
Delta Variant in the COVID-19 Pandemic: A Comparative Study on Clinical Outcomes Based on Vaccination Status

 , , , ,
, , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection: Clinical Characteristics and Blood Sample Collection
2.3. Statistical Analysis
3. Results
3.1. Patient’s Characteristics, Demographic Parameters, the Smoking Status, Symptoms on Hospital Admission, Comorbidities, Vaccine Type, and the Delay between Complete Vaccination–Infection (Table 1, Table 2, Table 3, Table 4 and Table 5)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Vaccinated, n = 44 1 | Unvaccinated, n = 153 1 | p-Value 2 |
|---|---|---|---|
| Sex | 0.008 | ||
| Females | 16 (36%) | 90 (59%) | |
| Males | 28 (64%) | 63 (41%) | |
| Age | 0.10 | ||
| Mean (SD) | 59 (16) | 64 (15) | |
| Median (IQR) | 62 (50, 72) | 66 (54, 74) | |
| Body Mass Index | 0.3 | ||
| Mean (SD) | 28.3 (4.8) | 29.0 (4.9) | |
| Median (IQR) | 27.7 (25.2, 31.2) | 28.0 (26.0, 32.6) |
| Characteristic | Vaccinated, n = 44 1 | Unvaccinated, n = 153 1 | p-Value 2 |
|---|---|---|---|
| Smoking status | 0.14 | ||
| Smoker | 10 (23%) | 41 (27%) | |
| Ex-smoker | 10 (23%) | 17 (11%) | |
| Non-smoker | 24 (55%) | 95 (62%) |
| Symptoms on Hospital Admission | Vaccinated, n = 44 1 | Unvaccinated, n = 153 1 | p-Value 2 |
|---|---|---|---|
| Fever | 0.7 | ||
| YES | 31 (70%) | 112 (73%) | |
| NO | 13 (30%) | 41 (27%) | |
| Chills | 0.2 | ||
| YES | 32 (73%) | 95 (62%) | |
| NO | 12 (27%) | 58 (38%) | |
| Cough | 0.6 | ||
| YES | 34 (77%) | 113 (74%) | |
| NO | 10 (23%) | 40 (26%) | |
| Dyspnea | 0.3 | ||
| YES | 24 (55%) | 97 (63%) | |
| NO | 20 (45%) | 56 (37%) | |
| Arthralgia | 0.7 | ||
| YES | 6 (14%) | 28 (18%) | |
| NO | 38 (86%) | 124 (81%) | |
| Myalgias | 0.8 | ||
| YES | 13 (30%) | 49 (32%) | |
| NO | 31 (70%) | 104 (68%) | |
| Diarrhea | 0.13 | ||
| YES | 1 (2.3%) | 16 (10%) | |
| NO | 43 (98%) | 137 (90%) |
| Comorbidities | Vaccinated, n = 44 1 | Unvaccinated, n = 153 1 | p-Value 2 |
|---|---|---|---|
| Obesity | 0.3 | ||
| YES | 16 (36%) | 68 (44%) | |
| NO | 28 (64%) | 85 (56%) | |
| Diabetes | 0.5 | ||
| YES | 15 (34%) | 43 (28%) | |
| NO | 29 (66%) | 109 (72%) | |
| Arterial Hypertension | 0.8 | ||
| YES | 26 (59%) | 94 (61%) | |
| NO | 18 (41%) | 59 (39%) | |
| Cardiovascular disease | 0.4 | ||
| YES | 21 (48%) | 63 (41%) | |
| NO | 23 (52%) | 90 (59%) | |
| Respiratory disease | 0.8 | ||
| YES | 8 (18%) | 31 (20%) | |
| NO | 36 (82%) | 122 (80%) | |
| Chronic kidney disease | 0.7 | ||
| YES | 2 (4.5%) | 12 (7.8%) | |
| NO | 42 (95%) | 141 (92%) | |
| CANCER | 0.5 | ||
| YES | 4 (9.1%) | 8 (5.2%) | |
| NO | 40 (91%) | 145 (95%) |
| Vaccin Manufacturer | Average Difference between Vaccination and Admission Date (Months) |
|---|---|
| BNT162b2 | 6 |
| ChAdOx1-S | 5 |
| Ad26.COV2.S | 2 |
3.2. Disease Severity Assessed by CT Score and Padua Score
3.3. Padua Score
3.4. Oxygen Therapy, Ventilation Requirement and the Dynamic of ABG
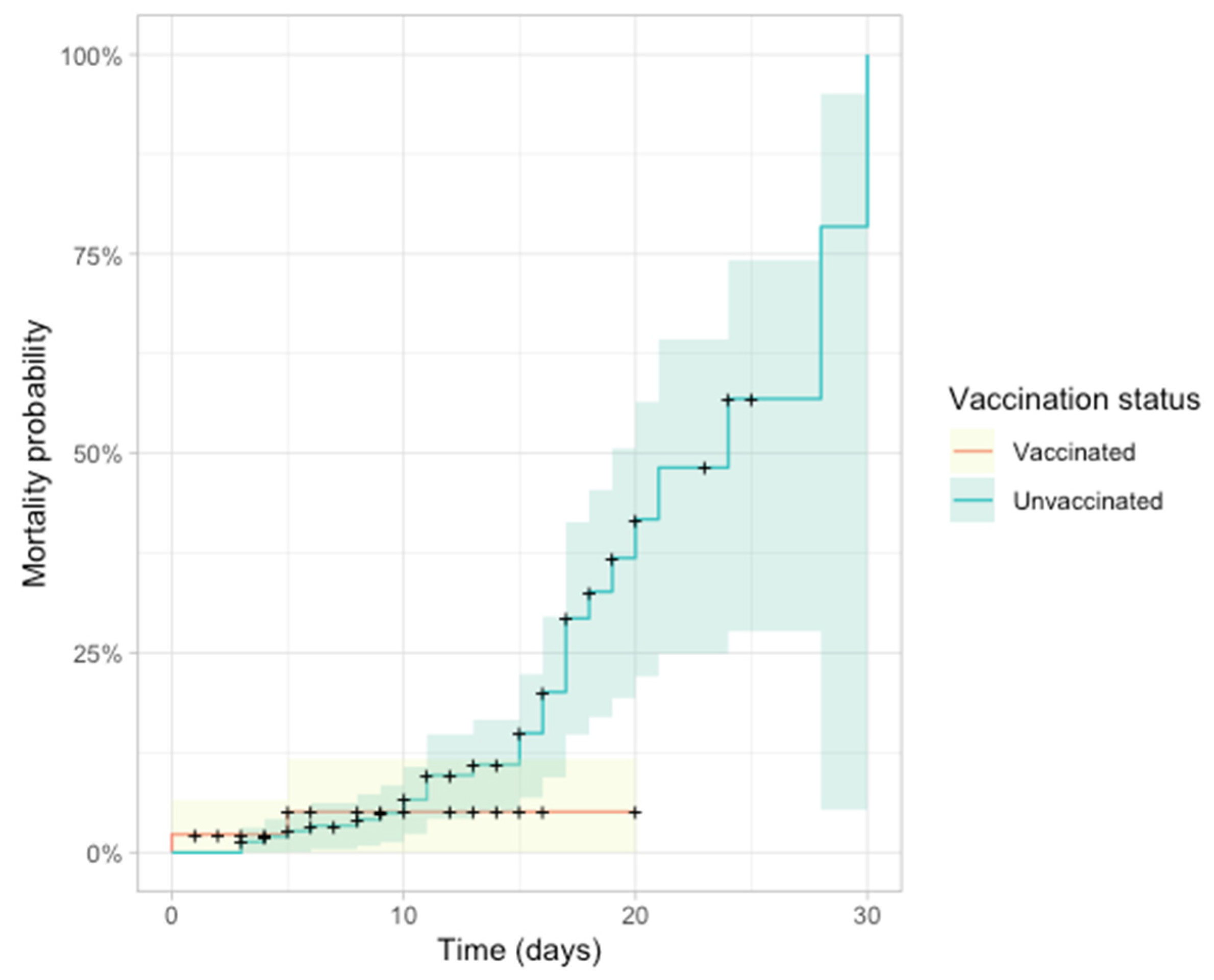
3.5. ICU Admission and Mortality
4. Discussion
4.1. Top of Form
4.2. Bottom of Form
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carabelli, A.M.; Peacock, T.P.; Thorne, L.G.; Harvey, W.T.; Hughes, J.; de Silva, T.I.; Peacock, S.J.; Barclay, W.S.; de Silva, T.I.; Towers, G.J.; et al. SARS-CoV-2 Variant Biology: Immune Escape, Transmission and Fitness. Nat. Rev. Microbiol. 2023, 21, 162–177. [Google Scholar] [CrossRef]
- Nesseler, N.; Fadel, G.; Mansour, A.; Para, M.; Falcoz, P.E.; Mongardon, N.; Porto, A.; Bertier, A.; Levy, B.; Cadoz, C.; et al. Extracorporeal Membrane Oxygenation for Respiratory Failure Related to COVID-19: A Nationwide Cohort Study. Anesthesiology 2022, 136, 732–748. [Google Scholar] [CrossRef] [PubMed]
- Bruxvoort, K.J.; Sy, L.S.; Qian, L.; Ackerson, B.K.; Luo, Y.; Lee, G.S.; Tian, Y.; Florea, A.; Aragones, M.; Tubert, J.E.; et al. Effectiveness of MRNA-1273 against Delta, Mu, and Other Emerging Variants of SARS-CoV-2: Test Negative Case-Control Study. BMJ 2021, 375, e068848. [Google Scholar] [CrossRef] [PubMed]
- Hitchings, M.D.T.; Ranzani, O.T.; Torres, M.S.S.; de Oliveira, S.B.; Almiron, M.; Said, R.; Borg, R.; Schulz, W.L.; de Oliveira, R.D.; da Silva, P.V.; et al. Effectiveness of CoronaVac among Healthcare Workers in the Setting of High SARS-CoV-2 Gamma Variant Transmission in Manaus, Brazil: A Test-Negative Case-Control Study. Lancet Reg. Health Am. 2021, 1, 100025. [Google Scholar] [CrossRef] [PubMed]
- Al Fayez, N.; Nassar, M.S.; Alshehri, A.A.; Alnefaie, M.K.; Almughem, F.A.; Alshehri, B.Y.; Alawad, A.O.; Tawfik, E.A. Recent Advancement in MRNA Vaccine Development and Applications. Pharmaceutics 2023, 15, 1972. [Google Scholar] [CrossRef] [PubMed]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Mascellino, M.T.; Di Timoteo, F.; De Angelis, M.; Oliva, A. Overview of the Main Anti-SARS-CoV-2 Vaccines: Mechanism of Action, Efficacy and Safety. Infect. Drug Resist. 2021, 14, 3459. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Vaccines: MODERNA|PFIZER/BIONTECH|ASTRAZENECA-YouTube. Available online: https://www.youtube.com/watch?v=35Idb_lCU4o (accessed on 11 March 2023).
- How Does Vaxzevria, the Oxford-AstraZeneca COVID-19 Vaccine Work?|COVID-19 Info Vaccines. Available online: https://www.covid19infovaccines.com/en-posts/how-does-vaxzevria-the-oxford-astrazeneca-covid-19-vaccine-work (accessed on 11 March 2023).
- Mitsi, E.; Diniz, M.O.; Reiné, J.; Collins, A.M.; Robinson, R.E.; Hyder-Wright, A.; Farrar, M.; Liatsikos, K.; Hamilton, J.; Onyema, O.; et al. Respiratory Mucosal Immune Memory to SARS-CoV-2 after Infection and Vaccination. Nat. Commun. 2023, 14, 6815. [Google Scholar] [CrossRef] [PubMed]
- Steenblock, C.; Schwarz, P.E.H.; Ludwig, B.; Linkermann, A.; Zimmet, P.; Kulebyakin, K.; Tkachuk, V.A.; Markov, A.G.; Lehnert, H.; de Angelis, M.H.; et al. COVID-19 and Metabolic Disease: Mechanisms and Clinical Management. Lancet. Diabetes Endocrinol. 2021, 9, 786. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Delta Variant: What Is Happening with Transmission, Hospital Admissions, and Restrictions? BMJ 2021, 373, n1513. [Google Scholar] [CrossRef]
- Alizon, S.; Haim-Boukobza, S.; Foulongne, V.; Verdurme, L.; Trombert-Paolantoni, S.; Lecorche, E.; Roquebert, B.; Sofonea, M.T. Rapid Spread of the SARS-CoV-2 Delta Variant in Some French Regions, June 2021. Eurosurveillance 2021, 26, 2100573. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.W.X.; Chiew, C.J.; Ang, L.W.; Mak, T.M.; Cui, L.; Toh, M.P.H.S.; Lim, Y.D.; Lee, P.H.; Lee, T.H.; Chia, P.Y.; et al. Clinical and Virological Features of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Variants of Concern: A Retrospective Cohort Study Comparing B.1.1.7 (Alpha), B.1.351 (Beta), and B.1.617.2 (Delta). Clin. Infect. Dis. 2022, 75, E1128–E1136. [Google Scholar] [CrossRef] [PubMed]
- Dissanayake, H. COVID-19 and Metabolic Syndrome. Best Pract. Res. Clin. Endocrinol. Metab. 2023, 37, 101753. [Google Scholar] [CrossRef] [PubMed]
- Rico-Martín, S.; Calderón-García, J.F.; Basilio-Fernández, B.; Clavijo-Chamorro, M.Z.; Muñoz-Torrero, J.F.S. Metabolic Syndrome and Its Components in Patients with COVID-19: Severe Acute Respiratory Syndrome (SARS) and Mortality. A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2021, 8, 162. [Google Scholar] [CrossRef]
- Zhao, W.; Zhong, Z.; Xie, X.; Yu, Q.; Liu, J. Relation between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.H.; Dong, J.H.; An, W.M.; Lv, X.Y.; Yin, X.P.; Zhang, J.Z.; Dong, L.; Ma, X.; Zhang, H.J.; Gao, B.L. Clinical and Computed Tomographic Imaging Features of Novel Coronavirus Pneumonia Caused by SARS-CoV-2. J. Infect. 2020, 80, 394–400. [Google Scholar] [CrossRef]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Der Nigoghossian, C.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef] [PubMed]
- ORDIN 2103 12/10/2021 Portal Legislativ. Available online: https://legislatie.just.ro/Public/DetaliiDocument/247389 (accessed on 25 March 2023).
- Samieefar, N.; Rashedi, R.; Akhlaghdoust, M.; Mashhadi, M.; Darzi, P.; Rezaei, N. Delta Variant: The New Challenge of COVID-19 Pandemic, an Overview of Epidemiological, Clinical, and Immune Characteristics. Acta Bio Medica Atenei Parm. 2022, 93, e2022179. [Google Scholar] [CrossRef]
- Wei, L.; Zhaoyin, L.; Yuxuan, Z.; Yumin, Z.; Elita, L.Y.; Masrur, A.; Yu, M. Spatiotemporal Patterns and Progression of the Delta Variant of COVID-19 and Their Health Intervention Linkages in Southeast Asia. medRxiv 2021. [Google Scholar] [CrossRef]
- Zhang, M.; He, Y.; Jie, Z. Delta Variant: Partially Sensitive to Vaccination, but Still Worth Global Attention. J. Transl. Intern. Med. 2022, 10, 227. [Google Scholar] [CrossRef]
- Torjesen, I. COVID-19: Delta Variant Is Now UK’s Most Dominant Strain and Spreading through Schools. BMJ 2021, 373, n1445. [Google Scholar] [CrossRef]
- Dyer, O. COVID-19: Unvaccinated Face 11 Times Risk of Death from Delta Variant, CDC Data Show. BMJ 2021, 374, n2282. [Google Scholar] [CrossRef]
- Balachandran, S.; Moni, M.; Sathyapalan, D.T.; Varghese, P.; Jose, M.P.; Murugan, M.R.; Rajan, C.; Saboo, D.; Nair, S.S.; Varkey, R.A.; et al. A Comparison of Clinical Outcomes between Vaccinated and Vaccine-Naive Patients of COVID-19, in Four Tertiary Care Hospitals of Kerala, South India. Clin. Epidemiol. Glob. Health 2022, 13, 100971. [Google Scholar] [CrossRef]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, Risk of Hospital Admission, and Vaccine Effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef] [PubMed]
- Nordström, P.; Ballin, M.; Nordström, A. Effectiveness of Heterologous ChAdOx1 NCoV-19 and MRNA Prime-Boost Vaccination against Symptomatic COVID-19 Infection in Sweden: A Nationwide Cohort Study. Lancet Reg. Health Eur. 2021, 11, 100249. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of Effectiveness of Vaccines against SARS-CoV-2 Infection and COVID-19 Disease: Results of a Systematic Review and Meta-Regression. Lancet 2022, 399, 924. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, E.S.; Dorabawila, V.; Easton, D.; Bauer, U.E.; Kumar, J.; Hoen, R.; Hoefer, D.; Wu, M.; Lutterloh, E.; Conroy, M.B.; et al. COVID-19 Vaccine Effectiveness in New York State. N. Engl. J. Med. 2022, 386, 116–127. [Google Scholar] [CrossRef]
- Dutta, S.; Kaur, R.J.; Bhardwaj, P.; Sharma, P.; Ambwani, S.; Islam, S.; Tandon, A.; Abhayanand, J.P.; Sukhija, S.; Venkatesh, S.S.; et al. Adverse Events Reported from the COVID-19 Vaccines: A Descriptive Study Based on the WHO Database (VigiBase®). J. Appl. Pharm. Sci. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Enciu, B.G.; Pițigoi, D.; Zaharia, A.; Popescu, R.; Niculcea, A.; Crăciun, M.D.; Pistol, A. COVID-19 Vaccination in Romania and the Benefits of the National Electronic Registry of Vaccinations. Vaccines 2023, 11, 370. [Google Scholar] [CrossRef]
- Dascalu, S.; Geambasu, O.; Covaciu, O.; Chereches, R.M.; Diaconu, G.; Dumitra, G.G.; Gheorghita, V.; Popovici, E.D. Prospects of COVID-19 Vaccination in Romania: Challenges and Potential Solutions. Front. Public Health 2021, 9, 644538. [Google Scholar] [CrossRef]
- Kumari, N.; Ahmad, M.S.; Gupta, A.; Prakash, G. Comparison of HRCT Chest Findings among Vaccinated and Non-Vaccinated COVID-19 Patients. Int. J. Res. Med. Sci. 2022, 10, 2911–2915. [Google Scholar] [CrossRef]
- Lee, J.E.; Hwang, M.; Kim, Y.H.; Chung, M.J.; Sim, B.H.; Chae, K.J.; Yoo, J.Y.; Jeong, Y.J. Imaging and Clinical Features of COVID-19 Breakthrough Infections: A Study. Radiology 2022, 303, 682. [Google Scholar] [CrossRef] [PubMed]
- Marietta, M.; Ageno, W.; Artoni, A.; De Candia, E.; Gresele, P.; Marchetti, M.; Marcucci, R.; Tripodi, A. COVID-19 and Haemostasis: A Position Paper from Italian Society on Thrombosis and Haemostasis (SISET). Blood Transfus. 2020, 18, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Korishettar, G.; Chikkahonnaiah, P.; Tulimilli, S.R.V.; Dallavalasa, S.; Byrappa, S.H.; Madhunapantula, S.R.V.; Veeranna, R.P. Assessment of Clinical Profile and Treatment Outcome in Vaccinated and Unvaccinated SARS-CoV-2 Infected Patients. Vaccines 2022, 10, 1125. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.; Yoon, S.K.; Meece, J.; Olsho, L.E.W.; Caban-Martinez, A.J.; Fowlkes, A.L.; Lutrick, K.; et al. Prevention and Attenuation of COVID-19 with the BNT162b2 and MRNA-1273 Vaccines. N. Engl. J. Med. 2021, 385, 320–329. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 MRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]










| Prediction Variable (Compared Variable) | Odds Ratio | CI: 2.5–97.5% | p-Value |
|---|---|---|---|
| Vaccination status (Unvaccinated) | 3.50 | 1.71–7.31 | <0.001 |
| Sex (Males) | 2.38 | 1.27–4.57 | <0.001 |
| Age | 1.04 | 1.02–1.06 | <0.001 |
| BMI | 1.16 | 1.08–1.24 | <0.001 |
| Smoking status (Smoking) | 0.97 | 0.47–2.02 | 0.93 |
| Smoking status (Ex-smoker) | 1.53 | 0.58–4.30 | 0.4 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Characteristic | Beta | 95%CI | p-Value | Beta | 95% CI | p-Value |
| Vaccination status | ||||||
| Vaccinated | reference | — | reference | — | ||
| Unvaccinated | 11 | 3.2, 20 | 0.006 | 11.5 | 3.6, 19 | 0.004 |
| Sex (Male/Female) | ||||||
| Female | reference | — | reference | — | ||
| Male | 5.5 | −1.4, 12 | 0.12 | 6.7 | −0.17, 14 | 0.056 |
| Age (years) | 0.15 | −0.08, 0.38 | 0.2 | 0.15 | −0.08, 0.38 | 0.2 |
| BMI | 1.7 | 1.1, 2.4 | <0.001 | 1.6 | 0.93, 2.3 | <0.001 |
| Smoking status | ||||||
| Not smoking | reference | — | reference | — | ||
| Smoker | 5.1 | −3.0, 13 | 0.2 | 1.5 | −6.5, 9.4 | 0.7 |
| Ex-smoker | 9.2 | −1.0, 20 | 0.077 | 4.7 | −5.4, 15 | 0.4 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Characteristic | Beta | 95% CI | p-Value | Beta | 95% CI | p-Value |
| Vaccination status | ||||||
| Vaccinated | Reference | Reference | — | |||
| Unvaccinated | 0.55 | −0.14, 1.2 | 0.12 | 0.27 | −0.35, 0.90 | 0.4 |
| Sex | ||||||
| Female | Reference | Reference | — | |||
| Male | −0.03 | −0.60, 0.54 | >0.9 | 0.23 | −0.29, 0.75 | 0.4 |
| Age (years) | 0.05 | 0.04, 0.07 | <0.001 | 0.05 | 0.04, 0.07 | <0.001 |
| BMI | 0.12 | 0.06, 0.17 | <0.001 | 0.11 | 0.06, 0.17 | <0.001 |
| Characteristic | Vaccinated, n= 44 1 | Unvaccinated, n = 153 1 | p-Value 2 |
|---|---|---|---|
| Need for oxygen support on admission time | 0.003 | ||
| Ambiental air | 17 (39%) | 21 (14%) | |
| Nasal canula | 13 (30%) | 77 (50%) | |
| Reservoir mask | 13 (30%) | 40 (26%) | |
| Simple facial mask | 1 (2.3%) | 12 (7.8%) | |
| Venturi mask | 0 (0%) | 3 (2.0%) | |
| Need for oxygen support: worst | 0.047 | ||
| Ambiental air | 16 (36%) | 21 (14%) | |
| Nasal canula | 9 (20%) | 47 (31%) | |
| High Flow Nasal Cannula | 0 (0%) | 9 (6%) | |
| Reservoir mask | 14 (32%) | 59 (39%) | |
| Simple facial mask | 4 (9.1%) | 11 (7.2%) | |
| Non-invasive ventilation | 0 (0%) | 1 (0.7%) | |
| Venturi mask | 1 (2.3%) | 4 (2.6%) | |
| Need for oxygen support on discharge | 0.3 | ||
| Ambiental air | 23 (52%) | 58 (38%) | |
| Nasal canula | 11 (25%) | 44 (29.7%) | |
| High Flow Nasal Cannula | 0 (0%) | 13 (8.5%) | |
| Reservoir mask | 10 (23%) | 27 (18%) | |
| Simple facial mask | 0 (0%) | 8 (5.2%) | |
| Non-invasive ventilation | 0 (0%) | 1 (0.7%) | |
| Venturi mask | 0 (0%) | 1 (0.7%) |
| Characteristic | Vaccinated, n = 44 1 | Unvaccinated, n = 153 1 | p-Value 2 |
|---|---|---|---|
| ICU transfer | 0.07 | ||
| Yes | 2 (4.7%) | 23 (15%) | |
| No | 41 (95%) | 129 (85%) | |
| Death | 0.030 | ||
| Yes | 2 (4.5%) | 27 (18%) | |
| No | 42 (95%) | 125 (82%) |
| Characteristic | Mild, n = 30 1 | Moderate, n = 58 1 | Severe, n = 109 1 | p-Value 2 |
|---|---|---|---|---|
| ICU transfer | <0.001 | |||
| Yes | 1 (3.3%) | 1 (1.7%) | 23 (21%) | |
| No | 29 (97%) | 57 (98%) | 84 (79%) | |
| Death | <0.001 | |||
| Yes | 0 (0%) | 0 (0%) | 29 (27%) | |
| No | 30 (100%) | 58 (100%) | 79 (73%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vulturar, D.-M.; Moacă, L.-Ș.; Neag, M.A.; Mitre, A.-O.; Alexescu, T.-G.; Gherman, D.; Făgărășan, I.; Chețan, I.M.; Gherman, C.D.; Melinte, O.-E.; et al. Delta Variant in the COVID-19 Pandemic: A Comparative Study on Clinical Outcomes Based on Vaccination Status. J. Pers. Med. 2024, 14, 358. https://doi.org/10.3390/jpm14040358
Vulturar D-M, Moacă L-Ș, Neag MA, Mitre A-O, Alexescu T-G, Gherman D, Făgărășan I, Chețan IM, Gherman CD, Melinte O-E, et al. Delta Variant in the COVID-19 Pandemic: A Comparative Study on Clinical Outcomes Based on Vaccination Status. Journal of Personalized Medicine. 2024; 14(4):358. https://doi.org/10.3390/jpm14040358
Chicago/Turabian StyleVulturar, Damiana-Maria, Liviu-Ștefan Moacă, Maria Adriana Neag, Andrei-Otto Mitre, Teodora-Gabriela Alexescu, Diana Gherman, Iulia Făgărășan, Ioana Maria Chețan, Claudia Diana Gherman, Oana-Elena Melinte, and et al. 2024. "Delta Variant in the COVID-19 Pandemic: A Comparative Study on Clinical Outcomes Based on Vaccination Status" Journal of Personalized Medicine 14, no. 4: 358. https://doi.org/10.3390/jpm14040358
APA StyleVulturar, D. -M., Moacă, L. -Ș., Neag, M. A., Mitre, A. -O., Alexescu, T. -G., Gherman, D., Făgărășan, I., Chețan, I. M., Gherman, C. D., Melinte, O. -E., Trofor, A. C., & Todea, D. -A. (2024). Delta Variant in the COVID-19 Pandemic: A Comparative Study on Clinical Outcomes Based on Vaccination Status. Journal of Personalized Medicine, 14(4), 358. https://doi.org/10.3390/jpm14040358