

A Novel Risk Calculator to Predict Erectile Dysfunction in HIV-Positive Men


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pino, M.; Paiardini, M.; Marconi, V.C. Progress in achieving long-term HIV remission. Curr. Opin. HIV AIDS 2018, 13, 435–445. [Google Scholar] [CrossRef] [PubMed]
- De Rocco Ponce, M.; Selice, R.; Di Mambro, A.; De Toni, L.; Foresta, C.; Garolla, A. Estradiol–Testosterone Imbalance Is Associated with Erectile Dysfunction in Patients with Klinefelter Syndrome. J. Clin. Med. 2021, 10, 2319. [Google Scholar] [CrossRef] [PubMed]
- Darcis, G.; Berkhout, B.; Pasternak, A.O. Differences in HIV Markers between Infected Individuals Treated with Different ART Regimens: Implications for the Persistence of Viral Reservoirs. Viruses 2020, 12, 489. [Google Scholar] [CrossRef] [PubMed]
- Rebez, G.; Capogrosso, P.; Boeri, L.; Rizzo, M.; Miacola, C.; Cai, T.; Palumbo, F.; Ortensi, I.; Ceruti, C.; Lauretti, S.; et al. Effectiveness of Ginseng, Rutin and Moringa for the Treatment of Erectile Dysfunction: A Systematic Review. Uro 2022, 2, 65–73. [Google Scholar] [CrossRef]
- Bandera, A.; Gori, A.; Clerici, M.; Sironi, M. Phylogenies in ART: HIV reservoirs, HIV latency and drug resistance. Curr. Opin. Pharmacol. 2019, 48, 24–32. [Google Scholar] [CrossRef]
- De Vincentis, S.; Tartaro, G.; Rochira, V.; Santi, D. HIV and Sexual Dysfunction in Men. J. Clin. Med. 2021, 10, 1088. [Google Scholar] [CrossRef]
- Persu, C.; Braschi, E.; Lavelle, J. A review of prospective Clinical Trials for neurogenic bladder: The place of surgery, experimental techniques and devices. Cent. Eur. J. Urol. 2014, 67, 270–276. [Google Scholar] [CrossRef]
- Cao, S.; Gan, Y.; Dong, X.; Liu, J.; Lu, Z. Association of quantity and duration of smoking with erectile dysfunction: A dose-response meta-analysis. J. Sex. Med. 2014, 11, 2376–2384. [Google Scholar] [CrossRef]
- Kumsar, N.A.; Kumsar, Ş.; Dilbaz, N. Sexual dysfunction in men diagnosed as substance use disorder. Andrologia 2016, 48, 1229–1235. [Google Scholar] [CrossRef]
- Guaraldi, G. Evolving approaches and resources for clinical practice in the management of HIV infection in the HAART era. Germs 2011, 1, 6–8. [Google Scholar] [CrossRef]
- Des Jarlais, D.C.; Arasteh, K.; A McKnight, C.; Feelemyer, J.; Campbell, A.N.C.; Tross, S.; Cooper, H.L.F.; Hagan, H.; Perlman, D.C. What happened to the HIV epidemic among non-injecting drug users in New York City? Addiction 2017, 112, 290–298. [Google Scholar] [CrossRef]
- Wen, J.; Yeh, T.P.; Xie, H.; Yu, X.; Tang, J.; Chen, Y. Resilience, self-esteem, self-efficacy, social support, depression and ART adherence among people living with HIV in Sichuan, China. AIDS Care 2021, 33, 1414–1421. [Google Scholar] [CrossRef]
- Lagathu, C.; Béréziat, V.; Gorwood, J.; Fellahi, S.; Bastard, J.-P.; Vigouroux, C.; Boccara, F.; Capeau, J. Metabolic complications affecting adipose tissue, lipid and glucose metabolism associated with HIV antiretroviral treatment. Expert. Opin. Drug. Saf. 2019, 18, 829–840. [Google Scholar] [CrossRef]
- Yannas, D.; Frizza, F.; Vignozzi, L.; Corona, G.; Maggi, M.; Rastrelli, G. Erectile Dysfunction Is a Hallmark of Cardiovascular Disease: Unavoidable Matter of Fact or Opportunity to Improve Men’s Health? J. Clin. Med. 2021, 10, 2221. [Google Scholar] [CrossRef]
- Shubber, Z.; Mills, E.J.; Nachega, J.B.; Vreeman, R.; Freitas, M.; Bock, P.; Nsanzimana, S.; Penazzato, M.; Appolo, T.; Doherty, M.; et al. Patient-Reported Barriers to Adherence to Antiretroviral Therapy: A Systematic Review and Meta-Analysis. PLoS Med. 2016, 13, e1002183. [Google Scholar] [CrossRef]
- Cappelleri, J.C.; Rosen, R.C.; Smith, M.D.; Mishra, A.; Osterloh, I.H. Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology 1999, 54, 346–351. [Google Scholar] [CrossRef]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Zona, S.; Guaraldi, G.; Luzi, K.; Beggi, M.; Santi, D.; Stentarelli, C.; Madeo, B.; Rochira, V. Erectile dysfunction is more common in young to middle-aged HIV-infected men than in HIV-uninfected men. J. Sex. Med. 2012, 9, 1923–1930. [Google Scholar] [CrossRef] [PubMed]
- Green, M.L. Evaluation and management of dyslipidemia in patients with HIV infection. J. Gen. Intern. Med. 2002, 17, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, L.; Lanfranco, F.; Motta, G.; Zavattaro, M. Erectile Dysfunction in Men with Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2021, 10, 2730. [Google Scholar] [CrossRef]
- Dijkstra, M.; van Lunsen, R.H.; Kooij, K.W.; Davidovich, U.; van Zoest, R.A.; Wit, F.W.; Prins, M.; Reiss, P.; van der Loeff, M.F.S. HIV-1 status is independently associated with decreased erectile function among middle-aged MSM in the era of combination antiretroviral therapy. AIDS 2018, 32, 1137–1146. [Google Scholar] [CrossRef]
- Mulhall, J.P.; Luo, X.; Zou, K.H.; Stecher, V.; Galaznik, A. Relationship between age and erectile dysfunction diagnosis or treatment using real-world observational data in the USA. Int. J. Clin. Pract. 2016, 70, 1012–1018. [Google Scholar] [CrossRef]
- Luo, L.; Deng, T.; Zhao, S.; Li, E.; Liu, L.; Li, F.; Wang, J.; Zhao, Z. Association Between HIV Infection and Prevalence of Erectile Dysfunction: A Systematic Review and Meta-Analysis. J. Sex. Med. 2017, 14, 1125–1132. [Google Scholar] [CrossRef]
- Feldman, H.A.; Goldstein, I.; Hatzichristou, D.G.; Krane, R.J.; McKinlay, J.B. Impotence and Its Medical and Psychosocial Correlates: Results of the Massachusetts Male Aging Study. J. Urol. 1994, 151, 54–61. [Google Scholar] [CrossRef]
- Fumaz, C.R.; Ayestaran, A.; Perez-Alvarez, N.; Muñoz-Moreno, J.A.; Ferrer, M.J.; Negredo, E.; Clotet, B. Clinical and Emotional Factors Related to Erectile Dysfunction in HIV-Infected Men. Am. J. Mens Health 2017, 11, 647–653. [Google Scholar] [CrossRef]
- Juang, S.-E.; Ma, K.S.-K.; Kao, P.-E.; Wei, J.C.-C.; Yip, H.-T.; Chou, M.-C.; Hung, Y.-M.; Chin, N.-C. Human Papillomavirus Infection and the Risk of Erectile Dysfunction: A Nationwide Population-Based Matched Cohort Study. J. Pers. Med. 2022, 12, 699. [Google Scholar] [CrossRef]
- Santi, D.; Brigante, G.; Zona, S.; Guaraldi, G.; Rochira, V. Male sexual dysfunction and HIV–a clinical perspective. Nat. Rev. Urol. 2014, 11, 99–109. [Google Scholar] [CrossRef]
- Fan, J.; Peng, T.; Hui, J.; Ding, W.; He, B.; Zhang, H.; Wei, A. Erectile Dysfunction in Type-2 Diabetes Mellitus Patients: Predictors of Early Detection and Treatment. Urol. Int. 2021, 105, 986–992. [Google Scholar] [CrossRef]
- la Vignera, S.; Condorelli, R.A.; Vicari, E.; Calogero, A.E. Statins and erectile dysfunction: A critical summary of current evidence. J. Androl. 2012, 33, 552–558. [Google Scholar] [CrossRef]
- Miner, M.; Billups, K.L. Erectile dysfunction and dyslipidemia: Relevance and role of phosphodiesterase type-5 inhibitors and statins. J. Sex. Med. 2008, 5, 1066–1078. [Google Scholar] [CrossRef]
- Yuan, C.; Jian, Z.; Gao, X.; Jin, X.; Wang, M.; Xiang, L.; Li, H.; Wang, K. Type 2 diabetes mellitus increases risk of erectile dysfunction independent of obesity and dyslipidemia: A Mendelian randomization study. Andrology 2022, 10, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Saramies, J.; Koiranen, M.; Auvinen, J.; Uusitalo, H.; Hussi, E.; Becker, S.; Keinänen-Kiukaanniemi, S.; Tuomilehto, J.; Suija, K. A Natural History of Erectile Dysfunction in Elderly Men: A Population-Based, Twelve-Year Prospective Study. J. Clin. Med. 2022, 11, 2146. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Interpretation |
|---|---|
| 26–30 | no ED |
| 22–25 | mild ED |
| 17–21 | mild to moderate ED |
| 11–16 | moderate ED |
| 6–10 | severe ED |
| Parameter | Patients/Median Value |
|---|---|
| Total patients | 103 |
| Age (median) | 36.45 ± 9.88 years |
| BMI (median) | 23.7 ± 4.1 kg/m2 |
| Glycemia (median) | 92.23 ± 14.98 mg/dL |
| Total lipids (median) | 712.96 ± 198.56 mg/dL |
| Smoker | 69 (67%) |
| Non Smoker | 34 (33%) |
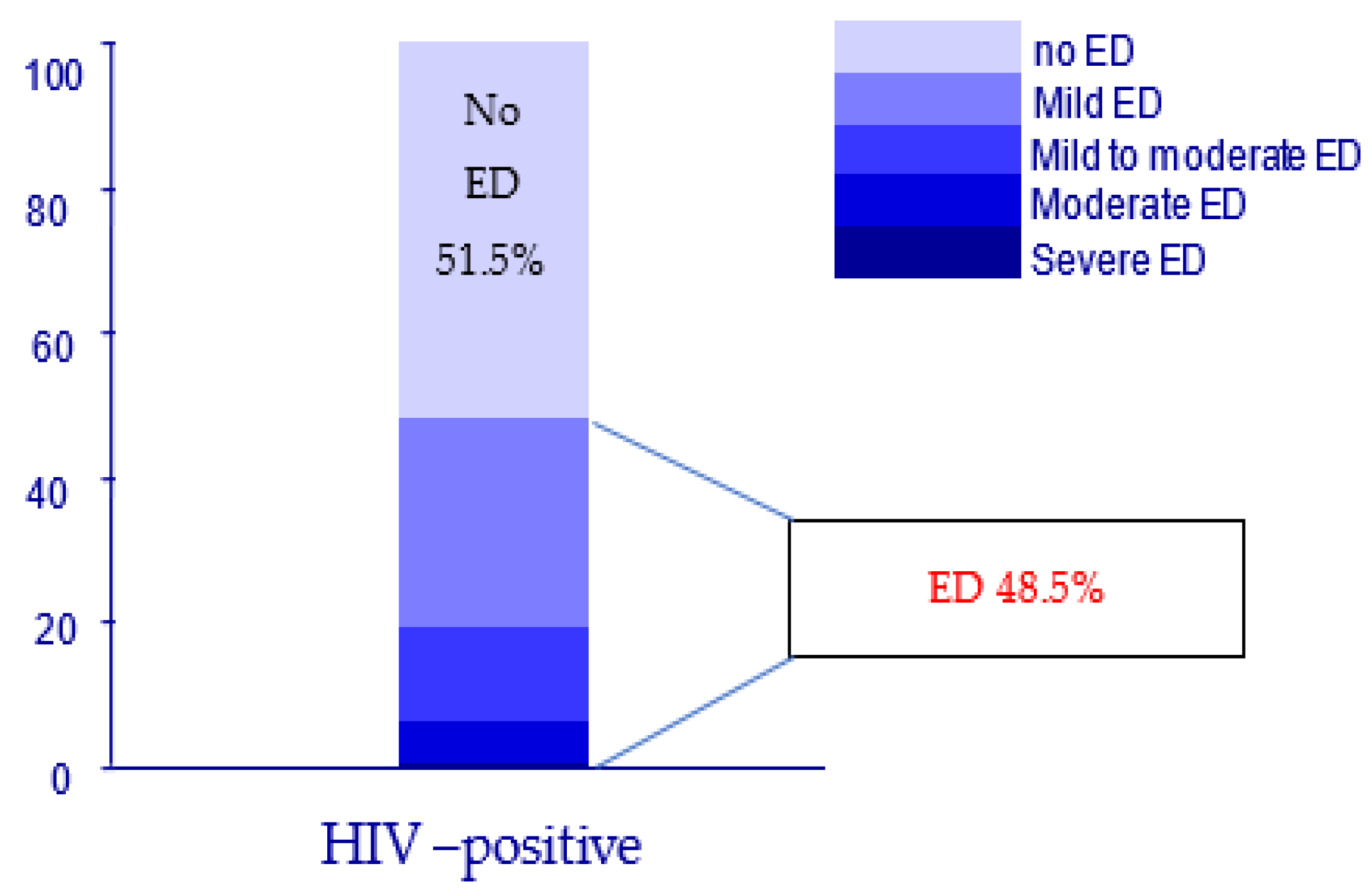
| No ED | 53 |
| With ED | 50 |
| ED prevalence | 48.5% |
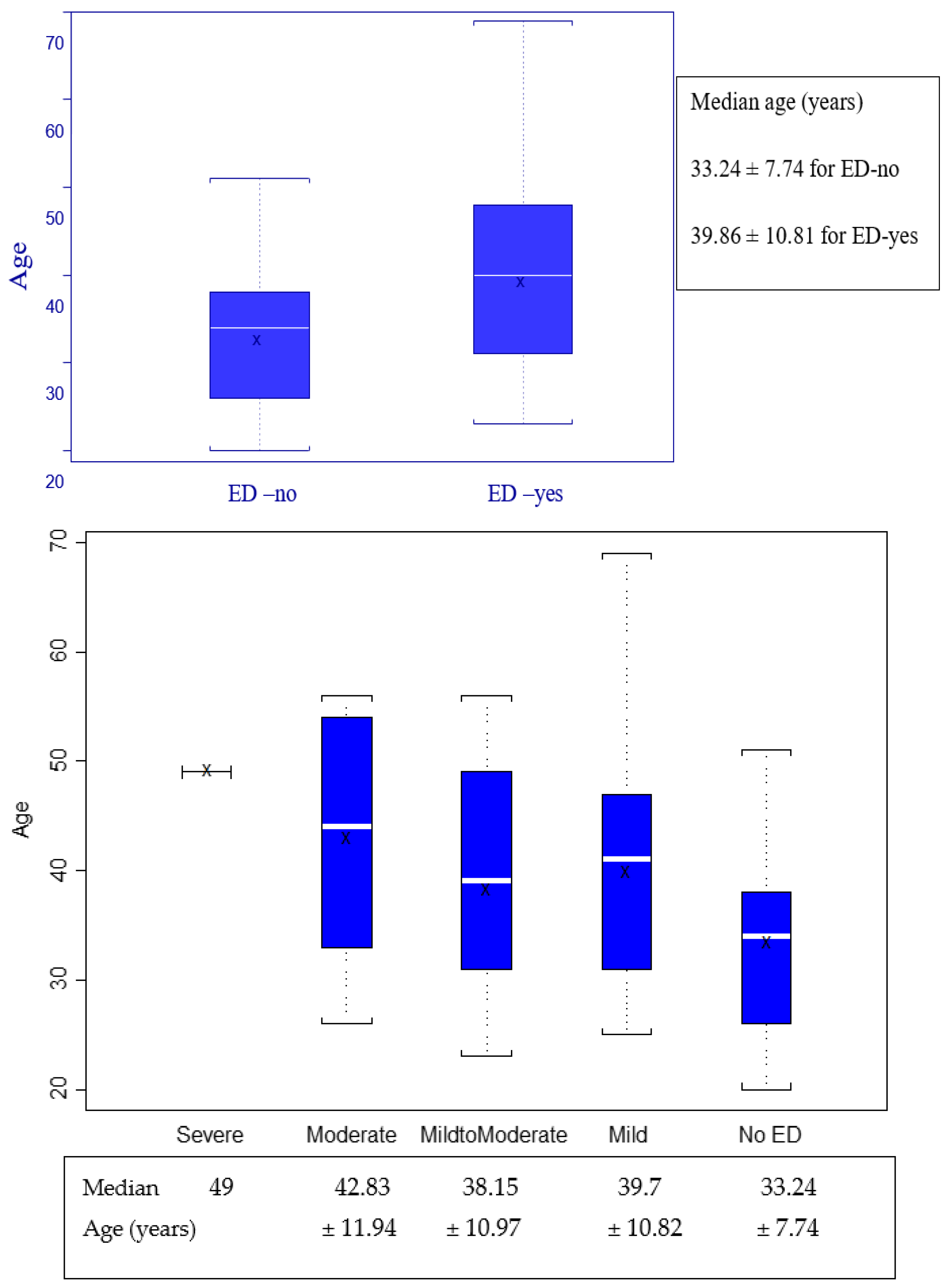
| Kruskal–Wallis Chi-Squared | DF | p-Value | |
|---|---|---|---|
| 1 | 9.9434 | 1 | p = 0.0016 |
| >mean(Age & ED == “ED yes”]) : [1] 39.86 >mean(Age & ED == “ED no”]) : [1] 33.2452830188679 | |||
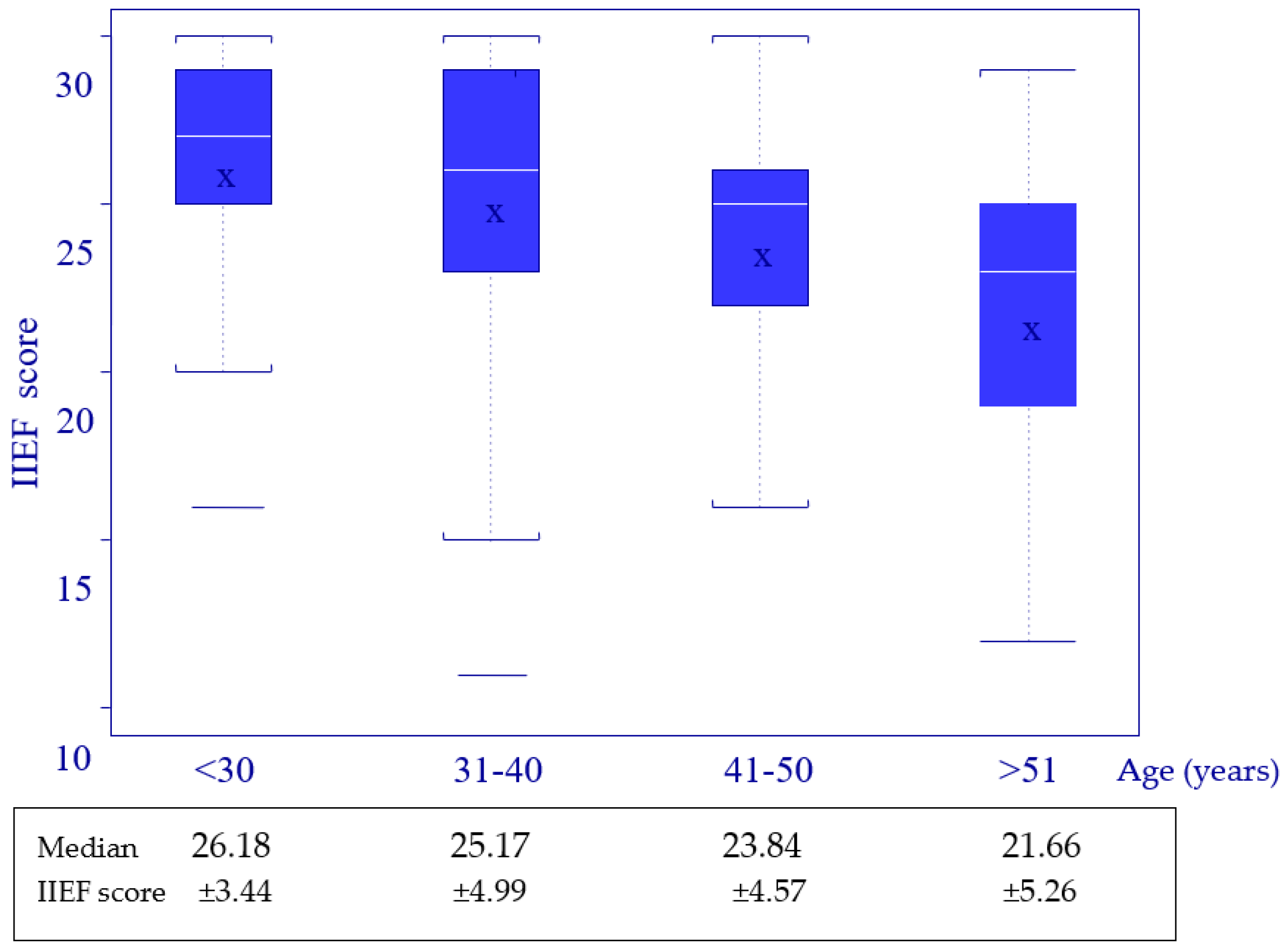
| 2 | 9.2325 | 3 | p = 0.0264 |
| >mean(IIEFscore & Age-Factor == “<30”]) : [1] 26.1818181818182 >mean(IIEFscore & Age-Factor == “31-40”]) : [1] 25.1714285714286 >mean(IIEFscore & Age-Factor == “41-50”]) : [1] 23.8461538461538 >mean(IIEFscore & Age-Factor == “>51”]) : [1] 21.6666666666667 | |||
| Kruskal-Wallis Chi-Squared | DF | p-Value | |
|---|---|---|---|
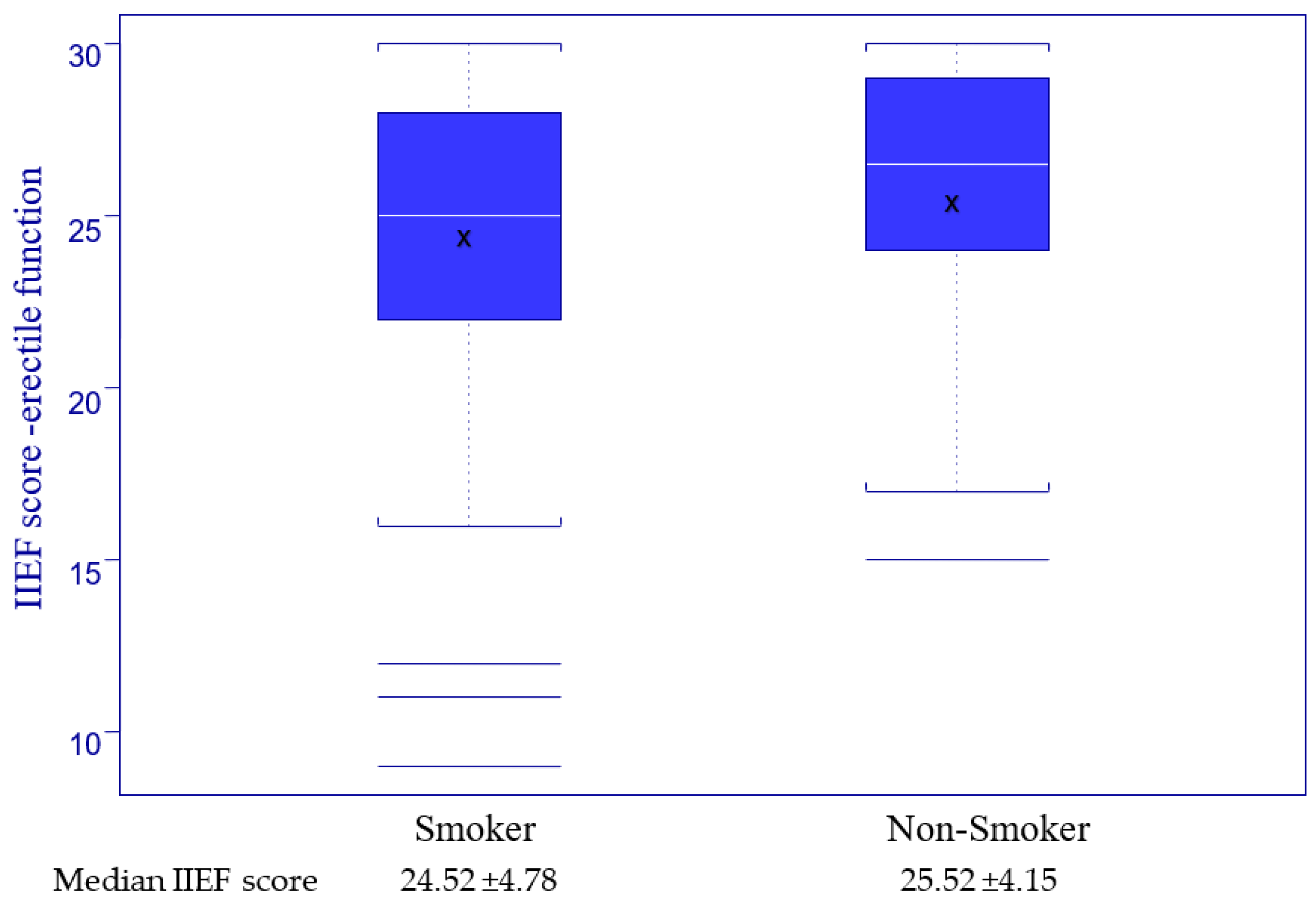
| 1. Smoking | 1.0233 | 1 | p = 0.3117 |
| >mean(IIEFscore & Smoking == “Yes”]) : [1] 24.5217391304348 >mean(IIEFscore & Smoking == “No”]) : [1] 25.5294117647059 | |||
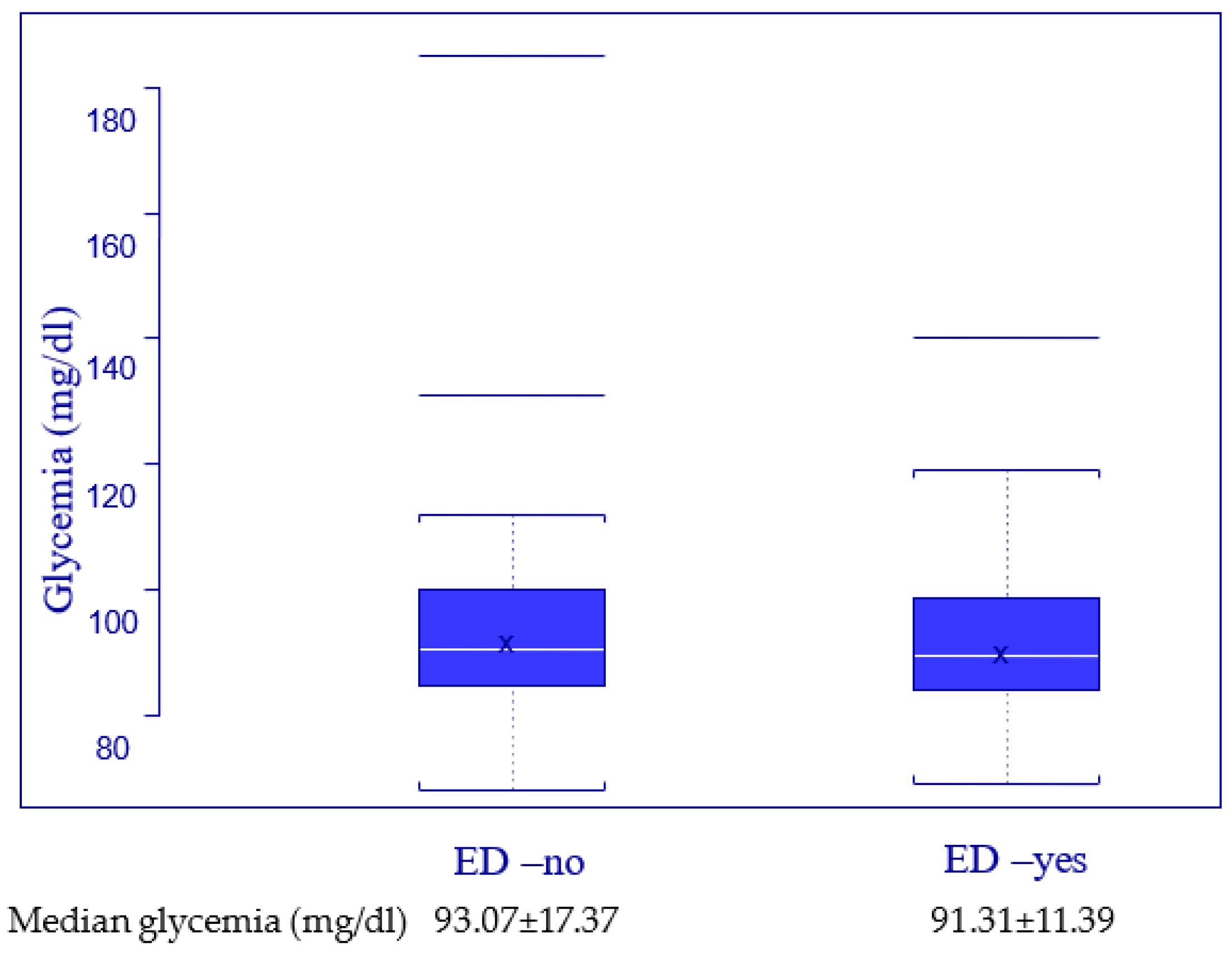
| 2. Glycemia | 0.2682 | 1 | p = 0.6046 |
| >mean(Glycemia & ED == “ED-yes”]) : [1] 91.3125 >mean(Glycemia & ED == “NoED”]) : [1] 93.0769230769231 | |||
| Erectile Function | Kruskal-Wallis Chi-Squared | DF | p-Value |
|---|---|---|---|
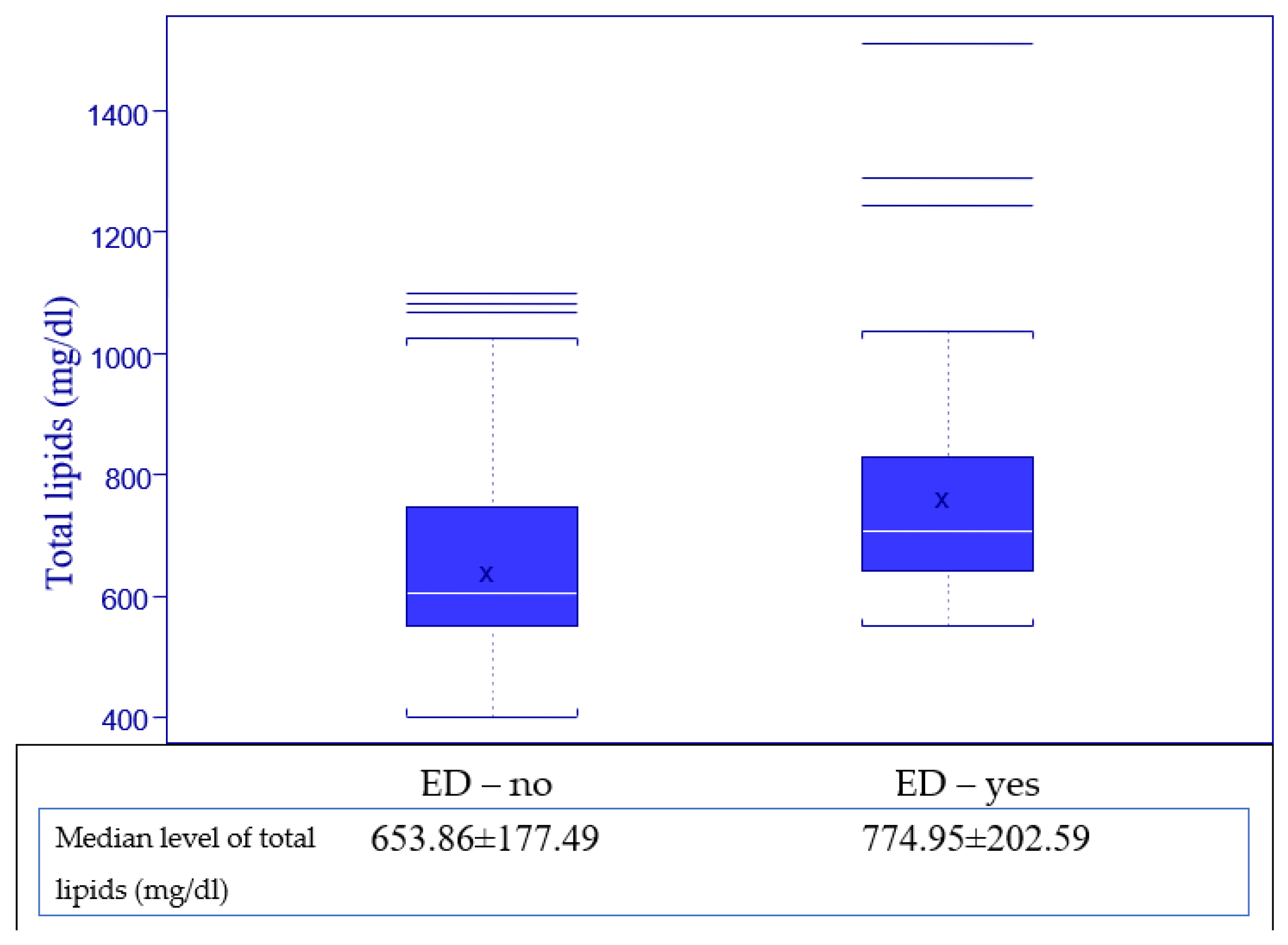
| Binary (yes, no) | 11.7778 | 1 | p = 0.0006 |
| >mean(TotLip & ED == “ED-yes”]) : [1] 774.951219512195 >mean(TotLip & ED == “ED-no”]) : [1] 653.860465116279 | |||
| Categorial | 10.7398 | 1 | p = 0.0132 |
| >mean(TotLip & ED-Cat == “Severe”]) : [1] 1511 >mean(TotLip & ED-Cat == “Moderate”]) : [1] 726 >mean(TotLip & ED-Cat == “MildtoModerate”]) : [1] 71.111111111111 >mean(TotLip & ED-Cat == “Mild”]) : [1] 757.384615384615 >mean(TotLip & ED-Cat == “NoED”]) : [1] 653.860465116279 | |||
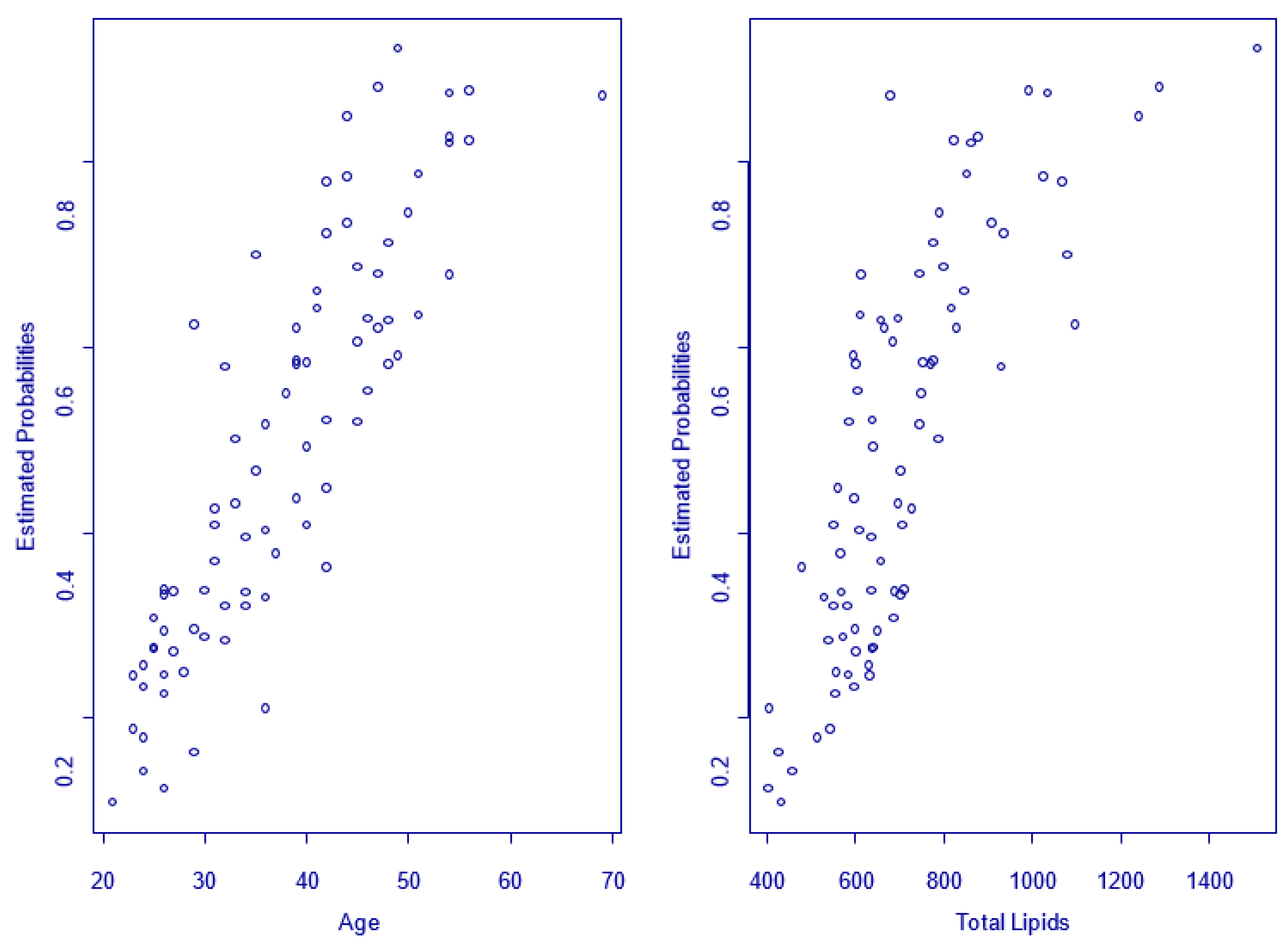
| Intercept | Age | Log (Total Lipids) | |
|---|---|---|---|
| Coefficients Value | −17.2248 | 0.0625 | 2.2736 |
| Std Error | 7.2814 | 0.0279 | 1.1580 |
| t-value | −2.3655 | 2.2339 | 1.9633 |
| p-value for Wald tests (significance test) | 0.0180 | 0.0254 | 0.0496 |
| >exp coeff | 3.3062 | 1.0645 | 9.7143 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chirca, N.; Streinu-Cercel, A.; Stefan, M.; Aurelian, J.; Persu, C. A Novel Risk Calculator to Predict Erectile Dysfunction in HIV-Positive Men. J. Pers. Med. 2023, 13, 679. https://doi.org/10.3390/jpm13040679
Chirca N, Streinu-Cercel A, Stefan M, Aurelian J, Persu C. A Novel Risk Calculator to Predict Erectile Dysfunction in HIV-Positive Men. Journal of Personalized Medicine. 2023; 13(4):679. https://doi.org/10.3390/jpm13040679
Chicago/Turabian StyleChirca, Narcis, Anca Streinu-Cercel, Marius Stefan, Justin Aurelian, and Cristian Persu. 2023. "A Novel Risk Calculator to Predict Erectile Dysfunction in HIV-Positive Men" Journal of Personalized Medicine 13, no. 4: 679. https://doi.org/10.3390/jpm13040679
APA StyleChirca, N., Streinu-Cercel, A., Stefan, M., Aurelian, J., & Persu, C. (2023). A Novel Risk Calculator to Predict Erectile Dysfunction in HIV-Positive Men. Journal of Personalized Medicine, 13(4), 679. https://doi.org/10.3390/jpm13040679