
Pharmacogenetic Expression of CYP2C19 in a Pediatric Population

 , and
, and
Abstract
:1. Introduction

{kind=link}
| Predicted Phenotype | Genotype | Examples of CYP2C19 Diplotypes |
|---|---|---|
| CYP2C19 ultra-rapid metabolizer | An individual carrying two increased function alleles | *17/*17 |
| CYP2C19 rapid metabolizer | An individual carrying one normal function allele and one increased function allele | *1/*17 |
| CYP2C19 normal metabolizer | An individual carrying two normal function alleles | *1/*1 |
| CYP2C19 likely intermediate metabolizer | An individual carrying one normal function allele and one decreased function allele or one increased function allele and one decreased function allele or two decreased function alleles | *1/*9, *9/*17, *9/*9 |
| CYP2C19 intermediate metabolizer | An individual carrying one normal function allele and one no function allele or one increased function allele and one no function allele | *1/*2, *1/*3, *2/*17, *3/*17 |
| CYP2C19 likely poor metabolizer | An individual carrying one decreased function allele and one no function allele | *2/*9, *3/*9 |
| CYP2C19 poor metabolizer | An individual carrying two no function alleles | *2/*2, *3/*3, *2/*3 |
| Indeterminate metabolizer | An individual carrying one or two uncertain function alleles | *1/*12, *2/*12, *12/*14 |
2. Selection of the Studies
3. Study Descriptions
3.1. Voriconazole and CYP2C19 Metabolizer Status
3.2. Clopidogrel and CYP2C19 Metabolizer Status
3.3. PPIs and CYP2C19 Metabolizer Status
3.4. Anti-Depressants and CYP2C19 Metabolizer Status
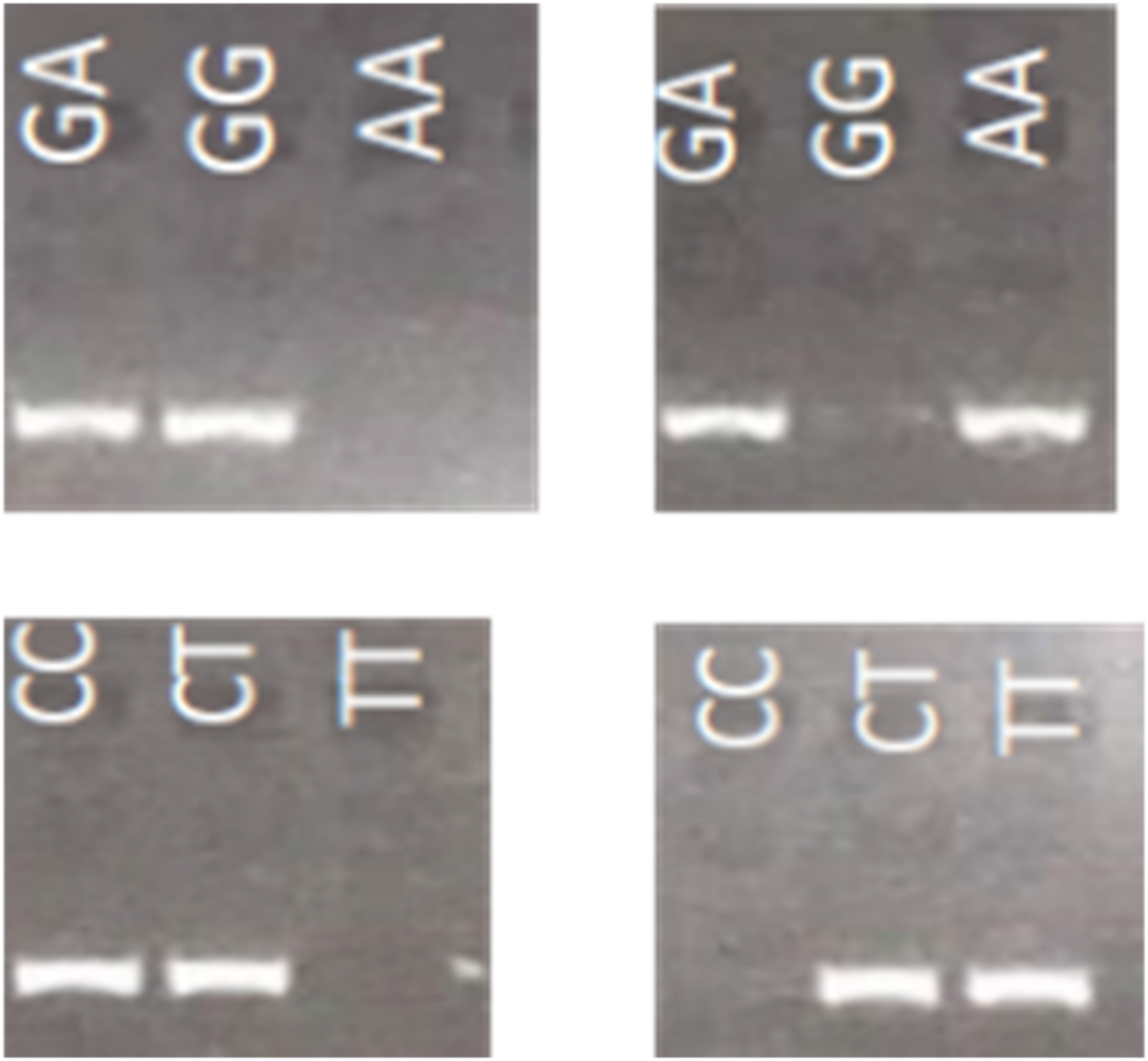
4. Genotyping Assays for CYP2C19
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Botton, M.R.; Whirl-Carrillo, M.; Del Tredici, A.L.; Sangkuhl, K.; Cavallari, L.H.; Agúndez, J.A.G.; Claudio-Campos, K.; Duconge, J.; Wadelius, M.; Woodahl, E.L.; et al. PharmVar GeneFocus: CYP2C19. Clin. Pharmacol. Ther. 2021, 109, 352–366. [Google Scholar] [CrossRef]
- Cohn, I.; Manshaei, R.; Liston, E.; Okello, J.B.A.; Khan, R.; Curtis, M.R.; Krupski, A.J.; Jobling, R.K.; Kalbfleisch, K.; Paton, T.A.; et al. Assessment of the Implementation of Pharmacogenomic Testing in a Pediatric Tertiary Care Setting. JAMA Netw. Open 2021, 4, e2110446. [Google Scholar] [CrossRef] [PubMed]
- Relling, M.V.; Klein, T.E.; Gammal, R.S.; Whirl-Carrillo, M.; Hoffman, J.M.; Caudle, K.E. The Clinical Pharmacogenetics Implementation Consortium: 10 Years Later. Clin. Pharmacol. Ther. 2020, 107, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.R.; Luzum, J.A.; Sangkuhl, K.; Gammal, R.S.; Sabatine, M.S.; Stein, C.M.; Kisor, D.F.; Limdi, N.A.; Lee, Y.M.; Scott, S.A.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2C19 Genotype and Clopidogrel Therapy: 2022 Update. Clin. Pharmacol. Ther. 2022, 1, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Mohamud, M.A.; Smith, A.R.; Jacobson, P.A.; Jaber, M.M.; Alharbi, A.F.; Fisher, J.; Kirstein, M.N. CYP2C19 Phenotype and Body Weight-Guided Voriconazole Initial Dose in Infants and Children after Hematopoietic Cell Transplantation. Antimicrob. Agents Chemother. 2021, 65, e0062321. [Google Scholar] [CrossRef]
- Zhao, Y.C.; Zou, Y.; Hou, J.J.; Xiao, C.L.; Zhang, B.K.; Li, J.K.; Xiang, D.-X.; Sandaradura, I.; Yan, M. Factors Affecting Voriconazole Trough Concentration and Optimal Maintenance Voriconazole Dose in Chinese Children. Antibiotics 2021, 10, 1542. [Google Scholar] [CrossRef]
- Owusu Obeng, A.; Egelund, E.F.; Alsultan, A.; Peloquin, C.A.; Johnson, J.A. CYP2C19 polymorphisms and therapeutic drug monitoring of voriconazole: Are we ready for clinical implementation of pharmacogenomics? Pharmacotherapy 2014, 34, 703–718. [Google Scholar] [CrossRef]
- Narita, A.; Muramatsu, H.; Sakaguchi, H.; Doisaki, S.; Tanaka, M.; Hama, A.; Shimada, A.; Takahashi, Y.; Yoshida, N.; Matsumoto, K.; et al. Correlation of CYP2C19 phenotype with voriconazole plasma concentration in children. J. Pediatr. Hematol. Oncol. 2013, 35, e219–e223. [Google Scholar] [CrossRef]
- Tian, X.; Zhang, C.; Qin, Z.; Wang, D.; Yang, J.; Zhang, X. Impact of CYP2C19 Phenotype and Drug-Drug Interactions on Voriconazole Concentration in Pediatric Patients. Antimicrob. Agents Chemother. 2021, 65, e0020721. [Google Scholar] [CrossRef]
- Hicks, J.K.; Quilitz, R.E.; Komrokji, R.S.; Kubal, T.E.; Lancet, J.E.; Pasikhova, Y.; Qin, D.; So, W.; Caceres, G.; Kelly, K.; et al. Prospective CYP2C19-Guided Voriconazole Prophylaxis in Patients with Neutropenic Acute Myeloid Leukemia Reduces the Incidence of Subtherapeutic Antifungal Plasma Concentrations. Clin. Pharmacol. Ther. 2020, 107, 563–570. [Google Scholar] [CrossRef]
- García-García, I.; Dapía, I.; Montserrat, J.; Martinez de Soto, L.; Bueno, D.; Díaz, L.; Queiruga, J.; Mariblanca, A.R.; Guerra-García, P.; Ramirez, E.; et al. Experience of a Strategy Including CYP2C19 Preemptive Genotyping Followed by Therapeutic Drug Monitoring of Voriconazole in Patients Undergoing Allogenic Hematopoietic Stem Cell Transplantation. Front. Pharmacol. 2021, 12, 717932. [Google Scholar] [CrossRef]
- Wang, J.; Xu, H.; Li, R.; Wu, S.; Zou, J.; Wang, Y. Model-Oriented Dose Optimization of Voriconazole in Critically Ill Children. Antimicrob. Agents Chemother. 2021, 65, e0049321. [Google Scholar] [CrossRef]
- Chen, J.; Wu, Y.; He, Y.; Feng, X.; Ren, Y.; Liu, S. Combined Effect of CYP2C19 Genetic Polymorphisms and C-Reactive Protein on Voriconazole Exposure and Dosing in Immunocompromised Children. Front. Pediatr. 2022, 10, 846411. [Google Scholar] [CrossRef]
- Li, D.; Chen, X.; Li, X.; Yuan, Y.; Jin, H.; Liu, G.; Zhang, H.; Xie, G. Effectiveness and safety of dual antiplatelet therapy in coronary aneurysms caused by Kawasaki disease in children: Study protocol for a multicenter randomized clinical trial. Transl. Pediatr. 2021, 10, 1914–1923. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, D.N.; Lancaster, C.A.; McElhinney, D.B.; Chen, S.; Stein, M.; Lin, A.; Đoàn, L.; Murray, J.M.; Gowan, M.A.; Maeda, K.; et al. Impact of a modified anti-thrombotic guideline on stroke in children supported with a pediatric ventricular assist device. J. Heart Lung Transplant. 2017, 36, 1250–1257. [Google Scholar] [CrossRef]
- El Rouby, N.; Lima, J.J.; Johnson, J.A. Proton pump inhibitors: From CYP2C19 pharmacogenetics to precision medicine. Expert Opin. Drug Metab. Toxicol. 2018, 14, 447–460. [Google Scholar] [CrossRef]
- Ward, R.M.; Tammara, B.; Sullivan, S.E.; Stewart, D.L.; Rath, N.; Meng, X.; Maguire, M.K.; Comer, G.M. Single-dose, multiple-dose, and population pharmacokinetics of pantoprazole in neonates and preterm infants with a clinical diagnosis of gastroesophageal reflux disease (GERD). Eur. J. Clin. Pharmacol. 2010, 66, 555–561. [Google Scholar] [CrossRef]
- Gumus, E.; Karaca, O.; Babaoglu, M.O.; Baysoy, G.; Balamtekin, N.; Demir, H.; Uslu, N.; Bozkurt, A.; Yuce, A.; Yasar, U. Evaluation of lansoprazole as a probe for assessing cytochrome P450 2C19 activity and genotype-phenotype correlation in childhood. Eur. J. Clin. Pharmacol. 2012, 68, 629–636. [Google Scholar] [CrossRef]
- Franciosi, J.P.; Mougey, E.B.; Williams, A.; Gomez-Suarez, R.A.; Thomas, C.; Creech, C.L.; George, K.; Corao, D.; Lima, J.J. Association Between CYP2C19*17 Alleles and pH Probe Testing Outcomes in Children with Symptomatic Gastroesophageal Reflux. J. Clin. Pharmacol. 2018, 58, 89–96. [Google Scholar] [CrossRef]
- Bernal, C.J.; Aka, I.; Carroll, R.J.; Coco, J.R.; Lima, J.J.; Acra, S.A.; Roden, D.M.; van Driest, S.L. CYP2C19 Phenotype and Risk of Proton Pump Inhibitor-Associated Infections. Pediatrics 2019, 144, e20190857. [Google Scholar] [CrossRef]
- Mougey, E.B.; Williams, A.; Coyne, A.J.K.; Gutiérrez-Junquera, C.; Fernández-Fernández, S.; Cilleruelo, M.L.; Rayo, A.; Echeverría, L.; Román, E.; Lois, C.G.; et al. CYP2C19 and STAT6 Variants Influence the Outcome of Proton Pump Inhibitor Therapy in Pediatric Eosinophilic Esophagitis. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, L.B.; Bishop, J.R.; Strawn, J.R. Pharmacogenetics of treating pediatric anxiety and depression. Pharmacogenomics 2019, 20, 867–870. [Google Scholar] [CrossRef] [PubMed]
- Hicks, J.K.; Sangkuhl, K.; Swen, J.J.; Ellingrod, V.L.; Müller, D.J.; Shimoda, K.; Bishop, J.R.; Kharasch, E.D.; Skaar, T.C.; Gaedigk, A.; et al. Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clin. Pharmacol. Ther. 2017, 102, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Ariefdjohan, M.; Lee, Y.M.; Stutzman, D.L.; LeNoue, S.; Wamboldt, M.Z. The Utility of Pharmacogenetic-Guided Psychotropic Medication Selection for Pediatric Patients: A Retrospective Study. Pediatr. Rep. 2021, 13, 421–433. [Google Scholar] [CrossRef]
- Strawn, J.R.; Poweleit, E.A.; Ramsey, L.B. CYP2C19-Guided Escitalopram and Sertraline Dosing in Pediatric Patients: A Pharmacokinetic Modeling Study. J. Child Adolesc. Psychopharmacol. 2019, 29, 340–347. [Google Scholar] [CrossRef]
- Aldrich, S.L.; Poweleit, E.A.; Prows, C.A.; Martin, L.J.; Strawn, J.R.; Ramsey, L.B. Influence of CYP2C19 Metabolizer Status on Escitalopram/Citalopram Tolerability and Response in Youth with Anxiety and Depressive Disorders. Front. Pharmacol. 2019, 10, 99. [Google Scholar] [CrossRef]
- Rossow, K.M.; Aka, I.T.; Maxwell-Horn, A.C.; Roden, D.M.; van Driest, S.L. Pharmacogenetics to Predict Adverse Events Associated with Antidepressants. Pediatrics 2020, 146, e20200957. [Google Scholar] [CrossRef]
- Kim, H.K.; Kang, H.J.; Ko, D.H.; Jeong, T.D.; Lee, W.; Chun, S.; Min, W.K. Comparison of the microarray-based assay, the real-time PCR assay, and the bidirectional sequencing method for CYP2C19 genotyping. Clin. Lab. 2015, 61, 1109–1112. [Google Scholar] [CrossRef]
- De Leon, J.; Susce, M.T.; Murray-Carmichael, E. The AmpliChip CYP450 genotyping test: Integrating a new clinical tool. Mol. Diagn. Ther. 2006, 10, 135–151. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, H.; Li, K.; Shi, M. Development of a Polymerase Chain Reaction/Ligase Detection Reaction Assay for Detection of CYP2C19 Polymorphisms. Genet. Test. Mol. Biomark. 2018, 22, 62–73. [Google Scholar] [CrossRef]
- Scott, S.A.; Tan, Q.; Baber, U.; Yang, Y.; Martis, S.; Bander, J.; Kornreich, R.; Hulot, J.-S.; Desnick, R.J. An Allele-Specific PCR System for Rapid Detection and Discrimination of the CYP2C19 *4A, *4B, and *17 Alleles: Implications for Clopidogrel Response Testing. J. Mol. Diagn. 2013, 15, 783–789. [Google Scholar] [CrossRef]
- Gaudet, M.; Fara, A.-G.; Beritognolo, I.; Sabatti, M. Allele-Specific PCR in SNP Genotyping. In Single Nucleotide Polymorphisms: Methods and Protocols; Komar, A.A., Ed.; Humana Press: Totowa, NJ, USA, 2009; pp. 415–424. [Google Scholar]
- Wangkumhang, P.; Chaichoompu, K.; Ngamphiw, C.; Ruangrit, U.; Chanprasert, J.; Assawamakin, A.; Tongsima, S. WASP: A Web-based Allele-Specific PCR assay designing tool for detecting SNPs and mutations. BMC Genom. 2007, 8, 275. [Google Scholar] [CrossRef] [Green Version]

| Authors (Year of Publication) | Title | Objectives | Study Type | Results |
|---|---|---|---|---|
| Narita et al. (2013) [8] | Correlation of CYP2C19 Phenotype with VCZ Plasma Concentration in Children | Analysis of the metabolizer status as defined by CYP2C19 genotype and VCZ plasma concentrations | Retrospective study | VCZ Cmin higher in PMs and IMs than in NMs and UMs |
| Takahashi et al. (2021) [5] | CYP2C19 Phenotype and Body Weight-Guided VCZ Initial Dose in Infants and Children after Hematopoietic Cell Transplantation | Characterize the effects of CYP2C19 metabolizer status with covariateson the PK variability of prophylactic VCZ in pediatric patients after hematopoietic cell transplantation (HSCT) | Observational study | Dose to achieve target concentration: 33–50% lower for PMs, IMs 25–50% higher for RMs, UMs |
| Tian et al. (2021) [9] | Impact of CYP2C19 Phenotype and Drug-Drug Interactions on Voriconazole Concentration in Pediatric Patients | To study the key factors that affect VCZ Cmin in Chinese pediatric patients with hematological malignancies who have undergone HSCT | Retrospective study | IM: 0.31 mg/mL/mg/kg PM: 0.48 mg/mL/mg/kg (higher Cmin) EM: 0.11 mg/mL/mg/kg UM: 0.09 mg/mL/mg/kg Omeprazole: increased VCZ concentration Rifampicin: decrease VCZ concentration |
| Hicks et al. (2020) [10] | Prospective CYP2C19-Guided Voriconazole Prophylaxis in Patients with Neutropenic Acute Myeloid Leukemia Reduces the Incidence of Subtherapeutic Antifungal Plasma Concentrations | Describe the implementation of a prospective quality improvement study to determine if a higher prophylactic voriconazole dosage of 300 mg twice daily for CYP2C19 rapid metabolizers reduces the incidence of subtherapeutic trough concentrations without increasing voriconazole-induced toxicities | Prospective study | RM: received increased starting doses UM: avoid VCZ NM, IM: received standard starting doses |
| Garcia-García et al. (2021) [11] | Experience of a Strategy Including CYP2C19 Preemptive Genotyping Followed by Therapeutic Drug Monitoring of Voriconazole in Patients Undergoing Allogenic Hematopoietic Stem Cell Transplantation | Provide information to individualize VCZ treatment in immunocompromised pediatric patients and compare the results with those of Hicks et al. | Analyses of pediatric patients preemptively tested for the CYP2C19 genotype | Starting dose changes in 29% of patients NMs and IMs: received standard starting doses RM and UM: received increased initial doses No PM in the cohort |
| Wang et al. (2021) [12] | Model-Oriented Dose Optimization of Voriconazole in Critically Ill Children. Antimicrobial Agents Chemother | To use a PK model to optimize voriconazole dosing regimen in children with critical illness | Pharmacokinetic modeling study | 30–40% lower maintenance doses in PM compared to EM |
| Zhao et al. (2021) [6] | Factors Affecting Voriconazole Trough Concentration and Optimal Maintenance Voriconazole Dose in Chinese Children | Investigate maintenance dose to optimize VCZ therapy and factors affecting trough VCZ concentration | Non-interventional retrospective clinical study | CYP2C19 genotype influenced VCZ Cmin |
| Chen et al. (2022) [13] | Combined Effect of CYP2C19 Genetic Polymorphisms and C-Reactive Protein on Voriconazole Exposure and Dosing in Immunocompromised Children | Identify factors associated with VCZ concentrations and doses required to achieve therapeutic concentrations | Retrospective study | NM: lower VCZ exposure and high daily dose needed to achieve the therapeutic concentration compared to PM Influence of other factors on VCZ concentration, such as C reactive protein |
| Authors (Year of Publication) | Title | Objectives | Study Type | Results |
|---|---|---|---|---|
| Bernal et al. (2019) [20] | CYP2C19 phenotype and risk of proton pump inhibitor associated infections | To test the hypothesis that CYP2C19 metabolizing groups are associated with infectious events in children on PPIs | Retrospective cohort study | NM: higher infection rate compared to RM/UM |
| Franciosi et al. (2018) [19] | Association between CYP2C19*17 allele and pH probe testing in children with symptomatic gastroesophageal reflux | Investigate if PPI drug-resistant GERD may be related to CYP2C19 variants | Retrospective cohort study | CYP2C19*17 carriers: longer duration of exposure to an acidic pH |
| Mougey et al. (2019) [21] | CYP2C19 and STAT 6 variants influence the outcome of PPI Therapy in Pediatric Eosinophilic Esophagitis | Investigate the influence of the CYP2C19 genotypes on the treatment of eosinophilic esophagitis by PPIs | Prospective study | CYP2C19*17 carriers: insensitive to PPIs |
| Authors (Year of Publication) | Title | Objectives | Study Type | Results |
|---|---|---|---|---|
| Ariefdjohan et al. (2021) [24] | The utility of pharmacogenetic guided psychotropic medication selection for pediatric patients: a retrospective study | Describe trends and clinical experiences in the application of pharmacogenetic testing in pediatric patients with neuropsychiatric disorders | Retrospective study |
|
| Strawn et al. (2019) [25] | CYP2C19 guided escitalopram and sertraline dosing in pediatric patients: a pharmacokinetic modeling study | Assess the impact of CYP2C19 metabolizer status on exposure to SSRIs (escitalopram or sertraline) | Pharmacokinetic modeling study | PM: higher Cmax and AUC |
| Aldrich et al. (2019) [26] | Influence of CYP2C19 metabolizer status on escitalopram/citalopram tolerability and response in youth with anxiety and depressive disorders | Investigate the association between CYP2C19 metabolizer status and response to antidepressant treatment | Retrospective study | PM: more adverse effects due to escitalopram/citalopram |
| Rossow et al. (2020) [27] | Pharmacogenetics to predict adverse events associated with pediatric antidepressants | To determine the association between the CYP2C19 genotype and the risk of side effects of (es)citalopram | Retrospective study | NM: higher adverse effects due to sertraline and escitalopram (surprising effect due to physiological differences in adolescence) |
| Allele Name/SNP Position | SNP Identifier | Allele-Specific Primers—Forward | Allele-Specific Primers—Reverse |
|---|---|---|---|
| CYP2C19 *2 681 | rs4244285 | CACTATCATTGATTATTACCCG/A | CTCCATTTTGATCAGGAAGC |
| CYP2C19*3 636 | rs4986893 | GGATTGTAAGCACCCGCTGG/A | AGAACTTTGCCATCTTTTCCAG |
| CYP2C19*17 806 | rs12248560 | GTGTCTTCTGTTCTCTAAGC/T | CAAATGGGAAAAGGGAGAC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pierre-François, M.J.D.; Gagné, V.; Brukner, I.; Krajinovic, M. Pharmacogenetic Expression of CYP2C19 in a Pediatric Population. J. Pers. Med. 2022, 12, 1383. https://doi.org/10.3390/jpm12091383
Pierre-François MJD, Gagné V, Brukner I, Krajinovic M. Pharmacogenetic Expression of CYP2C19 in a Pediatric Population. Journal of Personalized Medicine. 2022; 12(9):1383. https://doi.org/10.3390/jpm12091383
Chicago/Turabian StylePierre-François, Marie Josette Déborah, Vincent Gagné, Ivan Brukner, and Maja Krajinovic. 2022. "Pharmacogenetic Expression of CYP2C19 in a Pediatric Population" Journal of Personalized Medicine 12, no. 9: 1383. https://doi.org/10.3390/jpm12091383
APA StylePierre-François, M. J. D., Gagné, V., Brukner, I., & Krajinovic, M. (2022). Pharmacogenetic Expression of CYP2C19 in a Pediatric Population. Journal of Personalized Medicine, 12(9), 1383. https://doi.org/10.3390/jpm12091383