


Postoperative Intracranial Hemorrhage after an Endoscopic L5-S1 Laminectomy and Discectomy: A Case Report and Literature Review


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Background
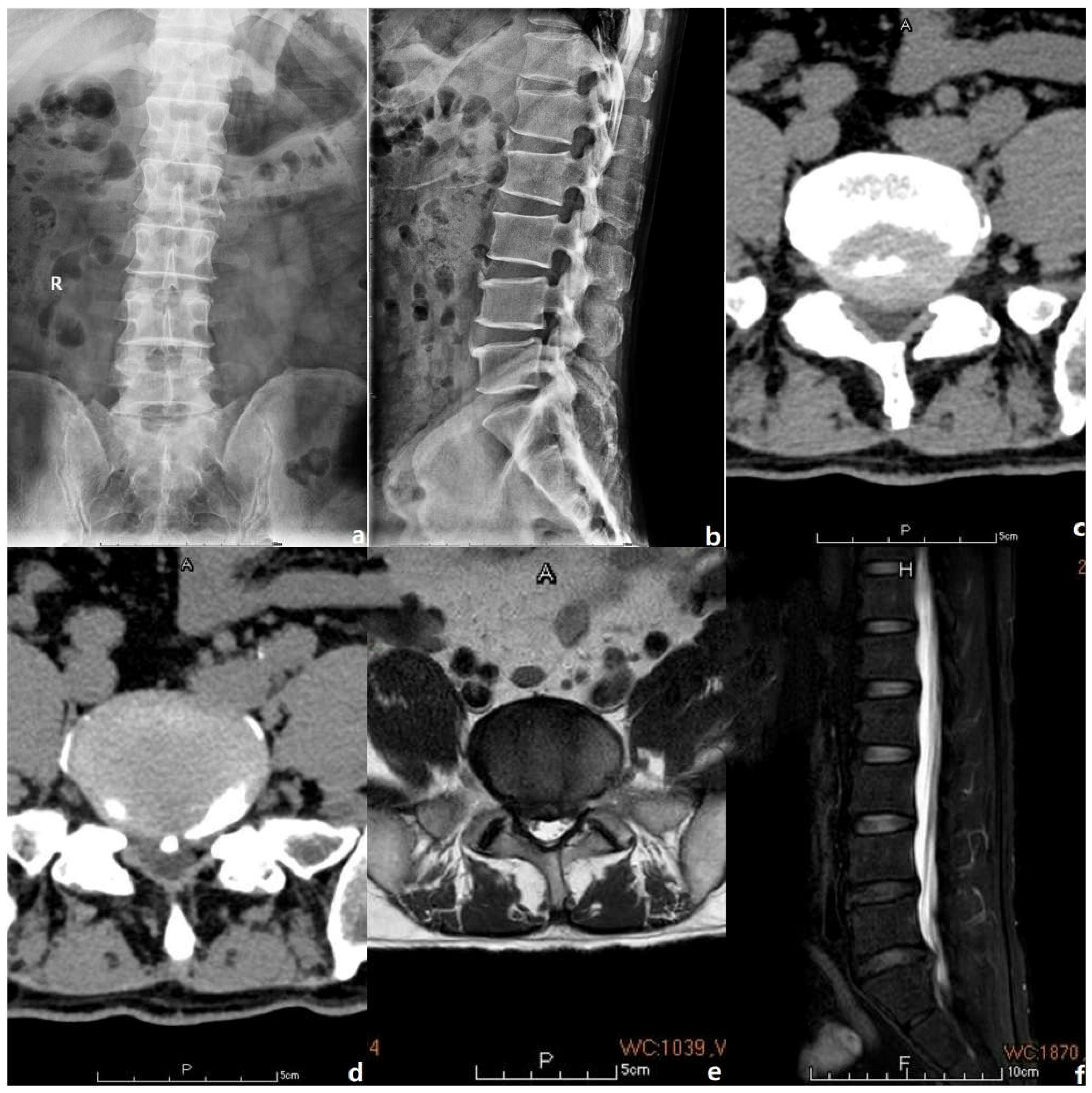
2. Case Presentation
2.1. Study Design
2.2. Basic Information
2.3. Operational Procedure
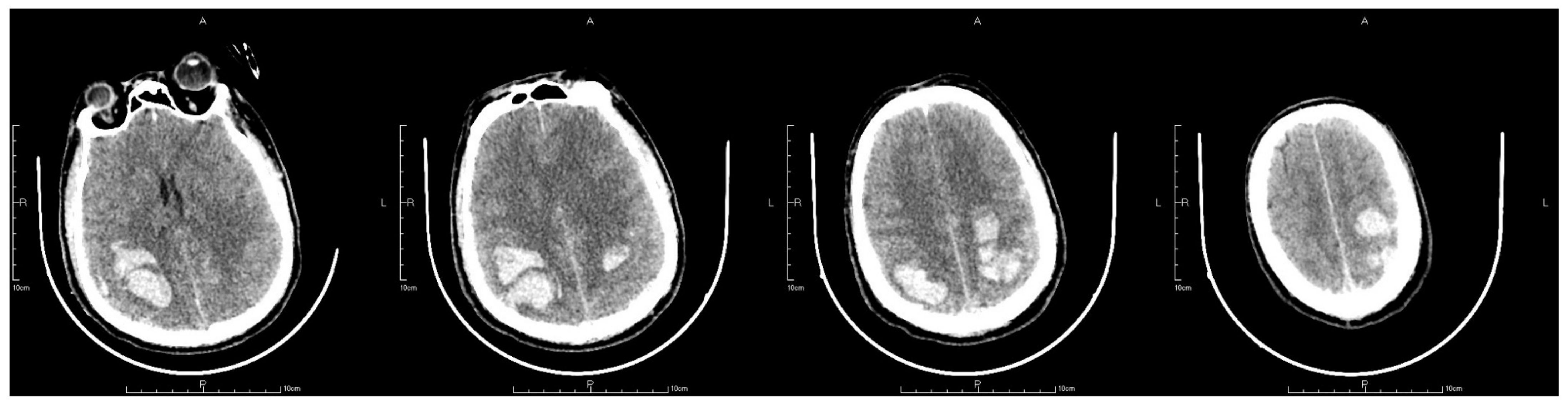
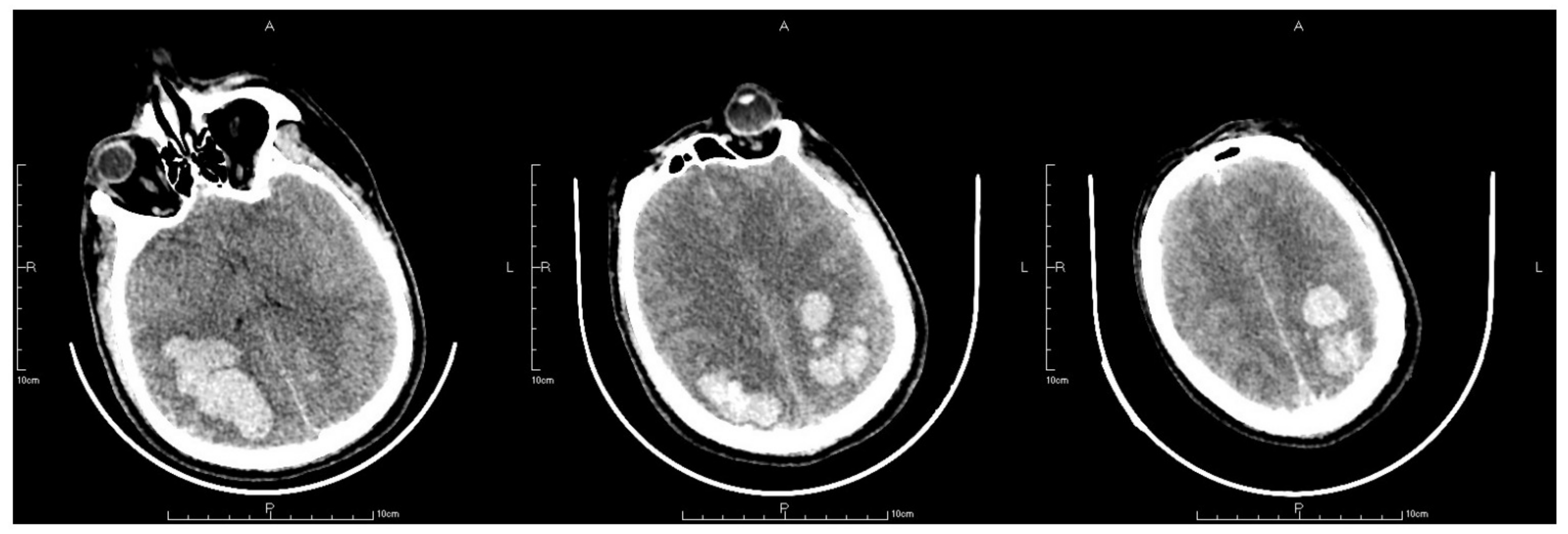
2.4. Postoperative Management
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, W.; Nolan, C.P.; Kumar, D.S.; Soh, R.C.C.; Oh, J.Y.-L. Intracerebral haemorrhage following spine surgery: A word of caution on the use of suction drains. Br. J. Neurosurg. 2021, 1–4. [Google Scholar] [CrossRef]
- Al-Saadi, T.; Al-Kindi, Y.; Allawati, M.; Al-Saadi, H. Intracranial Hemorrhage following Spinal Surgery: A Systematic Review of a Rare Complication. Surg. J. 2022, 8, e98–e107. [Google Scholar] [CrossRef]
- Hashidate, H.; Kamimura, M.; Nakagawa, H.; Takahara, K.; Uchiyama, S.; Kato, H. Cerebellar hemorrhage after spine surgery. J. Orthop. Sci. 2008, 13, 150–154. [Google Scholar] [CrossRef]
- Khalatbari, M.R.; Khalatbari, I.; Moharamzad, Y. Intracranial hemorrhage following lumbar spine surgery. Eur. Spine J. 2012, 21, 2091–2096. [Google Scholar] [CrossRef] [Green Version]
- Saxler, G.; Krämer, J.; Barden, B.; Kurt, A.; Pförtner, J.; Bernsman, K. The long-term clinical sequelae of incidental durotomy in lumbar disc surgery. Spine 2005, 30, 2298–2302. [Google Scholar] [CrossRef] [Green Version]
- Cammisa, F.P., Jr.; Girardi, F.P.; Sangani, P.K.; Parvataneni, H.K.; Cadag, S.; Sandhu, H.S. Incidental durotomy in spine surgery. Spine 2000, 25, 2663–2667. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, J.N.; Tosteson, T.D.; Lurie, J.D.; Tosteson, A.N.A.; Hanscom, B.; Skinner, J.S.; Abdu, W.A.; Hilibrand, A.S.; Boden, S.D.; Deyo, R.A. Surgical vs. nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT): A randomized trial. JAMA 2006, 296, 2441–2450. [Google Scholar] [CrossRef] [Green Version]
- De Noronha, R.J.; Sharrack, B.; Hadjivassiliou, M.; Romanowski, C.A.J. Subdural haematoma: A potentially serious consequence of spontaneous intracranial hypotension. J. Neurol. Neurosurg. Psychiatr. 2003, 74, 752–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francia, A.; Parisi, P.; Vitale, A.M.; Esposito, V. Life-threatening intracranial hypotension after diagnostic lumbar puncture. Neurol. Sci. 2001, 22, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Burkhard, P.R.; Duff, J.M. Bilateral subdural hematomas following routine lumbar diskectomy. Headache 2000, 40, 480–482. [Google Scholar] [CrossRef] [PubMed]
- Kaloostian, P.E.; Kim, J.E.; Bydon, A.; Sciubba, D.M.; Wolinsky, J.-P.; Gokaslan, Z.L.; Witham, T.F. Intracranial hemorrhage after spine surgery. J. Neurosurg. Spine 2013, 19, 370–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allouch, H.; Nahleh, K.A.; Mursch, K.; Shousha, M.; Alhashash, M.; Boehm, H. Symptomatic Intracranial Hemorrhage after Dural Tear in Spinal Surgery-A Series of 10 Cases and Review of the Literature. World Neurosurg. 2021, 150, e52–e65. [Google Scholar] [CrossRef]
- Hofler, R.C.; Wemhoff, M.P.; Johans, S.J.; Nockels, R.P. Cerebellar Hemorrhage Following an Uncomplicated Lumbar Spine Surgery: Case Report. J. Stroke Cereb. Dis. 2019, 28, e104–e105. [Google Scholar] [CrossRef] [PubMed]
- Beier, A.D.; Soo, T.M.; Claybrooks, R. Subdural hematoma after microdiscectomy: A case report and review of the literature. Spine J. 2009, 9, e9–e12. [Google Scholar] [CrossRef]
- Kuhn, J.; Hofmann, B.; Knitelius, H.O.; Coenen, H.H.; Bewermeyer, H. Bilateral subdural haematomata and lumbar pseudomeningocele due to a chronic leakage of liquor cerebrospinalis after a lumbar discectomy with the application of ADCON-L gel. J. Neurol. Neurosurg. Psychiatr. 2005, 76, 1031–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickerman, R.D.; Morgan, J. Acute intracranial subdural hematoma following a lumbar CSF leak caused by spine surgery. Spine 2006, 31, 1513–1514. [Google Scholar] [CrossRef]
- Schievink, W.I.; Meyer, F.B.; Atkinson, J.L.; Mokri, B. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. J. Neurosurg. 1996, 84, 598–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham, M.H.; Tuchman, A.; Platt, A.; Hsieh, P.C. Intracranial complications associated with spinal surgery. Eur. Spine J. 2016, 25, 888–894. [Google Scholar] [CrossRef]
- Floman, Y.; Millgram, M.A.; Ashkenazi, E.; Rand, N. Remote Cerebellar Hemorrhage Complicating Unintended Durotomy in Lumbar Spine Surgery. Int. J. Spine Surg. 2015, 9, 29. [Google Scholar] [CrossRef]
- Gaucher, D.J., Jr.; Perez, J.A., Jr. Subdural hematoma following lumbar puncture. Arch. Intern. Med. 2002, 162, 1904–1905. [Google Scholar] [CrossRef]
- Jang, J.W.; Lee, D.G.; Park, C.K. Rationale and Advantages of Endoscopic Spine Surgery. Int. J. Spine Surg. 2021, 15, S11–S20. [Google Scholar] [CrossRef] [PubMed]
- Choi, C.M. Biportal endoscopic spine surgery (BESS): Considering merits and pitfalls. J. Spine Surg. 2020, 6, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.G.; Kang, M.S.; Kim, S.Y.; Cho, K.C.; Na, Y.C.; Cho, J.M.; Jin, B.H. Dural Injury in Unilateral Biportal Endoscopic Spinal Surgery. Glob. Spine J. 2021, 11, 845–851. [Google Scholar] [CrossRef]
- Ahn, Y. Endoscopic spine discectomy: Indications and outcomes. Int. Orthop. 2019, 43, 909–916. [Google Scholar] [CrossRef]
- Chu, P.-L.; Wang, T.; Zheng, J.-L.; Xu, C.-Q.; Yan, Y.-J.; Ma, Q.-S.; Yin, M.-C.; Tian, D.-S. Global and Current Research Trends of Unilateral Biportal Endoscopy/Biportal Endoscopic Spinal Surgery in the Treatment of Lumbar Degenerative Diseases: A Bibliometric and Visualization Study. Orthop. Surg. 2022, 14, 635–643. [Google Scholar] [CrossRef]
- Joh, J.Y.; Choi, G.; Kong, B.-J.; Park, H.S.; Lee, S.-H.; Chang, S.H. Comparative study of neck pain in relation to increase of cervical epidural pressure during percutaneous endoscopic lumbar discectomy. Spine 2009, 34, 2033–2038. [Google Scholar] [CrossRef] [PubMed]
- Kirshner, H.; Schrag, M. Management of Intracerebral Hemorrhage: Update and Future Therapies. Curr. Neurol. Neurosci. Rep. 2021, 21, 57. [Google Scholar] [CrossRef]
- Shen, J.; Guo, F.; Yang, P.; Xu, F. Influence of hypertension classification on hypertensive intracerebral hemorrhage location. J. Clin. Hypertens. 2021, 23, 1992–1999. [Google Scholar] [CrossRef]
- Schrag, M.; Kirshner, H. Management of Intracerebral Hemorrhage: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 75, 1819–1831. [Google Scholar] [CrossRef]
- Elijovich, L.; Patel, P.V.; Hemphill, J.C., 3rd. Intracerebral hemorrhage. Semin. Neurol. 2008, 28, 657–667. [Google Scholar] [CrossRef] [Green Version]
- Telfeian, A.E.; Shen, J.; Ali, R.; Oyelese, A.; Fridley, J.; Gokaslan, Z.L. Incidence and Implications of Incidental Durotomy in Transforaminal Endoscopic Spine Surgery: Case Series. World Neurosurg. 2020, 134, e951–e955. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Raorane, H.D.; Wu, P.H.; Heo, D.H.; Sharma, S.B.; Jang, T., II. Incidental Durotomy during Endoscopic Stenosis Lumbar Decompression: Incidence, Classification, and Proposed Management Strategies. World Neurosurg. 2020, 139, e13–e22. [Google Scholar] [CrossRef]
- Pan, M.; Li, Q.; Li, S.; Mao, H.; Meng, B.; Zhou, F.; Yang, H. Percutaneous Endoscopic Lumbar Discectomy: Indications and Complications. Pain Physician 2020, 23, 49–56. [Google Scholar] [PubMed]
- Sen, R.D.; White-Dzuro, G.; Ruzevick, J.; Kim, C.W.; Witt, J.-P.; Telfeian, A.E.; Wang, M.Y.; Hofstetter, C.P. Intra- and Perioperative Complications Associated with Endoscopic Spine Surgery: A Multi-Institutional Study. World Neurosurg. 2018, 120, e1054–e1060. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.Y.; Ju, C.I.; Kim, S.W. Bilateral Subdural Hematoma due to an Unnoticed Dural Tear during Spine Surgery. J. Korean Neurosurg. Soc. 2010, 47, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-J.; Kim, S.-K.; Lee, S.-C.; Kim, W.; Han, S.; Kang, S.-S. Dural Tears in Percutaneous Biportal Endoscopic Spine Surgery: Anatomical Location and Management. World Neurosurg. 2020, 136, e578–e585. [Google Scholar] [CrossRef]
- Lewandrowski, K.-U.; Hellinger, S.; De Carvalho, P.S.T.; Ramos, M.R.F.; Soriano-SáNchez, J.-A.; Xifeng, Z.; Calderaro, A.L.; Dos Santos, T.S.; León, J.F.R.; de Lima e SilvA, M.S.; et al. Dural Tears During Lumbar Spinal Endoscopy: Surgeon Skill, Training, Incidence, Risk Factors, and Management. Int. J. Spine Surg. 2021, 15, 280–294. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, Y.; Mei, X.; Liu, S.; Fiani, B.; Fan, X.; Yu, Y. Postoperative Intracranial Hemorrhage after an Endoscopic L5-S1 Laminectomy and Discectomy: A Case Report and Literature Review. J. Pers. Med. 2023, 13, 196. https://doi.org/10.3390/jpm13020196
Xie Y, Mei X, Liu S, Fiani B, Fan X, Yu Y. Postoperative Intracranial Hemorrhage after an Endoscopic L5-S1 Laminectomy and Discectomy: A Case Report and Literature Review. Journal of Personalized Medicine. 2023; 13(2):196. https://doi.org/10.3390/jpm13020196
Chicago/Turabian StyleXie, Yizhou, Xi Mei, Shanyu Liu, Brian Fiani, Xiaohong Fan, and Yang Yu. 2023. "Postoperative Intracranial Hemorrhage after an Endoscopic L5-S1 Laminectomy and Discectomy: A Case Report and Literature Review" Journal of Personalized Medicine 13, no. 2: 196. https://doi.org/10.3390/jpm13020196
APA StyleXie, Y., Mei, X., Liu, S., Fiani, B., Fan, X., & Yu, Y. (2023). Postoperative Intracranial Hemorrhage after an Endoscopic L5-S1 Laminectomy and Discectomy: A Case Report and Literature Review. Journal of Personalized Medicine, 13(2), 196. https://doi.org/10.3390/jpm13020196