
Comparative Study of Sperm Selection Techniques for Pregnancy Rates in an Unselected IVF–ICSI Population
 ,
,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
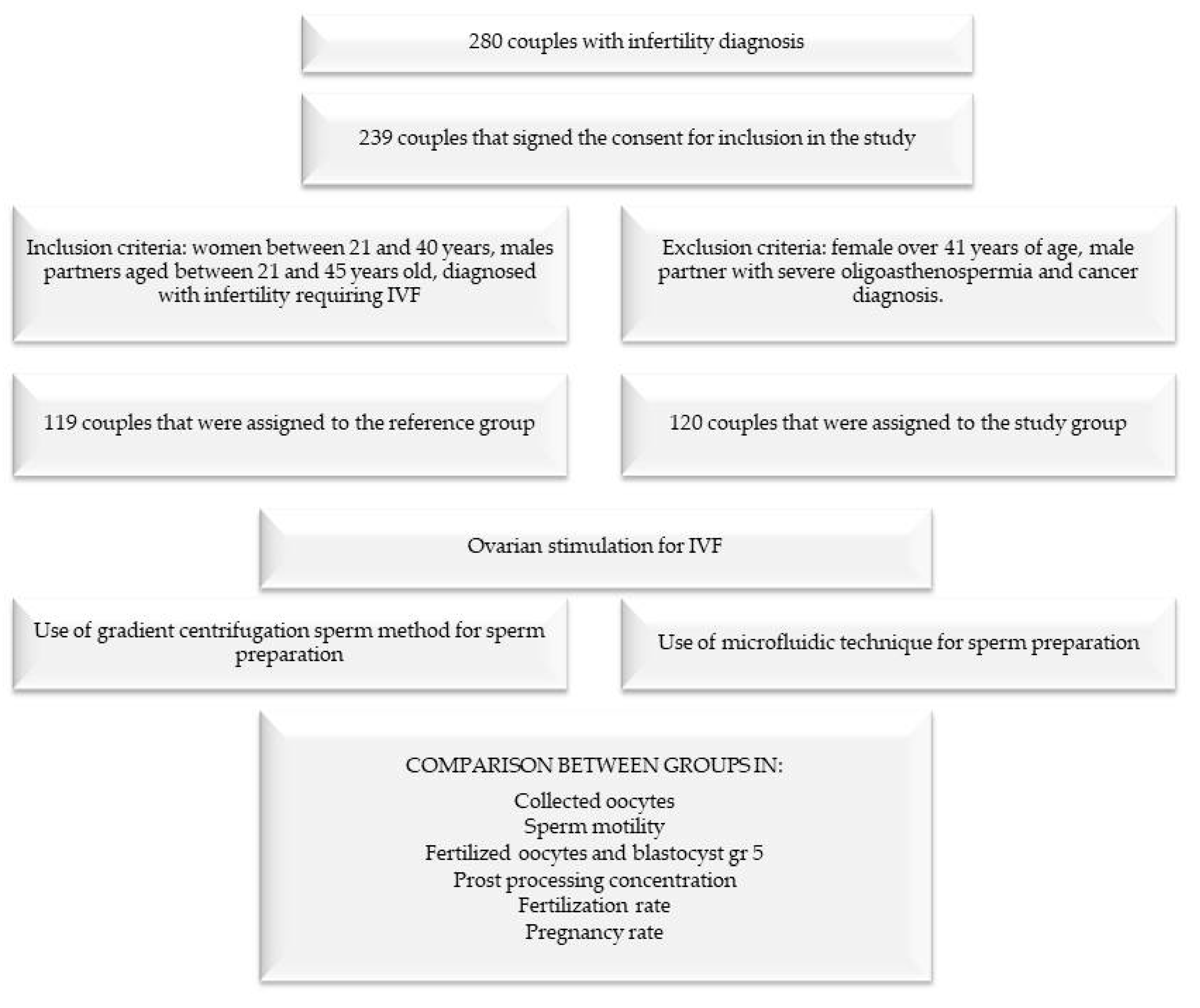
2.1. Population
2.2. Methods
2.3. Laboratory Procedures
Statistical Analysis
3. Results
3.1. Predictors
3.2. Comparisons between Study and Reference Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oseguera-López, I.; Ruiz-Díaz, S.; Ramos-Ibeas, P.; Pérez-Cerezales, S. Novel Techniques of Sperm Selection for Improving IVF and ICSI Outcomes. Front. Cell Dev. Biol. 2019, 7, 298. [Google Scholar]
- Zini, A.; Boman, J.M.; Belzile, E.; Ciampi, A. Sperm DNA damage is associated with an increased risk of pregnancy loss after IVF and ICSI: Systematic review and meta-analysis. Hum. Reprod. 2008, 23, 2663–2668. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Singh, A.K. Trends of Male Factor Infertility, an Important Cause of Infertility: A Review of Literature. J. Hum. Reprod. Sci. 2015, 8, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Weng, L. IVF-on-a-Chip: Recent Advances in Microfluidics Technology for In Vitro Fertilization. SLAS Technol. 2019, 24, 373–385. [Google Scholar] [CrossRef]
- Kashaninejad, N.; Shiddiky, M.J.A.; Nguyen, N.T. Advances in Microfluidics-Based Assisted Reproductive Technology: From Sperm Sorter to Reproductive System-on-a-Chip. Adv. Biosyst. 2018, 2, 1700197. [Google Scholar] [CrossRef]
- Simopoulou, M.; Gkoles, L.; Bakas, P.; Giannelou, P.; Kalampokas, T.; Pantos, K.; Koutsilieris, M. Improving ICSI: A review from the spermatozoon perspective. Syst. Biol. Reprod. Med. 2016, 62, 359–371. [Google Scholar] [CrossRef] [Green Version]
- Parinaud, J.; Mieusset, R.; Vieitez, G.; Labal, B.; Richoilley, G. Influence of sperm parameters on embryo quality. Fertil. Steril. 1993, 60, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Piccolomini, M.M.; Bonetti, T.C.; Motta, E.L.; Serafini, P.C.; Alegretti, J.R. How general semen quality influences the blastocyst formation rate: Analysis of 4205 IVF cycles. JBRA Assist. Reprod. 2018, 22, 89–94. [Google Scholar] [CrossRef]
- Agarwal, A.; Baskaran, S.; Parekh, N.; Cho, C.-L.; Henkel, R.; Vij, S.; Arafa, M.; Panner Selvam, M.K.; Shah, R. Male infertility. Lancet 2021, 397, 319–333. [Google Scholar] [CrossRef]
- Neri, Q.V.; Lee, B.; Rosenwaks, Z.; Machaca, K.; Palermo, G.D. Understanding fertilization through intracytoplasmic sperm injection (ICSI). Cell Calcium 2014, 55, 24–37. [Google Scholar]
- Kishi, K.; Ogata, H.; Ogata, S.; Mizusawa, Y.; Okamoto, E.; Matsumoto, Y.; Kokeguchi, S.; Shiotani, M. Frequency of sperm DNA fragmentation according to selection method: Comparison and relevance of a microfluidic device and a swim-up procedure. J. Clin. Diagn. Res. 2015, 9, QC14–QC16. [Google Scholar] [CrossRef] [PubMed]
- Anbari, F.; Khalili, M.A.; Sultan, A.A.M.; Mangoli, E.; Nabi, A.; Dehghanpour, F.; Sabour, M. Microfluidic sperm selection yields higher sperm quality compared to conventional method in ICSI program: A pilot study. Syst. Biol. Reprod. Med. 2021, 67, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Avendaño, C.; Oehninger, S. DNA fragmentation in morphologically normal spermatozoa: How much should we be concerned in the ICSI era? J. Androl. 2011, 32, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, P.; Takmaz, T.; Yazici, M.G.K.; Alagoz, O.A.; Yesiladali, M.; Sevket, O.; Ficicioglu, C. Does the use of microfluidic sperm sorting for the sperm selection improve in vitro fertilization success rates in male factor infertility? J. Obstet. Gynaecol. Res. 2021, 47, 382–388. [Google Scholar] [CrossRef]
- Muratori, M.; Tarozzi, N.; Carpentiero, F.; Danti, S.; Perrone, F.M.; Cambi, M.; Casini, A.; Azzari, C.; Boni, L.; Maggi, M.; et al. Sperm selection with density gradient centrifugation and swim up: Effect on DNA fragmentation in viable spermatozoa. Sci. Rep. 2019, 9, 7492. [Google Scholar] [CrossRef] [Green Version]
- Zini, A.; Finelli, A.; Phang, D.; Jarvi, K. Influence of semen processing technique on human sperm DNA integrity. Urology 2000, 56, 1081–1084. [Google Scholar] [CrossRef]
- Chapuis, A.; Gala, A.; Ferrières-Hoa, A.; Mullet, T.; Bringer-Deutsch, S.; Vintejoux, E.; Torre, A.; Hamamah, S. Sperm quality and paternal age: Effect on blastocyst formation and pregnancy rates. Basic Clin. Androl. 2017, 27, 2. [Google Scholar] [CrossRef] [Green Version]
- Jeyendran, R.S.; Caroppo, E.; Rouen, A.; Anderson, A.; Puscheck, E. Selecting the most competent sperm for assisted reproductive technologies. Fertil. Steril. 2019, 111, 851–863. [Google Scholar]
- Phiphattanaphiphop, C.; Leksakul, K.; Phatthanakun, R.; Khamlor, T. A novel microfluidic chip-based sperm-sorting device constructed using design of experiment method. Sci. Rep. 2020, 10, 17143. [Google Scholar] [CrossRef]
- Tasoglu, S.; Safaee, H.; Zhang, X.; Kingsley, J.L.; Catalano, P.N.; Gurkan, U.A.; Nureddin, A.; Kayaalp, E.; Anchan, R.M.; Maas, R.L.; et al. Exhaustion of racing sperm in nature-mimicking microfluidic channels during sorting. Small 2013, 9, 3374–3384. [Google Scholar] [CrossRef] [Green Version]
- Eugster, A.; Vingerhoets, A. Psychological aspects of in vitro fertilization: A review. Soc. Sci. Med. 1999, 48, 575–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pujol, A.; García-Peiró, A.; Ribas-Maynou, J.; Lafuente, R.; Mataró, D.; Vassena, R. A microfluidic sperm-sorting device reduces the proportion of sperm with double-stranded DNA fragmentation. Zygote 2022, 30, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Broekmans, F.; Humaidan, P.; Lainas, G.; Töyli, M.; Le Clef, N.; Vermeulen, N. Reply: Questionable recommendation for LPS for IVF/ICSI in ESHRE guideline 2019: Ovarian stimulation for IVF/ICSI. Hum. Reprod. 2021, 2021, hoab006. [Google Scholar] [CrossRef]
- Berendsen, J.T.W.; Kruit, S.A.; Atak, N.; Willink, E.; Segerink, L.I. Flow-free microfluidic device for quantifying chemotaxis in spermatozoa. Anal. Chem. 2020, 92, 3302–3306. [Google Scholar] [CrossRef] [PubMed]
- Quinn, M.M.; Jalalian, L.; Ribeiro, S.; Ona, K.; Demirci, U.; Cedars, M.I.; Rosen, M.P. Microfluidic sorting selects sperm for clinical use with reduced DNA damage compared to density gradient centrifugation with swim-up in split semen samples. Hum. Reprod. 2018, 33, 1388–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardona Barberán, A.; Boel, A.; Vanden Meerschaut, F.; Stoop, D.; Heindryckx, B. Diagnosis and treatment of male infertility-related fertilization failure. J. Clin. Med. 2020, 9, 3899. [Google Scholar] [CrossRef]
- Schuster, T.G.; Cho, B.; Keller, L.M.; Takayama, S.; Smith, G.D. Isolation of motile spermatozoa from semen samples using microfluidics. Reprod. Biomed. Online 2003, 7, 75–81. [Google Scholar]
- Omidi, M.; Aflatoonian, B.; Tahajjodi, S.S.; Khalili, M.A. Attempts for generation of embryonic stem cells from human embryos following in vitro embryo twinning. Stem Cells Dev. 2019, 28, 303–309. [Google Scholar] [CrossRef]
- Vaughan, D.A.; Sakkas, D. Sperm selection methods in the 21st century. Biol. Reprod. 2019, 101, 1076–1082. [Google Scholar]
- Smith, G.D.; Takayama, S. Application of microfluidic technologies to human assisted reproduction. MHR Basic Sci. Reprod. Med. 2017, 23, 257–268. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Age | N | Mean | Std. Deviation |
|---|---|---|---|
| Control group | 119 | 35.62 | 4.495 |
| Study group | 120 | 34.08 | 4.923 |
| Initial concentration (millions/mL) | |||
| Control group | 119 | 39.679 | 35.51766 |
| Study group | 120 | 40.231 | 23.80462 |
| Post-processing concentration | |||
| Control group | 119 | 24.462 | 27.0717 |
| Study group | 120 | 16.312 | 11.4606 |
| Oocytes collected | |||
| Control group | 119 | 9.66 | 6.626 |
| Study group | 120 | 10.98 | 6.819 |
| Motility A + B (%) | |||
| Control group | 119 | 46.84 | 23.76532 |
| Study group | 120 | 57.00 | 17.39545 |
| Oocytes Collected | Study Group | Control Group | t | df | p-Value |
|---|---|---|---|---|---|
| Mean | 10.98 | 9.66 | 1.5265 | 237 | 0.1282 |
| SD | 6.82 | 6.63 | |||
| SEM | 0.62 | 0.61 | |||
| Total number of blastocysts | |||||
| Mean | 2.66 | 1.63 | 0.3028 | 109 | 0.0462 |
| SD | 1.71 | 0.15 | |||
| SEM | 0.16 | 2.28 | |||
| Post-processing concentration | |||||
| Mean | 16.312 | 24.877 | 3.1268 | 231 | 0.002 |
| SD | 11.461 | 27.496 | |||
| SEM | 1.051 | 2.575 | |||
| Fertilization rate | |||||
| Mean | 80.13 | 79.79 | 0.1539 | 238 | 0.8778 |
| SD | 17.01 | 17.38 | |||
| SEM | 1.55 | 1.59 | |||
| Cumulative pregnancy rate | |||||
| Mean | 51.0415 | 40.2080 | 1.8916 | 238 | 0.049 |
| SD | 45.8039 | 42.8701 | |||
| SEM | 4.1813 | 3.9135 | |||
| Motility A + B (%) | |||||
| Mean | 99.75 | 35.00 | 30.0985 | 120 | 0.001 |
| SD | 2.74 | 14.14 | |||
| SEM | 0.25 | 10.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaha, I.; Naghi, P.; Stefan, L.; Bunescu, C.; Radu, M.; Muresan, M.E.; Sandor, M.; Sachelarie, L.; Huniadi, A. Comparative Study of Sperm Selection Techniques for Pregnancy Rates in an Unselected IVF–ICSI Population. J. Pers. Med. 2023, 13, 619. https://doi.org/10.3390/jpm13040619
Zaha I, Naghi P, Stefan L, Bunescu C, Radu M, Muresan ME, Sandor M, Sachelarie L, Huniadi A. Comparative Study of Sperm Selection Techniques for Pregnancy Rates in an Unselected IVF–ICSI Population. Journal of Personalized Medicine. 2023; 13(4):619. https://doi.org/10.3390/jpm13040619
Chicago/Turabian StyleZaha, Ioana, Petronela Naghi, Liana Stefan, Cosmina Bunescu, Mihaela Radu, Mariana Eugenia Muresan, Mircea Sandor, Liliana Sachelarie, and Anca Huniadi. 2023. "Comparative Study of Sperm Selection Techniques for Pregnancy Rates in an Unselected IVF–ICSI Population" Journal of Personalized Medicine 13, no. 4: 619. https://doi.org/10.3390/jpm13040619
APA StyleZaha, I., Naghi, P., Stefan, L., Bunescu, C., Radu, M., Muresan, M. E., Sandor, M., Sachelarie, L., & Huniadi, A. (2023). Comparative Study of Sperm Selection Techniques for Pregnancy Rates in an Unselected IVF–ICSI Population. Journal of Personalized Medicine, 13(4), 619. https://doi.org/10.3390/jpm13040619