2–1.3) | 1.3 (0.5–3.5) | 1.7 (0.6–4.9) | 0.23 |
| Multivariate-adjusted 6 | 1 | 0.6 (0.3–1.3) | 0.56 (0.25–1.3) | 1.4 (0.53–3.8) | 1.8 (0.6–5.3) | 0.25 |
| Mexican American/Hispanic (n = 1151) | ||||||
| Unadjusted | 1 | 3 (0.5–18) | 2.6 (0.3–22) | 0.8 (0.1–8.2) | 2.2 (0.1–35) | 0.56 |
| Age-adjusted | 1 | 3 (0.5–18) | 2.6 (0.3–22) | 0.7 (0.1–8.1) | 2.1 (0.1–36) | 0.53 |
| Multivariate-adjusted 6 | 1 | 2 (0.33–12) | 2 (0.3–12) | 0.5 (0.04–6) | 1.2 (0.1–25) | 0.35 |
| Demographic Characteristic | Serum 25 (OH)D Concentrations 2 | |||||
|---|---|---|---|---|---|---|
| <30 nmol/L 3 | 30–˂50 nmol/L | 50–˂75 nmol/L | 75–˂100 nmol/L | ≥100 nmol/L | p for Interaction 4 | |
| OR | OR (95%CI) | OR (95%CI) | OR (95%CI) | OR (95%CI) | ||
| Supplement use | 0.95 | |||||
| Yes | 1 | 2.1 (0.7–6) | 2.3 (0.8–7) | 3 (1.1–8) | 2.5 (0.8–7) | |
| No | 1 | 1.4 (0.7–3) | 1.5 (0.6–3.6) | 2.1 (0.99–5) | 1.3 (0.4–4.4) | |
| Season of survey | 0.59 | |||||
| Winter | 1 | 2.3 (0.9–8-5) | 2.7 (1.1–7) | 3.1 (1.4–7) | 2.4 (0.85–7) | |
| Summer | 1 | 1.3 (0.6–3) | 1.3 (0.6–3) | 1.8 (0.8–4) | 1.4 (0.6–3.3) | |
| Race-ethnicity | 0.12 | |||||
| Non-Hispanic white | 1 | 3 (1.1–8) | 2.9 (1.1–8) | 3.7 (1.4–10) | 2.9 (0.99–8) | |
| Non-Hispanic black | 1 | 0.6 (0.3–1.4) | 0.6 (0.3–1.4) | 1.5 (0.6–4) | 2 (0.6–6) | |
| Mexican American/Hispanic | 1 | 2 (0.3–11) | 1.8 (0.3–10) | 0.4 (0.04–5) | 1.1 (0.1–21) | |
| Others | 1 | 1.1 (0.1–13) | 3 (0.3–32) | 2.6 (0.3–26) | 2.8 (0.3–28) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ganji, V.; Sukik, L.; Hoque, B.; Boutefnouchet, L.; Shi, Z. Association of Serum 25-Hydroxyvitamin D Concentration with Breast Cancer Risk in Postmenopausal Women in the US. J. Pers. Med. 2022, 12, 944. https://doi.org/10.3390/jpm12060944
Ganji V, Sukik L, Hoque B, Boutefnouchet L, Shi Z. Association of Serum 25-Hydroxyvitamin D Concentration with Breast Cancer Risk in Postmenopausal Women in the US. Journal of Personalized Medicine. 2022; 12(6):944. https://doi.org/10.3390/jpm12060944
Chicago/Turabian StyleGanji, Vijay, Layan Sukik, Bushra Hoque, Linda Boutefnouchet, and Zumin Shi. 2022. "Association of Serum 25-Hydroxyvitamin D Concentration with Breast Cancer Risk in Postmenopausal Women in the US" Journal of Personalized Medicine 12, no. 6: 944. https://doi.org/10.3390/jpm12060944
APA StyleGanji, V., Sukik, L., Hoque, B., Boutefnouchet, L., & Shi, Z. (2022). Association of Serum 25-Hydroxyvitamin D Concentration with Breast Cancer Risk in Postmenopausal Women in the US. Journal of Personalized Medicine, 12(6), 944. https://doi.org/10.3390/jpm12060944