
Development of a Novel Nordic Hamstring Exercise Performance Test Device: A Reliability and Intervention Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
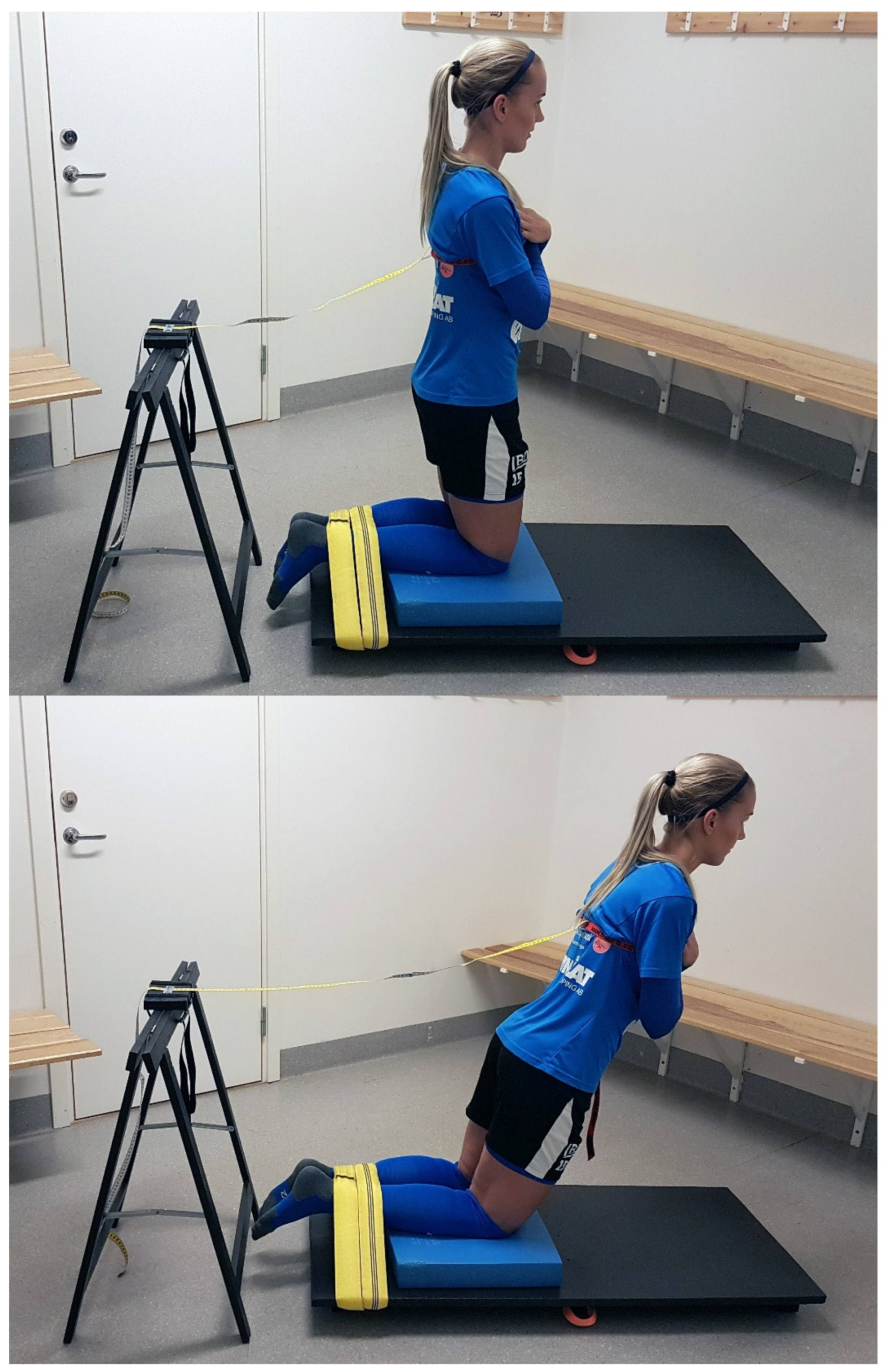
2.3. Development of the Test Device
2.4. Experimental Set-Up
2.5. Exercise Intervention Protocol
2.6. Statistical Analyses
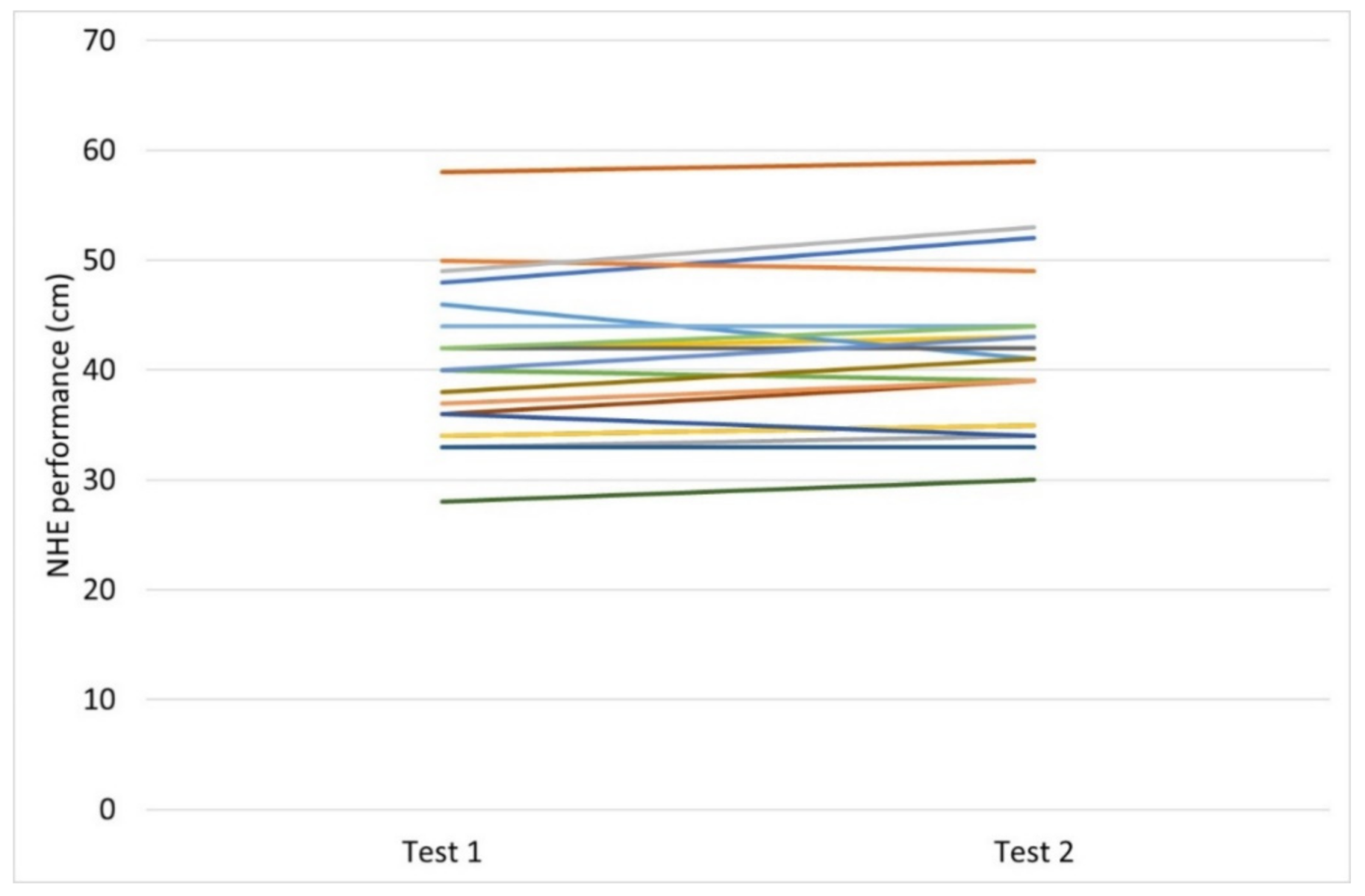
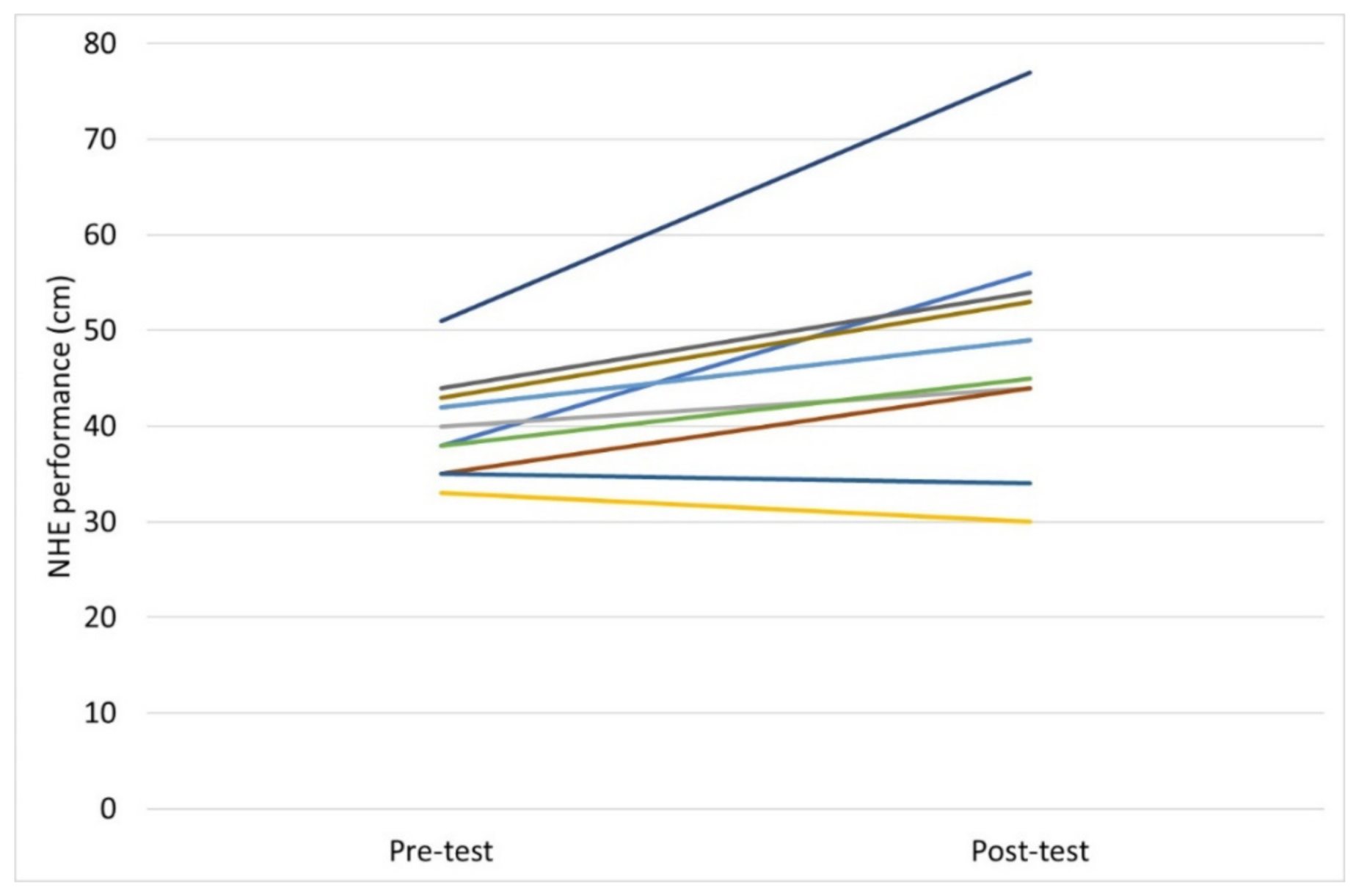
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ekstrand, J.; Hägglund, M.; Waldén, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagglund, M.; Walden, M.; Ekstrand, J. Risk factors for lower extremity muscle injury in professional soccer: The UEFA Injury Study. Am. J. Sports Med. 2013, 41, 327–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malliaropoulos, N.; Papacostas, E.; Kiritsi, O.; Papalada, A.; Gougoulias, N.; Maffulli, N. Posterior thigh muscle injuries in elite track and field athletes. Am. J. Sports Med. 2010, 38, 1813–1819. [Google Scholar] [CrossRef]
- Askling, C.; Tengvar, M.; Saartok, T.; Thorstensson, A. Sports related hamstring strains--two cases with different etiologies and injury sites. Scand. J. Med. Sci. Sports 2000, 10, 304–307. [Google Scholar] [CrossRef]
- Brooks, J.H.; Fuller, C.W.; Kemp, S.P.; Reddin, D.B. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am. J. Sports Med. 2006, 34, 1297–1306. [Google Scholar] [CrossRef]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Budtz-Jørgensen, E.; Hölmich, P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: A cluster-randomized controlled trial. Am. J. Sports Med. 2011, 39, 2296–2303. [Google Scholar] [CrossRef]
- van der Horst, N.; Smits, D.W.; Petersen, J.; Goedhart, E.A.; Backx, F.J. The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: A randomized controlled trial. Am. J. Sports Med. 2015, 43, 1316–1323. [Google Scholar] [CrossRef]
- Askling, C.; Karlsson, J.; Thorstensson, A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand. J. Med. Sci. Sports 2003, 13, 244–250. [Google Scholar] [CrossRef]
- Sugiura, Y.; Saito, T.; Sakuraba, K.; Sakuma, K.; Suzuki, E. Strength deficits identified with concentric action of the hip extensors and eccentric action of the hamstrings predispose to hamstring injury in elite sprinters. J. Orthop. Sports Phys. Ther. 2008, 38, 457–464. [Google Scholar] [CrossRef] [Green Version]
- Cuthbert, M.; Ripley, N.; McMahon, J.J.; Evans, M.; Haff, G.G.; Comfort, P. The Effect of Nordic Hamstring Exercise Intervention Volume on Eccentric Strength and Muscle Architecture Adaptations: A Systematic Review and Meta-analyses. Sports Med. 2020, 50, 83–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Dyk, N.; Behan, F.P.; Whiteley, R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: A systematic review and meta-analysis of 8459 athletes. Br. J. Sports Med. 2019, 53, 1362–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aagaard, P.; Andersen, J.L. Correlation between contractile strength and myosin heavy chain isoform composition in human skeletal muscle. Med. Sci. Sports Exerc. 1998, 30, 1217–1222. [Google Scholar] [CrossRef]
- Green, B.; Bourne, M.N.; Pizzari, T. Isokinetic strength assessment offers limited predictive validity for detecting risk of future hamstring strain in sport: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.A.; Bond, E.Q.; Sisto, S.A.; Nadler, S.F. The intra- and interrater reliability of hip muscle strength assessments using a handheld versus a portable dynamometer anchoring station. Arch. Phys. Med. Rehabil. 2004, 85, 598–603. [Google Scholar] [CrossRef] [PubMed]
- Thorborg, K.; Bandholm, T.; Schick, M.; Jensen, J.; Hölmich, P. Hip strength assessment using handheld dynamometry is subject to intertester bias when testers are of different sex and strength. Scand. J. Med. Sci. Sports 2013, 23, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Opar, D.A.; Piatkowski, T.; Williams, M.D.; Shield, A.J. A novel device using the Nordic hamstring exercise to assess eccentric knee flexor strength: A reliability and retrospective injury study. J. Orthop. Sports Phys. Ther. 2013, 43, 636–640. [Google Scholar] [CrossRef] [Green Version]
- Giacomo, J.; Lahti, J.; Hegyi, A.; Gerus, P.; Morin, J. A new testing and training device for hamstring muscle function. Sport Perform. Sci. Rep. 2018, 1, 1–4. [Google Scholar]
- Hickey, J.T.; Hickey, P.F.; Maniar, N.; Timmins, R.G.; Williams, M.D.; Pitcher, C.A.; Opar, D.A. A Novel Apparatus to Measure Knee Flexor Strength during Various Hamstring Exercises: A Reliability and Retrospective Injury Study. J. Orthop. Sports Phys. Ther. 2018, 48, 72–80. [Google Scholar] [CrossRef]
- Weatherwax, R.M.; Harris, N.K.; Kilding, A.E.; Dalleck, L.C. Incidence of V O2max Responders to Personalized versus Standardized Exercise Prescription. Med. Sci. Sports Exerc. 2019, 51, 681–691. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Domholdt, E. Physical Therapy Research: Principles and Applications, 2nd ed.; W.B. Saunders Company: Philadelphia, PA, USA, 2000. [Google Scholar]
- Shechtman, O. The coefficient of variation as an index of measurement reliability. In Methods of Clinical Epidemiology; Doi, S.A.R., Williams, G.M., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 39–49. [Google Scholar]
- Rhea, M.R. Determining the magnitude of treatment effects in strength training research through the use of the effect size. J. Strength Cond. Res. 2004, 18, 918–920. [Google Scholar] [PubMed]
- Grant, J.A.; Mohtadi, N.G.; Maitland, M.E.; Zernicke, R.F. Comparison of home versus physical therapy-supervised rehabilitation programs after anterior cruciate ligament reconstruction: A randomized clinical trial. Am. J. Sports Med. 2005, 33, 1288–1297. [Google Scholar] [CrossRef] [PubMed]
- van Dyk, N.; Witvrouw, E.; Bahr, R. Interseason variability in isokinetic strength and poor correlation with Nordic hamstring eccentric strength in football players. Scand. J. Med. Sci. Sports 2018, 28, 1878–1887. [Google Scholar] [CrossRef] [Green Version]
- Chalker, W.J.; Shield, A.J.; Opar, D.A.; Rathbone, E.N.; Keogh, J.W.L. Effect of acute augmented feedback on between limb asymmetries and eccentric knee flexor strength during the Nordic hamstring exercise. PeerJ 2018, 6, e4972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmins, R.G.; Bourne, M.N.; Shield, A.J.; Williams, M.D.; Lorenzen, C.; Opar, D.A. Biceps Femoris Architecture and Strength in Athletes with a Previous Anterior Cruciate Ligament Reconstruction. Med. Sci. Sports Exerc. 2016, 48, 337–345. [Google Scholar] [CrossRef] [Green Version]
- NordBord. NordBord Hamstring Testing System. Available online: https://valdperformance.com/nordbord/ (accessed on 28 June 2021).
- Medeiros, T.M.; Ribeiro-Alvares, J.B.; Fritsch, C.G.; Oliveira, G.S.; Severo-Silveira, L.; Pappas, E.; Baroni, B.M. Effect of Weekly Training Frequency With the Nordic Hamstring Exercise on Muscle-Strain Risk Factors in Football Players: A Randomized Trial. Int. J. Sports Physiol. Perform. 2020, 15, 1026–1033. [Google Scholar] [CrossRef]
- Augustsson, J.; Esko, A.; Thomeé, R.; Svantesson, U. Weight training of the thigh muscles using closed vs. open kinetic chain exercises: A comparison of performance enhancement. J. Orthop. Sports Phys. Ther. 1998, 27, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Bahr, R.; Thorborg, K.; Ekstrand, J. Evidence-based hamstring injury prevention is not adopted by the majority of Champions League or Norwegian Premier League football teams: The Nordic Hamstring survey. Br. J. Sports Med. 2015, 49, 1466–1471. [Google Scholar] [CrossRef] [Green Version]
- Alonso-Fernandez, D.; Lopez-Barreiro, J.; Garganta, R.; Taboada-Iglesias, Y. Acute impact of Nordic hamstring exercise on sprint performance after 24, 48 and 72 hours. Sports Biomech. 2021, 1–15. [Google Scholar] [CrossRef]
- Sale, D.G. Neural adaptation to resistance training. Med. Sci. Sports Exerc. 1988, 20 (Suppl. 5), S135–S145. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, N.D.M.; Miramonti, A.A.; Hill, E.C.; Smith, C.M.; Cochrane-Snyman, K.C.; Housh, T.J.; Cramer, J.T. Greater Neural Adaptations following High- vs. Low-Load Resistance Training. Front. Physiol. 2017, 8, 331. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N.S.; Heckbert, S.R. Patients as their own controls in studies of therapeutic efficacy: Can we trust the results of non-randomized trials? J. Gen. Intern. Med. 1988, 3, 381–383. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± SD |
|---|---|
| Age, year | 20 ± 4 |
| Height, m | 1.69 ± 0.06 |
| Weight, kg | 63 ± 6 |
| Football practice, hours per week | 5.4 ± 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Augustsson, J.; Augustsson, S.R. Development of a Novel Nordic Hamstring Exercise Performance Test Device: A Reliability and Intervention Study. Sports 2022, 10, 26. https://doi.org/10.3390/sports10020026
Augustsson J, Augustsson SR. Development of a Novel Nordic Hamstring Exercise Performance Test Device: A Reliability and Intervention Study. Sports. 2022; 10(2):26. https://doi.org/10.3390/sports10020026
Chicago/Turabian StyleAugustsson, Jesper, and Sofia Ryman Augustsson. 2022. "Development of a Novel Nordic Hamstring Exercise Performance Test Device: A Reliability and Intervention Study" Sports 10, no. 2: 26. https://doi.org/10.3390/sports10020026
APA StyleAugustsson, J., & Augustsson, S. R. (2022). Development of a Novel Nordic Hamstring Exercise Performance Test Device: A Reliability and Intervention Study. Sports, 10(2), 26. https://doi.org/10.3390/sports10020026