
The Role of Allergen-Specific Immunotherapy in ENT Diseases: A Systematic Review

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
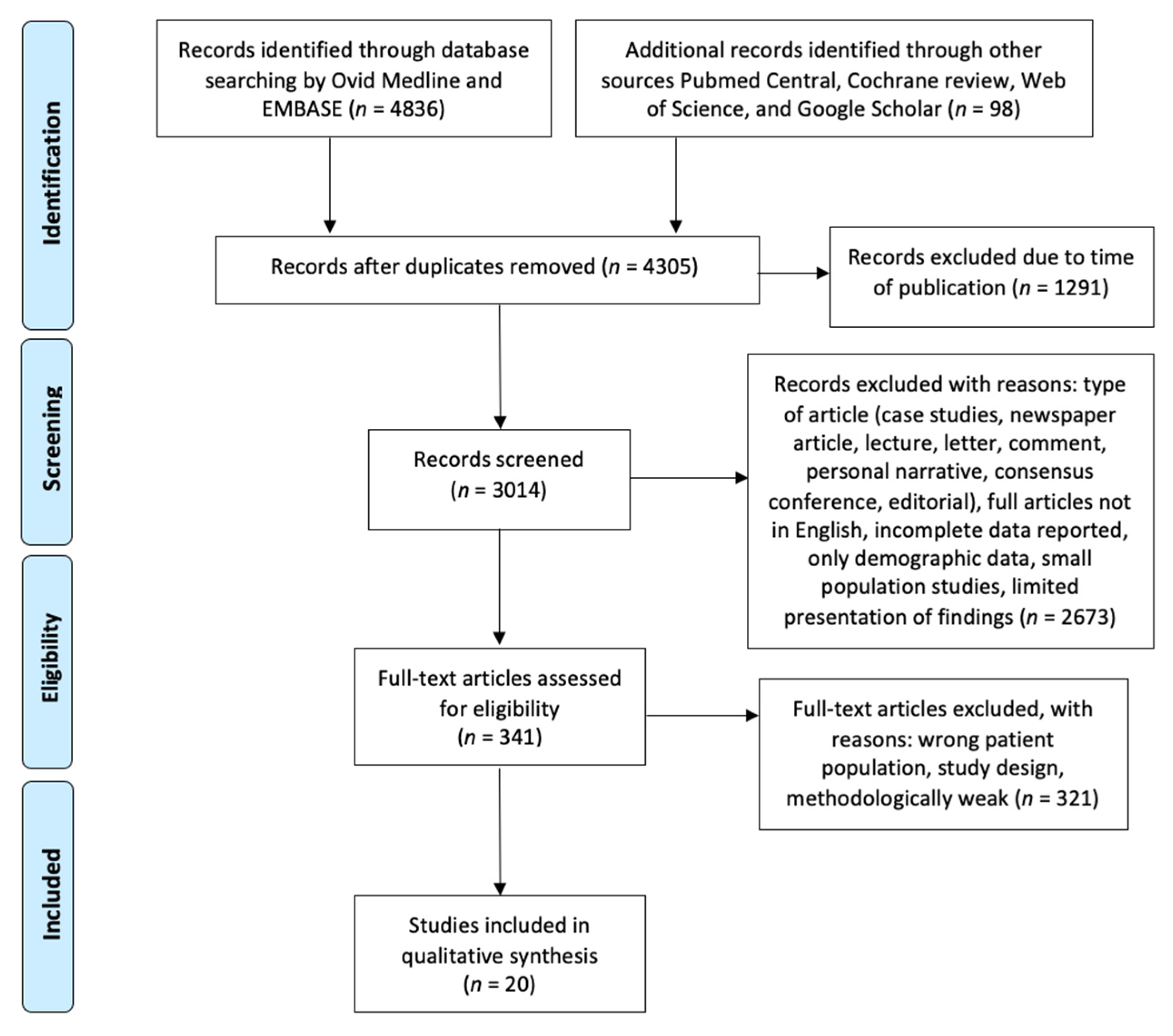
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
3. Results and Discussion
3.1. Efficacy of Allergen-Specific Immunotherapy in the Treatment of Local Allergic Rhinitis
3.2. Efficacy of Allergen-Specific Immunotherapy in Acute and Chronic Rhinosinusitis
3.2.1. Efficacy of Allergen-Specific Immunotherapy in Acute Rhinosinusitis
3.2.2. Efficacy of Allergen-Specific Immunotherapy in Chronic Rhinosinusitis

{kind=link}
| Authors (Years) | Type of Study | Patients (n) | Methods | Duration of AIT Therapy | Duration of FUP | Mean Outcomes Measured | Results | Conclusions | Y/N |
|---|---|---|---|---|---|---|---|---|---|
| Nishioka et al., 1994 [77] | Prospective study | 72 CRS with allergy, post-surgery | Not specified | 14.9 months (range 0.75–44.3 months) | Effect of AIT on middle meatotomy patency, synechiae formation, and recurrent polyps in allergic patients | AIT given either before or after surgery does not statistically influence middle meatotomy patency, synechiae formation, or recurrence of polyps after FESS | AIT does not influence the outcomes measured | N | |
| Schlenter et al., 1983 [78] | Prospective study | 65 post-surgery | N/A | N/A | Symptoms and radiographic scores | AIT group had less severe symptoms score and greater improvements of radiographic score | The treatment of allergic sinusitis with hyposensitization offers a better prognosis in the long run | Y | |
| Asakura et al., 1990 [79] | Prospective study | 52 children with CRS (no prior surgery) | Children were treated with either the combination of antigen specific immunotherapy and medication with lysozyme chloride preparation or medication alone | 2–3 months | N/A | Scoring system of individual symptoms (sneezing, rhinorrhea, nasal obstruction, overall symptoms), objective signs (hypertrophy of turbinates, amount of nasal secretions), radiographic findings (XP shadow of maxillary sinus) | Symptoms and radiographic improvements were significantly better in AIT group | The addition of AIT can improve patients’ symptoms and radiographic outcomes | Y |
| Nathan et al., 2004 [80] | Retrospective case series | 114 | Patients were surveyed twice, with the first a recall of symptoms before starting immunotherapy and the second an evaluation of current symptoms | 3.3 years (mean), at least 12 months | N/A | Sinusitis Outcomes Questionnaire | Mean reduction of 51% in the overall symptom score of the patients after receiving immunotherapy and 54% fewer surgeries | Immunotherapy is an effective treatment for patients with sinus disease and AR | Y |
| Li et al., 2021 [81] | Prospective study | 64 CRSwNP with AR post-surgery | Patients were divided into three treatment groups represented by standard medication alone; standard medication and nasal irrigations; standard medication, nasal irrigations and specific subcutaneous immunotherapy | >3 years | N/A | SNOT-22, TNSS, electron microscopy inflammatory mediators (ECP, IL-8, IFN- γ, IL-25, IL-33, and IL-17) | Clinical scoring improvement, more orderly arrangement of the cilia and lower expression levels of inflammatory mediators after 1 year follow up in IT group | The addition of AIT can improve patients’ symptoms and quality of life, promote the epithelialization of the mucosa in the surgical cavity and adjust the local immune response | Y |
| Steehler et al., 2021 [85] | Retrospective study | 132 CRSwNP subtypes post-surgery | Electronic records review of maintenance therapy for postoperative treatment, follow-up visits, pathology findings, CT imaging data, and outside records | Not specified | At least 12 months | Polyp recurrence, revision ESS, oral steroid use, oral antibiotic use | Polyp recurrence and ESS revision rates were significantly lower in CCAD than other CRSwNP subtypes in an additional AIT setting | Given the association of inhalant allergy with CCAD, AIT is a consideration in the treatment regimen for these patients | Y |
| Folker et al., 1998 [89] | Retrospective cohort study | 22 AFRS post-surgery | Study patients were treated with specific immunotherapy fungal antigens while control group received no immunotherapy | >24 months | 12–50 months (range) | CRS Survey, Kupferberg stage, corticosteroid use | AIT treated group achieved better results in all outcomes | Significant reduction in polyp reformation, corticosteroid requirements and improved quality of life in AFRS patients receiving additional AIT | Y |
| Bassichis et al., 2001 [90] | Retrospective cohort study | 60 AFRS post-surgery | Review of the database focusing on postoperative management (nasal irrigation, intranasal steroids, systemic steroids, antibiotics, immunotherapy, in-office procedures and repeat surgery) | Not specified | 48.5 months (mean) | Revision surgery, outpatient intervention | Less revision surgery (11% vs. 33%) and less clinic visits in the IT treated arm | Post-operative AIT with relevant fungal antigens is an important aspect of the treatment of AFS resulting in decrease re-operation rates and office visits requiring intervention | Y |
| Marple et al., 2002 [91] | Cross- sectional study of prospective protocol | 17 AFRS post-surgery | Outpatient records review of follow up, SNOT-20 quality-of-life survey, ongoing medical/surgical intervention and blood immunoglobulin levels | Not specified | 46–138 months (range) | Kupferberg stage, IgE levels, SNOT-20 in long term follow up | No significant difference in long-term outcomes was seen between those patients treated with fungus-specific IT and those treated with other methods | After successful initial treatment and control of AFRS, many patients can achieve a quiescent disease state | Y |
3.3. Efficacy of Allergen-Specific Immunotherapy in AT Diseases
3.4. Efficacy of Allergen-Specific Immunotherapy in Management of Otitis Media
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Noon, L. Prophylactic Inoculations Againsthay Fever. Lancet 1911, 1, 1572–1573. [Google Scholar] [CrossRef] [Green Version]
- Breiteneder, H.; Diamant, Z.; Eiwegger, T.; Fokkens, W.J.; Traidl-Hoffmann, C.; Nadeau, K.; O’Hehir, R.E.; O’Mahony, L.; Pfaar, O.; Torres, M.J. Future Research Trends in Understanding the Mechanisms Underlying Allergic Diseases for Improved Patient Care. Allergy 2019, 74, 2293–2311. [Google Scholar] [CrossRef] [PubMed]
- Sugita, K.; Steer, C.A.; Martinez-Gonzalez, I.; Altunbulakli, C.; Morita, H.; Castro-Giner, F.; Kubo, T.; Wawrzyniak, P.; Ruckert, B.; Sudo, K. Type 2 Innate Lymphoid Cells Disrupt Bronchial Epithelial Barrier Integrity by Targeting Tight Junctions through IL-13 in Asthmatic Patients. J. Allergy Clin. Immunol. 2018, 141, 300–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, A.; Hirahara, K.; Kiuchi, M.; Nakayama, T. Eosinophils: Cells Known for over 140 Years with Broad and New Functions. Allergol. Int. 2021, 70, 3–8. [Google Scholar] [CrossRef]
- Keegan, A.D.; Leonard, W.J.; Zhu, J. Recent Advances in Understanding the Role of IL-4 Signaling. Fac. Rev. 2021, 10, 71. [Google Scholar] [CrossRef]
- Ring, J.; Gutermuth, J. 100 Years of Hyposensitization: History of Allergen-Specific Immunotherapy ASIT. Allergy 2011, 66, 713–724. [Google Scholar] [CrossRef]
- Meadows, A.; Kaambwa, B.; Novielli, N.; Huissoon, A.; Fry-Smith, A.; Meads, C.; Barton, P.; Dretzke, J. A Systematic Review and Economic Evaluation of Subcutaneous and Sublingual Allergen Immunotherapy in Adults and Children with Seasonal Allergic Rhinitis. Health Technol. Assess. 2013, 17, 1–322. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.Y.; Erekosima, N.; Suarez-Cuervo, C.; Ramanathan, M.; Kim, J.M.; Ward, D.; Chelladurai, Y.; Segal, J.B. Allergen-Specific Immunotherapy for the Treatment of Allergic Rhinoconjunctivitis and/or Asthma. Comparative Effectiveness Review; Report No.: 13-EHC061-EF; Agency for Healthcare Research and Quality: Rockville, MD, USA, 3 May 2013.
- Pfaar, O.; Urry, Z.; Robinson, D.S.; Sager, A.; Richards, D.; Hawrylowicz, C.M.; Brautigam, M.; Klimek, L. A randomized placebo-controlled trial of rush preseasonal depigmented polymerized grass pollen immunotherapy. Allergy 2012, 67, 272–279. [Google Scholar] [CrossRef]
- Pfaar, O.; Biedermann, T.; Klimek, L.; Sager, A.; Robinson, D.S. Depigmented-Polymerized Mixed Grass/Birch Pollen Extract Immunotherapy Is Effective in Polysensitized Patients. Allergy 2013, 68, 1306–1313. [Google Scholar] [CrossRef]
- Klimek, L.; Uhlig, J.; Mosges, R.; Rettig, K.; Pfaar, O. A high polymerized grass pollen extract is efficacious and safe in a randomized double-blind, placebo-controlled study using a novel up-dosing cluster-protocol. Allergy 2014, 69, 1629–1638. [Google Scholar] [CrossRef]
- Bozek, A.; Kolodziejczyk, K.; Krajewska-Wojtys, A.; Jarzab, J. Pre-Seasonal, Subcutaneous Immunotherapy: A Double-Blinded, Placebo-Controlled Study in Elderly Patients with an Allergy to Grass. Ann. Allergy Asthma Immunol. 2016, 116, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Calderon, M.A.; Alves, B.; Jacobson, M.; Hurwitz, B.; Sheikh, A.; Durham, S. Allergen Injection Immunotherapy for Seasonal Allergic Rhinitis. Cochrane Database Syst. Rev. 2007, 2007, CD001936. [Google Scholar] [CrossRef] [PubMed]
- Moreno, V.; Alvarino, M.; Rodriguez, F.; Roger, A.; Pena-Arellano, M.I.; Lleonart, R.; Pagan, J.A.; Navarro, J.A.; Navarro, L.A.; Vidal, C. Randomized Dose-Response Study of Subcutaneous Immunotherapy with a Dermatophagoides Pteronyssinus Extract in Patients with Respiratory Allergy. Immunotherapy 2016, 8, 265–277. [Google Scholar] [CrossRef] [Green Version]
- Cox, L.; Nelson, H.; Lockey, R.; Calabria, C.; Chacko, T.; Finegold, I.; Nelson, M.; Weber, R.; Bernstein, D.I.; Blessing-Moore, J. Allergen Immunotherapy: A Practice Parameter Third Update. J. Allergy Clin. Immunol. 2011, 127, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Zuberbier, T.; Bachert, C.; Bousquet, P.J.; Passalacqua, G.; Walter Canonica, G.; Merk, H.; Worm, M.; Wahn, U.; Bousquet, J. GA(2)LEN/EAACI Pocket Guide for Allergen-Specific Immunotherapy for Allergic Rhinitis and Asthma. Allergy 2010, 65, 1525–1530. [Google Scholar] [CrossRef] [PubMed]
- Radulovic, S.; Calderon, M.A.; Wilson, D.; Durham, S. Sublingual Immunotherapy for Allergic Rhinitis. Cochrane Database Syst. Rev. 2010, 2010, CD002893. [Google Scholar] [CrossRef] [PubMed]
- Lou, H.; Huang, Y.; Ouyang, Y.; Zhang, Y.; Xi, L.; Chu, X.; Wang, Y.; Wang, C.; Zhang, L. Artemisia annua-sublingual immunotherapy for seasonal allergic rhinitis: A randomized controlled trial. Allergy 2020, 75, 2026–2036. [Google Scholar] [CrossRef]
- Meltzer, E.O.; Wallace, D.; Friedman, H.S.; Navaratnam, P.; Scott, E.P.; Nolte, H. Meta-Analyses of the Efficacy of Pharmacotherapies and Sublingual Allergy Immunotherapy Tablets for Allergic Rhinitis in Adults and Children. Rhinology 2021, 59, 422–432. [Google Scholar] [CrossRef]
- Pfaar, O.; Bachert, C.; Kuna, P.; Panzner, P.; Dzupinova, M.; Klimek, L.; Nimwegen, M.J.; Boot, J.D.; Yu, D.; Opstelten, D.J.E. Sublingual Allergen Immunotherapy with a Liquid Birch Pollen Product in Patients with Seasonal Allergic Rhinoconjunctivitis with or without Asthma. J. Allergy Clin. Immunol. 2019, 143, 970–977. [Google Scholar] [CrossRef] [Green Version]
- Bozek, A.; Ignasiak, B.; Filipowska, B.; Jarzab, J. House Dust Mite Sublingual Immunotherapy: A Double-Blind, Placebo-Controlled Study in Elderly Patients with Allergic Rhinitis. Clin. Exp. Allergy 2013, 43, 242–248. [Google Scholar] [CrossRef]
- Lin, Z.; Liu, Q.; Li, T.; Chen, D.; Chen, D.; Xu, R. The Effects of House Dust Mite Sublingual Immunotherapy in Patients with Allergic Rhinitis According to Duration. Int. Forum Allergy Rhinol. 2016, 6, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.E.; Choi, Y.S.; Kim, M.S.; Han, D.H.; Rhee, C.S.; Lee, C.H.; Kim, D.Y. Efficacy of Sublingual Immunotherapy with House Dust Mite Extract in Polyallergen Sensitized Patients with Allergic Rhinitis. Ann. Allergy Asthma Immunol. 2011, 107, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Didier, A.; Worm, M.; Horak, F.; Sussman, G.; Beaumont, O.; Le Gall, M.; Melac, M.; Malling, H.J. Sustained 3-Year Efficacy of Pre- and Coseasonal 5-Grass-Pollen Sublingual Immunotherapy Tablets in Patients with Grass Pollen-Induced Rhinoconjunctivitis. J. Allergy Clin. Immunol. 2011, 128, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Rienzo, V.D.; Minelli, M.; Musarra, A.; Sambugaro, R.; Pecora, S.; Canonica, W.G.; Passalacqua, G. Post-Marketing Survey on the Safety of Sublingual Immunotherapy in Children below the Age of 5 Years. Clin. Exp. Allergy 2005, 35, 560–564. [Google Scholar] [CrossRef]
- Yukselen, A.; Kendirli, S.G.; Yilmaz, M.; Altintas, D.U.; Karakoc, G.B. Effect of One-Year Subcutaneous and Sublingual Immunotherapy on Clinical and Laboratory Parameters in Children with Rhinitis and Asthma: A Randomized, Placebo-Controlled, Double-Blind, Double-Dummy Study. Int. Arch. Allergy Immunol. 2012, 157, 288–298. [Google Scholar] [CrossRef]
- Khinchi, M.S.; Poulsen, L.K.; Carat, F.; Andre, C.; Hansen, A.B.; Malling, H.J. Clinical Efficacy of Sublingual and Subcutaneous Birch Pollen Allergen-Specific Immunotherapy: A Randomized, Placebo-Controlled, Double-Blind, Double-Dummy Study. Allergy 2004, 59, 45–53. [Google Scholar] [CrossRef]
- Quirino, T.; Iemoli, E.; Siciliani, E.; Parmiani, S.; Milazzo, F. Sublingual versus Injective Immunotherapy in Grass Pollen Allergic Patients: A Double Blind (Double Dummy) Study. Clin. Exp. Allergy 1996, 26, 1253–1261. [Google Scholar] [CrossRef]
- Cavaliere, C.; Incorvaia, C.; Begvarfaj, E.; Orlando, M.P.; Turchetta, R.; Musacchio, A.; Ralli, M.; Ciofalo, A.; Greco, A.; Vincentiis, M. The Safety of Sublingual Immunotherapy, Can the Rare Systemic Reactions Be Prevented? Exp. Opin. Drug Saf. 2021, 20, 259–264. [Google Scholar] [CrossRef]
- Bousquet, J.; Khaltaev, N.; Cruz, A.A.; Denburg, J.; Fokkens, W.J.; Togias, A.; Zuberbier, T.; Baena-Cagnani, C.E.; Canonica, G.W.; Weel, C. Allergic Rhinitis and Its Impact on Asthma (ARIA) 2008 Update (in Collaboration with the World Health Organization, GA(2)LEN and AllerGen. Allergy 2008, 63 (Suppl. 86), 8–160. [Google Scholar] [CrossRef]
- Pfaar, O.; Bachert, C.; Bufe, A.; Buhl, R.; Ebner, C.; Eng, P.; Friedrichs, F.; Fuchs, T.; Hamelmann, E.; Hartwig-Bade, D. Guideline on Allergen-Specific Immunotherapy in IgE-Mediated Allergic Diseases: S2k Guideline of the German Society for Allergology and Clinical Immunology (DGAKI. In the Society for Pediatric Allergy and Environmental Medicine (GPA), the Medical Association of German Allergologists (AeDA), the Austrian Society for Allergy and Immunology (OGAI), the Swiss Society for Allergy and Immunology (SGAI), the German Society of Dermatology (DDG), the German Society of Oto- Rhino-Laryngology, Head and Neck Surgery (DGHNO-KHC), the German Society of Pediatrics and Adolescent Medicine (DGKJ), the Society for Pediatric Pneumology (GPP), the German Respiratory Society (DGP), the German Association of ENT Surgeons (BV-HNO), the Professional Federation of Paediatricians and Youth Doctors (BVKJ), the Federal Association of Pulmonologists (BDP) and the German Dermatologists Association (BVDD). Allerg. J. Int. 2014, 23, 282–319. [Google Scholar]
- Bousquet, J.; Schunemann, H.J.; Togias, A.; Bachert, C.; Erhola, M.; Hellings, P.W.; Klimek, L.; Pfaar, O.; Wallace, D.; Ansotegui, I. Next-Generation Allergic Rhinitis and Its Impact on Asthma (ARIA) Guidelines for Allergic Rhinitis Based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and Real-World Evidence. J. Allergy Clin. Immunol. 2020, 145, 70–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bousquet, J.; Pfaar, O.; Togias, A.; Schunemann, H.J.; Ansotegui, I.; Papadopoulos, N.G.; Tsiligianni, I.; Agache, I.; Anto, J.M.; Bachert, C. ARIA Care Pathways for Allergen Immunotherapy. Allergy 2019, 74, 2087–2102. [Google Scholar] [CrossRef] [PubMed]
- Wise, S.K.; Lin, S.Y.; Toskala, E.; Orlandi, R.R.; Akdis, C.A.; Alt, J.A.; Azar, A.; Baroody, F.M.; Bachert, C.; Canonica, G.W. International Consensus Statement on Allergy and Rhinology: Allergic Rhinitis. Int. Forum Allergy Rhinol. 2018, 8, 108–352. [Google Scholar] [PubMed]
- Durham, S.R.; Emminger, W.; Kapp, A.; Monchy, J.G.; Rak, S.; Scadding, G.K.; Wurtzen, P.A.; Andersen, J.S.; Tholstrup, B.; Riis, B. SQ-Standardized Sublingual Grass Immunotherapy: Confirmation of Disease Modification 2 Years after 3 Years of Treatment in a Randomized Trial. J. Allergy Clin. Immunol. 2012, 129, 717–725.e5. [Google Scholar] [CrossRef] [Green Version]
- Durham, S.R.; Walker, S.M.; Varga, E.M.; Jacobson, M.R.; O’Brien, F.; Noble, W.; Till, S.J.; Hamid, Q.-A.K.T. Long-Term Clinical Efficacy of Grass-Pollen Immunotherapy. N. Engl. J. Med. 1999, 341, 468–475. [Google Scholar] [CrossRef] [Green Version]
- Pfaar, O.; Nell, M.J.; Boot, J.D.; Versteeg, S.A.; Ree, R.; Roger, A.; Riechelmann, H.; Sperl, A.; Oude Elberink, J.N.; Diamant, Z. A Randomized, 5-Arm Dose Finding Study with a Mite Allergoid SCIT in Allergic Rhinoconjunctivitis Patients. Allergy 2016, 71, 967–976. [Google Scholar] [CrossRef]
- Karakoc-Aydiner, E.; Eifan, A.O.; Baris, S.; Gunay, E.; Akturk, E.; Akkoc, T.; Bahceciler, N.N.; Barlan, I.B. Long-Term Effect of Sublingual and Subcutaneous Immunotherapy in Dust Mite-Allergic Children with Asthma/Rhinitis: A 3-Year Prospective Randomized Controlled Trial. J. Investig Allergol. Clin. Immunol. 2015, 25, 334–342. [Google Scholar]
- Rudman Spergel, A.K.; Minnicozzi, M.; Wheatley, L.M.; Togias, A. Is Allergen Immunotherapy in Children Disease Modifying? A Review of the Evidence. Curr. Allergy Asthma Rep. 2018, 18, 47. [Google Scholar] [CrossRef]
- Alvaro-Lozano, M.; Akdis, C.A.; Akdis, M.; Alviani, C.; Angier, E.; Arasi, S.; Arzt-Gradwohl, L.; Barber, D.; Bazire, R.; Cavkaytar, O. EAACI Allergen Immunotherapy User’s Guide. Pediatr. Allergy Immunol. 2020, 31 (Suppl. 25), 1–101. [Google Scholar] [CrossRef]
- Hoang, M.P.; Samuthpongtorn, J.; Chitsuthipakorn, W.; Seresirikachorn, K.; Snidvongs, K. Rhinology Allergen-Specific Immunotherapy for Local Allergic Rhinitis: A Systematic Review and Meta-Analysis. Rhinology 2022, 60, 11–19. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; the PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Commun. Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campo, P.; Salas, M.; Lopez, N.B.; Rondon, C. Local Allergic Rhinitis. Immunol. Allergy Clin. N. Am. 2016, 36, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Huggins, K.G.; Brostoff, J. Local Production of Specific IgE Antibodies in Allergic—Rhinitis Patients with Negative Skin Test. Lancet 1975, 2, 148–150. [Google Scholar] [CrossRef]
- Rondón, C.; Campo, P.; Herrera, R.; Blanca-Lopez, N.; Melendez, L.; Canto, G.; Torres, M.J.; Blanca, M.J. Nasal Allergen Provocation Test with Multiple Aeroallergens Detects Polysensitization in Local Allergic Rhinitis. Allergy Clin. Immunol. 2011, 128, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Vardouniotis, A.; Doulaptsi, M.; Aoi, N.; Karatzanis, A.; Kawauchi, H.; Prokopakis, E. Local Allergic Rhinitis Revisited. Curr. Allergy Asthma Rep. 2020, 19, 22. [Google Scholar] [CrossRef]
- Rondon, C.; Campo, P.; Gould, H.J.; Barrionuevo, E.; Gevaert, P.; Blanca, M. Local IgE in Non-Allergic Rhinitis. Clin. Exp. Allergy 2015, 45, 872–881. [Google Scholar]
- Scadding, G.K.; Scadding, G.W. Innate and Adaptive Immunity: ILC2 and Th2 Cells in Upper and Lower Airway Allergic Diseases. J. Allergy Clin. Immunol. Pract. 2021, 9, 1851–1857. [Google Scholar] [CrossRef]
- Arasi, S.; Pajno, G.B.; Lau, S.; Matricardi, P.M. Local Allergic Rhinitis: A Critical Reappraisal from a Paediatric Perspective. Pediatr. Allergy Immunol. 2016, 27, 569–573. [Google Scholar] [CrossRef]
- Campo, P.; Eguiluz-Gracia, I.; Bogas, S.; Salas, M.; Plaza Seron, C.; Perez, N.; Mayorga, C.; Torres, M.J.; Shamji, M.H.; Rondon, D. Local allergic Rhinitis: Implications for management. Clin. Exp. Allergy 2019, 49, 6–16. [Google Scholar] [CrossRef] [Green Version]
- Eguiluz-Gracia, I.; Ariza, A.; Testera-Montes, A.; Rondón, C.; Campo, P. Allergen Immunotherapy for Local Respiratory Allergy. Curr. Allergy Asthma Rep. 2020, 20, 23. [Google Scholar] [CrossRef]
- Eguiluz-Gracia, I.; Pérez-Sánchez, N.; Bogas, G.; Campo, P.; Rondón, C. How to Diagnose and Treat Local Allergic Rhinitis: A Challenge for Clinicians. J. Clin. Med. 2019, 8, 1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rondon, C.; Blanca-López, N.; Aranda, A.; Herrera, R.; Rodriguez-Bada, J.L.; Canto, G.; Mayorga, C.; Torres, M.J.; Campo, P.; Blanca, M. Local Allergic Rhinitis: Allergen Tollerance and Immunologic Changes after Presesonal Immunotherapy with Grass Pollen. J. Allergy Clin. Immunol. 2011, 127, 1069–1071. [Google Scholar] [CrossRef] [PubMed]
- Rondón, C.; Campo, P.; Salas, M. Efficacy and safety of D. pteronyssinus immunotherapy in local allergic rhinitis: A double-blind placebo-controlled clinical trial. Allergy 2016, 71, 1057–1061. [Google Scholar] [CrossRef]
- Rondón, C.; Blanca-López, N.; Campo, P. Specific Immunotherapy in Local Allergic Rhinitis: A Randomized, Double-Blind Placebo-Controlled Trial with Phleum Pratense Subcutaneous Allergen Immunotherapy. Allergy 2018, 73, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Bozek, A.; Kołodziejczyk, K. Efficacy and safety of birch pollen immunotherapy for local allergic rhinitis. Ann. Allergy Asthma Immunol. 2018, 120, 53–58. [Google Scholar] [CrossRef]
- Bozek, A.; Galuszka, B.; Gawlik, R.; Misiolek, M.; Scierski, W.; Grzanka, A.; Canonica, G.W. Allergen Immunotherapy against House Dust Mites in Patients with Local Allergic Rhinitis and Asthma. J. Asthma 2021, 1–9. [Google Scholar] [CrossRef]
- Yin, Z.X.; Mi, Y.; Zhai, X. Sublingual Immuno- Therapy of Dermatophagoides Farinae Drops in Nasal Cavity Local Allergy. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2019, 33, 75–79. [Google Scholar]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 20, 1–464. [Google Scholar] [CrossRef]
- Savolainen, S. Allergy in Patients with Acute Maxillary Sinusitis. Allergy 1989, 44, 116–122. [Google Scholar] [CrossRef]
- Schatz, M.; Zeiger, R.S.; Chen, W.; Yang, S.J.; Corrao, M.A.; Quinn, V.P. The burden of rhinitis in a managed care organization. Ann. Allergy Asthma Immunol. 2008, 101, 240–247. [Google Scholar] [CrossRef]
- Rantala, A.; Jaakkola, J.J.; Jaakkola, M.S. Respiratory Infections in Adults with Atopic Disease and IgE Antibodies to Common Aeroallergens. PLoS ONE 2013, 19, e68582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmans, R.; Wagemakers, A.; Drunen, C.; Hellings, P.; Fokkens, W. Acute and Chronic Rhinosinusitis and Allergic Rhinitis in Relation to Comorbidity, Ethnicity and Environment. PLoS ONE 2018, 13, e0192330. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.W.; Wang, S.K.; Lu, M.C.; Wang, C.L.; Koo, M. Acute Rhinosinusitis among Pediatric Patients with Allergic Rhinitis: A Nationwide, Population-Based Cohort Study. PLoS ONE 2019, 14, e0211547. [Google Scholar] [CrossRef] [Green Version]
- De Corso, E.; Lucidi, D.; Cantone, E.; Ottaviano, G.; Di Cesare, T.; Seccia, V.; Paludetti, G.; Galli, J. Clinical Evidence and Biomarkers Linking Allergy and Acute or Chronic Rhinosinusitis in Children: A Systematic Review. Curr. Allergy Asthma Rep. 2020, 20, 68. [Google Scholar] [CrossRef]
- Pant, H.; Ferguson, B.J.; Macardle, P.J. The Role of Allergy in Rhinosinusitis. Curr. Opin. Otolaryngol. Head Neck Surg. 2009, 17, 232–238. [Google Scholar] [CrossRef]
- Frerichs, K.A.; Nigten, G.; Romeijn, K.; Kaper, N.M.; Grolman, W.; Heijden, G.J. Inconclusive Evidence for Allergic Rhinitis to Predict a Prolonged or Chronic Course of Acute Rhinosinusitis. Otolaryngol. Head Neck Surg. 2014, 150, 22–27. [Google Scholar] [CrossRef]
- Leo, G.; Incorvaia, C.; Cazzavillan, A.; Consonni, D.; Zuccotti, G.V. Could Seasonal Allergy Be a Risk Factor for Acute Rhinosinusitis in Children? J. Laryngol. Otol. 2018, 132, 150–153. [Google Scholar] [CrossRef]
- Stevens, W.W.; Ocampo, C.J.; Berdnikovs, S.; Sakashita, M.; Mahdavinia, M.; Suh, L.; Takabayashi, T.; Norton, J.E.; Hulse, K.E.; Conley, D.B.; et al. Cytokines in Chronic Rhinosinusitis. Role in Eosinophilia and Aspirin-exacerbated Respiratory Disease. Am. J. Respir. Crit. Care Med. 2015, 192, 682–694. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, N.; Bo, M.; Holtappels, G.; Zheng, M.; Lou, H.; Wang, H.; Zhang, L.; Bachert, C. Diversity of TH Cytokine Profiles in Patients with Chronic Rhinosinusitis: A Multicenter Study in Europe, Asia, and Oceania. J. Allergy Clin. Immunol. 2016, 138, 1344–1353. [Google Scholar] [CrossRef] [Green Version]
- Mortuaire, G.; Gengler, I.; Balden, M.; Capron, M.; Lefèvre, G. Impact of Allergy on Phenotypic and Endotypic Profiles of Nasal Polyposis. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2018, 135, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Wilson, K.F.; McMains, K.C.; Orlandi, R.R. The Association between Allergy and Chronic Rhinosinusitis with and without Nasal Polyps: An Evidence-Based Review with Recommendations. Int. Forum Allergy Rhinol. 2014, 4, 93–103. [Google Scholar] [CrossRef]
- Rosati, M.G.; Peters, A.T. Relationships among allergic rhinitis, asthma, and chronic rhinosinusitis. Am. J. Rhinol. Allergy 2016, 30, 3044–3047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeYoung, K.; Wentzel, J.L.; Schlosser, R.J.; Nguyen, S.A.; Soler, Z.M. Systematic Review of Immunotherapy for Chronic Rhinosinusitis. Am. J. Rhinol. Allergy 2014, 28, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Borish, L.; Baroody, F.M.; Kim, M.S.; Lieberman, J.A.; Peters, A.; Stevens, W.W.; Bernstein, J.A. Yardstick for the medical management of chronic rhinosinusitis. Ann. Allergy Asthma Immunol. 2022, 128, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, G.J.; Cook, P.R.; Davis, W.E.; McKinsey, J.P. Immunotherapy in Patients Undergoing Functional Endoscopic Sinus Surgery. Otolaryngol. Head Neck Surg. 1994, 110, 406–412. [Google Scholar] [CrossRef]
- Schlenter, W.W.; Mann, W.J. Operative Therapy in Chronic Sinusitis—Results in Allergic and Nonallergic Patients. Laryngol. Rhinol. Otol. 1983, 62, 284–288. [Google Scholar] [CrossRef]
- Asakura, K.; Kojima, T.; Shirasaki, H.; Kataura, A. Evaluation of the Effects of Antigen Specific Immunotherapy on Chronic Sinusitis in Children with Allergy. Auris Nasus Larynx 1990, 17, 33–38. [Google Scholar] [CrossRef]
- Nathan, R.A.; Santilli, J.; Rockwell, W.; Glassheim, J. Effectiveness of Immunotherapy for Recurring Sinusitis Associated with Allergic Rhinitis as Assessed by the Sinusitis Outcomes Questionnaire. Ann. Allergy Asthma Immunol. 2004, 92, 668–672. [Google Scholar] [CrossRef]
- Li, J.; Kang, H.; Hong, S.; Shen, Y. Effect of Postoperative Specific Immunotherapy Combined with Nasal Irrigation on Chronic Rhinosinusitis with Allergic Rhinitis. Iran J. Allergy Asthma Immunol. 2021, 20, 432–440. [Google Scholar] [CrossRef]
- Tan, B.K.; Zirkle, W.; Chandra, R.K.; Lin, D.; Conley, D.B.; Peters, A.T.; Grammer, L.C.; Schleimer, R.P.; Kern, R.C. Atopic Profile of Patients Failing Medical Therapy for Chronic Rhinosinusitis. Int. Forum Allergy Rhinol. 2011, 1, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Gaudio, J.M. Central Compartment Atopic Disease: The Missing Link in the Allergy and Chronic Rhinosinusitis with Nasal Polyps Saga. Int. Forum Allergy Rhinol. 2020, 10, 1191–1192. [Google Scholar] [CrossRef] [PubMed]
- Marcus, S.; Schertzer, J.; Roland, L.T.; Wise, S.K.; Levy, J.M.; DelGaudio, J.M. Central Compartment Atopic Disease: Prevalence of Allergy and Asthma Compared with Other Subtypes of Chronic Rhinosinusitis with Nasal Polyps. Int. Forum Allergy Rhinol. 2020, 10, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Steehler, A.J.; Vuncannon, J.R.; Wise, S.K.; DelGaugio, J.M. Central Compartment Atopic Disease: Outcomes Compared with Other Subtypes of Chronic Rhinosinusitis with Nasal Polyps. Int. Forum Allergy Rhinol. 2021, 11, 1549–1556. [Google Scholar] [CrossRef]
- Edwards, T.S.; Del Gaudio, J.M.; Levy, J.M.; Wise, S.K. A Prospective Analysis of Systemic and Local Aeroallergen Sensitivity in Central Compartment Atopic Disease. Otolaryngol. Head Neck Surg. 2022. [Google Scholar] [CrossRef]
- Bent, J.P.; Kuhn, F.A. Diagnosis of Allergic Fungal Sinusitis. Otolaryngol. Head Neck Surg. 1994, 111, 580–588. [Google Scholar] [CrossRef]
- Gan, E.C.; Thamboo, A.; Rudmik, L.; Hwang, P.H.; Ferguson, B.J.; Javer, A.R. Medical management of allergic fungal rhinosinusitis following endoscopic sinus surgery: An evidence-based review and recommendations. Int. Forum Allergy Rhinol. 2014, 4, 702–715. [Google Scholar] [CrossRef]
- Folker, R.J.; Marple, B.F.; Mabry, R.L.; Mabry, C.S. Treatment of Allergic Fungal Sinusitis: A Comparison Trial of Postoperative Immunotherapy with Specific Fungal Antigens. Laryngoscope 1998, 108, 1623–1627. [Google Scholar] [CrossRef]
- Bassichis, B.A.; Marple, B.F.; Mabry, R.L.; Newcomer, M.T.; Schwade, N.D. Use of Immunotherapy in Previously Treated Patients with Allergic Fungal Sinusitis. Otolaryngol. Head Neck Surg. 2001, 125, 487–490. [Google Scholar] [CrossRef]
- Marple, B.; Newcomer, M.; Schwade, N.; Mabry, R. Natural History of Allergic Fungal Rhinosinusitis: A 4- to 10-Year Follow-Up. Otolaryngol. Head Neck Surg. 2002, 127, 361–366. [Google Scholar] [CrossRef]
- Ameli, F.; Brocchetti, F.; Tosca, M.A.; Signori, A.; Ciprandi, G. Adenoidal Hypertrophy and Allergic Rhinitis: Is There an Inverse Relationship? Am. J. Rhinol. Allergy 2013, 27, e5–e10. [Google Scholar] [CrossRef] [PubMed]
- Papatziamos, G.; Van Hage-Hamsten, M.; Lundahl, J.; Hemlin, C. IgE-Positive Plasma Cells Are Present in Adenoids of Atopic Children. Acta Otolaryngol. 2006, 126, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, H.; Okayama, Y.; Niyonsaba, F.; Fujimori, M.; Enomoto, F.; Yoshikawa, H.; Ikeda, K.; Saito, H. Comparison of Human Tonsillar Mast Cell Localization and Ultrastructural Observations between IgE-Mediated Allergic and Nonallergic Donors. Allergy Asthma Proc. 2006, 27, 415–421. [Google Scholar] [CrossRef]
- Cho, K.S.; Kim, S.H.; Hong, S.L.; Lee, J.; Mun, S.J.; Roh, Y.E.; Kim, Y.M.; Kim, H.Y. Local Atopy in Childhood Adenotonsillar Hypertrophy. Am. J. Rhinol. Allergy 2018, 32, 160–166. [Google Scholar] [CrossRef]
- De Corso, E.; Galli, J.; Di Cesare, T.; Lucidi, D.; Ottaviano, G.; Seccia, V.; Bussu, F.; Passali, G.C.; Paludetti, G.; Cantone, E. A Systematic Review of the Clinical Evidence and Biomarkers Linking Allergy to Adeno-Tonsillar Disease. Int. J. Pediatr. Otorhinolaryngol. 2021, 147, 110799. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi-Shabestari, M.; Jabbari Moghaddam, Y.; Ghaharri, H. Is There Any Correlation between Allergy and Adenotonsillar Tissue Hypertrophy? Int. J. Pediatr. Otorhinolaryngol. 2011, 75, 589–591. [Google Scholar] [CrossRef] [PubMed]
- Modrzynski, M.; Zawisza, E. An Analysis of the Incidence of Adenoid Hypertrophy in Allergic Children. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 713–719. [Google Scholar] [CrossRef]
- Torretta, S.; Pignataro, L.; Carioli, D.; Ibba, T.; Folino, F.; Rosazza, C.; Fattizzo, M.; Marchisio, P. Phenotype Profiling and Allergy in Otitis-Prone Children. Front Pediatr. 2018, 6, 383. [Google Scholar] [CrossRef]
- Capper, R.; Canter, R.J. Is the Incidence of Tonsillectomy Influenced by the Family Medical or Social History? Clin. Otolaryngol. Allied Sci. 2001, 26, 484–487. [Google Scholar] [CrossRef]
- Choi, I.J.; Rhee, C.S.; Lee, C.H.; Kim, D.Y. Effect of Allergic Rhinitis on the Expression of Human β-Defensin 2 in Tonsils. Ann. Allergy Asthma Immunol. 2013, 110, 178–183. [Google Scholar] [CrossRef]
- Ciprandi, G.; Incorvaia, C.; Dell’Albani, I.; Di Cara, G.; Barberi, S.; Puccinelli, P.; Frati, F.; Group, R.I.N.O.B.I.T.S. Allergen Immunotherapy May Exert an Extra-Anti-Allergic Activity in Children. J. Biol. Regul. Homeost. Agents 2013, 27, 1053–1057. [Google Scholar] [PubMed]
- Barberi, S.; Ciprandi, G.; Verduci, E.; D’Auria, E.; Poli, P.; Pietra, B.; Incorvaia, C.; Buttafava, S.; Frati, F.; Riva, E. Effect of High-Dose Sublingual Immunotherapy on Respiratory Infections in Children Allergic to House Dust Mite. Asia Pac. Allergy 2015, 5, 163–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Occasi, F.; De Castro, G.; Zicari, A.M.; Indinnimeo, L.; Tancredi, G.; Duse, M. Sublingual Immunotherapy in Children and Its Potential Beneficial Collateral Effect on Respiratory Tract Infections. Curr. Med. Res. Opin. 2015, 31, 939–941. [Google Scholar] [CrossRef] [PubMed]
- Linkov, G.; Toskala, E. Sublingual Immunotherapy: What We Can Learn from the European Experience. Curr. Opin. Otolaryngol. Head Neck Surg. 2014, 22, 208–210. [Google Scholar] [CrossRef]
- Paradise, J.L.; Rockette, H.E.; Colborn, D.K.; Bernard, B.S.; Smith, C.G.; Kurs-Lasky, M.; Janosky, J.E. Otitis Media in 2253 Pittsburgh-Area Infants: Prevalence and Risk Factors during the First Two Years of Life. Pediatrics 1997, 99, 318–333. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Manoukian, J.J.; Tewfik, T.L.; Sobol, S.E.; Joubert, P.; Mazer, B.D.; Schloss, M.D.; Taha, R.; Hamid, Q.A. Evidence of Allergic Inflammation in the Middle Ear and Nasopharynx in Atopic Children with Otitis Media with Effusion. J. Otolaryngol. 2004, 33, 345–351. [Google Scholar] [CrossRef]
- MacIntyre, E.A.; Heinrich, J. Otitis Media in Infancy and the Development of Asthma and Atopic Disease. Curr. Allergy Asthma Rep. 2012, 12, 547–550. [Google Scholar] [CrossRef]
- MacIntyre, E.A.; Chen, C.M.; Herbarth, O.; Borte, M.; Schaaf, B.; Krämer, U.; Berg, A.; Wichmann, H.E.; Heinrich, J.; Group, L.I.S.A.S. Early-Life Otitis Media and Incident Atopic Disease at School Age in a Birth Cohort. Pediatr. Infect. Dis. J. 2010, 29, e96–e99. [Google Scholar] [CrossRef]
- Zielnik-Jurkiewicz, B.; Stankiewicz-Szymczak, W. Pro-Inflammatory Interleukins in Middle Ear Effusions from Atopic and Non-Atopic Children with Chronic Otitis Media with Effusion. Eur. Arch. Otorhinolaryngol. 2016, 273, 1369–1378. [Google Scholar] [CrossRef]
- Kanazawa, H.; Yoshida, N.; Shinnabe, A.; Iino, Y. Antigen-Specific IgE in Middle Ear Effusion of Patients with Eosinophilic Otitis Media. Ann. Allergy Asthma Immunol. 2014, 113, 88–92. [Google Scholar] [CrossRef]
- Iino, Y. Role of IgE in Eosinophilic Otitis Media. Allergol. Int. 2010, 59, 233–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Xu, M.; Zhang, J.; Zeng, L.; Wang, Y.; Zheng, Q.Y. Risk Factors for Chronic and Recurrent Otitis Media-a Meta-Analysis. PLoS ONE 2014, 9, e86397. [Google Scholar]
- Ciprandi, G.; Torretta, S.; Marseglia, G.L.; Licari, A.; Chiappini, E.; Benazzo, M.; Tosca, M.A.; Marchisio, P. Allergy and Otitis Media in Clinical Practice. Curr. Allergy Asthma Rep. 2020, 20, 33. [Google Scholar] [CrossRef] [PubMed]
- Torretta, S.; Marchisio, P. Otitis Media in Children: A Proposal for a New Nosological Classification. Int. J. Pediatr. Otorhinolaryngol. 2017, 93, 174–175. [Google Scholar] [CrossRef]
- De Corso, E.; Cantone, E.; Galli, J.; Seccia, V.; Lucidi, D.; Di Cesare, T.; Ottaviano, G.; Sergi, B.; Paludetti, G.; Fetoni, A.R. Otitis Media in Children: Which Phenotypes Are Most Linked to Allergy? A Systematic Review. Pediatr. Allergy Immunol. 2021, 32, 524–534. [Google Scholar] [CrossRef] [PubMed]
- Kreiner-Møller, E.; Chawes, B.L.; Caye-Thomasen, P.; Bønnelykke, K.; Bisgaard, H. Allergic Rhinitis Is Associated with Otitis Media with Effusion: A Birth Cohort Study. Clin. Exp. Allergy 2012, 42, 1615–1620. [Google Scholar] [CrossRef]
- La Mantia, I.; Varricchi, A.; Ciprandi, G. Allergen Immunotherapy in Children with Otitis Media with Effusion: A Preliminary Experience. Eur. Ann. Allergy Clin. Immunol. 2021, 53, 288–290. [Google Scholar] [CrossRef]
- Hurst, D.S. Efficacy of Allergy Immunotherapy as a Treatment for Patients with Chronic Otitis Media with Effusion. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 1215–1223. [Google Scholar] [CrossRef]

| Authors (Years) | Type of Study | Patients (n) | Methods | Duration of AIT Therapy | Duration of FUP | Mean Outcomes Measured | Results | Conclusions | Y/N |
|---|---|---|---|---|---|---|---|---|---|
| Rondon Cet al., 2011 [54] | Pilot, observational | 20 | Preseasonal grass SCIT+ rescue medication in the spring vs. rescue medication (control group) | 6 months | 12 months | NAPT to grass SPT, grass pollen sIgG and sIgE, symptom and medication scores, medication-free days, severity of LAR symptoms | ↑NAPT, ↑ sIgG to grass pollen ↓ symptoms, ↓ rescue medication ↓ scores and severity of rhinitis in the following spring | SCIT with grass pollen showed to be safe and effective in patients with LAR; SCIT can modify the disease course with an important reduction in severity | Y |
| Rondon C et al., 2016 [55] | DBPC | 36 | Pangramin plus DP or placebo | 24 months | N/A | NAPT, TdSS, TdMS, CdSMS, MFD, SPT, DP-sIgE and DP-sIgG4, adverse events | ↑ NAPT, ↓ TdSS and TdMS ↑ MFD ↑ sIgG4 no systemic reactions were reported | AIT-DP is clinically effective and safe, | Y |
| Rondon C et al., 2018 [56] | DBPC | 56 | Phl -SCIT with a depigmented polymerized pollen vaccine or placebo for the first year, and Phl-SCIT the second year | 24 months | N/A | CSMS during GPS, organ-specific symptoms, MFD, rhinitis severity and asthma control RQLQ, NAPT, sIgG4, safety | Significant improvements of all clinical outcomes | SCIT with depigmented polymerized allergen extracts was a safe and clinically effective treatment for LAR to Phl pratense. | Y |
| Bozek A et al., 2018 [57] | DBPC | 28 | Birch SCIT | 24 months | N/A | SMS, sIgE and IgG4 and nasal -specific IgE to Bet v 1, SMS | ↓ SMS ↑ Ig G4, ↓ nasal-specific IgE | AIT for birch pollen was clinically effective and exhibited good tolerance | Y |
| Bozek A et al., 2021 [58] | DBPC | 32 | 12-month treatment of SLIT for HDM | N/A | N/A | TRSS, TASS, TSS, TMS, FEV1 | ↓ in TRSS, TASS, TSS and TMS ↑ FEV1 after 12 months of treatment | SLIT can improve nasal and bronchial symptoms and reduce symptomatic treatment in patients with LAR and asthma and with hyperresponsiveness to HDMs. | Y |
| Yin ZX et al., 2019 [59] | Observational | 60 | Sublingual immunotherapy of Dermatophagoides farinae drops | 3 years | N/A | Symptom scores, VAS Eosinophils in nasal secretions, nasal secretions sIgE, nasal mucous membrane excitation test | Improvement of symptom and VAS scores, eosinophilia counts in nasal secretion, nasal secretions allergen sIgE test, nasal mucous membrane excitation test | Sublingual immunotherapy of Dermatophagoides farinae drops in nasal cavity local allergy was effective | Y |
| Authors (Years) | Type of Study | Patients (n) | Methods | Duration of AIT Therapy | Duration of FUP | Mean Outcomes Measured | Results | Conclusions | Y/N |
|---|---|---|---|---|---|---|---|---|---|
| Ciprandi et al., 2013 [102] | Case- control | 77 | To investigate the impact of SLIT on extra-allergic outcomes (number of infections and drug prescriptions) in children with allergic rhinitis. | 2 years | 2 years | The use of drugs, the presence of respiratory symptoms and extra-allergic clinical manifestations | SLIT is effective in reducing the number of respiratory infections, drug prescriptions and improving symptoms in treated children compared to controls. | SLIT exerts adjunctive anti-allergic effects. | Y |
| Barberi et al., 2015 [103] | Case- control | 40 | To investigate the impact of a 6-months high-dose house dust mite SLIT on respiratory tract infections in children with allergic rhinitis. | 6 months | N/A | The number of respiratory infections (acute rhinosinusitis, otitis, pharyngotonsillitis, laryngitis, bronchitis, pneumonia), the presence of fever, snoring, the use of antibiotics, anti-inflammatory drugs, oral corticosteroids and fever-reducers | A significantly reduction in the number of respiratory infections (i.e., pharyngo-tonsillitis, bronchitis, fever episodes), and in antibiotics/antipyretics prescriptions was documented in the study group compared to the control one. | A short course of SLIT could reduce the number of respiratory tract infections in allergic rhinitis children. | Y |
| Occasi et al., 2015 [104] | Case- control | 265 | To evaluate the effectiveness of SLIT on susceptibility to respiratory tract infections in children with allergic rhinitis. | 2 years | 6 years | The number of respiratory tract infections | The number of respiratory tract infections was significantly reduced in the study group compared to the control group during the last two years of the treatment; no differences were detected before. | SLIT could have possible benefic effects on respiratory infections | Y |
| Authors (Years) | Type of Study | Patients (n) | Methods | Results | Duration of AIT Therapy | Duration of FUP | Mean Outcomes Measured | Conclusions | Y/N |
|---|---|---|---|---|---|---|---|---|---|
| La Mantia et al., 2021 [118] | Case- control | 40 | To investigate the effectiveness of 2-year dust mite immunotherapy in children with allergic rhinitis and otitis media with effusion. | Complete recovery was attested in more than 50% of treated children compared to 15% of children receiving anti-allergic treatment alone. | 2 years | 18 months | Change in tympanometry findings | OME has an allergic background, and it could effectively respond to specific AIT. | Y |
| Hurst, 2008 [119] | Cross sectional | 52 | To assess the therapeutic benefit on middle ear complaints deriving from specific allergen immunotherapy. | An atopic status was discovered in 100% of patients. Complete/partial recovery was attested in more than 95% of treated patients. | 4 years (as a mean) | 2–8 years (range) | Resolution of OME (documented by means of pneumatic otoscopy, tympanometry, audiometry); episodes of acute ear discharge; needing for tympanostomy tube placement | OME is an immune mediated allergic condition responding to specific AIT | Y |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantone, E.; Gallo, S.; Torretta, S.; Detoraki, A.; Cavaliere, C.; Di Nola, C.; Spirito, L.; Di Cesare, T.; Settimi, S.; Furno, D.; et al. The Role of Allergen-Specific Immunotherapy in ENT Diseases: A Systematic Review. J. Pers. Med. 2022, 12, 946. https://doi.org/10.3390/jpm12060946
Cantone E, Gallo S, Torretta S, Detoraki A, Cavaliere C, Di Nola C, Spirito L, Di Cesare T, Settimi S, Furno D, et al. The Role of Allergen-Specific Immunotherapy in ENT Diseases: A Systematic Review. Journal of Personalized Medicine. 2022; 12(6):946. https://doi.org/10.3390/jpm12060946
Chicago/Turabian StyleCantone, Elena, Stefania Gallo, Sara Torretta, Aikaterini Detoraki, Carlo Cavaliere, Claudio Di Nola, Luca Spirito, Tiziana Di Cesare, Stefano Settimi, Daniela Furno, and et al. 2022. "The Role of Allergen-Specific Immunotherapy in ENT Diseases: A Systematic Review" Journal of Personalized Medicine 12, no. 6: 946. https://doi.org/10.3390/jpm12060946
APA StyleCantone, E., Gallo, S., Torretta, S., Detoraki, A., Cavaliere, C., Di Nola, C., Spirito, L., Di Cesare, T., Settimi, S., Furno, D., Pignataro, L., & De Corso, E. (2022). The Role of Allergen-Specific Immunotherapy in ENT Diseases: A Systematic Review. Journal of Personalized Medicine, 12(6), 946. https://doi.org/10.3390/jpm12060946