
Comparison of Transforaminal Lumbar Interbody Fusion in the Ambulatory Surgery Center and Traditional Hospital Settings, Part 1: Multi-Center Assessment of Surgical Safety




Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gerling, M.C.; Hale, S.D.; White-Dzuro, C.; Pierce, K.E.; Naessig, S.A.; Ahmad, W.; Passias, P.G. Ambulatory spine surgery. J. Spine Surg. 2019, 5 (Suppl. S2), S147–S153. [Google Scholar] [CrossRef] [PubMed]
- Pendharkar, A.V.; Shahin, M.N.; Ho, A.L.; Sussman, E.S.; Purger, D.A.; Veeravagu, A.; Ratliff, J.K.; Desai, A.M. Outpatient spine surgery: Defining the outcomes, value, and barriers to implementation. Neurosurg. Focus 2018, 44, E11. [Google Scholar] [CrossRef] [PubMed]
- Sivaganesan, A.; Hirsch, B.; Phillips, F.M.; McGirt, M.J. Spine Surgery in the Ambulatory Surgery Center Setting: Value-Based Advancement or Safety Liability? Neurosurgery 2018, 83, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Witiw, C.D.; Wilson, J.R.; Fehlings, M.G.; Traynelis, V.C. Ambulatory Surgical Centers: Improving Quality of Operative Spine Care? Global Spine J. 2020, 10 (Suppl. S1), 29S–35S. [Google Scholar] [CrossRef]
- Park, J.; Ham, D.W.; Kwon, B.T.; Park, S.M.; Kim, H.J.; Yeom, J.S. Minimally Invasive Spine Surgery: Techniques, Technologies, and Indications. Asian Spine J. 2020, 14, 694–701. [Google Scholar] [CrossRef]
- Vaishnav, A.S.; Othman, Y.A.; Virk, S.S.; Gang, C.H.; Qureshi, S.A. Current state of minimally invasive spine surgery. J. Spine Surg. 2019, 5 (Suppl. S1), S2–S10. [Google Scholar] [CrossRef] [PubMed]
- Lewandrowski, K.U.; Ferrara, L.; Cheng, B. Expandable Interbody Fusion Cages: An Editorial on the Surgeon’s Perspective on Recent Technological Advances and Their Biomechanical Implications. Int. J. Spine Surg. 2020, 14, S56–S62. [Google Scholar] [CrossRef]
- Heemskerk, J.L.; Oluwadara Akinduro, O.; Clifton, W.; Quinones-Hinojosa, A.; Abode-Iyamah, K.O. Long-term clinical outcome of minimally invasive versus open single-level transforaminal lumbar interbody fusion for degenerative lumbar diseases: A meta-analysis. Spine J. 2021, 21, 2049–2065. [Google Scholar] [CrossRef]
- Schlesinger, S.; Krugman, K.; Abbott, D.; Arle, J. Thirty-Day Outcomes from Standalone Minimally Invasive Surgery-Transforaminal Lumbar Interbody Fusion Patients in an Ambulatory Surgery Center vs. Hospital Setting. Cureus 2020, 12, e10197. [Google Scholar] [CrossRef]
- Smith, W.D.; Wohns, R.N.; Christian, G.; Rodgers, E.J.; Rodgers, W.B. Outpatient Minimally Invasive Lumbar Interbody: Fusion Predictive Factors and Clinical Results. Spine 2016, 41 (Suppl. S8), S106–S122. [Google Scholar] [CrossRef]
- Villavicencio, A.T.; Nelson, E.L.; Mason, A.; Rajpal, S.; Burneikiene, S. Preliminary results on feasibility of outpatient instrumented transforaminal lumbar interbody fusion. J. Spinal Disord. Tech. 2013, 26, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Emstad, E.; Del Monaco, D.C.; Fielding, L.C.; Block, J.E. The VariLift((R)) Interbody Fusion System: Expandable, standalone interbody fusion. Med. Devices 2015, 8, 219–230. [Google Scholar] [CrossRef]
- Bovonratwet, P.; Ottesen, T.D.; Gala, R.J.; Rubio, D.R.; Ondeck, N.T.; McLynn, R.P.; Grauer, J.N. Outpatient elective posterior lumbar fusions appear to be safely considered for appropriately selected patients. Spine J. 2018, 18, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Garcia, R.M.; Khanna, R.; Dahdaleh, N.S.; Cybulski, G.; Lam, S.; Smith, Z.A. Thirty-Day Readmission Risk Factors Following Single-Level Transforaminal Lumbar Interbody Fusion (TLIF) for 4992 Patients From the ACS-NSQIP Database. Global Spine J. 2017, 7, 220–226. [Google Scholar] [CrossRef]
- Dai, Z.; Feng, D.P.; Wu, K.L.; Zhu, J.Y.; Li, Z.W. Hidden blood loss of minimally invasive hybrid lumbar interbody fusion: An analysis of influencing factors. BMC Musculoskelet Disord. 2022, 23, 1099. [Google Scholar] [CrossRef]
- Patel, A.A.; Zfass-Mendez, M.; Lebwohl, N.H.; Wang, M.Y.; Green, B.A.; Levi, A.D.; Vanni, S.; Williams, S.K. Minimally Invasive Versus Open Lumbar Fusion: A Comparison of Blood Loss, Surgical Complications, and Hospital Course. Iowa Orthop. J. 2015, 35, 130–134. [Google Scholar]
- Senker, W.; Gruber, A.; Gmeiner, M.; Stefanits, H.; Sander, K.; Rossler, P.; Pflugmacher, R. Surgical and Clinical Results of Minimally Invasive Spinal Fusion Surgery in an Unselected Patient Cohort of a Spinal Care Unit. Orthop. Surg. 2018, 10, 192–197. [Google Scholar] [CrossRef]
- Zhou, Y.; Fu, X.; Yang, M.; Ke, S.; Wang, B.; Li, Z. Hidden blood loss and its possible risk factors in minimally invasive transforaminal lumbar interbody fusion. J. Orthop. Surg. Res. 2020, 15, 445. [Google Scholar] [CrossRef]
- Hammad, A.; Wirries, A.; Ardeshiri, A.; Nikiforov, O.; Geiger, F. Open versus minimally invasive TLIF: Literature review and meta-analysis. J. Orthop. Surg. Res. 2019, 14, 229. [Google Scholar] [CrossRef]
- Hu, S.S. Blood loss in adult spinal surgery. Eur. Spine J. 2004, 13 (Suppl. S1), S3–S5. [Google Scholar] [CrossRef]
- Lei, F.; Li, Z.; He, W.; Tian, X.; Zheng, L.; Kang, J.; Feng, D. Total and hidden blood loss between open posterior lumbar interbody fusion and transforaminal lumbar interbody fusion by Wiltse approach. Medicine 2020, 99, e19864. [Google Scholar] [CrossRef]
- Calvo-Echenique, A.; Cegonino, J.; Perez Del Palomar, A. Is there any advantage of using stand-alone cages? A numerical approach. Biomed. Eng. Online 2019, 18, 63. [Google Scholar] [CrossRef] [PubMed]
- Shuman, W.H.; Baron, R.B.; Neifert, S.N.; Martini, M.L.; Chapman, E.K.; Schupper, A.J.; Caridi, J.M.; Steinberger, J. MIS-TLIF Procedure is Improving with Experience: Systematic Review of the Learning Curve over the Last Decade. Clin. Spine Surg. 2022, 35, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Barrett-Tuck, R.; Del Monaco, D.; Block, J.E. One and two level posterior lumbar interbody fusion (PLIF) using an expandable, stand-alone, interbody fusion device: A VariLift((R)) case series. J. Spine Surg. 2017, 3, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Neely, W.F.; Fichtel, F.; Del Monaco, D.C.; Block, J.E. Treatment of Symptomatic Lumbar Disc Degeneration with the VariLift-L Interbody Fusion System: Retrospective Review of 470 Cases. Int. J. Spine Surg. 2016, 10, 15. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | ASC (n = 53) | In-Hospital (n = 114) | p-Value |
|---|---|---|---|
| Female, n (%) | 29 (55) | 60 (53) | 0.87 |
| Age, mean (SD) yrs | 51 (9.8) | 63 (13.0) | 0.001 |
| BMI, mean (SD) kg/m2 | 29 (4.5) | 28 (5.1) | 0.39 |
| Smoker, n (%) | 16 (31) | 32 (28) | 0.77 |
| Primary Diagnosis, n (%) | |||
| Degenerative Disc Disease | 0 (0.0) | 15 (13) | 0.001 |
| Spondylolisthesis | 1 (2) | 15 (13) | |
| Spinal Stenosis | 52 (98) | 81 (71) | |
| Other | 0 (0.0) | 3 (3) | |
| Prior Spine Surgery, n (%) | 23 (43) | 71 (62) | 0.03 |
| Adjacent-level Fusion, n (%) | 6 (11) | 20 (18) | 0.36 |
| Charlson Index, n (%) | |||
| 0 | 19 (36) | 18 (16) | 0.01 |
| 1 | 14 (26) | 12 (11) | |
| 2 | 16 (30) | 23 (20) | |
| 3 | 2 (4) | 35 (31) | |
| 4 | 1 (2) | 20 (18) | |
| 5 | 1 (2) | 4 (4) | |
| 6 | 0 (0) | 2 (2) | |
| ASA Grade, n (%) | |||
| I | 2 (4) | 0 (0) | 0.003 |
| II | 36 (68) | 59 (52) | |
| III | 12 (23) | 52 (46) | |
| IV | 0 (0) | 1 (1) | |
| Functional Status, n (%) | |||
| Ambulatory | 53 (100) | 109 (96) | 0.33 |
| Wheelchair | 0 (0) | 5 (4) | |
| Leg Pain Score, median (range) | 8 (1–8) | 7 (1–9) | 0.36 |
| Back Pain Score, median (range) | 5 (1–7) | 7 (1–9) | 0.49 |
| Variable | ASC (n = 53) | In-Hospital (n = 114) | p-Value |
|---|---|---|---|
| Treated Level, n (%) | |||
| L2–3 | 0 (0) | 7 (5) | 0.003 |
| L3–4 | 4 (7) | 24 (18) | |
| L4–5 | 20 (37) | 63 (47) | |
| L5–S1 | 30 (56) | 39 (29) | |
| No. of Levels, n (%) | |||
| 1 | 52 (98) | 95 (83) | 0.004 |
| 2 | 1 (2) | 19 (17) | |
| Supplemental Fixation, n (%) | 3 (6) | 12 (11) | 0.79 |
| Blood Loss, median (range) cc | 250 (25–1100) | 100 (19–1000) | 0.001 |
| Transfusion, n (%) | 0 (0) | 2 (2) | 0.48 |
| Operative Duration, mean (SD) hrs | 2.1 (0.5) | 1.8 (0.7) | 0.008 |
| Complications, n (%) | 4 (8) | 17 (15) | 0.14 |
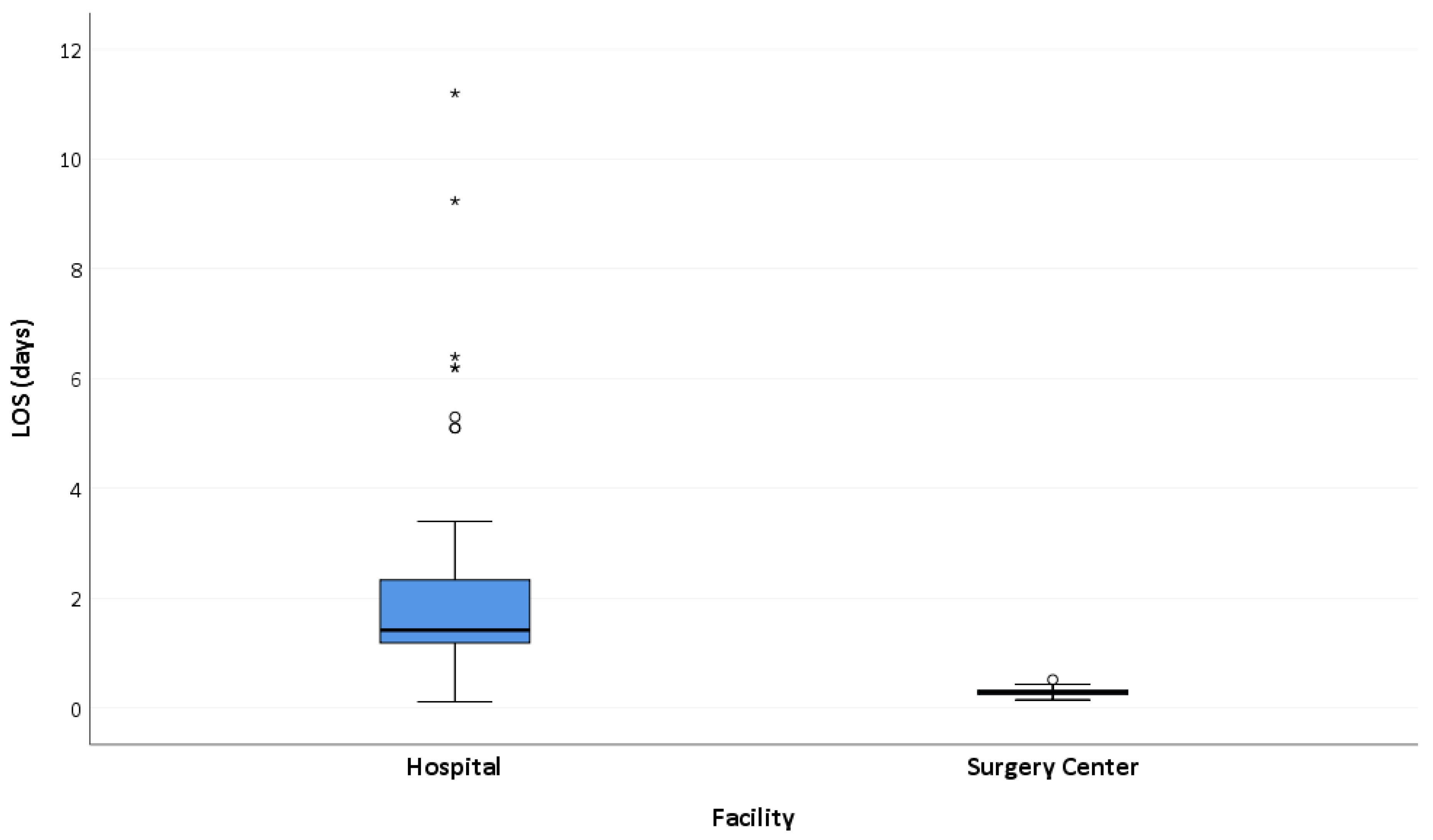
| Length of Stay, median (SD) days | 0.3 (0.15–0.52) | 1.4 (0.11–11.2) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schlesinger, S.M.; Gelber, B.R.; Gerber, M.B.; Lorio, M.P.; Block, J.E. Comparison of Transforaminal Lumbar Interbody Fusion in the Ambulatory Surgery Center and Traditional Hospital Settings, Part 1: Multi-Center Assessment of Surgical Safety. J. Pers. Med. 2023, 13, 311. https://doi.org/10.3390/jpm13020311
Schlesinger SM, Gelber BR, Gerber MB, Lorio MP, Block JE. Comparison of Transforaminal Lumbar Interbody Fusion in the Ambulatory Surgery Center and Traditional Hospital Settings, Part 1: Multi-Center Assessment of Surgical Safety. Journal of Personalized Medicine. 2023; 13(2):311. https://doi.org/10.3390/jpm13020311
Chicago/Turabian StyleSchlesinger, Scott M., Benjamin R. Gelber, Mark B. Gerber, Morgan P. Lorio, and Jon E. Block. 2023. "Comparison of Transforaminal Lumbar Interbody Fusion in the Ambulatory Surgery Center and Traditional Hospital Settings, Part 1: Multi-Center Assessment of Surgical Safety" Journal of Personalized Medicine 13, no. 2: 311. https://doi.org/10.3390/jpm13020311
APA StyleSchlesinger, S. M., Gelber, B. R., Gerber, M. B., Lorio, M. P., & Block, J. E. (2023). Comparison of Transforaminal Lumbar Interbody Fusion in the Ambulatory Surgery Center and Traditional Hospital Settings, Part 1: Multi-Center Assessment of Surgical Safety. Journal of Personalized Medicine, 13(2), 311. https://doi.org/10.3390/jpm13020311