

Assessment of Amikacin- and Capreomycin-Related Adverse Drug Reactions in Patients with Multidrug-Resistant Tuberculosis and Exploring the Role of Genetic Factors
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Full mtDNA Genome Sequencing
2.3. Statistics
3. Results
3.1. Otoxicity and Nephrotoxicity Occurrence Rates in Patients with MDR-TB
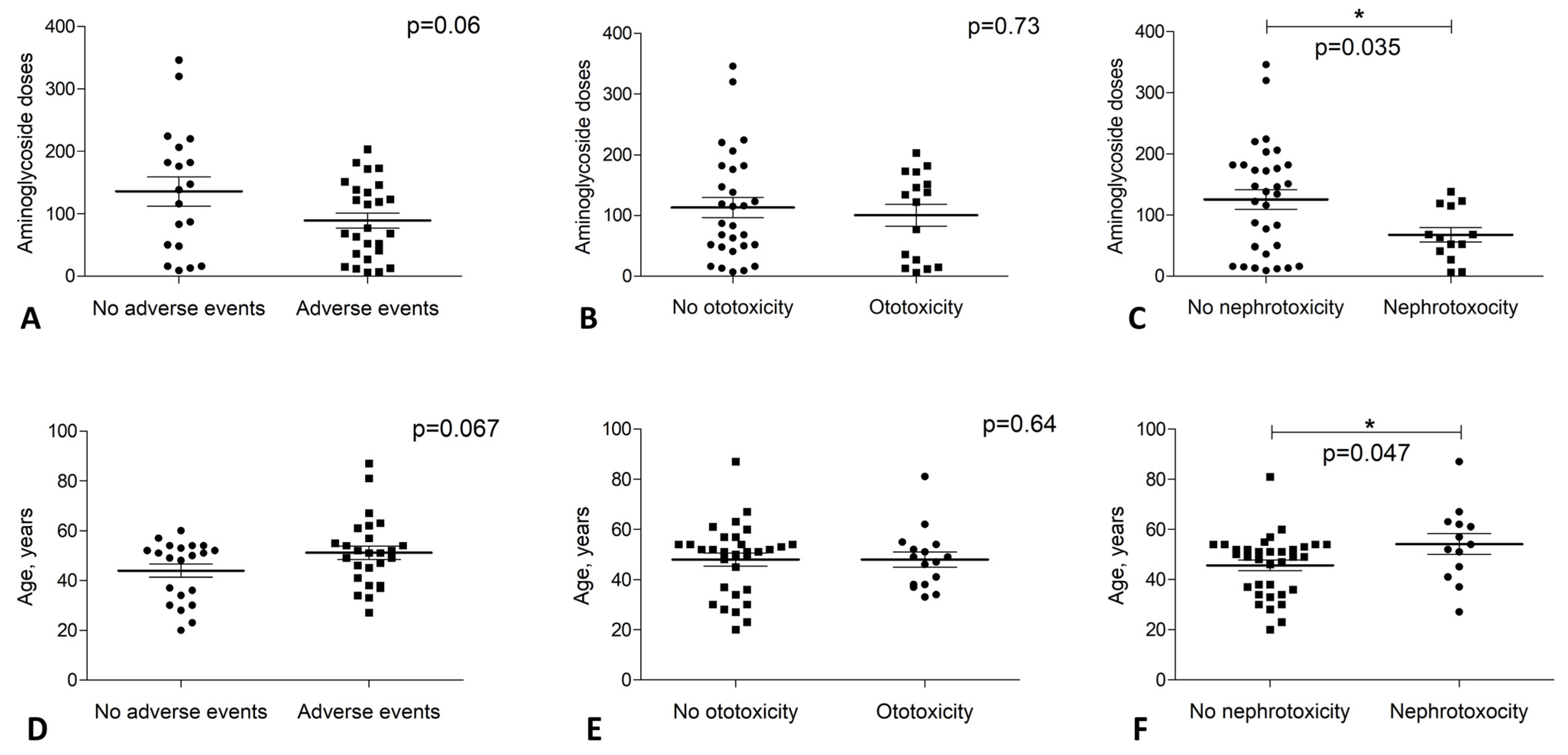
3.2. Ototoxicity Events Were Not Associated with Treatment Duration
3.3. Nephrotoxicity Events Mostly Occurred at the Beginning of the TB Treatment
3.4. Nephrotoxicity Events Were Age-Related
3.5. Amikacin Use Was Associated with Ototoxicity Development in Patients with MDR-TB
3.6. Factor Analysis for Nephrotoxicity Occurrence
3.7. Full mtDNA Genome Sequencing Did Not Show Mitochondrial Association with ADR Occurrence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Tuberculosis. Available online: https://www.who.int/news-room/fact-sheets/detail/tuberculosis (accessed on 10 October 2022).
- World Health Organization. Meeting Report of the WHO Expert Consultation on the Definition of Extensively Drug-Resistant Tuberculosis, 27–29 October 2020; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-001866-2. [Google Scholar]
- World Health Organization. Global Tuberculosis Report 2022; World Health Organization: Geneva, Switzerland, 2022; ISBN 978-92-4-006172-9. [Google Scholar]
- World Health Organization. Global Tuberculosis Report 2019; World Health Organization: Geneva, Switzerland, 2019; ISBN 978-92-4-156571-4. [Google Scholar]
- MacDougall, C. Aminoglycosides. In Goodman & Gilman’s: The Pharmacological Basis of Therapeutics, 13rd ed.; Brunton, L.L., Hilal-Dandan, R., Knollmann, B.C., Eds.; McGraw-Hill Education: New York, NY, USA, 2017. [Google Scholar]
- Jiang, M.; Karasawa, T.; Steyger, P.S. Aminoglycoside-Induced Cochleotoxicity: A Review. Front. Cell. Neurosci. 2017, 11, 308. [Google Scholar] [CrossRef] [Green Version]
- Xie, Y.; Nishi, S.; Iguchi, S.; Imai, N.; Sakatsume, M.; Saito, A.; Ikegame, M.; Iino, N.; Shimada, H.; Ueno, M.; et al. Expression of Osteopontin in Gentamicin-Induced Acute Tubular Necrosis and Its Recovery Process. Kidney Int. 2001, 59, 959–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthrie, O.W. Aminoglycoside Induced Ototoxicity. Toxicology 2008, 249, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.F.P.; Silva, C.A.; Barbieri, C.D.; Oliveira, G.M.; Zanetta, D.M.T.; Burdmann, E.A. Prevalence and Risk Factors for Aminoglycoside Nephrotoxicity in Intensive Care Units. Antimicrob. Agents Chemother. 2009, 53, 2887–2891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Society of Health-System Pharmacists. AHFS Drug Information 2008; American Society of Health-System Pharmacists: Bethesda, MD, USA, 2008; ISBN 9781585282067/1585282065. [Google Scholar]
- Lanvers-Kaminsky, C.; Ciarimboli, G. Pharmacogenetics of Drug-Induced Ototoxicity Caused by Aminoglycosides and Cisplatin. Pharmacogenomics 2017, 18, 1683–1695. [Google Scholar] [CrossRef]
- Prezant, T.R.; Agapian, J.V.; Bohlman, M.C.; Bu, X.; Öztas, S.; Qiu, W.-Q.; Arnos, K.S.; Cortopassi, G.A.; Jaber, L.; Rotter, J.I.; et al. Mitochondrial Ribosomal RNA Mutation Associated with Both Antibiotic–Induced and Non–Syndromic Deafness. Nat. Genet. 1993, 4, 289. [Google Scholar] [CrossRef]
- Zhao, H.; Li, R.; Wang, Q.; Yan, Q.; Deng, J.-H.; Han, D.; Bai, Y.; Young, W.-Y.; Guan, M.-X. Maternally Inherited Aminoglycoside-Induced and Nonsyndromic Deafness Is Associated with the Novel C1494T Mutation in the Mitochondrial 12S RRNA Gene in a Large Chinese Family. Am. J. Hum. Genet. 2004, 74, 139–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, L.; Young, W.Y.; Li, R.; Wang, Q.; Qian, Y.; Guan, M.X. Clinical Evaluation and Sequence Analysis of the Complete Mitochondrial Genome of Three Chinese Patients with Hearing Impairment Associated with the 12S RRNA T1095C Mutation. Biochem. Biophys. Res. Commun. 2004, 325, 1503–1508. [Google Scholar] [CrossRef]
- Rovite, V.; Wolff-Sagi, Y.; Zaharenko, L.; Nikitina-Zake, L.; Grens, E.; Klovins, J. Genome Database of the Latvian Population (LGDB): Design, Goals, and Primary Results. J. Epidemiol. 2018, 28, 353–360. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Treatment Guidelines for Drug Resistant Tuberculosis 2016 Update; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-154963-9. [Google Scholar]
- World Health Organization. Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis; World Health Organization: Geneva, Switzerland, 2014; ISBN 978-92-4-154880-9. [Google Scholar]
- Fendt, L.; Zimmermann, B.; Daniaux, M.; Parson, W. Sequencing Strategy for the Whole Mitochondrial Genome Resulting in High Quality Sequences. BMC Genom. 2009, 10, 139. [Google Scholar] [CrossRef] [Green Version]
- Afgan, E.; Baker, D.; Bér´, B.; Batut, B.; van den Beek, M.; Bouvier, D.; Cech, M.; Chilton, J.; Clements, D.; Coraor, N.; et al. The Galaxy Platform for Accessible, Reproducible and Collaborative Biomedical Analyses: 2018 Update. Nucleic Acids Res. 2018, 46, 537–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nekrutenko, A.; Ostrovsky, A. Calling Variants in Non-Diploid Systems (Galaxy Training Materials). Available online: https://training.galaxyproject.org/archive/2021-10-01/topics/variant-analysis/tutorials/non-dip/tutorial.html (accessed on 11 May 2022).
- Robinson, J.T.; Thorvaldsdóttir, H.; Winckler, W.; Guttman, M.; Lander, E.S.; Getz, G.; Mesirov, J.P. Integrative Genomics Viewer. Nat. Biotechnol. 2011, 29, 24–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weissensteiner, H.; Pacher, D.; Kloss-Brandstätter, A.; Brandstätter, B.; Forer, L.; Unther Specht, G.; Urgen Bandelt, H.-J.; Kronenberg, F.; Salas, A.; Schönherr, S.; et al. HaploGrep 2: Mitochondrial Haplogroup Classification in the Era of High-Throughput Sequencing. Nucleic Acids Res. 2016, 44, W58–W63. [Google Scholar] [CrossRef] [PubMed]
- Preste, R.; Vitale, O.; Clima, R.; Gasparre, G.; Attimonelli, M. HmtVar: A New Resource for Human Mitochondrial Variations and Pathogenicity Data. Nucleic Acids Res. 2019, 47, D1202–D1210. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Pesini, E.; Lott, M.T.; Procaccio, V.; Poole, J.C.; Brandon, M.C.; Mishmar, D.; Yi, C.; Kreuziger, J.; Baldi, P.; Wallace, D.C. An Enhanced MITOMAP with a Global MtDNA Mutational Phylogeny. Nucleic Acids Res. 2007, 35 (Suppl. 1), D823–D828. [Google Scholar] [CrossRef] [Green Version]
- Barkāne, L.; Tuberculosis and Lung Diseases Center, Riga East Clinical University Hospital, Riga, Latvia. Personal communication, 2022.
- Tessa, A.; Giannotti, A.; Tieri, L.; Vilarinho, L.; Marotta, G.; Santorelli, F.M. Maternally Inherited Deafness Associated with a T1095C Mutation in the MDNA. Eur. J. Hum. Genet. 2001, 9, 147–149. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Greinwald, J.H.; Yang, L.; Choo, D.I.; Wenstrup, R.J.; Guan, M.-X. Molecular Analysis of the Mitochondrial 12S rRNA and tRNASer(UCN) Genes in Paediatric Subjects with Non-Syndromic Hearing Loss. J. Med. Genet. 2004, 41, 615–620. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, M.; Shintani, T.; Hirao, M.; Himi, T.; Yamaguchi, A.; Kikuchi, K. Aminoglycoside-Induced Hearing Loss in a Patient with the 961 Mutation in Mitochondrial DNA. ORL 2002, 64, 219–222. [Google Scholar] [CrossRef]
- Xing, G.; Chen, Z.; Wei, Q.; Tian, H.; Li, X.; Zhou, A.; Bu, X.; Cao, X. Maternally Inherited Non-Syndromic Hearing Loss Associated with Mitochondrial 12S RRNA A827G Mutation in a Chinese Family. Biochem. Biophys. Res. Commun. 2006, 344, 1253–1257. [Google Scholar] [CrossRef]
- Jing, W.; Zongjie, H.; Denggang, F.; Na, H.; Bin, Z.; Aifen, Z.; Xijiang, H.; Cong, Y.; Yunping, D.; Ring, H.Z.; et al. Mitochondrial Mutations Associated with Aminoglycoside Ototoxicity and Hearing Loss Susceptibility Identified by Meta-Analysis. J. Med. Genet. 2015, 52, 95–103. [Google Scholar] [CrossRef]
- Ding, Y.; Leng, J.; Fan, F.; Xia, B.; Xu, P. The Role of Mitochondrial DNA Mutations in Hearing Loss. Biochem. Genet. 2013, 51, 588–602. [Google Scholar] [CrossRef] [PubMed]
- Dillard, L.K.; Martinez, R.X.; Perez, L.L.; Fullerton, A.M.; Chadha, S.; McMahon, C.M. Prevalence of Aminoglycoside-Induced Hearing Loss in Drug-Resistant Tuberculosis Patients: A Systematic Review. J. Infect. 2021, 83, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Arnold, A.; Cooke, G.S.; Kon, O.M.; Dedicoat, M.; Lipman, M.; Loyse, A.; Chis Ster, I.; Harrison, T.S. Adverse Effects and Choice between the Injectable Agents Amikacin and Capreomycin in Multidrug-Resistant Tuberculosis. Antimicrob. Agents Chemother. 2017, 61, e02586-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melchionda, V.; Wyatt, H.; Capocci, S.; Garcia Medina, R.; Solamalai, A.; Katiri, S.; Hopkins, S.; Cropley, I.; Lipman, M. Amikacin Treatment for Multidrug Resistant Tuberculosis: How Much Monitoring Is Required? Eur. Respir. J. 2013, 42, 1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.-H.; Chung, J.; Lee, M.Y.; Lee, D.Y.; Kim, Y.H. Cochlear Damage Caused by the Striking Noise of Titanium Head Golf Driver. Clin. Exp. Otorhinolaryngol. 2019, 12, 18–26. [Google Scholar] [CrossRef]
- Hong, H.; Dooley, K.E.; Starbird, L.E.; Francis, H.W.; Farley, J.E. Adverse Outcome Pathway for Aminoglycoside Ototoxicity in Drug-Resistant Tuberculosis Treatment. Arch. Toxicol. 2019, 93, 1385–1399. [Google Scholar] [CrossRef]
- Huth, M.E.; Ricci, A.J.; Cheng, A.G. Mechanisms of Aminoglycoside Ototoxicity and Targets of Hair Cell Protection. Int. J. Otolaryngol. 2011. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Qian, Y.; Tang, X.; Wang, J.; Yang, L.; Liao, Z.; Li, R.; Ji, J.; Li, Z.; Chen, J.; et al. Aminoglycoside-Induced and Non-Syndromic Hearing Loss Is Associated with the G7444A Mutation in the Mitochondrial COI/TRNASer(UCN) Genes in Two Chinese Families. Biochem. Biophys. Res. Commun. 2006, 342, 843–850. [Google Scholar] [CrossRef]
- Tait, S.W.G.; Green, D.R. Mitochondrial Regulation of Cell Death. Cold Spring Harb. Perspect. Biol. 2013, 5, a008706. [Google Scholar] [CrossRef] [Green Version]
- Turchetta, R.; Mazzei, F.; Celani, T.; Cammeresi, M.G.; Orlando, M.P.; Altissimi, G.; de Vincentiis, C.; D’Ambrosio, F.; Messineo, D.; Ferraris, A.; et al. Audiological and Radiological Characteristics of a Family with T961G Mitochondrial Mutation. Int. J. Audiol. 2012, 51, 870–879. [Google Scholar] [CrossRef]
- Vila-Sanjurjo, A.; Smith, P.M.; Elson, J.L. Heterologous Inferential Analysis (HIA) and Other Emerging Concepts: In Understanding Mitochondrial Variation In Pathogenesis: There Is No More Low-Hanging Fruit. In Methods in Molecular Biology; Springer: New York, NY, USA, 2021. [Google Scholar]
- Igumnova, V.; Veidemane, L.; Vīksna, A.; Capligina, V.; Zole, E.; Ranka, R. The Prevalence of Mitochondrial Mutations Associated with Aminoglycoside-Induced Deafness in Ethnic Latvian Population: The Appraisal of the Evidence. J. Hum. Genet. 2018, 64, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Dzhemilova, L.U.; Posukh, O.L.; Tazetdinov, A.M.; Barashkov, N.A.; Zhuravskii, S.A.; Ponidelko, S.N.; Markova, T.G.; Tadinova, V.N.; Fedorova, S.A.; Maksimova, N.R.; et al. Analysis of Mitochondrial 12S rRNA and tRNA Ser(UCN) Genes in Patients with Nonsyndromic Sensorineural Hearing Loss from Various Regions of Russia. Russ. J. Genet. 2009, 45, 861–869. [Google Scholar] [CrossRef]
- Gao, Z.; Chen, Y.; Guan, M.-X. Mitochondrial DNA Mutations Associated with Aminoglycoside Induced Ototoxicity. J. Otol. 2017, 12, 1–8. [Google Scholar] [CrossRef]
- Pliss, L.; Tambets, K.; Loogväli, E.-L.; Pronina, N.; Lazdins, M.; Krumina, A.; Baumanis, V.; Villems, R. Mitochondrial DNA Portrait of Latvians: Towards the Understanding of the Genetic Structure of Baltic-Speaking Populations. Ann. Hum. Genet. 2006, 70, 439–458. [Google Scholar] [CrossRef]
- Salas, A.; Elson, J.L. Mitochondrial DNA as a Risk Factor for False Positives in Case-Control Association Studies. J. Genet. Genom. 2015, 42, 169–172. [Google Scholar] [CrossRef]
- La Morgia, C.; Maresca, A.; Caporali, L.; Valentino, M.L.; Carelli, V. Mitochondrial Diseases in Adults. J. Intern. Med. 2020, 287, 592–608. [Google Scholar] [CrossRef]
- Münch, C.; Harper, J.W. Mitochondrial Unfolded Protein Response Controls Matrix Pre-RNA Processing and Translation. Nature 2016, 534, 710–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter-Dennerlein, R.; Oeljeklaus, S.; Lorenzi, I.; Ronsör, C.; Bareth, B.; Schendzielorz, A.B.; Wang, C.; Warscheid, B.; Rehling, P.; Dennerlein, S. Mitochondrial Protein Synthesis Adapts to Influx of Nuclear-Encoded Protein. Cell 2016, 167, 471–483.e10. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. WHO Operational Handbook on Tuberculosis. Module 4: Treatment—Drug-Resistant Tuberculosis Treatment, 2022 Update; World Health Organisation: Geneva, Switzerland, 2022; ISBN 978-92-4-006312-9. [Google Scholar]


{kind=link}
| Characteristic | No. (%) of Patients | No. (%) of Patients with Adverse Events | ||||
|---|---|---|---|---|---|---|
| Total | Ototoxicity * | Nephrotoxicity * | Both Events | |||
| Biological sex | Male | 35 (74.5) | 19 (54.3) | 13 (37.1) | 8 (22.9) | 2 (5.7) |
| Female | 12 (25.5) | 7 (58.3) | 3 (25.0) | 5 (41.7) | 1 (8.3) | |
| p value ** | 1.000 | 0.505 | 0.269 | 1.000 | ||
| Smoking status | Non-smoker | 9 (19.1) | 6 (66.7) | 3 (33.3) | 4 (44.4) | 1 (11.1) |
| Smoking experience | 38 (80.9) | 20 (52.6) | 13 (34.2) | 9 (23.7) | 2 (5.3) | |
| p value | 0.711 | 1.000 | 0.237 | 0.464 | ||
| BMI | Underweight | 8 (17.0) | 5 (62.5) | 3 (37.5) | 3 (37.5) | 1 (12.5) |
| Normal | 33 (70.2) | 16 (48.5) | 11 (33.3) | 7 (21.2) | 2 (6.1) | |
| Overweight | 4 (8.5) | 3 (75.0) | 1 (25.0) | 2 (50.0) | 0 | |
| Obese | 2 (4.3) | 2 (100.0) | 1 (50.0) | 1 (50.0) | 0 | |
| p value | 0.387 | 0.936 | 0.463 | 0.822 | ||
| Alcohol consumption | Increased | 8 (17.0) | 3 (37.5) | 3 (37.5) | 0 | 0 |
| Normal | 39 (83.0) | 23 (59.0) | 13 (33.3) | 13 (33.3) | 3 (7.7) | |
| p value | 0.437 | 1.000 | 0.086 | 1.000 | ||
| HIV | Yes | 5 (10.6) | 3 (60.0) | 2 (40.0) | 2 (40.0) | 1 (20.0) |
| No | 42 (89.4) | 23 (54.8) | 14 (33.3) | 11 (26.2) | 2 (4.8) | |
| p value | 1.000 | 1.000 | 0.607 | 0.292 | ||
| ART | Yes | 3 (6.4) | 2 (66.7) | 1 (33.3) | 1 (33.3) | 0 |
| No | 44 (93.6) | 24 (54.5) | 15 (34.1) | 12 (27.3) | 3 (6.8) | |
| p value | 1.000 | 1.000 | 1.000 | 1.000 | ||
| DM | Yes | 6 (12.8) | 4 (66.7) | 3 (50.0) | 2 (33.3) | 1 (16.7) |
| No | 41 (87.2) | 22 (53.7) | 13 (31.7) | 11 (26.8) | 2 (4.9) | |
| p value | 0.678 | 0.395 | 1.000 | 0.343 | ||
| HCV | Yes | 8 (17.0) | 5 (62.5) | 4 (50.0) | 3 (37.5) | 2 (25.0) |
| No | 39 (83.0) | 21 (53.9) | 12 (30.8) | 10 (25.6) | 1 (2.6) | |
| p value | 0.716 | 0.416 | 0.666 | 0.071 | ||
| TB incident case | New case | 33 (70.2) | 17 (51.5) | 10 (30.3) | 8 (24.2) | 1 (3.0) |
| Recurrent case | 14 (29.8) | 9 (64.3) | 6 (42.9) | 5 (35.7) | 2 (14.3) | |
| p value | 0.528 | 0.506 | 0.486 | 0.208 | ||
| Injectable agent used | Amikacin | 2 | 2 (100.0) | 2 (100.0) | 1 (50.0) | 1 (50.0) |
| Capreomycin | 29 | 14 (48.3) | 5 (17.2) | 10 (34.5) | 1 (3.4) | |
| Amikacin + capreomycin *** | 16 | 10 (62.5) | 9 (56.3) | 2 (12.5) | 1 (6.3) | |
| p value | 0.282 | 0.004 | 0.222 | 0.034 | ||
| Renal impairment before treatment | Yes | 5 (10.6) | 5 (100.0) | 3 (60.0) | 4 (80.0) | 2 (40) |
| No | 42 (89.4) | 21 (50.0) | 13 (31.0) | 9 (21.4) | 1 (2.4) | |
| p value | 0.056 | 0.320 | 0.017 | 0.027 | ||
| Hearing impairment before treatment | Yes | 31 (66.0) | 16 (51.6) | 10 (32.3) | 8 (25.8) | 2 (6.5) |
| No | 16 (34.0) | 10 (62.5) | 6 (37.5) | 5 (31.3) | 1 (6.25) | |
| p value | 0.547 | 0.754 | 0.739 | 1.000 | ||
| Treatment outcome | Cured | 38 (80.9) | 21 (55.3) | 13 (34.2) | 10 (26.3) | 2 (5.3) |
| Interrupted treatment | 7 (14.9) | 3 (42.9) | 1 (14.3) | 2 (28.6) | 0 | |
| Died | 1 (2.1) | 1 (100.0) | 1 (100.0) | 0 | 0 | |
| Unknown | 1 (2.1) | 1 (100.0) | 1 (100.0) | 1 (100.0) | 1 (100.0) | |
| p value | 0.561 | 0.314 | 0.386 | 0.002 | ||
| All patients | 47 (100) | 26 (55.3) | 16 (34.0) | 13 (27.7) | 3 (6.4) | |
| Characteristic | No. (%) of Patients | No. (%) of Patients with Adverse Events | ||||
|---|---|---|---|---|---|---|
| Total | Ototoxicity * | Nephrotoxicity * | Both Events | |||
| mtDNA haplogroup | H | 19 (40.4) | 11 (57.9) | 7 (36.8) | 6 (31.6) | 2 (10.5) |
| HV | 1 (2.1) | 0 | 0 | 0 | 0 | |
| I | 1 (2.1) | 0 | 0 | 0 | 0 | |
| J | 3 (6.4) | 2 (66.7) | 0 | 2 (66.7) | 0 | |
| N | 1 (2.1) | 1 (100.0) | 1 (100.0) | 1 (100.0) | 1 (100.0) | |
| T | 6 (12.8) | 4 (66.7) | 4 (66.7) | 0 | 0 | |
| U | 10 (21.3) | 4 (40.0) | 3 (30.0) | 1 (10.0) | 0 | |
| V | 3 (6.4) | 2 (66.7) | 0 | 2 (66.7) | 0 | |
| W | 2 (4.3) | 1 (50.0) | 0 | 1 (50.0) | 0 | |
| X | 1 (2.1) | 1 (100.0) | 1 (100.0) | 0 | 0 | |
| SNVs in protein coding genes (only local private and global private SNVs) | yes | 18 (38.3) | 12 (66.7) | 7 (38.9) | 6 (33.3) | 1 (5.6) |
| no | 29 (61.7) | 14 (48.3) | 9 (31.0) | 7 (24.1) | 2 (9.5) | |
| p value | 0.245 | 0.753 | 0.521 | 1.00 | ||
| SNVs in 12S rRNA gene (any) | yes | 37 (78.7) | 20 (54.1) | 12 (32.4) | 10 (27.0) | 2 (5.4) |
| no | 10 (21.3) | 6 (60.0) | 4 (40.0) | 3 (30.0) | 1 (10.0) | |
| p value | 1.000 | 0.716 | 1.000 | 0.521 | ||
| SNVs in tRNA genes (any) | yes | 26 (55.3) | 15 (58.0) | 11 (42.3) | 7 (27.0) | 3 (11.5) |
| no | 21 (44.7) | 11 (52.4) | 5 (23.8) | 6 (28.6) | 0 | |
| p value | 0.774 | 0.227 | 1.000 | 0.242 | ||
| All patients | 47 | 26 (55.3) | 16 (34.0) | 13 (27.7) | 3 (6.4) | |
| Patient ID | mtDNA Haplo- Group ** | Oto-Toxicity | Nephro-Toxicity | SNV | Gene | Gene Function | Effect of SNV | Association with Deafness or Hearing Loss [24] |
|---|---|---|---|---|---|---|---|---|
| MDR-A1 | T2b8 | + | + | m.9254A > G | MT-CO3 | Protein coding | Synonymous | no |
| m.15287T > C | MT-CYB | Protein coding | Missense | yes | ||||
| m.16213G > A | non-coding | non-coding | Unknown | no | ||||
| MDR-A3 | H1h1 | + | − | m.14482C > T | MT-ND6 | Protein coding | Synonymous | no |
| m.146T > C | MT-ND6 | non-coding | Unknown | no | ||||
| m.14564A > G | non-coding | Protein coding | Missense | no | ||||
| MDR-A4 | H3b + 16129 | − | + | m.12879T > C | MT-ND5 | Protein coding | Synonymous | no |
| MDR-A6 *** | H | + | − | m.3834G > C | MT-ND1 | Protein coding | Synonymous | no |
| m.12882C > T | MT-ND5 | Protein coding | Synonymous | no | ||||
| m.73A > G | MT-ND5 | non-coding | Unknown | no | ||||
| m.146T > C | non-coding | non-coding | Unknown | no | ||||
| m.13350A > G | non-coding | Protein coding | Synonymous | no | ||||
| m.16114C > T | non-coding | non-coding | Unknown | no | ||||
| m.16192C > T | non-coding | non-coding | Unknown | no | ||||
| m.16311T > C | non-coding | non-coding | Unknown | no | ||||
| m.5654T > C | MT-TA | tRNA | No change in three-dimensional interactions | no | ||||
| m.4395A > G | MT-TQ | tRNA | No change in three-dimensional interactions | no | ||||
| MDR-B2 *** | H+152 | + | − | m.15833C > T | MT-CYB | Protein coding | Synonymous | no |
| m.3796A > G | MT-ND1 | Protein coding | Missense | no | ||||
| m.73A > G | MT-ND4L | non-coding | Unknown | no | ||||
| m.10550A > G | non-coding | Protein coding | Synonymous | no | ||||
| m.16304T > C | non-coding | non-coding | Unknown | no | ||||
| m.16356T > C | non-coding | non-coding | Unknown | no | ||||
| m.16362T > C | non-coding | non-coding | Unknown | no | ||||
| m.5821G > A | MT-TC | tRNA | No change in three-dimensional interactions | yes | ||||
| m.4435A > G | MT-TM | tRNA | Involved in post-trans-criptional modifications | yes | ||||
| m.4336T > C | MT-TQ | tRNA | No change in three-dimensional interactions | yes | ||||
| MDR-B4 | V7a | − | + | m.195T > C | non-coding | non-coding | Unknown | no |
| MDR-B6 | V | − | + | m.16189T > C | non-coding | non-coding | Unknown | no |
| MDR-B7 | W1i | − | + | m.7080T > C | MT-CO1 | Protein coding | Missense | no |
| m.16179C > T | non-coding | non-coding | Unknown | no | ||||
| MDR-C4 | U3b2a1 | − | + | m.1709G > A | MT-ND2 | rRNA | Unknown | no |
| m.5333T > C | MT-RNR2 | Protein coding | Synonymous | no | ||||
| MDR-C5 | H1b1 | + | − | m.3591G > A | MT-ND1 | Protein coding | Synonymous | no |
| MDR-C7 | H+195 | − | + | m.310T > C | non-coding | non-coding | Unknown | no |
| MDR-D1 | U5a1b1h | + | − | m.16093T > C | non-coding | non-coding | Unknown | no |
| MDR-D5 | T1a1b | + | − | m.9438G > A | MT-CO3 | Protein coding | Missense | no |
| m.15323G > A | MT-CYB | Protein coding | Missense | no | ||||
| MDR-D7 | J1c4b | − | + | m.16093T > C | non-coding | non-coding | Unknown | no |
| MDR-E1 | H11 | + | − | m.8898C > T | MT-ATP6 | Protein coding | Synonymous | no |
| m.7389T > C | MT-CO1 | Protein coding | Missense | no | ||||
| m.9554G > A | MT-CO3 | Protein coding | Synonymous | no | ||||
| m.4215A > G | MT-ND1 | Protein coding | Synonymous | no | ||||
| m.16278C > T | non-coding | non-coding | Unknown | no | ||||
| m.961T > A | MT-RNR1 | rRNA | Unknown | no | ||||
| MDR-E4 | H5a1a | + | + | m.93A > G | non-coding | non-coding | Unknown | no |
| m.16483G > A | non-coding | non-coding | Unknown | no | ||||
| MDR-F4 | U4a2 | + | − | m.16145G > A | non-coding | non-coding | Unknown | no |
| MDR-F6 | X2c1a | + | − | m.11662T > C | MT-ND4 | Protein coding | Synonymous | no |
| MDR-G2 | T2b4a | + | − | m.6593A > G | MT-CO1 | Protein coding | Synonymous | no |
| MDR-G4 | H1b2 | − | + | m.4496C > T | MT-ND2 | Protein coding | Synonymous | no |
| m.11248A > G | MT-ND4 | Protein coding | Synonymous | no | ||||
| m.12510C > T | MT-ND5 | Protein coding | Synonymous | no | ||||
| m.14259G > A | MT-ND6 | Protein coding | Missense | no | ||||
| m.73A > G | non-coding | non-coding | Unknown | no | ||||
| MDR-G5 | H17a | + | + | m.8712C > T | MT-ATP6 | Protein coding | Synonymous | no |
| m.152T > C | non-coding | non-coding | Unknown | no | ||||
| m.310T > C | non-coding | non-coding | Unknown | no | ||||
| MDR-H4 | H6c1 | − | + | m.150C > T | non-coding | non-coding | Unknown | no |
| MDR-H6 | J1c2t | − | + | m.9615T > C | MT-CO3 | Protein coding | Synonymous | no |
| m.4892C > T | MT-ND2 | Protein coding | Synonymous | no | ||||
| m.13359G > A | MT-ND5 | Protein coding | Synonymous | no | ||||
| m.310T > C | non-coding | non-coding | Unknown | no | ||||
| m.16209T > C | non-coding | non-coding | Unknown | no |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freimane, L.; Barkāne, L.; Kivrane, A.; Sadovska, D.; Ulanova, V.; Ranka, R. Assessment of Amikacin- and Capreomycin-Related Adverse Drug Reactions in Patients with Multidrug-Resistant Tuberculosis and Exploring the Role of Genetic Factors. J. Pers. Med. 2023, 13, 599. https://doi.org/10.3390/jpm13040599
Freimane L, Barkāne L, Kivrane A, Sadovska D, Ulanova V, Ranka R. Assessment of Amikacin- and Capreomycin-Related Adverse Drug Reactions in Patients with Multidrug-Resistant Tuberculosis and Exploring the Role of Genetic Factors. Journal of Personalized Medicine. 2023; 13(4):599. https://doi.org/10.3390/jpm13040599
Chicago/Turabian StyleFreimane, Lauma, Linda Barkāne, Agnija Kivrane, Darja Sadovska, Viktorija Ulanova, and Renāte Ranka. 2023. "Assessment of Amikacin- and Capreomycin-Related Adverse Drug Reactions in Patients with Multidrug-Resistant Tuberculosis and Exploring the Role of Genetic Factors" Journal of Personalized Medicine 13, no. 4: 599. https://doi.org/10.3390/jpm13040599
APA StyleFreimane, L., Barkāne, L., Kivrane, A., Sadovska, D., Ulanova, V., & Ranka, R. (2023). Assessment of Amikacin- and Capreomycin-Related Adverse Drug Reactions in Patients with Multidrug-Resistant Tuberculosis and Exploring the Role of Genetic Factors. Journal of Personalized Medicine, 13(4), 599. https://doi.org/10.3390/jpm13040599