

Muscle Asymmetries in the Lower Limbs of Male Soccer Players: Preliminary Findings on the Association between Countermovement Jump and Tensiomyography
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anamnestic Questionnaire and Anthropometrics
2.2. Jump Performance, Inter-Limb Asymmetry, and BLD Assessment
2.3. Tensiomyography
2.4. Statistical Analyses
3. Results
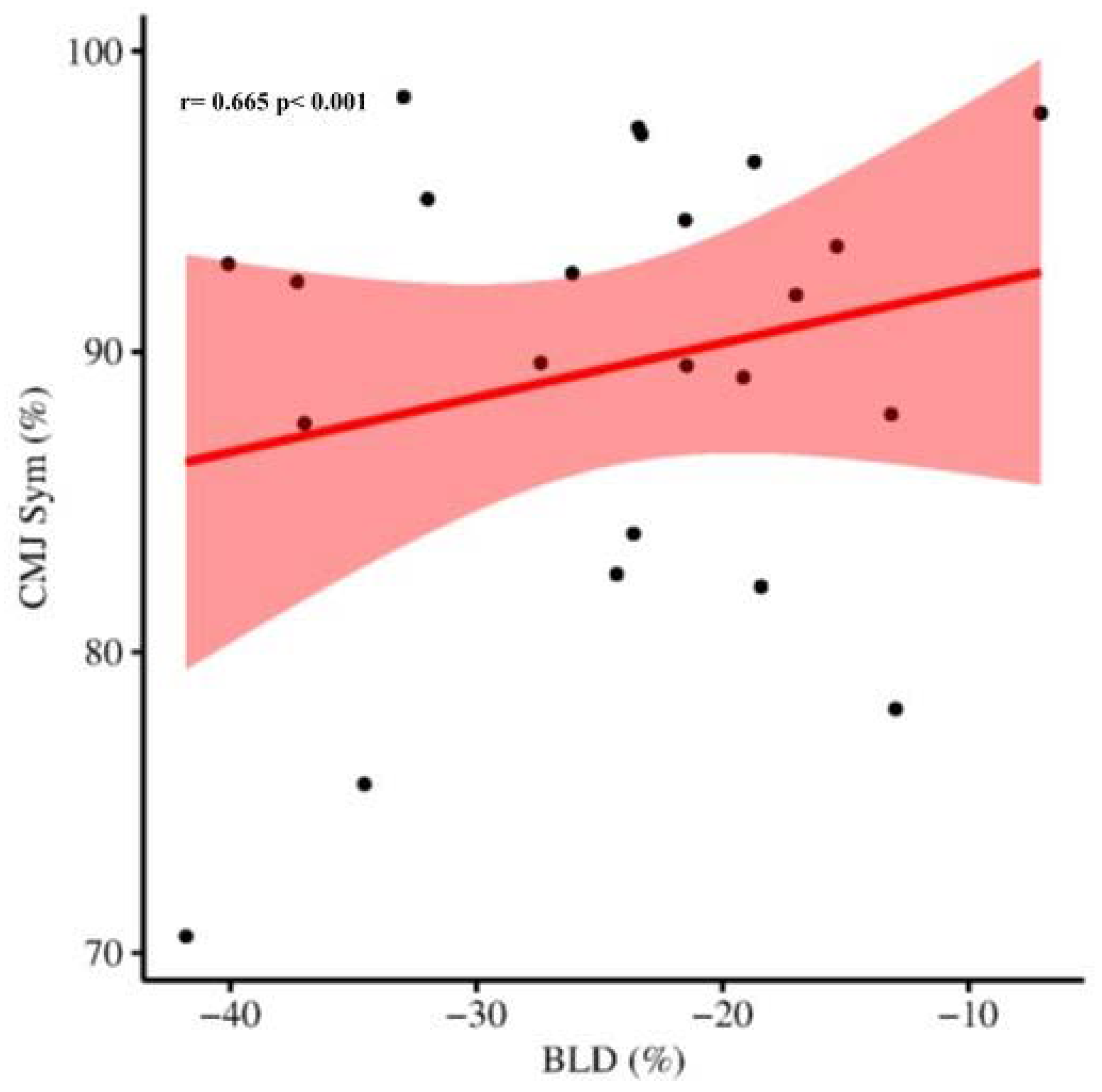
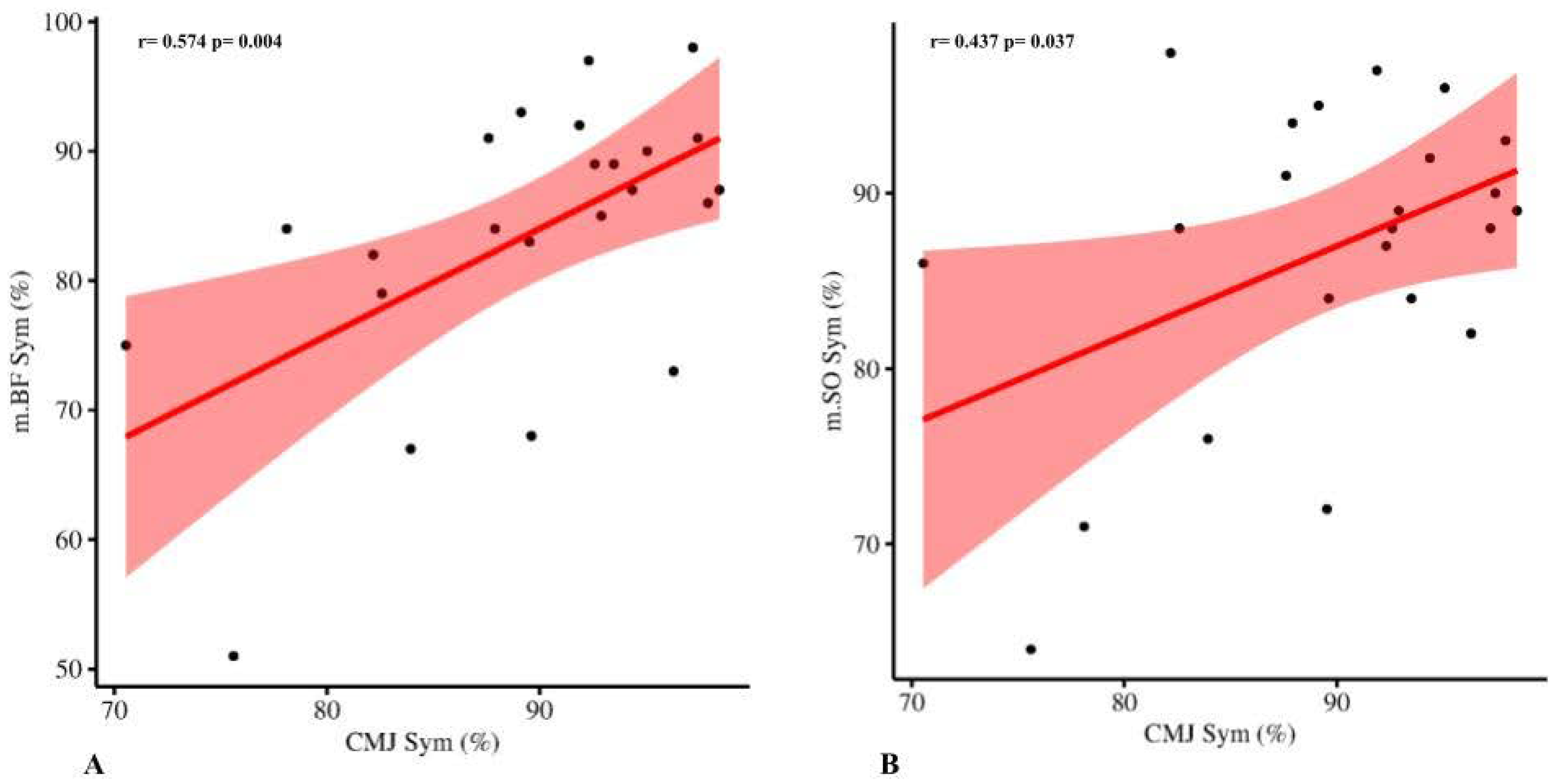
3.1. CMJ Asymmetry, Bilateral Deficit, and TMG
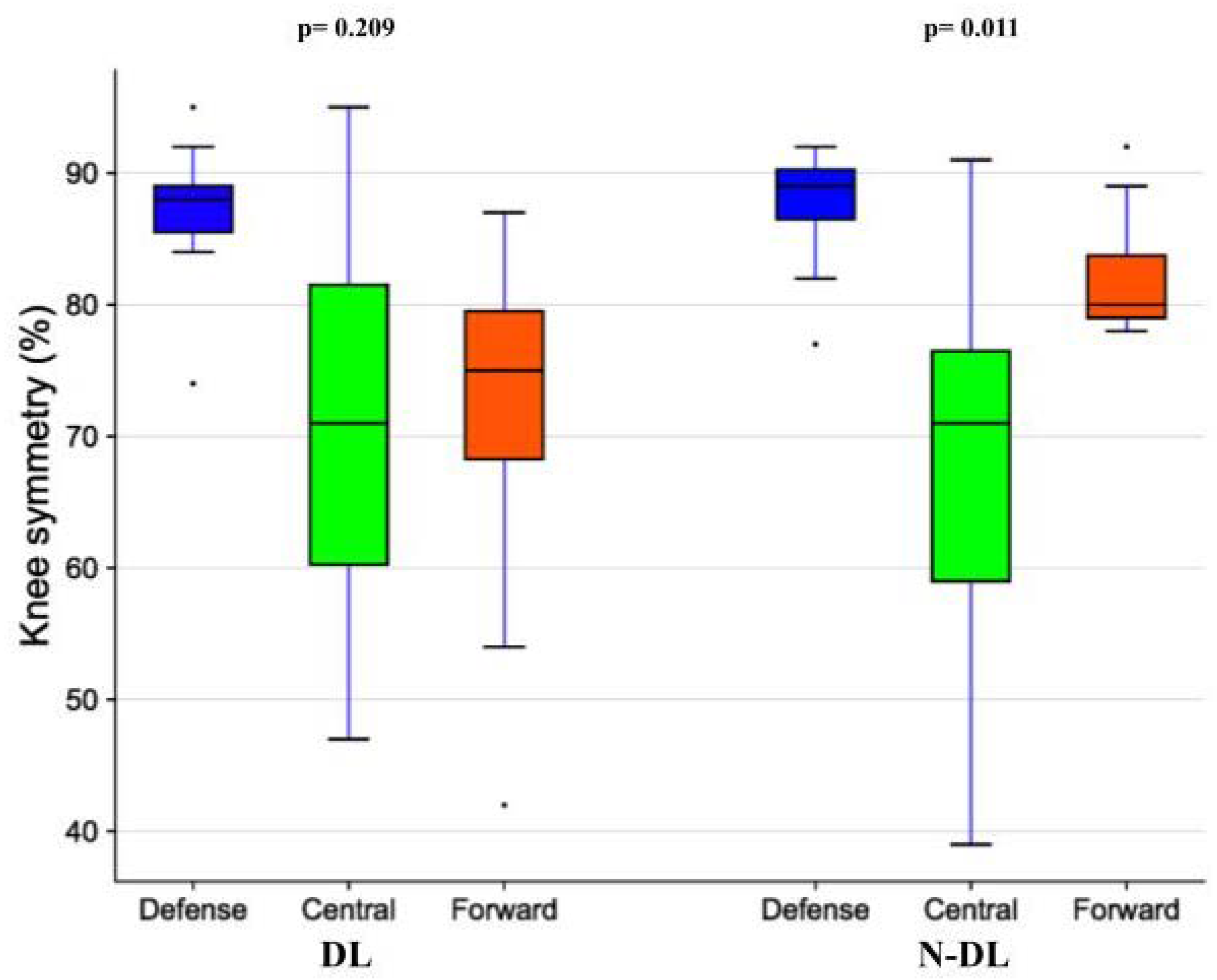
3.2. Playing Position
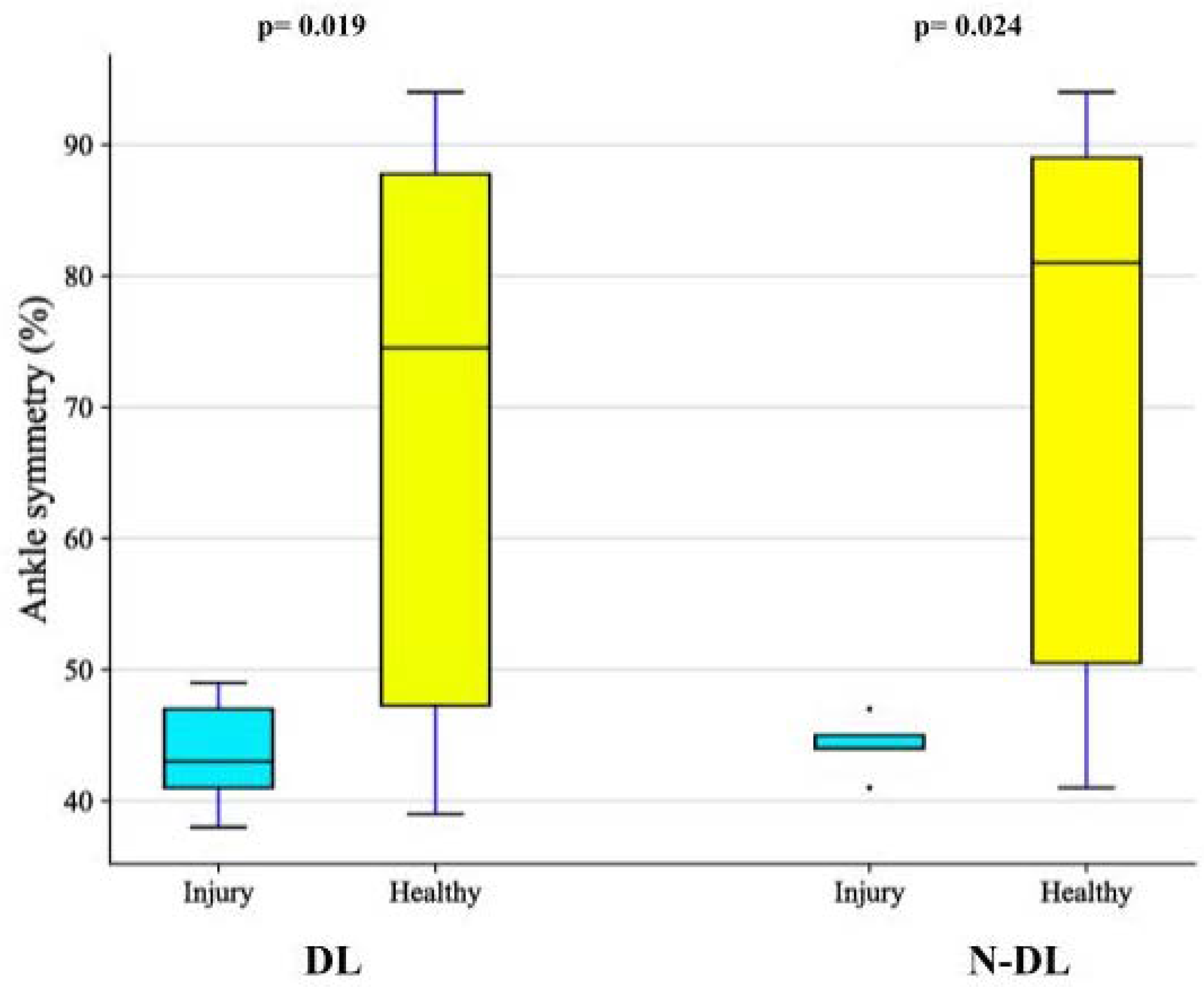
3.3. History of Injuries
4. Discussion
Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bishop, C.; Turner, A.; Read, P. Effects of Inter-Limb Asymmetries on Physical and Sports Performance: A Systematic Review. J. Sports Sci. 2018, 36, 1135–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castagna, C.; Castellini, E. Vertical Jump Performance in Italian Male and Female National Team Soccer Players. J. Strength Cond. Res. 2013, 27, 1156–1161. [Google Scholar] [CrossRef]
- Jakobi, J.M.; Chilibeck, P.D. Bilateral and Unilateral Contractions: Possible Differences in Maximal Voluntary Force. Can. J. Appl. Physiol. 2001, 26, 12–33. [Google Scholar] [CrossRef] [PubMed]
- Škarabot, J.; Cronin, N.; Strojnik, V.; Avela, J. Bilateral Deficit in Maximal Force Production. Eur. J. Appl. Physiol. 2016, 116, 2057–2084. [Google Scholar] [CrossRef]
- Dickin, D.C.; Too, D. Effects of Movement Velocity and Maximal Concentric and Eccentric Actions on the Bilateral Deficit. Res. Q. Exerc. Sport 2006, 77, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Botton, C.E.; Radaelli, R.; Wilhelm, E.N.; Rech, A.; Brown, L.E.; Pinto, R.S. Neuromuscular Adaptations to Unilateral vs. Bilateral Strength Training in Women. J. Strength Cond. Res. 2016, 30, 1924–1932. [Google Scholar] [CrossRef]
- Ascenzi, G.; Ruscello, B.; Filetti, C.; Bonanno, D.; Di Salvo, V.; Nuñez, F.J.; Mendez-Villanueva, A.; Suarez-Arrones, L. Bilateral Deficit and Bilateral Performance: Relationship with Sprinting and Change of Direction in Elite Youth Soccer Players. Sports 2020, 8, 82. [Google Scholar] [CrossRef]
- Bishop, C.; Berney, J.; Lake, J.; Loturco, I.; Blagrove, R.; Turner, A.; Read, P. Bilateral Deficit during Jumping Tasks: Relationship with Speed and Change of Direction Speed Performance. J. Strength Cond. Res. 2021, 35, 1833–1840. [Google Scholar] [CrossRef]
- Heishman, A.; Daub, B.; Miller, R.; Brown, B.; Freitas, E.; Bemben, M. Countermovement Jump Inter-Limb Asymmetries in Collegiate Basketball Players. Sports 2019, 7, 103. [Google Scholar] [CrossRef] [Green Version]
- Pain, M.T.G. Considerations for Single and Double Leg Drop Jumps: Bilateral Deficit, Standardizing Drop Height, and Equalizing Training Load. J. Appl. Biomech. 2014, 30, 722–727. [Google Scholar] [CrossRef]
- Pérez-Castilla, A.; García-Ramos, A.; Janicijevic, D.; Delgado-García, G.; de la Cruz, J.C.; Rojas, F.J.; Cepero, M. Between-Session Reliability of Performance and Asymmetry Variables Obtained during Unilateral and Bilateral Countermovement Jumps in Basketball Players. PLoS ONE 2021, 16, e0255458. [Google Scholar] [CrossRef] [PubMed]
- Pleša, J.; Kozinc, Ž.; Šarabon, N. Bilateral Deficit in Countermovement Jump and Its Influence on Linear Sprinting, Jumping, and Change of Direction Ability in Volleyball Players. Front. Physiol. 2022, 13, 768906. [Google Scholar] [CrossRef]
- Bobbert, M.F.; De Graaf, W.W.; Jonk, J.N.; Casius, L.J.R. Explanation of the Bilateral Deficit in Human Vertical Squat Jumping. J. Appl. Physiol. 2006, 100, 493–499. [Google Scholar] [CrossRef]
- Burger, H.; Valenčič, V.; Marinček, Č.; Kogovšek, N. Properties of Musculus Gluteus Maximus in Above-Knee Amputees. Clin. Biomech. 1996, 11, 35–38. [Google Scholar] [CrossRef]
- García-García, O.; Cuba-Dorado, A.; Álvarez-Yates, T.; Carballo-López, J.; Iglesias-Caamaño, M. Clinical Utility of Tensiomyography for Muscle Function Analysis in Athletes. Open Access J. Sport. Med. 2019, 10, 49–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenčič, V.; Knez, N. Measuring of Skeletal Muscles’ Dynamic Properties. Artif. Organs 1997, 21, 240–242. [Google Scholar] [CrossRef]
- Paravlic, A.H.; Milanović, Z.; Abazović, E.; Vučković, G.; Spudić, D.; Majcen Rošker, Z.; Pajek, M.; Vodičar, J. The Muscle Contractile Properties in Female Soccer Players: Inter-Limb Comparison Using Tensiomyography. J. Musculoskelet. Neuronal Interact. 2022, 22, 179–192. [Google Scholar]
- Simunič, B.; Degens, H.; Rittweger, J.; Narici, M.; Mekjavić, I.B.; Pišot, R. Noninvasive Estimation of Myosin Heavy Chain Composition in Human Skeletal Muscle. Med. Sci. Sports Exerc. 2011, 43, 1619–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Manso, J.M.; Rodríguez-Ruiz, D.; Rodríguez-Matoso, D.; de Yves, S.; Sarmiento, S.; Quiroga, M. Assessment of Muscle Fatigue after an Ultra-Endurance Triathlon Using Tensiomyography (TMG). J. Sports Sci. 2011, 29, 619–625. [Google Scholar] [CrossRef]
- Hunter, A.M.; Galloway, S.D.R.; Smith, I.J.; Tallent, J.; Ditroilo, M.; Fairweather, M.M.; Howatson, G. Assessment of Eccentric Exercise-Induced Muscle Damage of the Elbow Flexors by Tensiomyography. J. Electromyogr. Kinesiol. 2012, 22, 334–341. [Google Scholar] [CrossRef]
- Zubac, D.; Paravlić, A.; Koren, K.; Felicita, U.; Šimunič, B. Plyometric Exercise Improves Jumping Performance and Skeletal Muscle Contractile Properties in Seniors. J. Musculoskelet. Neuronal Interact. 2019, 19, 38–49. [Google Scholar] [PubMed]
- Paravlic, A.H.; Pisot, R.; Simunic, B. Muscle-Specific Changes of Lower Extremities in the Early Period after Total Knee Arthroplasty: Insight from Tensiomyography. J. Musculoskelet. Neuronal Interact. 2020, 20, 390–397. [Google Scholar] [PubMed]
- Zubac, D.; Šimunič, B. Skeletal Muscle Contraction Time and Tone Decrease after 8 Weeks of Plyometric Training. J. Strength Cond. Res. 2017, 31, 1610–1619. [Google Scholar] [CrossRef] [PubMed]
- Seijas, R.; Marín, M.; Rivera, E.; Alentorn-Geli, E.; Barastegui, D.; Álvarez-Díaz, P.; Cugat, R. Gluteus Maximus Contraction Velocity Assessed by Tensiomyography Improves Following Arthroscopic Treatment of Femoroacetabular Impingement. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Diaz, P.; Alentorn-Geli, E.; Ramon, S.; Marin, M.; Steinbacher, G.; Rius, M.; Seijas, R.; Ballester, J.; Cugat, R. Comparison of Tensiomyographic Neuromuscular Characteristics between Muscles of the Dominant and Non-Dominant Lower Extremity in Male Soccer Players. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 2259–2263. [Google Scholar] [CrossRef]
- Alvarez-Diaz, P.; Alentorn-Geli, E.; Ramon, S.; Marin, M.; Steinbacher, G.; Boffa, J.J.; Cuscó, X.; Ares, O.; Ballester, J.; Cugat, R. Effects of Anterior Cruciate Ligament Injury on Neuromuscular Tensiomyographic Characteristics of the Lower Extremity in Competitive Male Soccer Players. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 2264–2270. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Alvarez-Diaz, P.; Ramon, S.; Marin, M.; Steinbacher, G.; Rius, M.; Seijas, R.; Ares, O.; Cugat, R. Assessment of Gastrocnemius Tensiomyographic Neuromuscular Characteristics as Risk Factors for Anterior Cruciate Ligament Injury in Male Soccer Players. Knee Surg. Sport. Traumatol. Arthrosc. 2015, 23, 2502–2507. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Alvarez-Diaz, P.; Ramon, S.; Marin, M.; Steinbacher, G.; Boffa, J.J.; Cuscó, X.; Ballester, J.; Cugat, R. Assessment of Neuromuscular Risk Factors for Anterior Cruciate Ligament Injury through Tensiomyography in Male Soccer Players. Knee Surg. Sport. Traumatol. Arthrosc. 2015, 23, 2508–2513. [Google Scholar] [CrossRef]
- Loturco, I.; Pereira, L.A.; Kobal, R.; Abad, C.C.C.; Komatsu, W.; Cunha, R.; Arliani, G.; Ejnisman, B.; Pochini, A.D.C.; Nakamura, F.Y.; et al. Functional Screening Tests: Interrelationships and Ability to Predict Vertical Jump Performance. Int. J. Sports Med. 2018, 39, 189–197. [Google Scholar] [CrossRef]
- Gil, S.; Loturco, I.; Tricoli, V.; Ugrinowitsch, C.; Kobal, R.; Cal Abad, C.C.; Roschel, H. Tensiomyography Parameters and Jumping and Sprinting Performance in Brazilian Elite Soccer Players. Sport. Biomech. 2015, 14, 340–350. [Google Scholar] [CrossRef]
- Lewis, M.D.; Young, W.B.; Knapstein, L.; Lavender, A.; Talpey, S.W. Countermovement Jump Variables Not Tensiomyography Can Distinguish between Sprint and Endurance Focused Track Cyclists. Biol. Sport 2022, 39, 67–72. [Google Scholar] [CrossRef]
- García-García, O.; Serrano-Gómez, V.; Hernández-Mendo, A.; Morales-Sánchez, V. Baseline Mechanical and Neuromuscular Profile of Knee Extensor and Flexor Muscles in Professional Soccer Players at the Start of the Pre-Season. J. Hum. Kinet. 2017, 58, 23–34. [Google Scholar] [CrossRef] [Green Version]
- López-Fernández, J.; García-Unanue, J.; Sánchez-Sánchez, J.; Colino, E.; Hernando, E.; Gallardo, L. Bilateral Asymmetries Assessment in Elite and Sub-Elite Male Futsal Players. Int. J. Environ. Res. Public Health 2020, 17, 3169. [Google Scholar] [CrossRef]
- Kuruganti, U.; Murphy, T.; Pardy, T. Bilateral Deficit Phenomenon and the Role of Antagonist Muscle Activity during Maximal Isometric Knee Extensions in Young, Athletic Men. Eur. J. Appl. Physiol. 2011, 111, 1533–1539. [Google Scholar] [CrossRef]
- Rouissi, M.; Chtara, M.; Owen, A.; Chaalali, A.; Chaouachi, A.; Gabbett, T.; Chamari, K. Effect of Leg Dominance on Change of Direction Ability amongst Young Elite Soccer Players. J. Sports Sci. 2016, 34, 542–548. [Google Scholar] [CrossRef]
- Howard, J.D.; Enoka, R.M. Maximum Bilateral Contractions Are Modified by Neurally Mediated Interlimb Effects. J. Appl. Physiol. 1991, 70, 306–316. [Google Scholar] [CrossRef]
- Macgregor, L.J.; Hunter, A.M.; Orizio, C.; Fairweather, M.M.; Ditroilo, M. Assessment of Skeletal Muscle Contractile Properties by Radial Displacement: The Case for Tensiomyography. Sport. Med. 2018, 48, 1607–1620. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sport. Med. 2000, 30, 375–378. [Google Scholar] [CrossRef]
- Markovic, G.; Šarabon, N.; Pausic, J.; Hadžić, V. Adductor Muscles Strength and Strength Asymmetry as Risk Factors for Groin Injuries among Professional Soccer Players: A Prospective Study. Int. J. Environ. Res. Public Health 2020, 17, 4946. [Google Scholar] [CrossRef]
- Lohr, C.; Braumann, K.M.; Reer, R.; Schroeder, J.; Schmidt, T. Reliability of Tensiomyography and Myotonometry in Detecting Mechanical and Contractile Characteristics of the Lumbar Erector Spinae in Healthy Volunteers. Eur. J. Appl. Physiol. 2018, 118, 1349–1359. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillside, NJ, USA, 1988. [Google Scholar]
- Nuzzo, J.L.; Mcbride, J.M.; Cormie, P.; Mccaulley, G.O. Relationship between Countermovement Jump Performance and Multijoint Isometric and Dynamic Tests of Strength. J. Strength Cond. Res. 2008, 22, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.T.; Ryan, A.M.F.; Vallance, S.R.; Dias-Dougan, A.; Dugdale, J.H.; Hunter, A.M.; Hamilton, D.L.; Macgregor, L.J. Tensiomyography Derived Parameters Reflect Skeletal Muscle Architectural Adaptations Following 6-Weeks of Lower Body Resistance Training. Front. Physiol. 2019, 10, 1493. [Google Scholar] [CrossRef] [PubMed]
- Fukashiro, S.; Besier, T.F.; Barrett, R.; Cochrane, J.; Nagano, A.; Lloyd, D.G. Direction Control in Standing Horizontal and Vertical Jumps. Int. J. Sport Health Sci. 2005, 3, 272–279. [Google Scholar] [CrossRef] [Green Version]
- Falch, H.N.; Rædergård, H.G.; Van Den Tillaar, R. Relationship of Performance Measures and Muscle Activity between a 180° Change of Direction Task and Different Countermovement Jumps. Sports 2020, 8, 47. [Google Scholar] [CrossRef]
- Kipp, K.; Kim, H. Relative Contributions and Capacities of Lower Extremity Muscles to Accelerate the Body’s Center of Mass during Countermovement Jumps. Comput. Methods Biomech. Biomed. Engin. 2020, 23, 914–921. [Google Scholar] [CrossRef]
- Šimunič, B.; Koren, K.; Rittweger, J.; Lazzer, S.; Reggiani, C.; Rejc, E.; Pišot, R.; Narici, M.; Degens, H. Tensiomyography Detects Early Hallmarks of Bed-Rest-Induced Atrophy before Changes in Muscle Architecture. J. Appl. Physiol. 2019, 126, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Magnus, C.R.A.; Farthing, J.P. Greater Bilateral Deficit in Leg Press than in Handgrip Exercise Might Be Linked to Differences in Postural Stability Requirements. Appl. Physiol. Nutr. Metab. 2008, 33, 1132–1139. [Google Scholar] [CrossRef]
- Vandervoort, A.A.; Sale, D.G.; Moroz, J. Comparison of Motor Unit Activation during Unilateral and Bilateral Leg Extension. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1984, 56, 46–51. [Google Scholar] [CrossRef]
- Rejc, E.; Lazzer, S.; Antonutto, G.; Isola, M.; Di Prampero, P.E. Bilateral Deficit and EMG Activity during Explosive Lower Limb Contractions against Different Overloads. Eur. J. Appl. Physiol. 2010, 108, 157. [Google Scholar] [CrossRef]
- Della Villa, F.; Mandelbaum, B.R.; Lemak, L.J. The Effect of Playing Position on Injury Risk in Male Soccer Players: Systematic Review of the Literature and Risk Considerations for Each Playing Position. Am. J. Orthop. 2018, 47. [Google Scholar] [CrossRef]
- Haugen, T.A.; Tønnessen, E.; Seiler, S. Anaerobic Performance Testing of Professional Soccer Players 1995–2010. Int. J. Sports Physiol. Perform. 2013, 8, 148–156. [Google Scholar] [CrossRef]
- Bona, C.C.; Filho, H.T.; Izquierdo, M.; Ferraz, R.M.P.; Marques, M.C. Peak Torque and Muscle Balance in the Knees of Young U-15 and U-17 Soccer Athletes Playing Various Tactical Positions. J. Sports Med. Phys. Fitness 2017, 57, 923–929. [Google Scholar] [CrossRef]
- Romero-Moraleda, B.; Nedergaard, N.J.; Morencos, E.; Casamichana, D.; Ramirez-Campillo, R.; Vanrenterghem, J. External and Internal Loads during the Competitive Season in Professional Female Soccer Players According to Their Playing Position: Differences between Training and Competition. Res. Sport. Med. 2021, 29, 449–461. [Google Scholar] [CrossRef] [PubMed]
- Granero-Gil, P.; Gómez-Carmona, C.D.; Bastida-Castillo, A.; Rojas-Valverde, D.; De La Cruz, E.; Pino-Ortega, J. Influence of Playing Position and Laterality in Centripetal Force and Changes of Direction in Elite Soccer Players. PLoS ONE 2020, 15, e0232123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leventer, L.; Eek, F.; Hofstetter, S.; Lames, M. Injury Patterns among Elite Football Players: A Media-Based Analysis over 6 Seasons with Emphasis on Playing Position. Int. J. Sports Med. 2016, 37, 898–908. [Google Scholar] [CrossRef] [PubMed]
- McCall, A.; Carling, C.; Davison, M.; Nedelec, M.; Le Gall, F.; Berthoin, S.; Dupont, G. Injury Risk Factors, Screening Tests and Preventative Strategies: A Systematic Review of the Evidence That Underpins the Perceptions and Practices of 44 Football (Soccer) Teams from Various Premier Leagues. Br. J. Sports Med. 2015, 49, 583–589. [Google Scholar] [CrossRef]
- Owoeye, O.B.A.; VanderWey, M.J.; Pike, I. Reducing Injuries in Soccer (Football): An Umbrella Review of Best Evidence across the Epidemiological Framework for Prevention. Sports Med.-Open 2020, 6, 46. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of Muscle Injuries in Professional Football (Soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [Green Version]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Risk Factors for Lower Extremity Muscle Injury in Professional Soccer: The UEFA Injury Study. Am. J. Sports Med. 2013, 41, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Budtz-Jørgensen, E.; Hölmich, P. Preventive Effect of Eccentric Training on Acute Hamstring Injuries in Men’s Soccer: A Cluster-Randomized Controlled Trial. Am. J. Sports Med. 2011, 39, 2296–2303. [Google Scholar] [CrossRef]
- Biz, C.; Nicoletti, P.; Baldin, G.; Bragazzi, N.L.; Crimì, A.; Ruggieri, P. Hamstring Strain Injury (Hsi) Prevention in Professional and Semi-Professional Football Teams: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8272. [Google Scholar] [CrossRef] [PubMed]
- Green, B.; Pizzari, T. Calf Muscle Strain Injuries in Sport: A Systematic Review of Risk Factors for Injury. Br. J. Sports Med. 2017, 51, 1189–1194. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants (n = 23) | |
|---|---|
| Demographics | |
| Age, y | 18 ± 4 |
| Body mass, kg | 70.3 ± 5.4 |
| Body height, m | 1.80 ± 4.9 |
| BMI, kg/m2 | 21.69 ± 1.44 |
| Training history and characteristics | |
| Years of training in soccer, years | 13 ± 5 |
| Training frequency, training/week | 3 ± 0.3 |
| Training volume, min/week | 318 ± 57 |
| Strength & Conditioning, n (%) | 20 (87.0) |
| Playing position, n (%) | |
| Goalkeeper | 1 (4.3) |
| Defense | 7 (30.4) |
| Center | 8 (34.8) |
| Forward | 7 (30.4) |
| Health and injuries | |
| Quadriceps, n (%) | |
| Right | 1 (4.3) |
| Left | 1 (4.3) |
| Hamstrings, n (%) | |
| Right | 4 (17.4) |
| Left | 1 (4.3) |
| Knee, n (%) | |
| Right | 1 (4.3) |
| Left | 2 (8.7) |
| Leg, n (%) | |
| Right | 1 (4.3) |
| Left | 2 (8.7) |
| Ankle, n (%) | |
| Right | 5 (21.7) |
| Left | 5 (21.7) |
| Participants (n = 23) | |
|---|---|
| CMJ | |
| Peak Power, W | |
| Bilateral | 3870.7 ± 661.3 |
| DL | 2576.1 ± 485.4 |
| N-DL | 2602.3 ± 487.2 |
| Inter-limb symmetry, % | 89.4 ± 7.5 |
| BLD, % | 24.7 ± 9.4 |
| Peak Height, cm | |
| Bilateral | 45.4 ± 8.2 |
| DL | 34.0 ± 4.8 |
| N-DL | 35.1 ± 5.6 |
| Inter-limb symmetry, % | 91.9 ± 8.2 |
| BLD, % | 34.0 ± 10.6 |
| TMG | |
| Lateral symmetry | |
| m.AL, % | 67.3 ± 18.9 |
| m.BF, % | 83.5 ± 10.8 |
| m.GL, % | 87.4 ± 9.6 |
| m.GM, % | 89.0 ± 5.9 |
| m.GT, % | 85.6 ± 11.2 |
| m.RF, % | 87.0 ± 6.7 |
| m.SO, % | 86.7 ± 8.8 |
| m.TA, % | 77.1 ± 19.4 |
| m.VL, % | 88.7 ± 6.4 |
| m.VM, % | 88.3 ± 6.6 |
| Functional symmetry | |
| Achilles tendon, % | |
| DL | 87.4 ± 1.0 |
| N-DL | 85.1 ± 9.0 |
| Ligament patellae, % | |
| DL | 84.3 ± 6.7 |
| N-DL | 84.2 ± 8.5 |
| Knee, % | |
| DL | 74.7 ± 15.7 |
| N-DL | 77.9 ± 13.6 |
| Ankle, % | |
| DL | 63.3 ± 20.9 |
| N-DL | 66.5 ± 21.3 |
| Leg, % | |
| DL | 86.7 ± 7.1 |
| N-DL | 87.1 ± 7.5 |
| Defense | Central | Forward | |
|---|---|---|---|
| (n = 7) | (n = 8) | (n = 7) | |
| CMJ | |||
| Peak Power, W | |||
| Bilateral | 3902.3 ± 436.6 | 3631.5 ± 800.4 | 4043.0 ± 717.1 |
| DL | 2786.9 ± 556.1 | 2276.5 ± 431.8 | 2719.9 ± 374.5 |
| N-DL | 3033.1 ± 399.5 | 2377.4 ± 466.8 | 2421.3 ± 365.7 |
| Inter-limb symmetry, % | 87.5 ± 9.9 | 90.8 ± 5.5 | 89.2 ± 8.1 |
| BLD, % | 32.0 ± 9.8 | 22.4 ± 7.1 | 21.5 ± 8.4 |
| Peak Height, cm | |||
| Bilateral | 44.9 ± 8.4 | 42.5 ± 7.3 | 50.3 ± 8.1 |
| DL | 36.6 ± 5.5 | 31.3 ± 4.6 | 35.1 ± 2.8 |
| N-DL | 38.6 ± 6.5 | 33.0 ± 4.5 | 35.0 ± 5.0 |
| Inter-limb symmetry, % | 89.5 ± 11.5 | 93.4 ± 7.8 | 92.3 ± 5.8 |
| BLD, % | 39.5 ± 13.4 | 33.8 ± 7.3 | 28.3 ± 9.4 |
| TMG | |||
| Lateral symmetry | |||
| m.AL, % | 64.3 ± 18.9 | 72.9 ± 14.6 | 62.7 ± 20.8 |
| m.BF, % | 82.9 ± 8.4 | 84.6 ± 11.1 | 82.1 ± 14.3 |
| m.GL, % | 89.1 ± 5.7 | 84.7 ± 15.4 | 88.6 ± 3.3 |
| m.GM, % | 86.1 ± 7.3 | 90.6 ± 5.4 | 90.0 ± 4.9 |
| m.GT, % | 90.2 ± 4.8 | 86.5 ± 7.8 | 80.3 ± 17.8 |
| m.RF, % | 86.1 ± 6.6 | 84.3 ± 7.1 | 90.7 ± 5.8 |
| m.SO, % | 86.6 ± 7.8 | 88.0 ± 6.7 | 85.7 ± 12.7 |
| m.TA, % | 72.1 ± 24.7 | 77.9 ± 20.0 | 81.3 ± 15.4 |
| m.VL, % | 89.1 ± 6.5 | 86.9 ± 4.5 | 92.3 ± 6.0 |
| m.VM, % | 90.6 ± 6.3 | 86.6 ± 6.1 | 86.6 ± 7.2 |
| Functional symmetry | |||
| Achilles tendon, % | |||
| DL | 86.6 ± 5.0 | 84.4 ± 15.0 | 91.1 ± 6.8 |
| N-DL | 78.5 ± 8.6 | 89.5 ± 9.5 | 86.4 ± 6.0 |
| Ligament patellae, % | |||
| DL | 84.1 ± 6.5 | 84.4 ± 6.7 | 85.6 ± 7.5 |
| N-DL | 86.7 ± 5.1 | 83.1 ± 12.9 | 81.9 ± 4.7 |
| Knee, % | |||
| DL | 86.7 ± 5.1 | 70.9 ± 16.0 | 70.4 ± 16.0 |
| N-DL | 86.7 ± 6.7 | 67.8 ± 16.4 | 82.7 ± 5.5 |
| Ankle, % | |||
| DL | 59.0 ± 23.7 | 70.9 ± 21.3 | 55.0 ± 14.3 |
| N-DL | 73.4 ± 21.6 | 69.9 ± 22.8 | 53.7 ± 17.2 |
| Leg, % | |||
| DL | 85.4 ± 8.0 | 86.8 ± 9.6 | 87.3 ± 3.0 |
| N-DL | 83.3 ± 11.6 | 89.1 ± 5.6 | 88.1 ± 2.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buoite Stella, A.; Galimi, A.; Martini, M.; Di Lenarda, L.; Murena, L.; Deodato, M. Muscle Asymmetries in the Lower Limbs of Male Soccer Players: Preliminary Findings on the Association between Countermovement Jump and Tensiomyography. Sports 2022, 10, 177. https://doi.org/10.3390/sports10110177
Buoite Stella A, Galimi A, Martini M, Di Lenarda L, Murena L, Deodato M. Muscle Asymmetries in the Lower Limbs of Male Soccer Players: Preliminary Findings on the Association between Countermovement Jump and Tensiomyography. Sports. 2022; 10(11):177. https://doi.org/10.3390/sports10110177
Chicago/Turabian StyleBuoite Stella, Alex, Annalisa Galimi, Miriam Martini, Luca Di Lenarda, Luigi Murena, and Manuela Deodato. 2022. "Muscle Asymmetries in the Lower Limbs of Male Soccer Players: Preliminary Findings on the Association between Countermovement Jump and Tensiomyography" Sports 10, no. 11: 177. https://doi.org/10.3390/sports10110177
APA StyleBuoite Stella, A., Galimi, A., Martini, M., Di Lenarda, L., Murena, L., & Deodato, M. (2022). Muscle Asymmetries in the Lower Limbs of Male Soccer Players: Preliminary Findings on the Association between Countermovement Jump and Tensiomyography. Sports, 10(11), 177. https://doi.org/10.3390/sports10110177