

Impact of the COVID-19 Pandemic on Mortality Following Hip and Knee Joint Arthroplasty Surgeries: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Synthesis and Statistical Analyses
3. Results
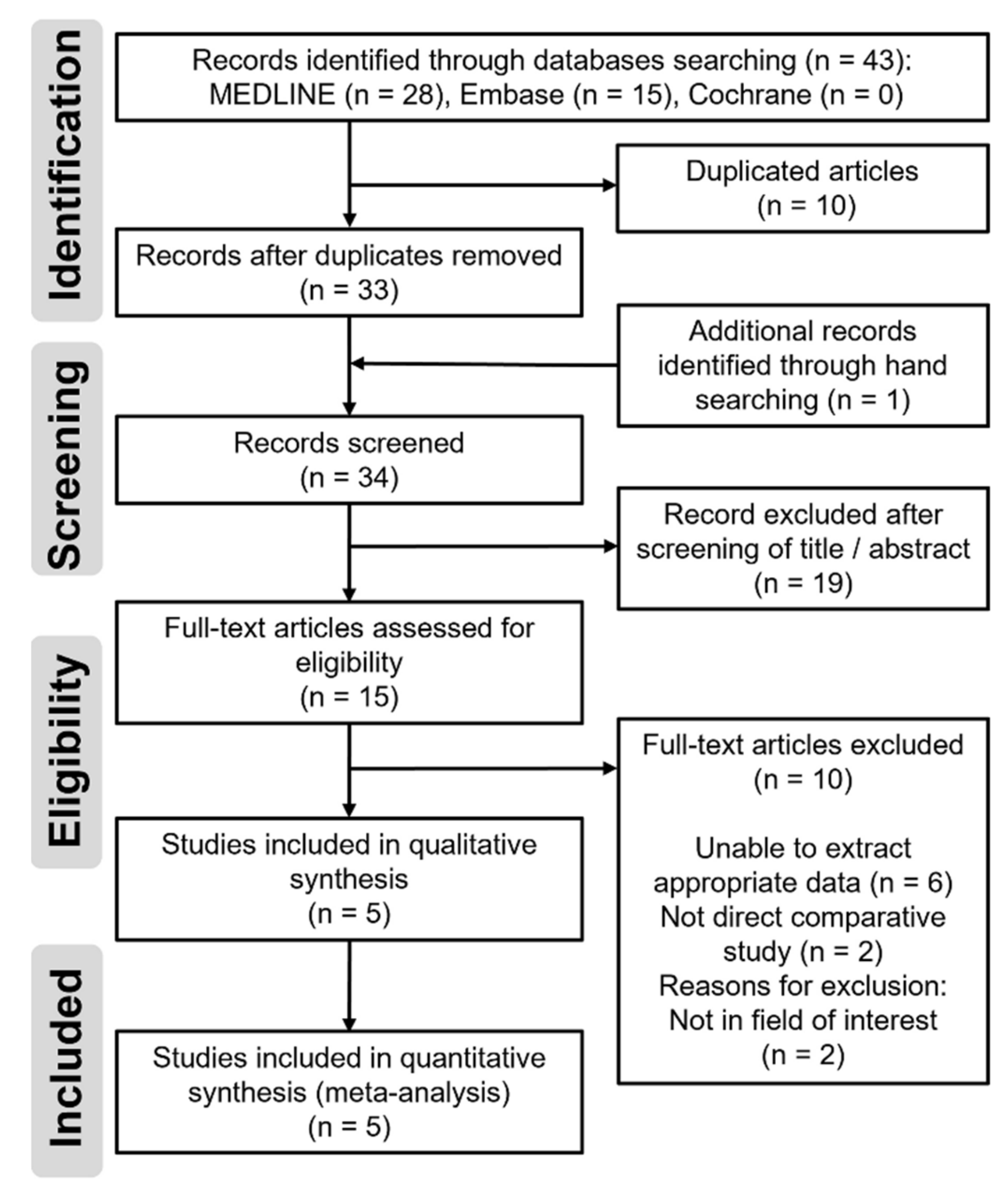
3.1. Study Identification
3.2. Study Characteristics and Demographics
3.3. Risk of Bias Assessment
3.4. Meta-Analysis
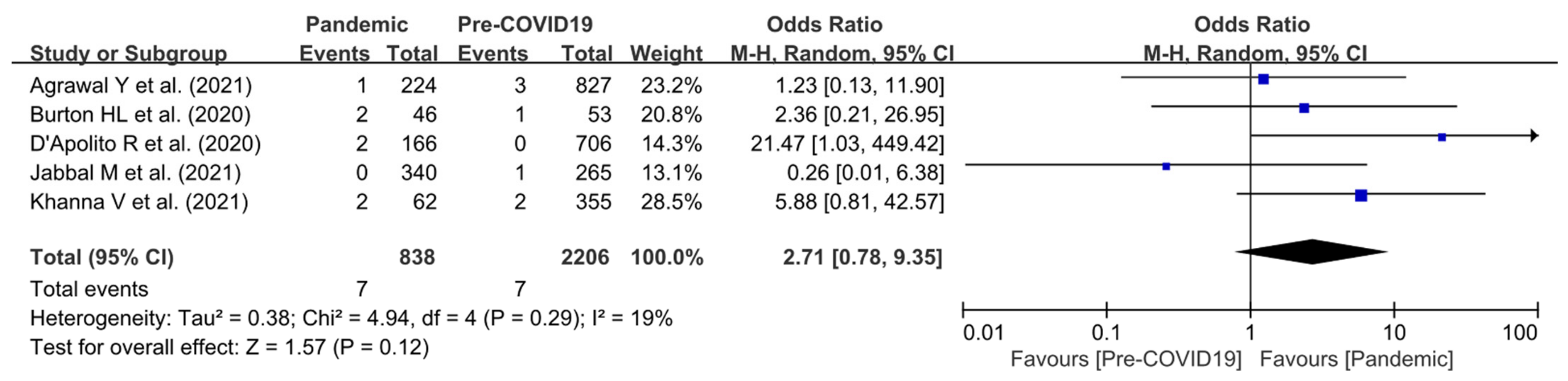
3.4.1. Overall Mortality Rate
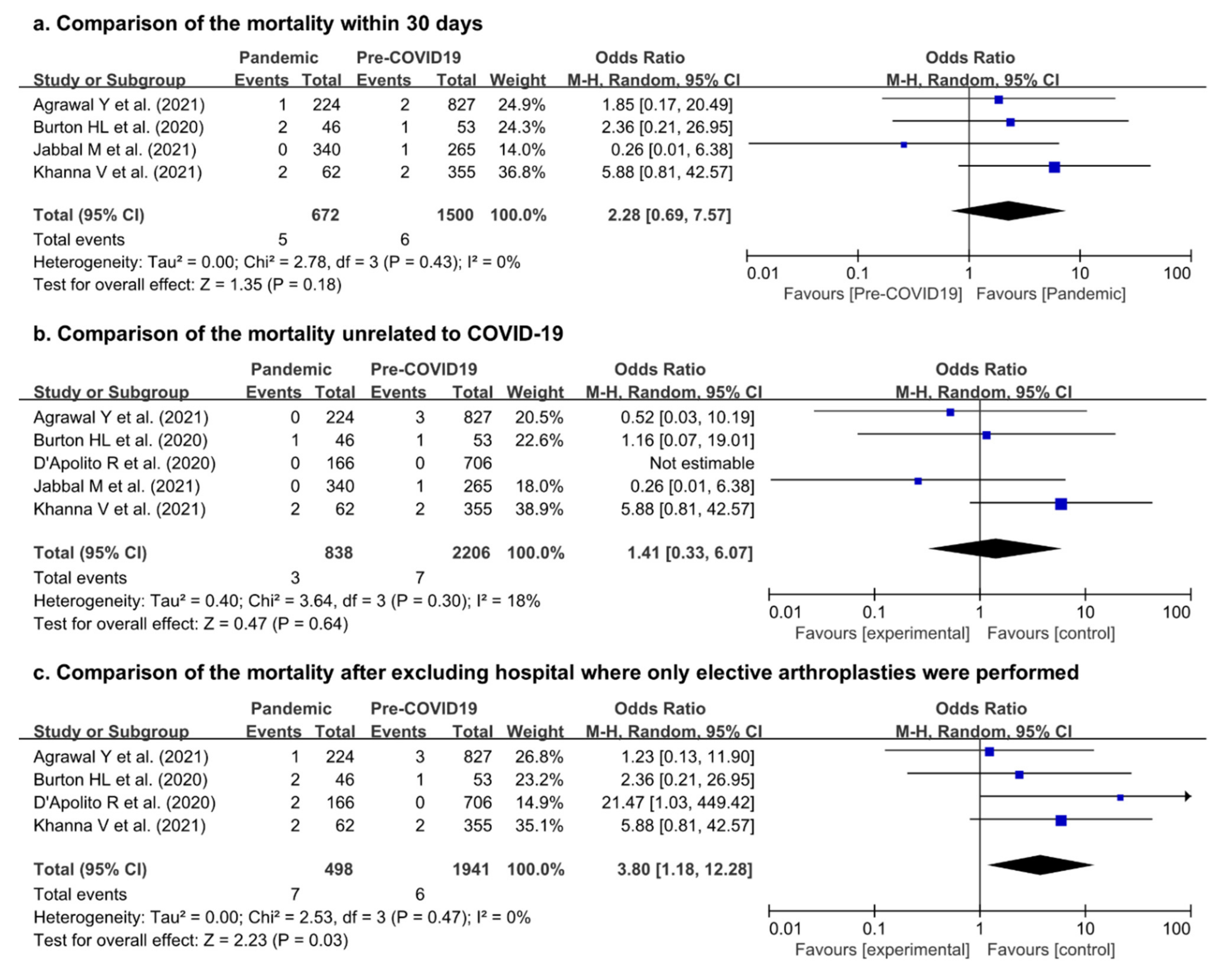
3.4.2. Subgroup Analyses for Mortality
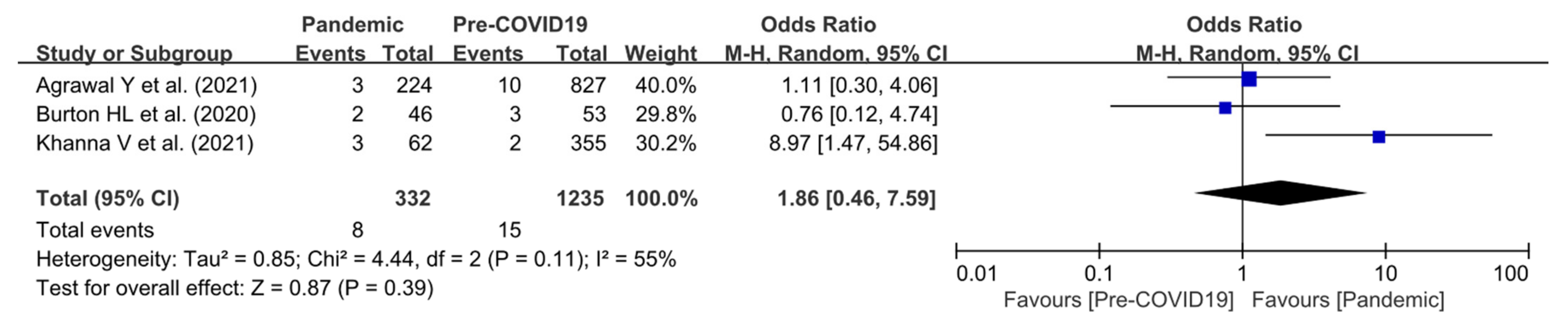
3.4.3. Readmission Rate within 30 Days
3.4.4. Comparison of Mortality Rate Following Hip and Knee Joint Arthroplasty in Each Country
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PubMed (19 March 2022). | ||
| Search Queries | Number of Articles | |
| #1 | “arthroplast * ” (Title/Abstract) | 77,820 |
| #2 | “arthroplasty” (MeSH Terms) OR “hemiarthroplasty” (MeSH Terms) | 80,950 |
| #3 | Search (#1 OR #2) | 107,943 |
| #4 | “COVID” (Title/Abstract) OR “SARS-COV-2” (Title/Abstract) | 223,760 |
| #5 | “COVID-19” (MeSH Terms) OR “SARS-COV-2” (MeSH Terms) | 148,502 |
| #6 | Search (#4 OR #5) | 233,472 |
| #7 | Search (#3 AND #6) | 216 |
| #8 | “mortalit *” (Title/Abstract) | 893,827 |
| #9 | “mortality” (MeSH Terms) | 416,458 |
| #10 | Search (#8 OR #9) | 1,149,574 |
| #11 | Search (#7 AND #10) | 28 |
| Embase (19 March 2022). | ||
| Search Queries | Number of Articles | |
| #1 | arthroplast *:ti,ab,kw | 91,951 |
| #2 | hemiarthroplast *:ti,ab,kw | 4517 |
| #3 | Search (#1 OR #2) | 93,979 |
| #4 | covid *:ti,ab,kw | 221,739 |
| #5 | COVID-19:ti,ab,kw | 217,672 |
| #6 | SARS-COV-2:ti,ab,kw | 81,114 |
| #7 | Search (#4 OR #5 OR #6) | 237,133 |
| #8 | mortalit *:ti,ab,kw | 1,315,660 |
| #9 | Search (#3 AND #7 AND #8) | 15 |
| Cochrane Library (19 March 2022). | ||
| Search Queries | Number of Articles | |
| #1 | arthroplast *:ti,ab,kw | 13,388 |
| #2 | hemiarthroplast *:ti,ab,kw | 529 |
| #3 | Search (#1 OR #2) | 13,611 |
| #4 | covid *:ti,ab,kw | 9797 |
| #5 | COVID-19:ti,ab,kw | 9308 |
| #6 | SARS-COV-2:ti,ab,kw | 3690 |
| #7 | Search (#4 OR #5 OR #6) | 9995 |
| #8 | mortalit *:ti,ab,kw | 94,978 |
| #9 | Search (#3 AND #7 AND #8) | 0 |
References
- Paul, K.D.; Levitt, E.; McGwin, G.; Brabston, E.W., 3rd; Gilbert, S.R.; Ponce, B.A.; Momaya, A.M. COVID-19 Impact on Orthopedic Surgeons: Elective Procedures, Telehealth, and Income. South. Med. J. 2021, 114, 311–316. [Google Scholar] [CrossRef] [PubMed]
- D’Apolito, R.; Faraldi, M.; Ottaiano, I.; Zagra, L. Disruption of Arthroplasty Practice in an Orthopedic Center in Northern Italy During the Coronavirus Disease 2019 Pandemic. J. Arthroplast. 2020, 35, S6–S9. [Google Scholar] [CrossRef] [PubMed]
- Forlenza, E.M.; Higgins, J.D.; Burnett, R.A.; Serino, J.; Della Valle, C.J. COVID-19 Infection After Total Joint Arthroplasty Is Associated With Increased Complications. J. Arthroplast. 2022, 37, S457–S464. [Google Scholar] [CrossRef] [PubMed]
- Stoneham, A.C.S.; Apostolides, M.; Bennett, P.M.; Hillier-Smith, R.; Witek, A.J.; Goodier, H.; Asp, R. Early outcomes of patients undergoing total hip arthroplasty for trauma during COVID-19. Bone Jt. Open 2020, 1, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, Y.; Vasudev, A.; Sharma, A.; Cooper, G.; Stevenson, J.; Parry, M.C.; Dunlop, D. Morbidity and mortality in patients undergoing lower limb arthroplasty surgery during the initial surge of the COVID-19 pandemic in the UK at a single-speciality orthopaedic hospital. Bone Jt. Open 2021, 2, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Khanna, V.; Nashikkar, P.S.; Mahajan, R.; Tripathi, S. Impact of Covid-19 pandemic on arthroplasty services and early experience after resuming surgeries at a ‘non Covid’ center. J. Clin. Orthop. Trauma 2021, 21, 101515. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, F.L.; Oh, I.S.; Hayes, T.L. Fixed- versus random-effects models in meta-analysis: Model properties and an empirical comparison of differences in results. Br. J. Math. Stat. Psychol. 2009, 62, 97–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, H.L.; Burden, E.; King, A.; Kassam, A.A.; Hubble, M.J.; Toms, A.D. Urgent Arthroplasty Interventions During the COVID-19 Pandemic: Operating Risks in Low-Prevalence Areas. Cureus 2020, 12, e12197. [Google Scholar] [CrossRef] [PubMed]
- Jabbal, M.; Campbel, N.; Savaridas, T.; Raza, A. Careful return to elective orthopaedic surgery in an acute hospital during the COVID-19 pandemic shows no increase in morbidity or mortality. Bone Jt. Open 2021, 2, 940–944. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, J.D.; Evans, S.; Morris, G.; Tillman, R.; Abudu, A.; Jeys, L.; Parry, M. Mortality of high-risk orthopaedic oncology patients during the COVID-19 pandemic: A prospective cohort study. J. Surg. Oncol. 2020, 122, 1027–1030. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, S.; Salottolo, K.; Madayag, R.; Pekarek, J.; Nwafo, N.; Wessel, A.; Duane, T.; Roberts, Z.; Lieser, M.; Corrigan, C.; et al. Delayed hospital admission for traumatic hip fractures during the COVID-19 pandemic. J. Orthop. Surg. Res. 2021, 16, 237. [Google Scholar] [CrossRef] [PubMed]
- Egol, K.A.; Konda, S.R.; Bird, M.L.; Dedhia, N.; Landes, E.K.; Ranson, R.A.; Solasz, S.J.; Aggarwal, V.K.; Bosco, J.A., 3rd; Furgiuele, D.L.; et al. Increased Mortality and Major Complications in Hip Fracture Care During the COVID-19 Pandemic: A New York City Perspective. J. Orthop. Trauma 2020, 34, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Dar, G.N.; Wani, M.I.; Mumtaz, M.U.; Kawoosa, A.A.; Ali, N. Delayed Fixation of Hip Fractures and Short-term Outcome in Coronavirus Positive Patients: A Prospective Cohort Study. J. Clin. Diagn. Res. 2021, 15, RC07–RC10. [Google Scholar] [CrossRef]
- Tripathy, S.K.; Varghese, P.; Panigrahi, S.; Panda, B.B.; Velagada, S.; Sahoo, S.S.; Naik, M.A.; Rao, S.K. Thirty-day mortality of patients with hip fracture during COVID-19 pandemic and pre-pandemic periods: A systematic review and meta-analysis. World J. Orthop. 2021, 12, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Tay, E. Hip fractures in the elderly: Operative versus nonoperative management. Singap. Med. J. 2016, 57, 178–181. [Google Scholar] [CrossRef]
- Ribeiro Xavier, C.; Sachetto Oliveira, R.; da Fonseca Vieira, V.; Lobosco, M.; Weber dos Santos, R. Characterisation of Omicron Variant during COVID-19 Pandemic and the Impact of Vaccination, Transmission Rate, Mortality, and Reinfection in South Africa, Germany, and Brazil. BioTech 2022, 11, 12. [Google Scholar] [CrossRef] [PubMed]





| Comparison | Reason for Exclusion | |
|---|---|---|
| De C. et al. (2021) [7] | Mortality after hip fracture (pandemic vs. pre-pandemic) | Impossible to extract the data of arthroplasty |
| Konda, S.R. et al. (2020) [3] | Mortality after hip fractures (COVID-19 infection vs. control) | Impossible to extract the data of arthroplasty |
| Malik-Tabassum, K. et al. (2021) [8] | Mortality after hip fracture (pandemic vs. pre-pandemic) | Impossible to extract the data of arthroplasty |
| Meena, O.P. et al. (2021) [9] | Mortality after arthroplasty for arthritis during pandemic period | No comparison between pandemic and pre-pandemic periods (single-arm study) |
| Slullitel, P.A. et al. (2020) [12] | Mortality after hip fracture (pandemic vs. pre-pandemic) | Impossible to extract the data of arthroplasty |
| Stoneham, A.C.S. et al. (2020) [4] | Mortality after arthroplasty for trauma during pandemic period | No comparison between pandemic and pre-pandemic periods (single-arm study) |
| Thakrar, A. et al. (2020) [13] | Mortality after hip fracture (pandemic vs. pre-pandemic) | Impossible to extract the data of arthroplasty |
| Wignall, A. et al. (2021) [10] | Mortality after hip fracture (pandemic vs. pre-pandemic) | Impossible to extract the data of arthroplasty |
| Author (Year) | Study Design | Country | Sample Size | Mean Age | Pandemic Study Period | Type of Arthroplasty | ||
|---|---|---|---|---|---|---|---|---|
| P | Pre-P | P | Pre-P | |||||
| Agrawal, Y. et al. (2021) [5] | RCS | UK | 224 | 827 | 69.4 (35 to 91) | 66.8 (17 to 96) | Mar/01/2020–May/31/2020 | Hip, knee |
| Burton, H.L. et al. (2020) [12] | RCS | UK | 46 | 53 | 78 (58 to 108) | 74.6 (45 to 88) | Apr/01/2020–Jun/16/2020 | Hip, knee |
| D’Apolito, R. et al. (2020) [2] | RCS | Italy | 166 | 706 | N/A | N/A | Feb//24/2020–Apr/10/2020 | Hip, knee |
| Jabbal, M. et al. (2021) [13] | RCS | UK | 340 | 265 | 68.5 (28 to 90) | N/A | Jul/01/2020–Jan/31/2021 | Hip, knee |
| Khanna, V. et al. (2021) [6] | RCS | India | 62 | 355 | 65.77 ± 12.26 | 64.23 ± 10.98 | Mar/01/2020–Aug/31/2020 | Hip, knee |
| Author (Year) | Urgency of Procedure | COVID-19 Screening | COVID-19 Positive | Death of COVID-19 Patients | MINORS Score | |
|---|---|---|---|---|---|---|
| P | Pre-P | |||||
| Agrawal, Y. et al. (2021) [5] | Elective (167) Urgent (57) | Elective (802) Urgent (24) | Early period: symptomatic patients Late period: all patients | 6/47 | 1 | 16 |
| Burton, H.L. et al. (2020) [12] | Elective (2) Urgent (44) | Elective (36) Urgent (17) | Early period: symptomatic patients Late period: all patients | 1/41 | 1 | 15 |
| D’Apolito, R. et al. (2020) [2] | Elective (159) Urgent (7) | Elective (625) Urgent (31) | Early period: symptomatic patients Late period: all patients | 2/NA | 2 | 15 |
| Jabbal, M. et al. (2021) [13] | Elective (340) | Elective (265) | All patients | 1/340 | 0 | 16 |
| Khanna, V. et al. (2021) [6] | Elective and urgent (62) | Elective and urgent (355) | All patients | 2/62 | 0 | 15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, E.J.; Kim, M.; Kim, C.-H. Impact of the COVID-19 Pandemic on Mortality Following Hip and Knee Joint Arthroplasty Surgeries: A Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 1441. https://doi.org/10.3390/jpm12091441
Lim EJ, Kim M, Kim C-H. Impact of the COVID-19 Pandemic on Mortality Following Hip and Knee Joint Arthroplasty Surgeries: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(9):1441. https://doi.org/10.3390/jpm12091441
Chicago/Turabian StyleLim, Eic Ju, Minboo Kim, and Chul-Ho Kim. 2022. "Impact of the COVID-19 Pandemic on Mortality Following Hip and Knee Joint Arthroplasty Surgeries: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 9: 1441. https://doi.org/10.3390/jpm12091441
APA StyleLim, E. J., Kim, M., & Kim, C. -H. (2022). Impact of the COVID-19 Pandemic on Mortality Following Hip and Knee Joint Arthroplasty Surgeries: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 12(9), 1441. https://doi.org/10.3390/jpm12091441