
The Magnitude of Cardiovascular Disease Risk Factors in Seafarers from 1994 to 2021: A Systematic Review and Meta-Analysis

 ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
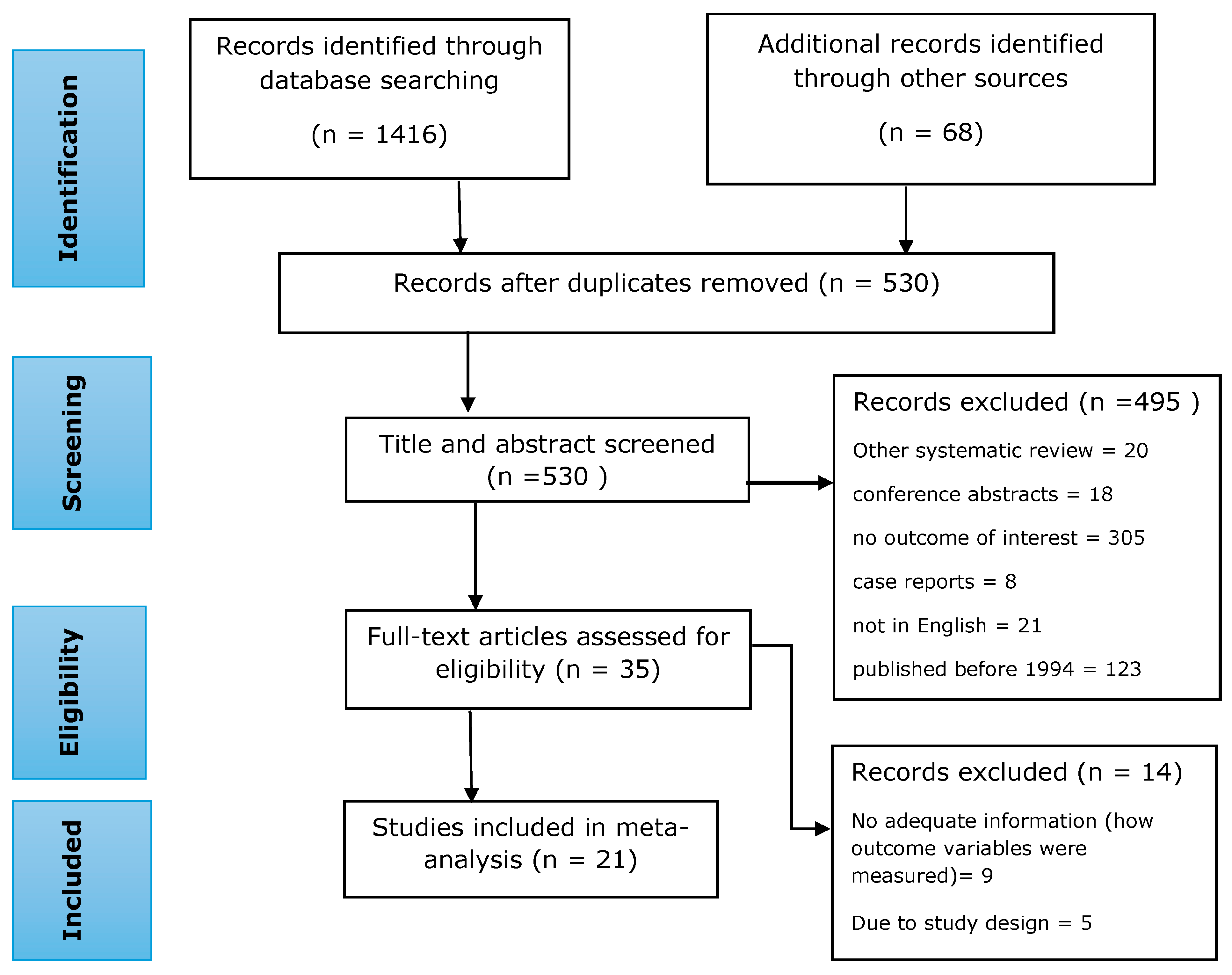
2. Methods
2.1. Research Questions
2.2. Search Strategy and Data Sources
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Outcome Variables
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Operational Definition of Outcome Variables in the Included Studies
3.3. Prevalence of CVD Risk Factors
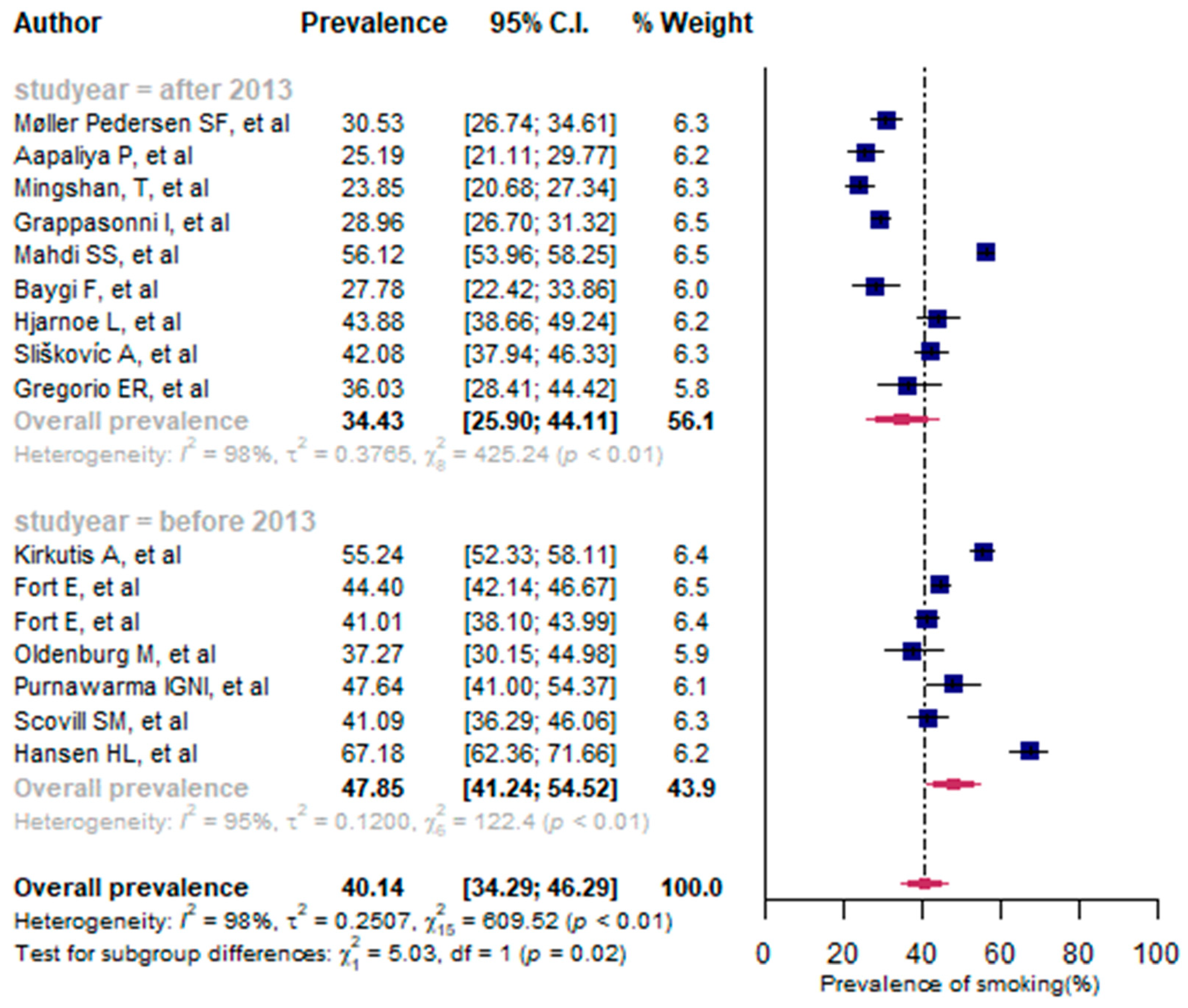
3.3.1. Prevalence of Smoking
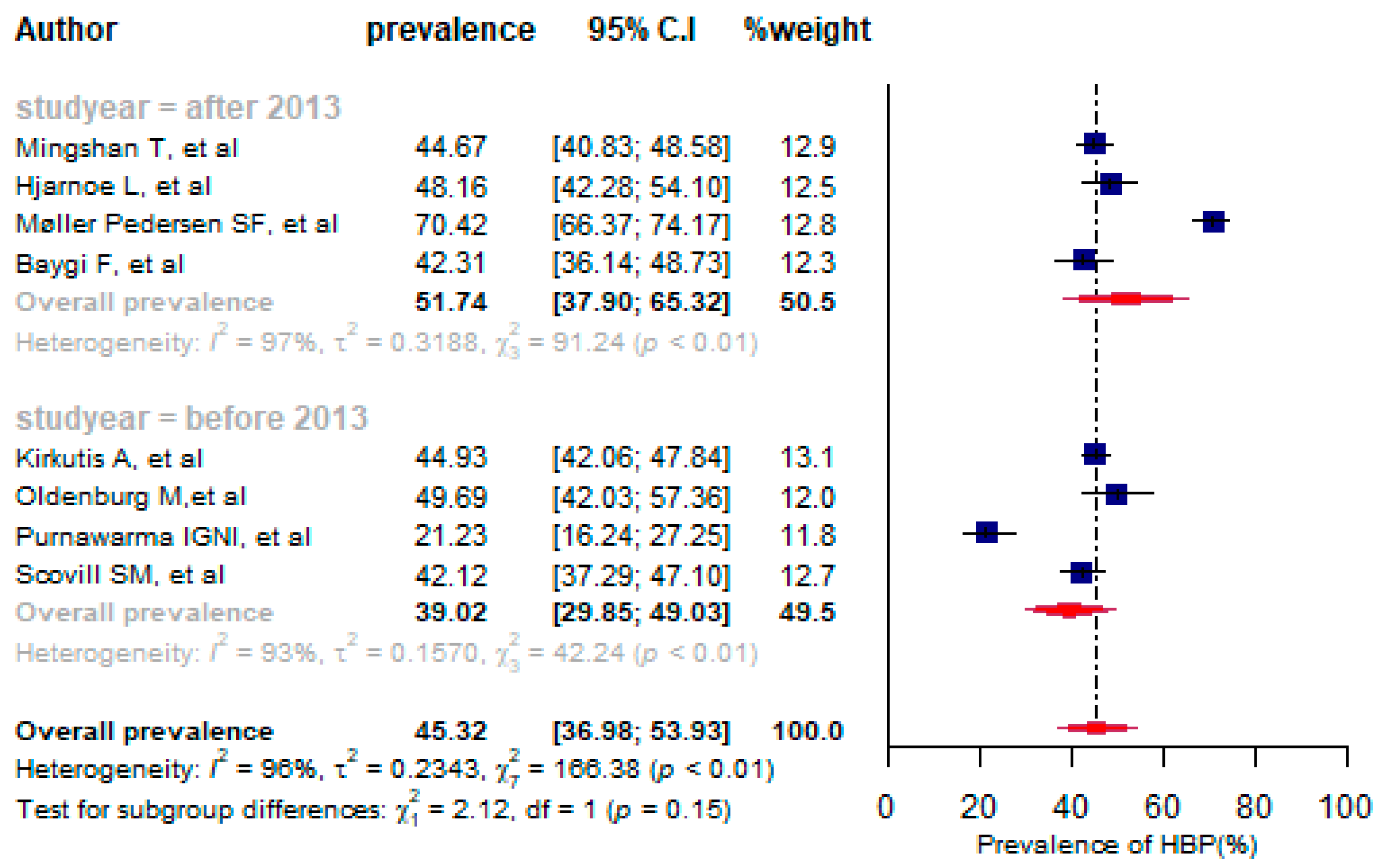
3.3.2. Prevalence of High Blood Pressure
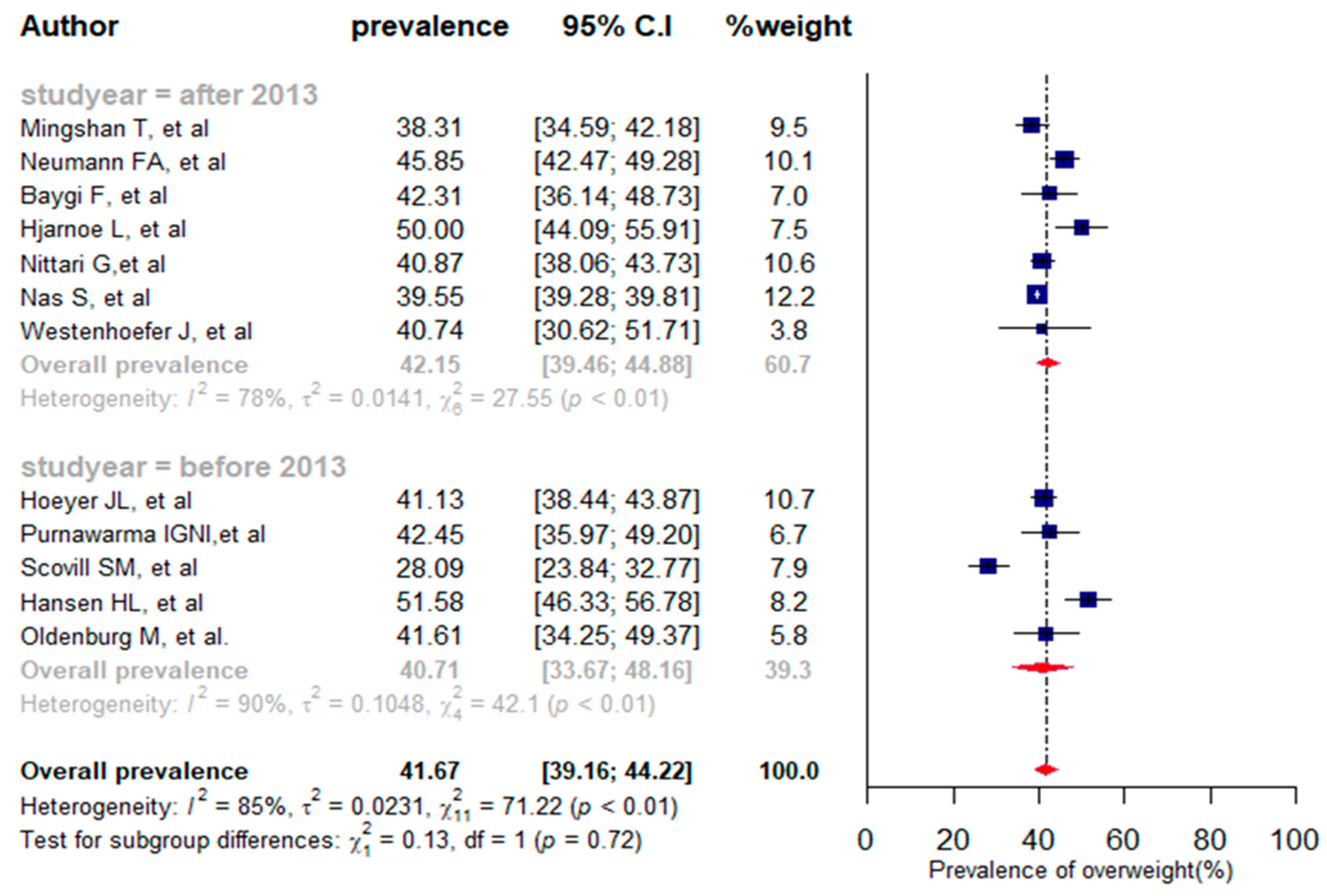
3.3.3. Prevalence of Overweight
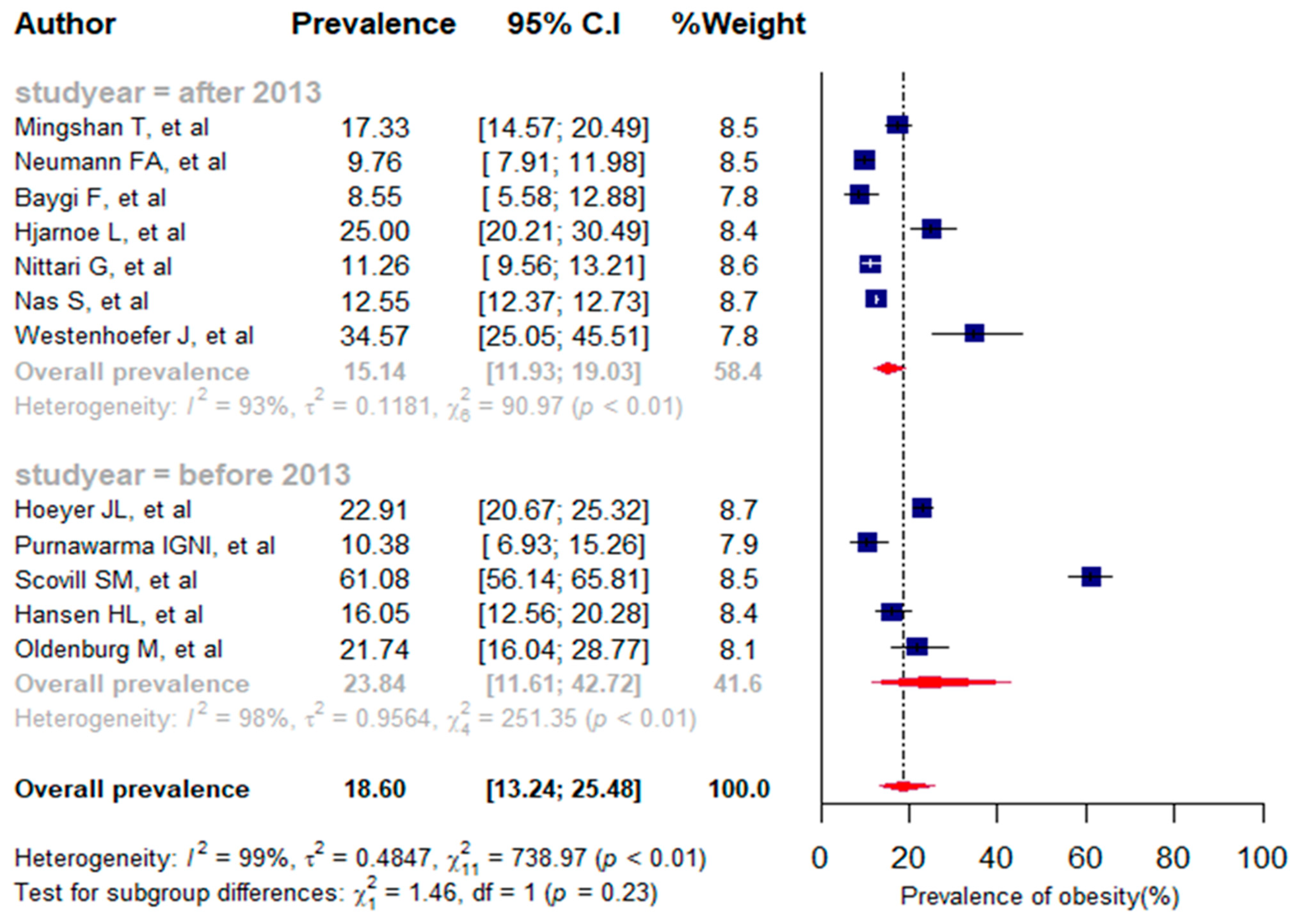
3.3.4. Prevalence of Obesity
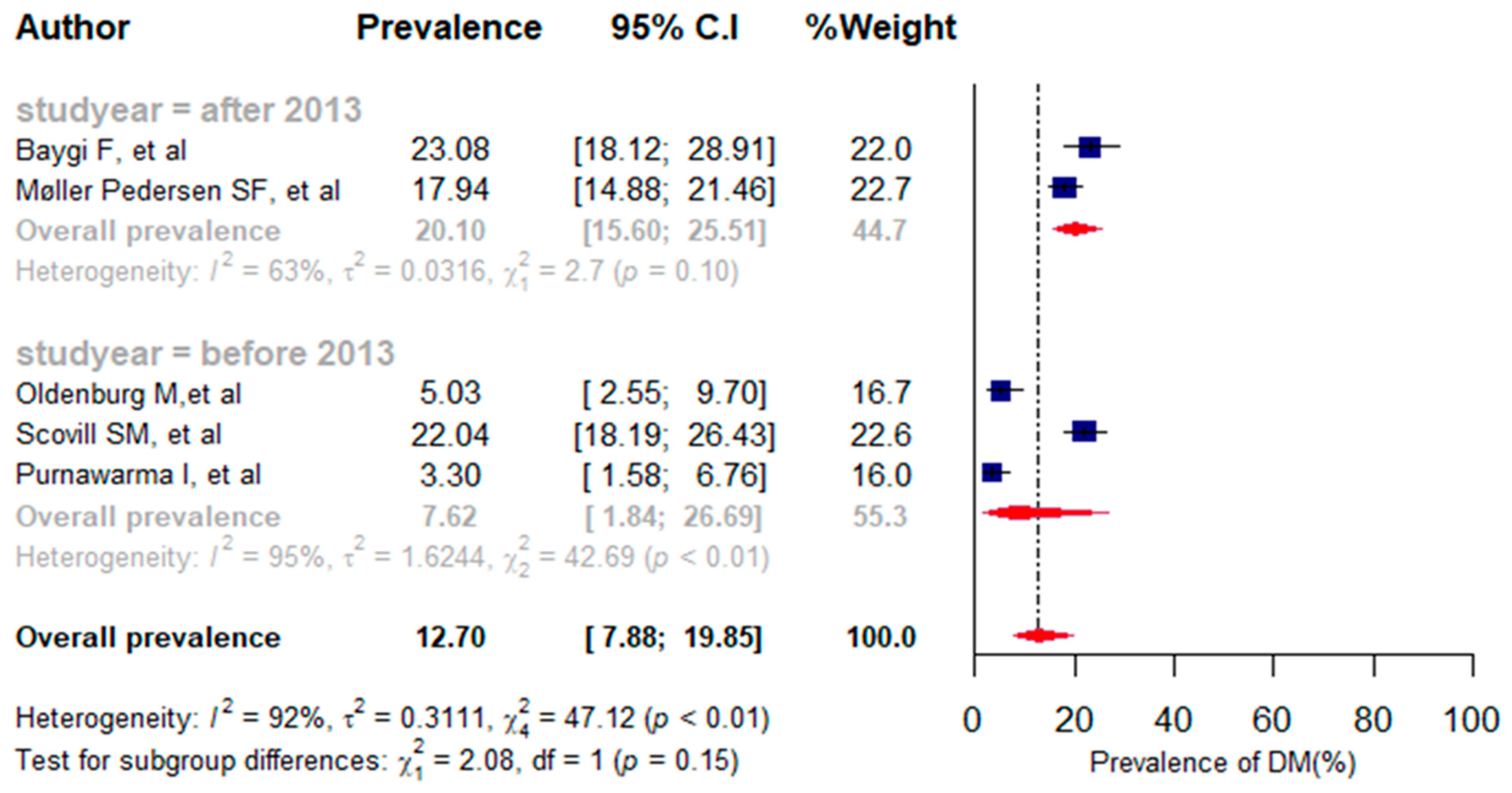
3.3.5. Prevalence of Diabetes Mellitus
3.3.6. Prevalence of Alcohol Consumption
3.4. Publication Bias
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baddour, L.M.; Addolorato, G.; Ammirati, E.; Mensah, G.; Johnson, C.; Rwegerera, G.M.; Roth, G.A. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar]
- Roberts, S.E.; Jaremin, B. Cardiovascular disease mortality in British merchant shipping and among British seafarers ashore in Britain. Int. Marit. Health 2010, 62, 107–116. [Google Scholar] [PubMed]
- Grappasonni, I.; Petrelli, F.; Amenta, F. Deaths on board ships assisted by the Centro Internazionale Radio Medico in the last 25 years. Travel. Med. Infect. Dis. 2012, 10, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Hansen, H.L. Surveillance of deaths on board Danish merchant ships, 1986-93: Implications for prevention. Occup. Environ. Med. 1996, 53, 269–275. [Google Scholar] [CrossRef]
- Bogdan, J.; Kotulak, E. Myocardial infarction (MI) at the work-site among Polish seafarers. The risk and the impact of occupational factors. Int. Marit. Health 2003, 54, 26–39. [Google Scholar]
- Jaremin, B.; Kotulak, E.; Starnawska, M.; Tomaszunas, S. Causes and circumstances of deaths of polish seafarers during sea voyages. J. Travel. Med. 1996, 3, 91–95. [Google Scholar] [CrossRef]
- Roberts, S.E. Mortality from disease among seafarers in British merchant shipping (1976–1995). Int. Marit. Health 2002, 53, 43–58. [Google Scholar]
- Jensen, O.C.; Laursen, F.V.; Sørensen, F.L. International surveillance of seafarers’ health and working environment. A pilot study of the method. Preliminary report. Int. Marit. Health 2001, 52, 59–67. [Google Scholar]
- Kirkutis, A.; Norkiene, S.; Griciene, P.; Gricius, J.; Yang, S.; Gintautas, J. Prevalence of hypertension in Lithuanian mariners. Proc. West. Pharmacol. Soc. 2004, 47, 71–75. [Google Scholar]
- Hansen, H.L.; Dahl, S.; Bertelsen, B.; Brix, J. Lifestyle, nutritional status and working conditions of Danish sailors. Travel Med. Int. 1994, 12, 139–143. [Google Scholar]
- Kivimäki, M.; Kawachi, I. Work Stress as a Risk Factor for Cardiovascular Disease. Curr. Cardiol. Rep. 2015, 17, 74. [Google Scholar] [CrossRef] [PubMed]
- Sagaro, G.G.; Dicanio, M.; Battineni, G.; Samad, M.A.; Amenta, F. Incidence of occupational injuries and diseases among seafarers: A descriptive epidemiological study based on contacts from onboard ships to the Italian Telemedical Maritime Assistance Service in Rome, Italy. BMJ Open. 2021, 11, e044633. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, M.; Jensen, H.J. Stress and strain among seafarers related to the occupational groups. Int. J. Environ. Res. Public. Health 2019, 16, 1153. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, M.; Jensen, H.J.; Latza, U.; Baur, X. Seafaring stressors aboard merchant and passenger ships. Int. J. Public Health 2009, 54, 96–105. [Google Scholar] [PubMed]
- Slišković, A.; Penezić, Z. Occupational stressors, risks and health in the seafaring population. Rev. Psychol. 2016, 22, 29–39. [Google Scholar] [CrossRef]
- Oldenburg, M.; Baur, X.; Schlaich, C. Occupational Risks and Challenges of Seafaring. 2010. Available online: https://www.jstage.jst.go.jp/article/joh/advpub/0/advpub_K10004/_article/-char/ja/ (accessed on 22 November 2021).
- Hjarnoe, L.; Leppin, A. A risky occupation? (Un) healthy lifestyle behaviors among Danish seafarers. Health Promot. Int. 2014, 29, 720–729. [Google Scholar] [CrossRef]
- Filikowski, J.; Rzepiak, M.; Renke, W.; Winnicka, A.; Smolińska, D. Selected risk factors of ischemic heart disease in Polish seafarers. Preliminary report. Int. Marit. Health 2003, 54, 40–46. [Google Scholar]
- Geving, I.H.; Jorgensen, K.U.; Le Thi, M.S.; Sandsund, M. Physical activity levels among offshore fleet seafarers. Int. Marit. Health 2007, 58, 103–114. [Google Scholar]
- Pougnet, R.; Pougnet, L.; Loddé, B.L.; Canals-Pol, M.L.; Jegaden, D.; Lucas, D.; Dewitte, J.D. Cardiovascular risk factors in seamen and fishermen: Review of literature. Int. Marit. Health 2013, 64, 107–113. [Google Scholar]
- Stoll, E.; Püschel, K.; Harth, V.; Oldenburg, M. Prevalence of alcohol consumption among seafarers and fishermen. Int. Marit. Health 2020, 71, 265–274. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of Observational Studies in Epidemiology: A Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar]
- Munn, Z.; Moola, S.; Riitano, D.; Lisy, K. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int. J. Health Policy Manag. 2014, 3, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Kassa, G.M. Mother-to-child transmission of HIV infection and its associated factors in Ethiopia: A systematic review and meta-analysis. BMC Infect. Dis. 2018, 18, 216. [Google Scholar] [CrossRef] [PubMed]
- Kassa, G.M.; Abajobir, A.A. Prevalence of common mental illnesses in Ethiopia: A systematic review and meta-analysis. Neurol. Psychiatry Brain Res. 2018, 30, 74–85. [Google Scholar]
- R Core Team, R. R: A Language and Environment for Statistical; Computing Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088. [Google Scholar] [CrossRef]
- Cochran, W.G. The Combination of Estimates from Different Experiments. Biometrics 2016, 10, 101–129. [Google Scholar] [CrossRef]
- Grant, J.; Hunter, A. Measuring inconsistency in knowledgebases. J. Intell. Inf. Syst. 2006, 27, 159–184. [Google Scholar] [CrossRef]
- Goto, A.; Arah, O.A.; Goto, M.; Terauchi, Y.; Noda, M. Severe hypoglycaemia and cardiovascular disease: Systematic review and meta-analysis with bias analysis. BMJ 2013, 347, 103. [Google Scholar] [CrossRef] [PubMed]
- Hoeyer, J.L.; Hansen, H.L. Obesity among Danish seafarers. Int. Marit. Health 2005, 56, 48–55. [Google Scholar] [PubMed]
- Oldenburg, M.; Jensen, H.J.; Latza, U.; Baur, X. Coronary risks among seafarers aboard German-flagged ships. Int. Arch. Occup. Environ. Health 2008, 81, 735–741. [Google Scholar] [CrossRef]
- Fort, E.; Massardier-Pilonchery, A.; Bergeret, A. Alcohol and nicotine dependence in French seafarers. Int. Marit. Health 2009, 60, 18–28. [Google Scholar]
- Fort, E.; Massardier-Pilonchéry, A.; Bergeret, A. Psychoactive substances consumption in French fishermen and merchant seamen. Int. Arch. Occup. Environ. Health 2010, 83, 497–509. [Google Scholar] [CrossRef]
- Purnawarma Irwin, G.N.I.; Jensen, O.C.; Canals, M.L.; García Bercedo, R.; Castaños Urkullu, A. Prevalence of cardiovascular risks factors and 10 year predictions of coronary heart disease in seafarers of Pertamina shipping (Indonesia). Med. Marit. 2011, 11, 49–60. [Google Scholar]
- Scovill, S.M.; Roberts, T.K.; McCarty, D.J. Health characteristics of inland waterway merchant marine captains and pilots. Occup. Med. 2012, 62, 638–641. [Google Scholar] [CrossRef]
- Møller Pedersen, S.F.; Jepsen, J.R. The metabolic syndrome among Danish seafarers. Int. Marit. Health 2013, 64, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Nas, S.; Fışkın, R. A research on obesity among Turkish seafarers. Int. Marit. Health 2014, 65, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Aapaliya, P.; Shinde, K.; Deswal, A.K.; Mohapatra, S.; Saleem, S.; Mangal, R.; Bithu, A.; Bithu, A.S.; Maurya, S.P.; Sanadhya, S.; et al. Assessment of oral health among seafarers in Mundra Port, Kutch, Gujarat: A cross-sectional study. Int. Marit. Health 2015, 66, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Mingshan, T.; Jepsen, J.R. Hypertension among Danish Seafarers. Available online: https://journals.viamedica.pl/international_maritime_health/article/view/48265 (accessed on 11 June 2020).
- Mahdi, S.S.; Sibilio, F.; Amenta, F. Dental hygiene habits and oral health status of seafarers. Int. Marit. Health 2016, 67, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Baygi, F.; Jensen, O.C.; Qorbani, M.; Farshad, A.; Salehi, S.A.; Mohammadi-Nasrabadi, F.; Asayesh, H.; Shidfar, F. Prevalence and associated factors of cardio-metabolic risk factors in Iranian seafarers. Int. Marit. Health 2016, 67, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Gregorio, E.R., Jr.; Kobayashi, J.; Medina, J.R.C.; Simbulan, N.P. Knowledge, attitudes, and related practices of Filipino seafarers regarding cardiovascular diseases. Int. Marit. Health 2016, 67, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Sliškovíc, A.; Penezíc, Z. Lifestyle factors in Croatian seafarers as relating to health and stress on board. Work 2017, 56, 371–380. [Google Scholar] [CrossRef]
- Westenhoefer, J.; von Katzler, R.; Jensen, H.J.; Zyriax, B.C.; Jagemann, B.; Harth, V.; Oldenburg, M. Cultural differences in food and shape related attitudes and eating behavior are associated with differences of Body Mass Index in the same food environment: Cross-sectional results from the Seafarer Nutrition Study of Kiribati and European seafarers on merchant ships. BMC Obes. 2018, 5, 1. [Google Scholar] [CrossRef]
- Grappasonni, I.; Scuri, S.; Petrelli, F.; Nguyen, C.T.T.; Sibilio, F.; Di Canio, M.; Samad, M.A.; Amenta, F. Survey on smoking habits among seafarers. Acta Biomed. 2019, 90, 497–505. [Google Scholar]
- Nittari, G.; Tomassoni, D.; Di Canio, M.; Traini, E.; Pirillo, I.; Minciacchi, A.; Amenta, F. Overweight among seafarers working on board merchant ships. BMC Public Health 2019, 19, 45. [Google Scholar] [CrossRef]
- Neumann, F.A.; Belz, L.; Dengler, D.; Harth, V.; von Münster, T.; Westenhöfer, J.; Oldenburg, M.; Zyriax, B.C. Eating behaviour and weight development of European and Asian seafarers during stay on board and at home. J. Occup. Med. Toxicol. 2021, 16, 41. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ.—Tech. Rep. Ser. 2000, 894, 252. [Google Scholar]
- Sagaro, G.G.; Battineni, G.; Di Canio, M.; Minciacchi, A.; Nittari, G.; Amenta, F. A descriptive epidemiological study of cardiovascular diseases among seafarers. Int. Marit. Health 2021, 72, 252–258. [Google Scholar] [CrossRef]
- The International Convention on Standards of Training, Certification and Watchkeeping for Seafarers (STCW). International Convention on Standards of Training, Certification and Watchkeeping for Seafarers (STCW). 1978. Available online: https://www.imo.org/en/About/Conventions/Pages/International-Convention-on-Standards-of-Training,-Certification-and-Watchkeeping-for-Seafarers-(STCW).aspx (accessed on 25 October 2021).
- ILO Labour Convention. Convention MLC, 2006—Maritime Labour Convention, 2006 (MLC, 2006). 2006. Available online: https://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C186 (accessed on 29 May 2020).
- ILO Labour Convention. Health Protection and Medical Care (Seafarers) Convention, 2006 (No. 164). 2006. Available online: https://www.ilo.org/dyn/normlex/en/f?p=1000:12100:::NO:12100:P12100_INSTRUMENT_ID:312309 (accessed on 6 October 2019).
- Sagaro, G.G.; Di Canio, M.; Amenta, F. Correlation between body mass index and blood pressure in seafarers. Clin. Exp. Hypertens. 2021, 43, 189–195. [Google Scholar] [CrossRef]
- Sagaro, G.G.; Battineni, G.; Di Canio, M.; Amenta, F. Self-reported modifiable risk factors of cardiovascular disease among seafarers: A cross-sectional study of prevalence and clustering. J. Pers. Med. 2021, 11, 512. [Google Scholar] [CrossRef]
- The International Convention on Standards of Training, Certification and Watchkeeping for Seafarers (STCW). Stcw a Guide For Seafarers Taking into Account the 2010 Manila Amendments. Available online: https://www.mptusa.com/pdf/STCW_guide_english.pdf (accessed on 8 May 2023).
- Hansen, H.L.; Hjarnoe, L.; Jepsen, J.R. Obesity continues to be a major health risk for Danish seafarers and fishermen. Int. Marit. Health 2011, 62, 98–103. [Google Scholar]
- Oldenburg, M.; Rieger, J.; Sevenich, C.; Harth, V. Nautical officers at sea: Emergency experience and need for medical training. J. Occup. Med. Toxicol. 2014, 9, 19. [Google Scholar] [CrossRef]
- Henny, C.; Hartington, K.; Scott, S.; Tveiten, A.; Canals, L. The business case for telemedicine. Int. Marit. Health 2013, 64, 129–135. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author Name and Year | Study Design | Sample Size | Prevalence (%) | Quality Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| HBP | Smoking | Diabetes Mellitus | Overweight | Obesity | Alcohol Use | ||||
| Hansen, H.L., et al., 1994 [10] | Cross-sectional | 390 | NA | 67.2 | NA | 51.6 | 16.1 | NA | 7 |
| Kirkutis, A., et al., 2004 [9] | Cross-sectional | 1135 | 44.9 | 55.2 | NA | NA | NA | 82.6 | 9 |
| Hoeyer, J.L., et al., 2005 [37] | Retrosp. Cross-sectional | 1257 | NA | NA | NA | 41 | 22.9 | NA | 8 |
| Oldenburg, M., et al., 2008 [38] | Cross-sectional | 161 | 49.7 | 37.3 | 5 | 41.6 | 21.7 | 73.9 | 9 |
| Fort, E., et al., 2009 [39] | Cross-sectional | 1847 | NA | 44 | NA | NA | NA | NA | 6 |
| Fort, E., et al., 2010 [40] | Cross-sectional | 1068 | NA | 41.4 | NA | NA | NA | 8.0 | 9 |
| Purnawarma, I., et al., 2011 [41] | Cross-sectional | 212 | 21.2 | 47.6 | 3.3 | 42.5 | 10.4 | NA | 7 |
| Scovill, S.M., et al., 2012 [42] | Cross-sectional | 387 | 42 | 41 | 22 | 28 | 61 | NA | 7 |
| Møller Pedersen, S.F., et al., 2013 [43] | Cross-sectional | 524 | 70.4 | 30.6 | 17.9 | NA | NA | 18.6 | 4 |
| Hjarnoe, L., et al., 2014 [17] | Cross-sectional | 272 | 48 | 44 | NA | 50 | 25 | NA | 5 |
| Nas, S., et al., 2014 [44] | Retrosp. Cross-sectional | 131,152 | NA | NA | NA | 39.6 | 12.5 | NA | 4 |
| Aapaliya, P., et al., 2015 [45] | Cross-sectional | 385 | NA | 25.2 | NA | NA | NA | 14.3 | 4 |
| Mingshan, T., et al., 2016 [46] | Cross-sectional | 629 | 44.7 | 23.9 | NA | 38.3 | 17.3 | 71.9 | 7 |
| Mahdi, S.S., et al., 2016 [47] | Cross-sectional | 2060 | NA | 56.11 | NA | NA | NA | 11.5 | 5 |
| Baygi, F., et al., 2016 [48] | Cross-sectional | 234 | 42.3 | 27.8 | 23.1 | 42.5 | 8.6 | NA | 6 |
| Gregorio, E.R., et al., 2016 [49] | Cross-sectional | 136 | NA | 36.0 | NA | NA | NA | 79.4 | 5 |
| Sliškovíc, A., et al., 2017 [50] | Cross-sectional | 530 | NA | 42.0 | NA | NA | NA | 41.7 | 6 |
| Westenhoefer, J., et al., 2018 [51] | Cross-sectional | 81 | NA | NA | NA | 40.7 | 34.6 | NA | 5 |
| Grappasonni, I., et al., 2019 [52] | Cross-sectional | 1478 | NA | 28.9 | NA | NA | NA | 19.5 | 9 |
| Nittari, G., et al., 2019 [53] | Retrosp.cross-sectional | 1155 | NA | NA | NA | 40.8 | 11.2 | NA | 5 |
| Neumann, F.A., et al., 2021 [54] | Cross-sectional | 820 | NA | NA | NA | 45.8 | 9.8 | NA | 8 |
| Age Group (Years) | Pooled Prevalence (95% CI) | I2 (p-Value) | |
|---|---|---|---|
| Overweight | 16–24 | 25.64% (18.43–34.48) | 77% (0.04) |
| 25–44 | 41.49% (37.25–45.86) | 80% (0.03) | |
| 45–66 | 48.84% (43.66–54.04) | 84% (0.001) | |
| Obesity | 16–24 | 5.10% (2.05–12.10) | 87% (0.001) |
| 25–44 | 15.14% (10.30–21.69) | 95% (0.001) | |
| 45–66 | 26.74% (20.13–34.59) | 94% (0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sagaro, G.G.; Angeloni, U.; Marotta, C.; Nittari, G.; Rezza, G.; Silenzi, A.; Battineni, G.; Amenta, F. The Magnitude of Cardiovascular Disease Risk Factors in Seafarers from 1994 to 2021: A Systematic Review and Meta-Analysis. J. Pers. Med. 2023, 13, 861. https://doi.org/10.3390/jpm13050861
Sagaro GG, Angeloni U, Marotta C, Nittari G, Rezza G, Silenzi A, Battineni G, Amenta F. The Magnitude of Cardiovascular Disease Risk Factors in Seafarers from 1994 to 2021: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2023; 13(5):861. https://doi.org/10.3390/jpm13050861
Chicago/Turabian StyleSagaro, Getu Gamo, Ulrico Angeloni, Claudia Marotta, Giulio Nittari, Giovanni Rezza, Andrea Silenzi, Gopi Battineni, and Francesco Amenta. 2023. "The Magnitude of Cardiovascular Disease Risk Factors in Seafarers from 1994 to 2021: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 13, no. 5: 861. https://doi.org/10.3390/jpm13050861
APA StyleSagaro, G. G., Angeloni, U., Marotta, C., Nittari, G., Rezza, G., Silenzi, A., Battineni, G., & Amenta, F. (2023). The Magnitude of Cardiovascular Disease Risk Factors in Seafarers from 1994 to 2021: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 13(5), 861. https://doi.org/10.3390/jpm13050861