

A New Digital Method to Quantify the Effects Produced by Carriere Motion Appliance
 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Experimental Procedure
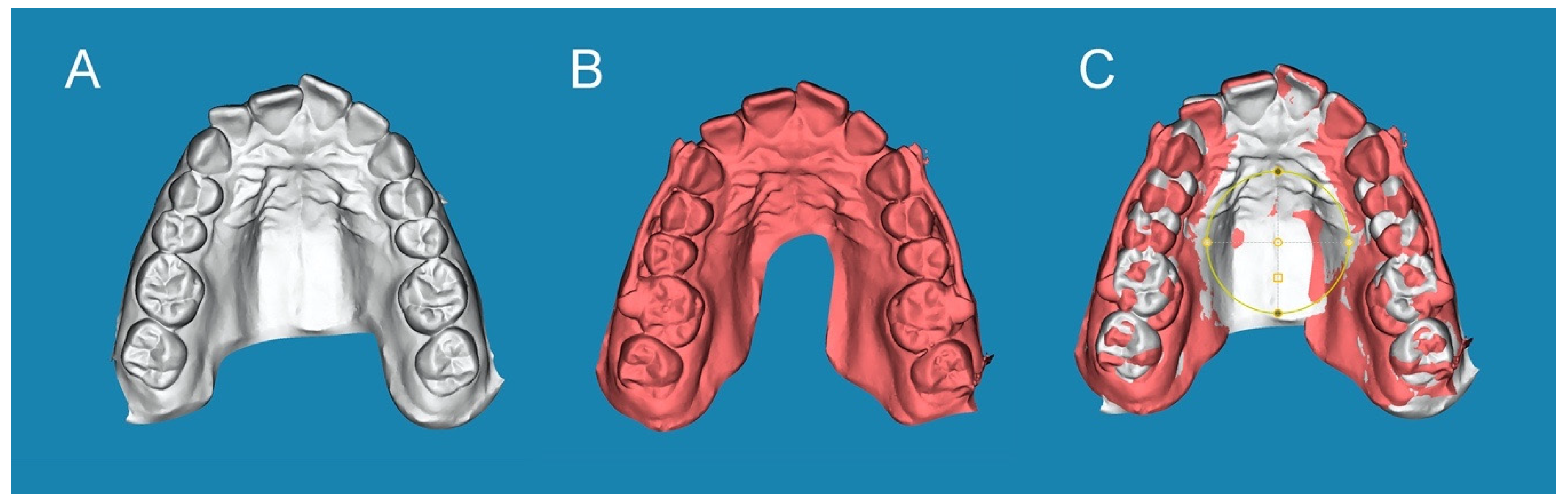
2.3. Alignment Procedure
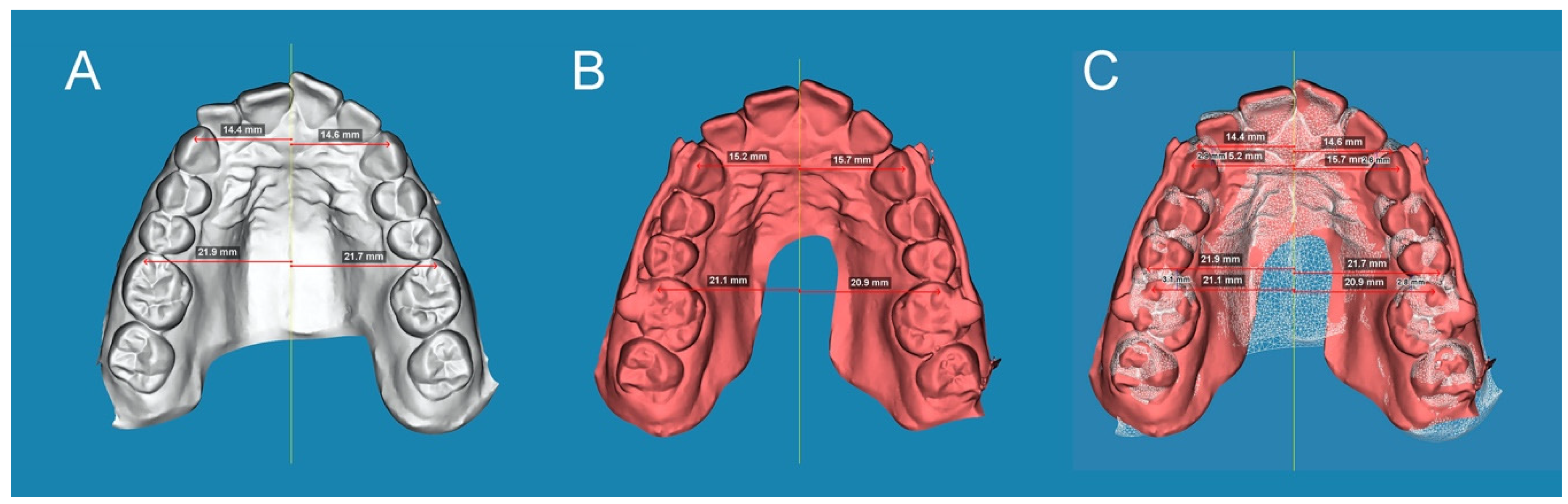
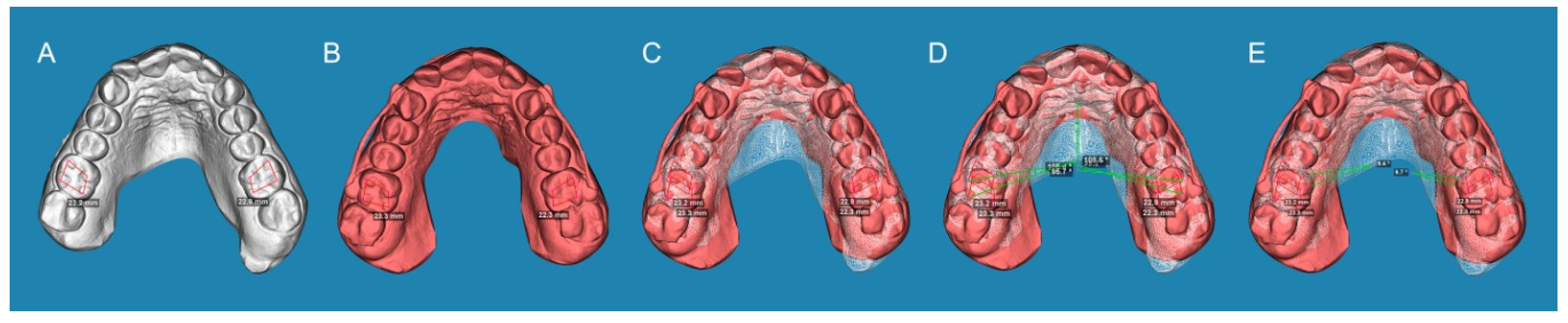
2.4. Measurement Procedure
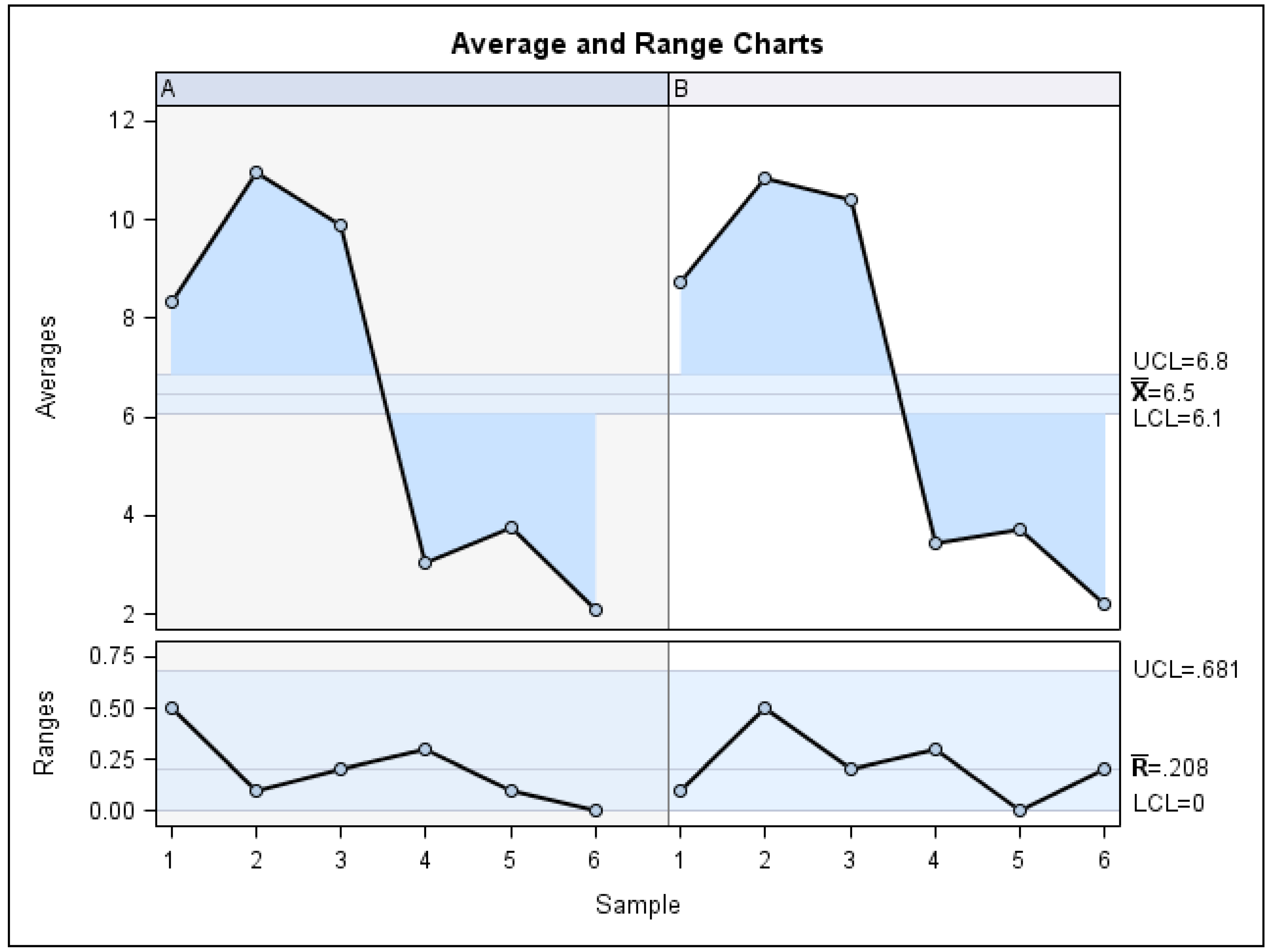
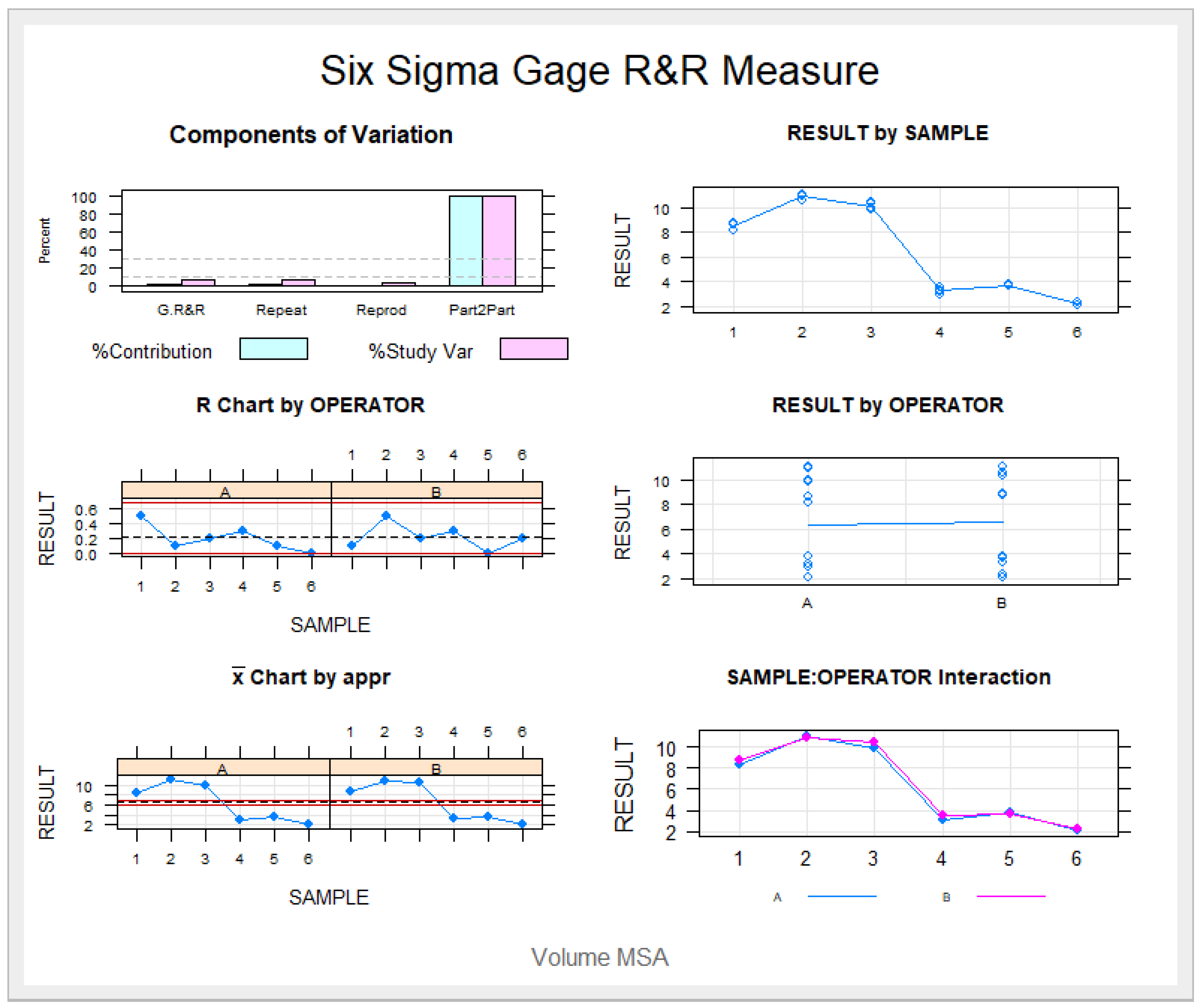
2.5. Validation of the Repeatability and Reproducibility of the Technique
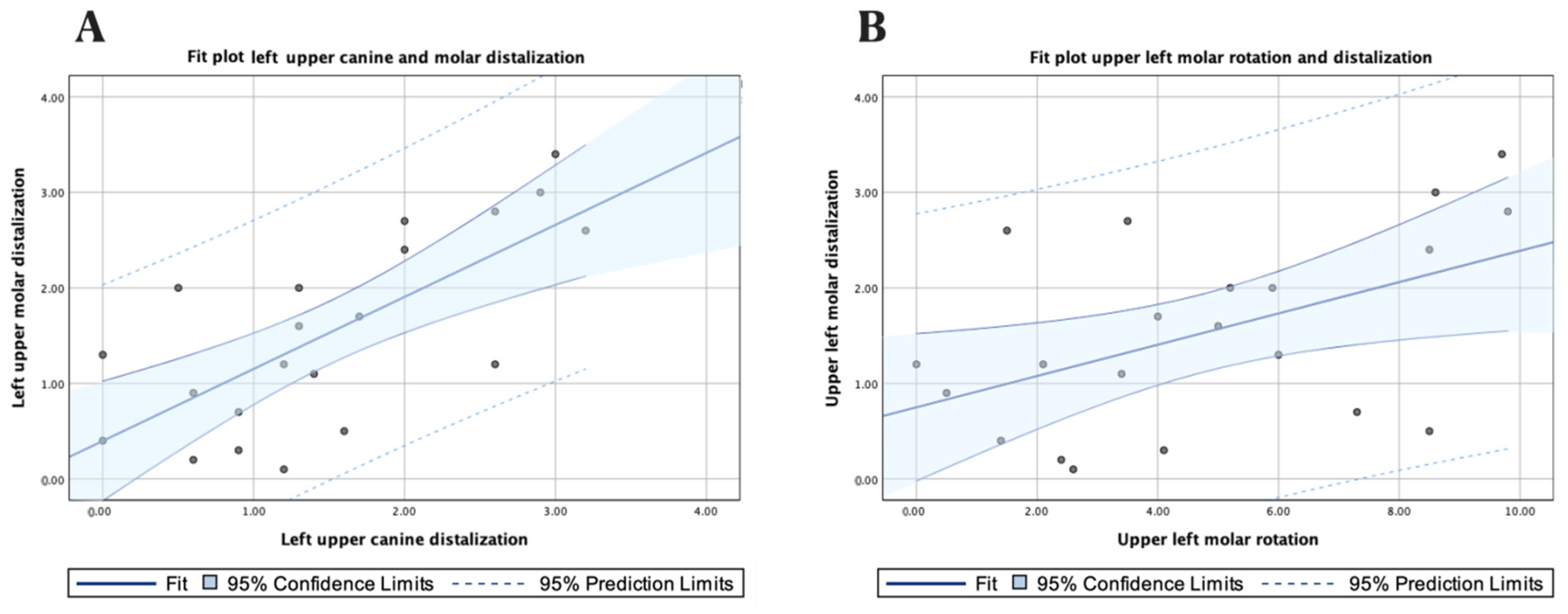
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yin, K.; Han, E.; Guo, J.; Yasumura, T.; Grauer, D.; Sameshima, G. Evaluating the treatment effectiveness and efficiency of Carriere Distalizer: A cephalometric and study model comparison of Class II appliances. Prog. Orthod. 2019, 20, 24. [Google Scholar] [CrossRef]
- McFarlane, B. Class II correction prior to orthodontics with the carriere distalizer. Int. J. Orthod. Milwaukee 2013, 24, 35–36. [Google Scholar] [PubMed]
- Fontana, M.; Cozzani, M.; Caprioglio, A. Non-compliance maxillary molar distalizing appliances: An overview of the last decade. Prog. Orthod. 2021, 13, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Kinzinger, G.; Eren, M.; Diedrich, P. Treatment effects of intraoral appliances with conventional anchorage designs for non-compliance maxillary molar distalization. A literature review. Eur. J. Orthod. 2008, 30, 558–571. [Google Scholar] [CrossRef] [PubMed]
- Sandifer, C.; English, J.; Colville, C.; Gallerano, R.; Akyalcin, S. Treatment effects of the Carrière distalizer using lingual arch and full fixed appliances. J. World Fed. Orthod. 2014, 3, e49–e54. [Google Scholar] [CrossRef]
- Antonarakis, G.S.; Kiliaridis, S. Maxillary molar distalization with non-compliance intramaxillary appliances in class II malocclusion: A systematic review. Angle Orthod. 2008, 78, 1133–1140. [Google Scholar] [CrossRef]
- Carrière, L. A new Class II distalizer. J. Clin. Orthod. 2004, 38, 224–231. [Google Scholar]
- Kim-Berman, H.; McNamara, J.A., Jr.; Lints, J.P.; McMullen, C.; Franchi, L. Treatment effects of the Carriere® Motion 3D™ appliance for the correction of Class II malocclusion in adolescents. Angle Orthod. 2019, 89, 839–846. [Google Scholar] [CrossRef]
- Schmid-Herrmann, C.U.; Delfs, J.; Mahaini, L.; Schumacher, E.; Hirsch, C.; Koehne, T.; Kahl-Nieke, B. Retrospective investigation of the 3D effects of the Carriere Motion 3D appliance using model and cephalometric superimposition. Clin. Oral Investig. 2023, 27, 631–643. [Google Scholar] [CrossRef]
- Hamilton, C.F.; Saltaji, H.; Preston, C.B.; Flores-Mir, C.; Tabbaa, S. Adolescent patients’ experience with the Carriere distalizer appliance. Eur. J. Paediatr. Dent. 2013, 14, 219–224. [Google Scholar]
- McNamara, J.A., Jr.; Franchi, L.; McClatchey, L.M.; Kim-Berman, H. Evaluating new approaches to the treatment of Class II and Class III malocclusions: The Carriere Motion appliance. In Embracing Novel Technologies in Dentistry and Orthodontics; Shroff B, Ed.; Monograph 57, Craniofacial Growth Series; Department of Orthodontics and Pediatric Dentistry and Center for Human Growth and Development, The University of Michigan: Ann Arbor, MI, USA, 2021. [Google Scholar]
- Rodrigues, H. Unilateral application of the Carriere distalizer. J. Clin. Orthod. 2011, 45, 177–180. [Google Scholar]
- Rodrigues, H. Nonextractin treatment of a Class II Open Bite in an Adult Patient. J. Clin. Orthod. 2012, 46, 367–371. [Google Scholar]
- Singh, D. Intraoral Approaches for Maxillary Molar Distalization: Case Series. J. Clin. Diagn. Res. 2017, 11, ZR01–ZR04. [Google Scholar] [CrossRef] [PubMed]
- Pardo Lopez, B.; DeCaros Villafranca, F.; Cobo Plana, J. Distalizer treatment of an adult Class II Division 2 malocclusion. J. Clin. Orthod. 2006, 40, 561–565. [Google Scholar]
- Areepong, D.; Kim, K.B.; Oliver, D.R.; Ueno, H. The Class II Carriere Motion appliance. Angle Orthod. 2020, 90, 491–499. [Google Scholar] [CrossRef]
- Luca, L.; Francesca, C.; Daniela, G.; Alfredo, S.G.; Giuseppe, S. Cephalometric analysis of dental and skeletal effects of Carriere Motion 3D appliance for Class II malocclusion. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 659–665. [Google Scholar] [CrossRef]
- Barakat, D.; Bakdach, W.M.M.; Youssef, M. Treatment effects of Carriere Motion Appliance on patients with class II malocclusion: A systematic review and meta-analysis. Int. Orthod. 2021, 19, 353–364. [Google Scholar] [CrossRef]
- Wilson, B.; Konstantoni, N.; Kim, K.B.; Foley, P.; Ueno, H. Three-dimensional cone-beam computed tomography comparison of shorty and standard Class II Carriere Motion appliance. Angle Orthod. 2021, 91, 423–432. [Google Scholar] [CrossRef]
- Fouda, A.S.; Attia, K.H.; Abouelezz, A.M.; El-Ghafour, M.A.; Aboulfotouh, M.H. Anchorage control using miniscrews in comparison to Essix appliance in treatment of postpubertal patients with Class II malocclusion using Carrière Motion Appliance. Angle Orthod. 2022, 92, 45–54. [Google Scholar] [CrossRef]
- Hashem, A.S. Effect of second molar eruption on efficiency of maxillary first molar distalization using Carriere distalizer appliance. Dental Press J. Orthod. 2021, 26, e2119146. [Google Scholar] [CrossRef]
- Dahlquist, A.; Gebauer, U.; Ingervall, B. The effect of a transpalatal arch for the correction of first molar rotation. Eur. J. Orthod. 1996, 18, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Henry, R. Relationship of the maxillary first permanent molar in normal occlusion and malocclusion. Am. J. Orthod. 1956, 42, 288–306. [Google Scholar] [CrossRef]
- Friel, S. Determination of the angle of rotation of the upper first molar to the median raphe of the palate in different types of malocclusion. Dental Pract. 1959, 9, 72–78. [Google Scholar]
- Ricketts, R. Occlusion—The medium of dentistry. J. Prosthet. Dent. 1969, 21, 39–60. [Google Scholar] [CrossRef] [PubMed]
- Ten Hoeve, A. Palatal bar and lip bumper in non-extraction treatment. J. Clin. Orthod. 1985, 19, 272–291. [Google Scholar]
- Jamilian, A.; Showkatbakhsh, R.; Amiri, S.S. Treatment effects of the R-appliance and twin block in Class II division 1 malocclusion. Eur. J. Orthod. 2011, 33, 354–358. [Google Scholar] [CrossRef]
- Chiu, P.P.; McNamara, J.A., Jr.; Franchi, L. A comparison of two intraoral molar distalization appliances: Distal jet versus pendulum. Am. J. Orthod. Dent. Orthop. 2005, 128, 353–365. [Google Scholar] [CrossRef]
- Haydar, S.; Üner, O. Comparison of Jones jig molar distalization appliance with extraoral traction. Am. J. Orthod. Dent. Orthop. 2000, 117, 49–53. [Google Scholar] [CrossRef]
- Bolla, E.; Muratore, F.; Carano, A.; Jay Bowman, S. Evaluation of maxillary molar distalization with the distal jet: A comparison with other contemporary methods. Angle Orthod. 2002, 72, 481–494. [Google Scholar]
- Chaqués-Asensi, J.; Kalra, V. Effects of the pendulum appliance on the dentofacial complex. J. Clin. Orthod. 2001, 35, 254–257. [Google Scholar]
- Van der Linden, F.P.G.M. Changes in the position of posterior teeth in relation to ruga points Am. J. Orthod. 1978, 74, 142–161. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.R. Rotated maxillary molars and their contribution to crowding and malocclusion. J. Gen. Orthod. 1991, 2, 26–27. [Google Scholar] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|
| Left upper canine displacement | 21 | 1.500 | 0.953 | 0 | 3.4 |
| Right upper canine displacement | 21 | 1.329 | 1.152 | 0 | 4.7 |
| Left upper molar displacement | 21 | 1.529 | 1.006 | 0.1 | 3.4 |
| Right upper molar displacement | 21 | 1.400 | 1.133 | 0 | 4 |
| Left upper molar derotation angle | 21 | 4.762 | 3.054 | 0 | 9.8 |
| Right upper molar derotation angle | 21 | 6.748 | 5.673 | 0 | 21.5 |
| n | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|
| Upper canine displacement | 42 | 1.414 | 1.048 | 0 | 4.7 |
| Upper molar displacement | 42 | 1.464 | 1.060 | 0 | 4 |
| Upper molar derotation angle | 42 | 5.755 | 4.611 | 0 | 21.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nercellas Rodríguez, A.R.; Colino Gallardo, P.; Zubizarreta-Macho, Á.; Colino Paniagua, C.; Alvarado Lorenzo, A.; Albaladejo Martínez, A. A New Digital Method to Quantify the Effects Produced by Carriere Motion Appliance. J. Pers. Med. 2023, 13, 859. https://doi.org/10.3390/jpm13050859
Nercellas Rodríguez AR, Colino Gallardo P, Zubizarreta-Macho Á, Colino Paniagua C, Alvarado Lorenzo A, Albaladejo Martínez A. A New Digital Method to Quantify the Effects Produced by Carriere Motion Appliance. Journal of Personalized Medicine. 2023; 13(5):859. https://doi.org/10.3390/jpm13050859
Chicago/Turabian StyleNercellas Rodríguez, Aldara Rosalía, Pedro Colino Gallardo, Álvaro Zubizarreta-Macho, Carlos Colino Paniagua, Alfonso Alvarado Lorenzo, and Alberto Albaladejo Martínez. 2023. "A New Digital Method to Quantify the Effects Produced by Carriere Motion Appliance" Journal of Personalized Medicine 13, no. 5: 859. https://doi.org/10.3390/jpm13050859
APA StyleNercellas Rodríguez, A. R., Colino Gallardo, P., Zubizarreta-Macho, Á., Colino Paniagua, C., Alvarado Lorenzo, A., & Albaladejo Martínez, A. (2023). A New Digital Method to Quantify the Effects Produced by Carriere Motion Appliance. Journal of Personalized Medicine, 13(5), 859. https://doi.org/10.3390/jpm13050859