

Prognosis Factors of Patients Undergoing Renal Replacement Therapy
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz-Terol, J.M.; Rocha, J.L.; Castro-de la Nuez, P.; García-Cabrera, E.; Vilches-Arenas, Á. Years of Potential Life Lost on Renal Replacement Therapy: Retrospective Study Cohort. J. Clin. Med. 2023, 12, 51. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.; Boenink, R.; Noordzij, M.; Bosdriesz, J.R.; Stel, V.S.; Beltrán, P.; Ruiz, J.C.; Seyahi, N.; Farnés, J.C.; Stendahl, M.; et al. The ERA-EDTA Registry Annual Report 2017: A summary. Clin. Kidney J. 2020, 13, 693–709. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.; Boenink, R.; Stel, V.S.; Santiuste de Pablos, C.; Tomović, F.; Golan, E.; Kerschbaum, J.; Seyahi, N.; Ioanou, K.; Beltrán, P.; et al. The ERA-EDTA Registry Annual Report 2018: A summary. Clin. Kidney J. 2021, 14, 107–123. Available online: https://academic.oup.com/ckj/article/14/1/107/6046935 (accessed on 18 January 2023). [CrossRef] [PubMed]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.C.; Held, P.J.; Port, F.K. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [Green Version]
- Naylor, K.L.; Kim, S.J.; McArthur, E.; Garg, A.X.; McCallum, M.K.; Knoll, G.A. Mortality in Incident Maintenance Dialysis Patients Versus Incident Solid Organ Cancer Patients: A Population-Based Cohort. Am. J. Kidney Dis. 2019, 73, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Rabbat, C.G.; Thorpe, K.E.; Russell, J.D.; Churchill, D.N. Comparison of mortality risk for dialysis patients and cadaveric first renal transplant recipients in Ontario, Canada. J. Am. Soc. Nephrol. 2000, 11, 917–922. [Google Scholar] [CrossRef]
- Yao, X.; Lei, W.; Shi, N.; Lin, W.; Du, X.; Zhang, P.; Chen, J. Impact of initial dialysis modality on the survival of patients with ESRD in eastern China: A propensity-matched study. BMC Nephrol. 2020, 21, 310. Available online: https://pubmed.ncbi.nlm.nih.gov/32727426/ (accessed on 18 January 2023). [CrossRef]
- Amsterdam UMC. ERA-EDTA Registry: ERA-EDTA Registry Annual Report 2017; Amsterdam UMC, Location AMC, Department of Medical Informatics: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Robinson, B.M.; Akizawa, T.; Jager, K.J.; Kerr, P.G.; Saran, R.; Pisoni, R.L. Factors affecting outcomes in patients reaching end-stage kidney disease worldwide: Differences in access to renal replacement therapy, modality use, and haemodialysis practices. Lancet 2016, 388, 294–306. [Google Scholar] [CrossRef]
- United States Renal Data System. 2018 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2018.
- Laupacis, A.; Keown, P.; Pus, N.; Krueger, H.; Ferguson, B.; Wong, C.; Muirhead, N. A study of the quality of life and cost-utility of renal transplantation. Kidney Int. 1996, 50, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Arrieta, J. Evaluación económica del tratamiento sustitutivo renal (hemodiálisis, diálisis peritoneal y trasplante) en España. Nefrologia 2010, 1 (Suppl. 1), 37–47. [Google Scholar]
- Stel, V.S.; de Jong, R.W.; Kramer, A.; Andrusev, A.M.; Baltar, J.M.; Barbullushi, M.; Bell, S.; de la Nuez, P.C.; Cernevskis, H.; Couchoud, C.; et al. Supplemented ERA-EDTA Registry data evaluated the frequency of dialysis, kidney transplantation, and comprehensive conservative management for patients with kidney failure in Europe. Kidney Int. 2021, 100, 182–195. [Google Scholar] [CrossRef] [PubMed]
- Junta de Andalucía. Orden de 27 de Septiembre de 2005, Por la Que se Crea el Sistema de Información de la Coordinación Autonómica de Trasplantes de Andalucía. Boletín Oficial de la Junta de Andalucía, BOJA no 200 de. 13 October 2005. [Google Scholar]
- Asociación Médica Mundial AMM. Declaración de Helsinki.—Principios Éticos Para las Investigaciones Médicas en Seres Humanos; Asociación Médica Mundial AMM: Ferney-Voltaire, Francia, 2013. [Google Scholar]
- Beddhu, S.; Bruns, F.J.; Saul, M.; Seddon, P.; Zeidel, M.L. A simple comorbidity scale predicts clinical outcomes and costs in dialysis patients. Am. J. Med. 2000, 108, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Venkat-Raman, G.; Tomson, C.; Gao, Y.; Cornet, R.; Stengel, B.; Gronhagen-Riska, C.; Reid, C.; Jacquelinet, C.; Schaeffner, E.; Boeschoten, E.; et al. New primary renal diagnosis codes for the ERA-EDTA. Nephrol. Dial. Transplant. 2012, 27, 4414–4419. [Google Scholar] [CrossRef]
- Sociedad Española de Nefrología (SEN); Registro Español de Enfermos Renales de las Comunidades Autónomas; Organización Nacional de Trasplantes (ONT). R Español de Enfermos Renales. Informe de Diálisis y Trasplantes 2018 (Datos Preliminares). Inf 2018 Congr la Soc Española Nefrol (SEN). 2019. Available online: https://www.senefro.org/contents/webstructure/SEN_2019_REER_modificada.pdf (accessed on 1 March 2023).
- Bayat, S.; Kessler, M.; Brianon, S.; Frimat, L. Survival of transplanted and dialysed patients in a French region with focus on outcomes in the elderly. Nephrol. Dial. Transplant. 2010, 25, 292–300. [Google Scholar] [CrossRef] [Green Version]
- McArthur, E.; Bota, S.E.; Sood, M.M.; Nesrallah, G.E.; Kim, S.J.; Garg, A.X.; Dixon, S.N. Comparing Five Comorbidity Indices to Predict Mortality in Chronic Kidney Disease: A Retrospective Cohort Study. Can. J. Kidney Health Dis. 2018, 5, 2054358118805418. [Google Scholar] [CrossRef] [Green Version]
- Kalantar-Zadeh, K.; Kovesdy, C.P.; Streja, E.; Rhee, C.M.; Soohoo, M.; Chen, J.L.; Molnar, M.Z.; Obi, Y.; Gillen, D.; Nguyen, D.V.; et al. Transition of care from pre-dialysis prelude to renal replacement therapy: The blueprints of emerging research in advanced chronic kidney disease. Nephrol. Dial. Transplant. 2017, 32 (Suppl. 2), ii91–ii98. [Google Scholar] [CrossRef] [Green Version]
- Rosansky, S.; Glassock, R.J.; Clark, W.F. Early start of dialysis: A critical review. Clin. J. Am. Soc. Nephrol. 2011, 6, 1222–1228. [Google Scholar] [CrossRef] [Green Version]
- Verberne, W.R.; Geers, A.B.; Jellema, W.T.; Vincent, H.H.; van Delden, J.J.; Bos, W.J. Comparative Survival among Older Adults with Advanced Kidney Disease Managed Conservatively Versus with Dialysis. Clin. J. Am. Soc. Nephrol. 2016, 11, 633–640. [Google Scholar] [CrossRef] [Green Version]
- Soleymanian, T.; Sheikh, V.; Tareh, F.; Argani, H.; Ossareh, S. Hemodialysis vascular access and clinical outcomes: An observational multicenter study. J. Vasc. Access 2017, 18, 35–42. [Google Scholar] [CrossRef]
- Tordoir, J.H.M.; Bode, A.S.; Van Loon, M.M. Preferred strategy for hemodialysis access creation in elderly patients. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 738–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aitken, E.; Thomson, P.; Bainbridge, L.; Kasthuri, R.; Mohr, B.; Kingsmore, D. A randomized controlled trial and cost-effectiveness analysis of early cannulation arteriovenous grafts versus tunneled central venous catheters in patients requiring urgent vascular access for hemodialysis. J. Vasc. Surg. 2017, 65, 766–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Cantón, C.; Rufino-Hernández, J.M.; Vega-Díaz, N.; Pérez-Borges, P.; Bosch-Benítez-Parodi, E.; Saavedra, P.; García-Gómez, C.; Marrero-Robayna, S.; Maceira-Cruz, B.; Rodríguez-Pérez, J.C.; et al. Supervivencia comparada a medio plazo entre diálisis peritoneal y hemodiálisis según el acceso vascular de inicio. Nefrologia 2013, 33, 629–639. [Google Scholar]
- Cabrera, J.; Fernández-Ruiz, M.; Trujillo, H.; González, E.; Molina, M.; Polanco, N.; Hernández, E.; Morales, E.; Gutiérrez, E.; Mori, J.R.; et al. Kidney transplantation in the extremely elderly from extremely aged deceased donors: A kidney for each age. Nephrol. Dial. Transplant. 2020, 35, 687–696. [Google Scholar] [CrossRef]
- Alfano, G.; Perrone, R.; Fontana, F.; Ligabue, G.; Giovanella, S.; Ferrari, A.; Gregorini, M.; Cappelli, G.; Magistroni, R.; Donati, G. Rethinking Chronic Kidney Disease in the Aging Population. Life 2022, 12, 1724. [Google Scholar] [CrossRef] [PubMed]
- Chandna, S.M.; Da Silva-Gane, M.; Marshall, C.; Warwicker, P.; Greenwood, R.N.; Farrington, K. Survival of elderly patients with stage 5 CKD: Comparison of conservative management and renal replacement therapy. Nephrol. Dial. Transplant. 2011, 26, 1608–1614. [Google Scholar] [CrossRef] [Green Version]
- Martínez, A.C.; Lima, A.O.D.L.; Terol, J.M.M.; García, J.M.; Rodríguez, C.R.; Mochón, L.G.; de la Nuez, P.C.; Fosalba, N.A. Optimal start in dialysis shows increased survival in patients with chronic kidney disease. PLoS ONE 2019, 14, e0219037. [Google Scholar] [CrossRef] [Green Version]
- Marrón, B.; Ortiz, A.; de Sequera, P.; Martín-Reyes, G.; de Arriba, G.; Lamas, J.M.; Ocaña, J.C.M.; Arrieta, J.; Martínez, F. Impact of end-stage renal disease care in planned dialysis start and type of renal replacement therapy—A Spanish multicentre experience. Nephrol. Dial. Transplant. 2006, 2121 (Suppl. S2), ii51–ii55. [Google Scholar] [CrossRef] [Green Version]
- Vonesh, E.F.; Snyder, J.J.; Foley, R.N.; Collins, A.J. The differential impact of risk factors on mortality in hemodialysis and peritoneal dialysis. Kidney Int. 2004, 66, 2389–2401. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| N = 11,551 (%) | CI95% | |
|---|---|---|
| Sex | ||
| Male | 7254 (62.8) | (61.9; 63.7) |
| Female | 4293 (37.2) | (36.3; 38.1) |
| Occupational status * | ||
| Active | 2414 (20.9) | (19.8; 21.9) |
| Inactive | 4677 (79.1) | (78.1; 80.2) |
| Comorbidities | ||
| Median Charlson index score (IQR) | 6 (2) | (6; 7) |
| Diabetes mellitus | 4443 (38.5) | (37.6; 39.4) |
| Congestive heart failure | 2184 (18.9) | (18.2; 19.6) |
| Myocardial infarction | 2066 (17.9) | (17.2; 18.6) |
| Peripheral vascular disease | 1737 (15.0) | (14.4; 15.7) |
| COPD | 1406 (12.2) | (11.6; 12.8) |
| Solid tumour localised | 1031 (8.9) | (8.4; 9.5) |
| Cerebrovascular accident | 983 (8.5) | (8.0; 9.0) |
| Connective tissue disease | 476 (4.1) | (3.8; 4.5) |
| Peptic ulcer disease | 372 (3.2) | (2.9; 3.6) |
| Mild liver disease | 388 (3.4) | (3.0; 3.7) |
| Moderate to severe liver disease | 195 (1.7) | (1.5; 1.9) |
| Leukemia/lymphoma | 175 (1.5) | (1.3; 1.8) |
| Dementia | 148 (1.3) | (1.1; 1.5) |
| Metastatic solid tumour | 117 (1.0) | (0.8; 1.2) |
| HIV | 96 (0.8) | (0.7; 1.0) |
| AIDS | 23 (0.2) | (0.1; 0.3) |
| HBV | 139 (1.2) | (1.0; 1.4) |
| HCV | 371 (3.2) | (2.9; 3.5) |
| End-stage kidney disease aetiology | ||
| Diabetic nephropathies | 2832 (24.5) | (23.7; 25.3) |
| Glomerular disease | 1747 (15.1) | (14.5; 15.8) |
| Hypertension and renovascular disease | 1684 (14.6) | (13.9; 15.2) |
| Renal tubulo-interstitial nephropathy | 1222 (10.6) | (10.0; 11.1) |
| Familial/hereditary nephropathies | 971 (8.4) | (7.9; 8.9) |
| Systemic diseases affecting the kidney | 389 (3.4) | (3.1; 3.7) |
| Miscellaneous renal disorders | 305 (2.6) | (2.4; 2.9) |
| Chronic renal failure; aetiology uncertain | 2401 (20.8) | (20.1; 21.5) |
| End-stage kidney disease follow-up | ||
| Without previous follow-up | 1541 (13.3) | (12.7; 14.0) |
| ESKD ≤ 6 months of follow-up | 1543 (13.4) | (12.7; 14.0) |
| ESKD > 6 months of follow-up | 8467 (73.3) | (72.5; 74.1) |
| Renal replacement therapy starts | ||
| Median age-onset RRT | 65 | (65.0; 66.0) |
| Programed | 7754 (67.8) | (66.9; 68.6) |
| Not programmed. | 3683 (32.2) | (31.4; 33.1) |
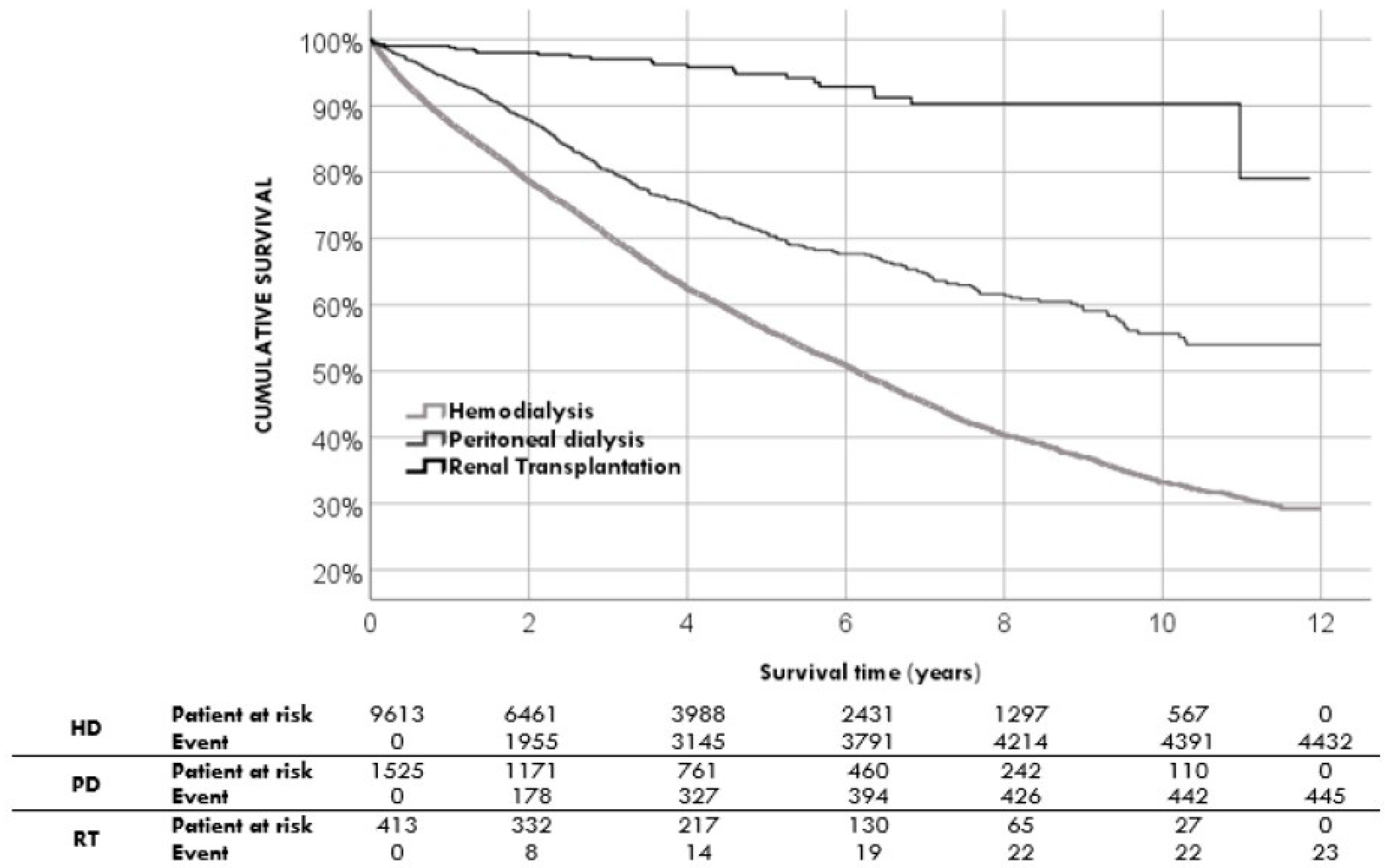
| Renal replacement therapy modalities at the beginning | ||
| Hemodialysis | 9613 (83.2) | (82.5; 83.9) |
| Peritoneal dialysis | 1525 (13.2) | (12.6; 13.8) |
| Renal transplantation | 413 (3.6) | (3.3; 3.9) |
| Vascular access devices at start | ||
| Venous catheter | 5227 (45.2) | (44.8; 46.0) |
| Arteriovenous (AV) fistula + AV graft | 4510 (39.0) | (38.2; 39.8) |
| None | 1814 (15.7) | (15.0; 16.4) |
| Transplantation Waiting List situation | ||
| Permanently excluded | 6358 (55.0) | (54.1; 55.9) |
| Temporary excluded | 423 (3.7) | (3.3; 4.0) |
| Screening not completed | 994 (8.6) | (8.1; 9.1) |
| Included and waiting | 229 (2.0) | (1.7; 2.2) |
| Included and transplanted | 3547 (30.7) | (29.9; 31.5) |
| Vital Status | ||
| Alive | 6651 (57.6) | (56.7; 58.5) |
| Death | 4900 (42.2) | (41.5; 43.3) |
| Age at death (median) | 75 | (74.7; 75.4) |
| Death causes | ||
| Infectious | 1118 (22.8) | (21.6; 23.9) |
| Cardiac | 983 (20.1) | (19.0; 21.2) |
| Neoplasm | 582 (11.9) | (11.0; 12.8) |
| Vascular | 501 (10.2) | (9.3; 11.0) |
| Gastrointestinal | 154 (3.1) | (2.6; 3.6) |
| Hepatic | 42 (0.9) | (0.6; 1.1) |
| Accidental | 10 (0.2) | (0.1; 0.3) |
| Multiple causes | 519 (10.6) | (9.7; 11.5) |
| Undetermined | 992 (20.2) | (19.1; 21.3) |
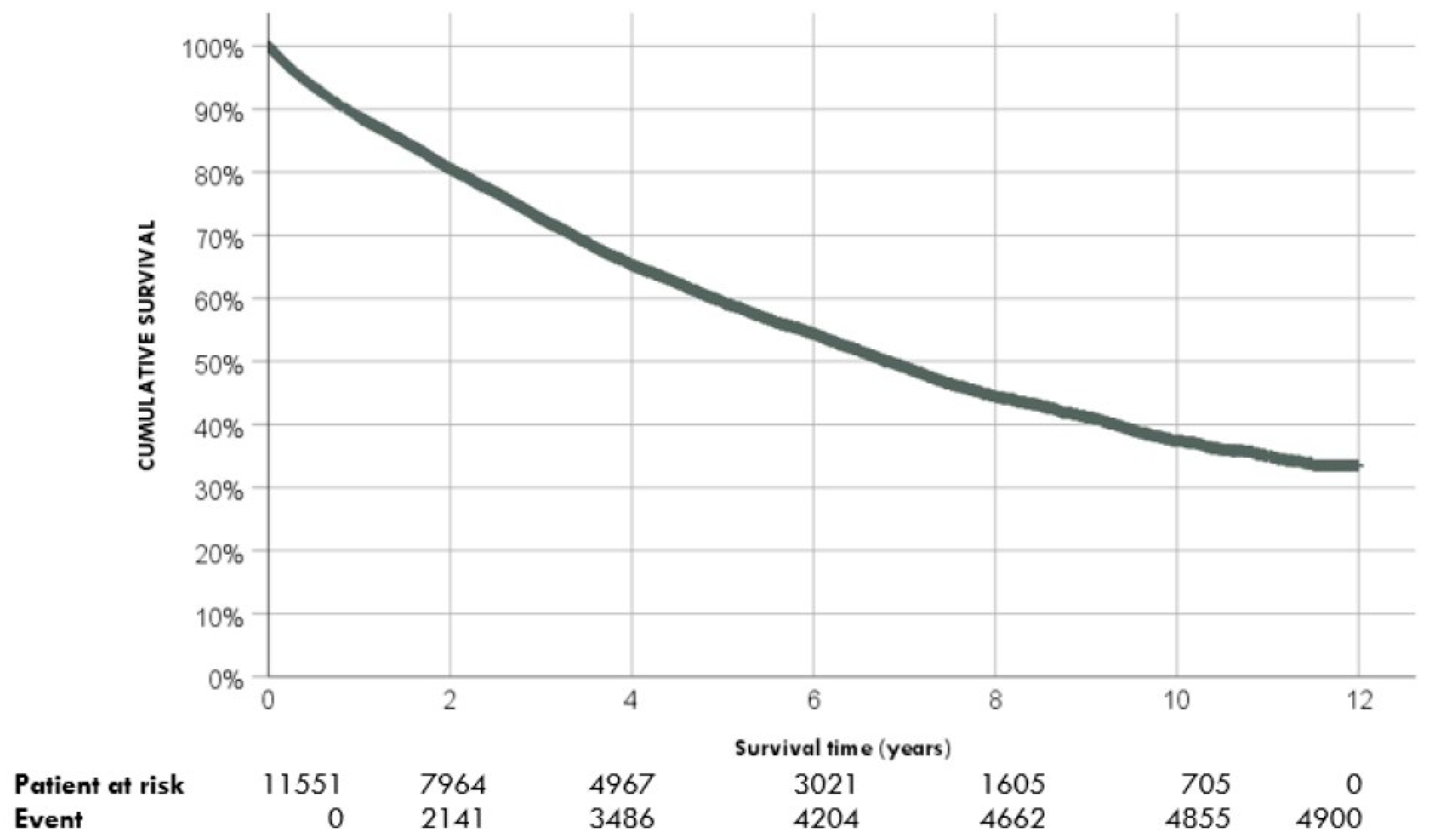
| Survival | % | CI95% |
|---|---|---|
| 1 year | 88.7 | (88.1; 89.3) |
| 3 years | 72.6 | (71.8; 73.4) |
| 5 years | 59.4 | (58.4; 60.4) |
| 10 years | 37.4 | (36.0; 38.8) |
| Alive N = 6651 | Death N = 4900 | p-Value | |||
|---|---|---|---|---|---|
| N (%) | CI95% | N (%) | CI95% | ||
| Sex | |||||
| Male | 2701 (40.6) | (39.4; 41.8) | 4552 (92.9) | (92.2; 93.6) | 0.001 |
| Female | 3945 (59.4) | (58.2; 60.6) | 348 (7.1) | (6.4; 7.8) | |
| Occupational Status | |||||
| Active | 1811 (64.4) | (62.6; 66.2) | 603 (14.1) | (13.0; 15.1) | <0.001 |
| Inactive | 1003 (35.6) | (33.8; 37.3) | 3674 (85.9) | (84.9; 86.9) | |
| Comorbidities | |||||
| Median Charlson index score | 5.0 | (5.0; 5.1) | 7.3 | (7.2; 7.3) | <0.001 |
| Diabetes mellitus | 2113 (31.8) | (30.7; 32.9) | 2330 (47.6) | (46.2; 49.0) | <0.001 |
| Congestive heart failure | 789 (11.9) | (11.1; 12.7) | 1395 (28.5) | (27.2; 29.7) | <0.001 |
| Myocardial infarction | 800 (12.0) | (11.3; 12.8) | 1266 (25.8) | (24.6; 27.1) | <0.001 |
| Peripheral vascular disease | 637 (9.6) | (8.9; 10.3) | 1100 (24.4) | (21.3; 23.6) | <0.001 |
| COPD | 578 (8.7) | (8.0; 9.4) | 828 (16.9) | (15.9; 18.0) | <0.001 |
| Solid tumour localised | 469 (7.1) | (6.5; 7.7) | 562 (11.5) | (10.6; 12.4) | <0.001 |
| Cerebrovascular accident | 452 (6.8) | (6.2; 7.4) | 531 (10.8) | (10.0; 11.7) | <0.001 |
| Connective tissue disease | 269 (4.0) | (3.6; 4.5) | 207 (4.2) | (3.7; 4.8) | 0.181 |
| Peptic ulcer disease | 152 (2.3) | (1.9; 2.7) | 220 (4.5) | (3.9; 5.1) | <0.001 |
| Mild liver disease | 181 (2.7) | (2.4; 3.1) | 207 (4.2) | (3.7; 4.8) | <0.001 |
| Moderate to severe liver disease | 73 (1.1) | (0.9; 1.4) | 122 (2.5) | (2.1; 3.0) | 0.004 |
| Leukemia/lymphoma | 63 (0.9) | (0.7; 1.2) | 112 (2.3) | (1.9; 2.7) | <0.001 |
| Dementia | 44 (0.7) | (0.5; 0.9) | 104 (2.1) | (1.7; 2.6) | <0.001 |
| Metastatic solid tumour | 36 (0.5) | (0.4; 0.7) | 81 (1.7) | (1.3; 2.0) | <0.001 |
| HIV | 52 (0.8) | (0.6; 1.0) | 44 (0.9) | (0.7; 1.2) | 0.497 |
| AIDS | 12 (0.2) | (0.1; 0.3) | 11 (0.2) | (0.1; 0.4) | 0.117 |
| HBV | 88 (1.3) | (1.1; 1.6) | 51 (1.0) | (0.8; 1.4) | 0.169 |
| HCV | 179 (2.7) | (2.3; 3.1) | 192 (3.9) | (3.4; 4.5) | <0.001 |
| End-stage kidney disease aetiology | <0.001 | ||||
| Diabetic nephropathies | 1397 (21.0) | (20.0; 22.0) | 1435 (29.3) | (28.0; 30.6) | |
| Glomerular disease | 1302 (19.6) | (18.6; 20.5) | 445 (9.1) | (8.3; 9.9) | |
| Hypertension and renovascular disease | 819 (12.3) | (11.5; 13.1) | 865 (17.7) | (16.6; 18.7) | |
| Renal tubulo-interstitial nephropathy | 609 (9.2) | (8.5; 9.9) | 613 (12.5) | (11.6; 13.4) | |
| Familial/hereditary nephropathies | 775 (11.7) | (10.9; 12.4) | 196 (4.0) | (3.5; 4.6) | |
| Systemic diseases affecting the kidney | 151 (2.3) | (1.9; 2.6) | 238 (4.9) | (4.3; 5.5) | |
| End-stage kidney disease follow-up | |||||
| Without previous follow-up | 833 (12.5) | (11.7; 13.3) | 708 (14.4) | (13.5; 15.5) | 0.002 |
| ESKD ≤ 6 months of follow-up | 863 (13.0) | (12.2; 13.8) | 680 (13.9) | (12.9; 14.9) | |
| ESKD > 6 months of follow-up | 4955 (74.5) | (73.4; 75.5) | 3512 (71.7) | (70.4; 72.9) | |
| Renal replacement therapy at start | |||||
| Median age onset RRT | 57.5 | (57.1; 57.8) | 69.7 | (69.4; 70.1) | <0.001 |
| Programed | 4825 (73.0) | (71.9; 74.1) | 2929 (60.7) | (59.3; 62.0) | <0.001 |
| Not programmed. | 1784 (27.0) | (25.9; 28.1) | 1899 (39.3) | (38.0; 40.7) | |
| Renal replacement therapy modalities at the beginning | |||||
| Hemodialysis | 5181 (77.9) | (76.9; 78.9) | 4432 (90.4) | (89.6; 91.2) | <0.001 |
| Peritoneal dialysis | 1080 (16.2) | (15.4; 17.1) | 445 (9.1) | (8.3; 9.9) | |
| Renal transplantation | 390 (5.9) | (5.8; 6.0) | 23 (0.4) | (0.3; 0.6) | |
| Vascular access devices at start | |||||
| Venous catheter | 2548 (38.3) | (37.6; 38.9) | 2679 (54.7) | (53.5; 56.9) | <0.001 |
| Arteriovenous (AV) fistula + AV graft | 2724 (41.0) | (40.2; 41.8) | 1786 (36.5) | (35.2; 37.8) | |
| None | 1379 (20.7) | (19.8; 21.7) | 435 (8.9) | (8.1; 9.7) | |
| Transplantation | |||||
| Transplantation | 3413 (51.3) | (50.1; 52.5) | 363 (7.4) | (6.7; 8.2) | <0.001 |
| N | HR | CI95% | p-Value | |
|---|---|---|---|---|
| Age-onset RRT | 11,551 | 1.06 | (1.06; 1.06) | <0.001 |
| Sex | 0.008 | |||
| Female | 4293 | 1 | ||
| Male | 7258 | 1.08 | (1.02; 1.15) | |
| Diabetic nephropathies | <0.001 | |||
| No | 8719 | 1 | ||
| Yes | 2832 | 1.45 | (1.37; 1.55) | |
| End-stage kidney disease follow-up | <0.001 | |||
| ESKD > 6 months of follow-up | 8647 | 1 | ||
| ESKD ≤ 6 months of follow-up | 3084 | 1.24 | (1.17; 1.32) | |
| Renal replacement therapy at start | <0.001 | |||
| Programed | 7754 | 1 | ||
| Not programmed. | 3683 | 1.67 | (1.58; 1.77) | |
| Vascular access devices at start | <0.001 | |||
| None | 1814 | 1 | ||
| AV fistula + AV graft | 4510 | 1.64 | (1.48; 1.82) | |
| Venous catheter | 5227 | 2.69 | (2.43; 2.97) | |
| Renal replacement therapy modalities at the beginning | <0.001 | |||
| Renal transplantation | 413 | 1 | ||
| Peritoneal dialysis | 1525 | 5.42 | (3.57; 8.24) | |
| Hemodialysis | 9613 | 9.67 | (6.42; 14.57) | |
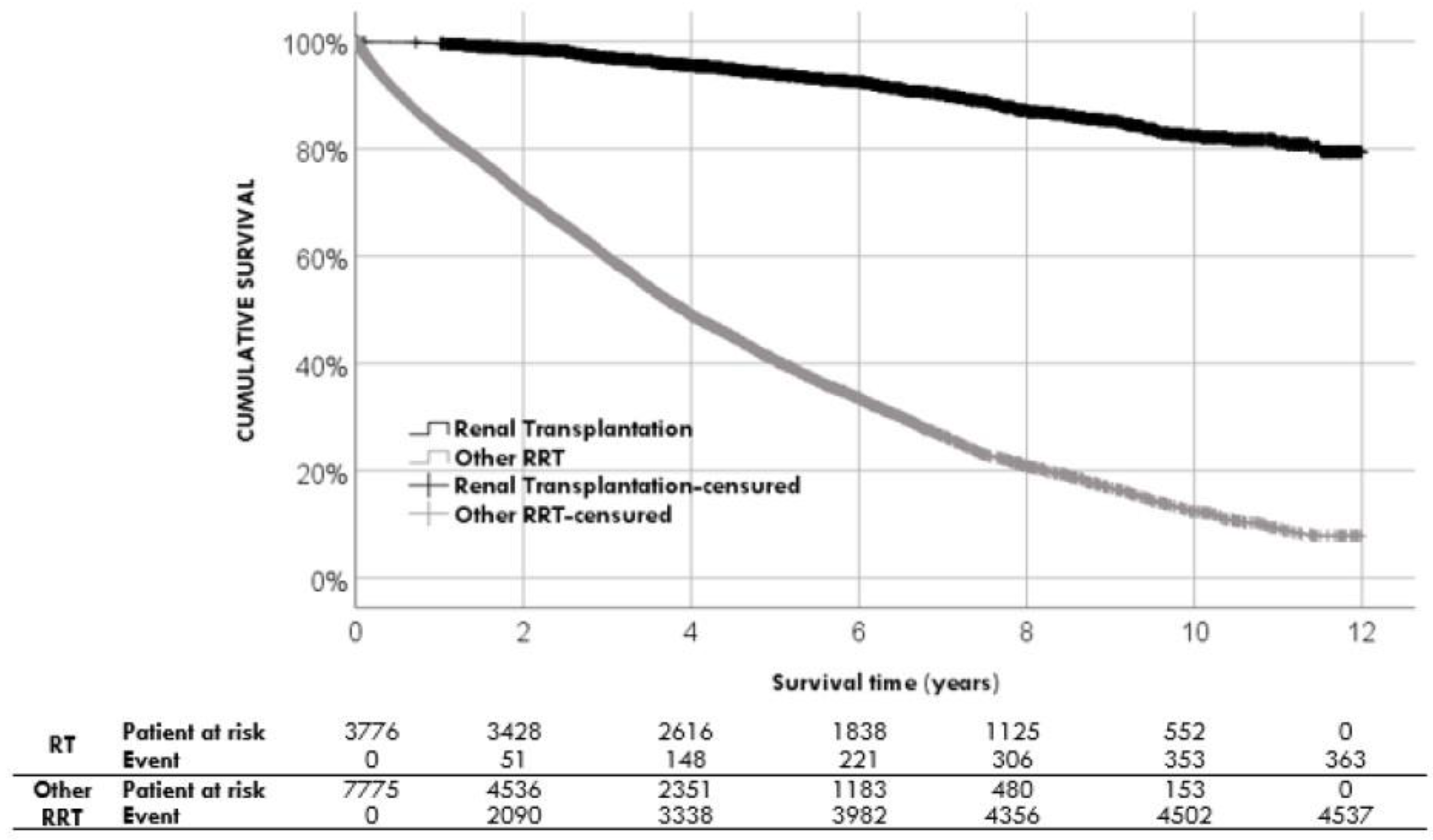
| Renal transplantation | <0.001 | |||
| Yes | 3776 | 1 | ||
| No | 7775 | 12.58 | (11.29; 14.02) | |
| HCV serology | <0.001 | |||
| Negative | 11,180 | 1 | ||
| Positive | 371 | 1.37 | (1.18; 1.58) | |
| Comorbidities | ||||
| Myocardial infarction | 2066 | 2.1 | (2.0; 2.2) | <0.001 |
| Congestive heart failure | 2184 | 2.4 | (2.2; 2.5) | <0.001 |
| Peripheral vascular disease | 1737 | 2.1 | (1.9; 2.2) | <0.001 |
| Dementia | 148 | 2.4 | (2.0; 2.9) | <0.001 |
| COPD | 1406 | 1.8 | (1.7; 2.0) | <0.001 |
| Peptic ulcer disease | 372 | 1.5 | (1.3; 1.7) | <0.001 |
| Mild liver disease | 388 | 1.5 | (1.3; 1.7) | <0.001 |
| Solid tumour localised | 1031 | 1.7 | (1.5; 1.8) | <0.001 |
| Leukemia/lymphoma | 175 | 2.7 | (2.3; 3.3) | <0.001 |
| Diabetes mellitus | 4443 | 1.8 | (1.7; 1.9) | <0.001 |
| Cerebrovascular accident | 983 | 1.7 | (1.5; 1.8) | <0.001 |
| Moderate to severe liver disease | 195 | 2.1 | (1.7; 2.5) | <0.001 |
| Metastatic solid tumour | 117 | 3.0 | (2.4; 3.8) | <0.001 |
| Charlson index score | <0.001 | |||
| Low (2–4) | 3749 | 1 | ||
| Medium (5–6) | 2881 | 4.2 | (3.8; 4.6) | |
| High (7–8) | 2764 | 6.6 | (5.9; 7.3) | |
| Very high (>8) | 2157 | 9.9 | (9.0; 10.9) | |
| HR | CI95% | p-Value | |
|---|---|---|---|
| Charlson index score | 1.15 | 1.14; 1.16 | <0.001 |
| Sex male | 1.08 | 1.02; 1.15 | 0.007 |
| Diabetic nephropathies | 1.16 | 1.08; 1.16 | <0.001 |
| ESKD > 6 months of follow-up | 0.92 | 0.86; 0.99 | 0.020 |
| RRT start not programed | 1.08 | 1.01; 1.16 | 0.025 |
| Vascular access devices at start | |||
| None | 1 | Ref. | <0.001 |
| Arteriovenous (AV) fistula + AV graft | 1.12 | 0.79; 1.59 | |
| Venous catheter | 1.46 | 1.03; 2.07 | |
| Renal transplantation | 0.13 | 0.11; 0.14 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Terol, J.M.; Rocha, J.L.; Castro-de la Nuez, P.; Egea-Guerrero, J.J.; Gil-Sacaluga, L.; García-Cabrera, E.; Vilches-Arenas, A. Prognosis Factors of Patients Undergoing Renal Replacement Therapy. J. Pers. Med. 2023, 13, 605. https://doi.org/10.3390/jpm13040605
Muñoz-Terol JM, Rocha JL, Castro-de la Nuez P, Egea-Guerrero JJ, Gil-Sacaluga L, García-Cabrera E, Vilches-Arenas A. Prognosis Factors of Patients Undergoing Renal Replacement Therapy. Journal of Personalized Medicine. 2023; 13(4):605. https://doi.org/10.3390/jpm13040605
Chicago/Turabian StyleMuñoz-Terol, José Manuel, José L. Rocha, Pablo Castro-de la Nuez, Juan José Egea-Guerrero, Luis Gil-Sacaluga, Emilio García-Cabrera, and Angel Vilches-Arenas. 2023. "Prognosis Factors of Patients Undergoing Renal Replacement Therapy" Journal of Personalized Medicine 13, no. 4: 605. https://doi.org/10.3390/jpm13040605
APA StyleMuñoz-Terol, J. M., Rocha, J. L., Castro-de la Nuez, P., Egea-Guerrero, J. J., Gil-Sacaluga, L., García-Cabrera, E., & Vilches-Arenas, A. (2023). Prognosis Factors of Patients Undergoing Renal Replacement Therapy. Journal of Personalized Medicine, 13(4), 605. https://doi.org/10.3390/jpm13040605