
Psychological Adaptations to High-Intensity Interval Training in Overweight and Obese Adults: A Topical Review



Abstract
:1. Introduction
1.1. Obesity: A Public Health Challenge
1.2. Exercise, Obesity and Mental Health
1.3. High-Intensity Interval Training and Obesity
2. Methods
2.1. Literature Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
3. Results
3.1. Articles Retrieved
3.2. Article Characteristics
3.3. Exercise Protocols
4. Psychological Adaptations
4.1. Adherence
4.2. Affective Responses
4.3. Exercise Enjoyment
4.4. Health-Related Quality of Life
4.5. Anxiety
4.6. Depression
5. Discussion
5.1. Future Research
5.2. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Overweight and Obesity. WHO Fact Sheet N°311 Website. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 9 June 2021).
- World Health Organization. Noncommunicable Diseases Country Profiles 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Romieu, I.; Dossus, L.; Barquera, S.; Blottiere, H.M.; Franks, P.W.; Gunter, M.; Hwalla, N.; Hursting, S.D.; Leitzmann, M.; Margetts, B.; et al. Obesity, Energy balance and obesity: What are the main drivers? Cancer Causes Control. 2017, 28, 247–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremmel, M.; Gerdtham, U.G.; Nilsson, P.M.; Saha, S. Economic Burden of Obesity: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2017, 14, 435. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Li, H. Obesity: Epidemiology, Pathophysiology, and Therapeutics. Front. Endocrinol. 2021, 12, 706978. [Google Scholar] [CrossRef] [PubMed]
- Do, K.; Brown, R.E.; Wharton, S.; Ardern, C.I.; Kuk, J.L. Association between cardiorespiratory fitness and metabolic risk factors in a population with mild to severe obesity. BMC Obes. 2018, 5, 5. [Google Scholar] [CrossRef]
- de Wit, L.M.; van Straten, A.; van Herten, M.; Penninx, B.W.; Cuijpers, P. Depression and body mass index, a u-shaped association. BMC Public Health 2009, 9, 14. [Google Scholar] [CrossRef] [Green Version]
- Schvey, N.A.; Sbrocco, T.; Bakalar, J.L.; Ress, R.; Barmine, M.; Gorlick, J.; Pine, A.; Stephens, M.; Tanofsky-Kraff, M. The Experience of Weight Stigma Among Gym Members with Overweight and Obesity. Stigma Health 2017, 2, 292–306. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Polonsky, H.M. The Psychosocial Burden of Obesity. Endocrinol. Metab. Clin. N. Am. 2016, 45, 677–688. [Google Scholar] [CrossRef]
- Baumeister, H.; Harter, M. Mental disorders in patients with obesity in comparison with healthy probands. Int. J. Obes. 2007, 31, 1155–1164. [Google Scholar] [CrossRef] [Green Version]
- Montesi, L.; El Ghoch, M.; Brodosi, L.; Calugi, S.; Marchesini, G.; Dalle Grave, R. Long-term weight loss maintenance for obesity: A multidisciplinary approach. Diabetes Metab. Syndr. Obes. 2016, 9, 37–46. [Google Scholar]
- Backhouse, S.H.; Ekkekakis, P.; Bidle, S.J.; Foskett, A.; Williams, C. Exercise makes people feel better but people are inactive: Paradox or artifact? J. Sport Exerc. Psychol. 2007, 29, 498–517. [Google Scholar] [CrossRef] [Green Version]
- Carraca, E.V.; Encantado, J.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; van Baak, M.; Dicker, D.; Ermolao, A.; Farpour-Lambert, N.; et al. Effect of exercise training on psychological outcomes in adults with overweight or obesity: A systematic review and meta-analysis. Obes. Rev. 2021, 22 (Suppl. S4), e13261. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E. The Health Benefits of Exercise in Overweight and Obese Patients. Curr. Sports Med. Rep. 2019, 18, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Pearsall, R.; Smith, D.J.; Pelosi, A.; Geddes, J. Exercise therapy in adults with serious mental illness: A systematic review and meta-analysis. BMC Psychiatry 2014, 14, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gariepy, G.; Nitka, D.; Schmitz, N. The association between obesity and anxiety disorders in the population: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 407–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, K.M.; Bruffaerts, R.; Simon, G.E.; Alonso, J.; Angermeyer, M.; de Girolamo, G.; Demyttenaere, K.; Gasquet, I.; Haro, J.M.; Karam, E.; et al. Obesity and mental disorders in the general population: Results from the world mental health surveys. Int. J. Obes. 2008, 32, 192–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2009, 43, 1–2. [Google Scholar] [PubMed]
- Kercher, V.M.; Kercher, K.; Bennion, T.; Levy, P.; Alexander, C.; Amaral, P.C.; Li, Y.-M.; Han, J.; Liu, Y.; Wang, R.; et al. 2022 Fitness Trends from Around the Globe. ACSMs Health Fit. J. 2022, 26, 21–37. [Google Scholar] [CrossRef]
- Zhai, L.; Zhang, Y.; Zhang, D. Sedentary behaviour and the risk of depression: A meta-analysis. Br. J. Sports Med. 2015, 49, 705–709. [Google Scholar] [CrossRef]
- American College of Sports Medicine; Liguori, G.; Feito, Y.; Fountaine, C.; Roy, B.A. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2021. [Google Scholar]
- Roy, M.; Williams, S.M.; Brown, R.C.; Meredith-Jones, K.A.; Osborne, H.; Jospe, M.; Taylor, R.W. High-Intensity Interval Training in the Real World: Outcomes from a 12-Month Intervention in Overweight Adults. Med. Sci. Sports Exerc. 2018, 50, 1818–1826. [Google Scholar] [CrossRef]
- Salmon, J.; Owen, N.; Crawford, D.; Bauman, A.; Sallis, J.F. Physical activity and sedentary behavior: A population-based study of barriers, enjoyment, and preference. Health Psychol. 2003, 22, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Stutts, W.C. Physical activity determinants in adults. Perceived benefits, barriers, and self efficacy. AAOHN J. 2002, 50, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Owen, N.; Bauman, A.E.; Sallis, J.F.; Brown, W. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sports Exerc. 2002, 34, 1996–2001. [Google Scholar] [CrossRef]
- Jung, M.E.; Bourne, J.E.; Beauchamp, M.R.; Robinson, E.; Little, J.P. High-intensity interval training as an efficacious alternative to moderate-intensity continuous training for adults with prediabetes. J. Diabetes Res. 2015, 2015, 191595. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Little, J.P.; Macdonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Batrakoulis, A.; Jamurtas, A.Z.; Fatouros, I.G. High-Intensity Interval Training in Metabolic Diseases: Physiological Adaptations. ACSM’s Health Fit. J. 2021, 25, 54–59. [Google Scholar] [CrossRef]
- Sabag, A.; Little, J.P.; Johnson, N.A. Low-volume high-intensity interval training for cardiometabolic health. J. Physiol. 2021; online ahead of print. [Google Scholar] [CrossRef]
- Sultana, R.N.; Sabag, A.; Keating, S.E.; Johnson, N.A. The Effect of Low-Volume High-Intensity Interval Training on Body Composition and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1687–1721. [Google Scholar] [CrossRef]
- Taylor, J.L.; Holland, D.J.; Spathis, J.G.; Beetham, K.S.; Wisloff, U.; Keating, S.E.; Coombes, J.S. Guidelines for the delivery and monitoring of high intensity interval training in clinical populations. Prog. Cardiovasc. Dis. 2019, 62, 140–146. [Google Scholar] [CrossRef]
- Batrakoulis, A. European survey of fitness trends for 2020. ACSMs Health Fit. J. 2019, 23, 28–35. [Google Scholar] [CrossRef]
- Cassidy, S.; Thoma, C.; Houghton, D.; Trenell, M.I. High-intensity interval training: A review of its impact on glucose control and cardiometabolic health. Diabetologia 2017, 60, 7–23. [Google Scholar] [CrossRef] [Green Version]
- Weston, K.S.; Wisloff, U.; Coombes, J.S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Turk, Y.; Theel, W.; Kasteleyn, M.J.; Franssen, F.M.E.; Hiemstra, P.S.; Rudolphus, A.; Taube, C.; Braunstahl, G.J. High intensity training in obesity: A Meta-analysis. Obes. Sci. Pract. 2017, 3, 258–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Middleton, K.R.; Anton, S.D.; Perri, M.G. Long-Term Adherence to Health Behavior Change. Am. J. Lifestyle Med. 2013, 7, 395–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekkekakis, P.; Parfitt, G.; Petruzzello, S.J. The pleasure and displeasure people feel when they exercise at different intensities: Decennial update and progress towards a tripartite rationale for exercise intensity prescription. Sports Med. 2011, 41, 641–671. [Google Scholar] [CrossRef]
- Ekkekakis, P.; Vazou, S.; Bixby, W.R.; Georgiadis, E. The mysterious case of the public health guideline that is (almost) entirely ignored: Call for a research agenda on the causes of the extreme avoidance of physical activity in obesity. Obes. Rev. 2016, 17, 313–329. [Google Scholar] [CrossRef]
- Batrakoulis, A.; Loules, G.; Georgakouli, K.; Tsimeas, P.; Draganidis, D.; Chatzinikolaou, A.; Papanikolaou, K.; Deli, C.K.; Syrou, N.; Comoutos, N.; et al. High-intensity interval neuromuscular training promotes exercise behavioral regulation, adherence and weight loss in inactive obese women. Eur. J. Sport Sci. 2020, 20, 783–792. [Google Scholar] [CrossRef]
- Poon, E.T.; Little, J.P.; Sit, C.H.; Wong, S.H. The effect of low-volume high-intensity interval training on cardiometabolic health and psychological responses in overweight/obese middle-aged men. J. Sports Sci. 2020, 38, 1997–2004. [Google Scholar] [CrossRef]
- Arad, A.D.; Albu, J.B.; DiMenna, F.J. Feasibility of a progressive protocol of high-intensity interval training for overweight/obese, sedentary African American women: A retrospective analysis. BMC Sports Sci. Med. Rehabil. 2020, 12, 59. [Google Scholar] [CrossRef]
- Cheema, B.S.; Davies, T.B.; Stewart, M.; Papalia, S.; Atlantis, E. The feasibility and effectiveness of high-intensity boxing training versus moderate-intensity brisk walking in adults with abdominal obesity: A pilot study. BMC Sports Sci. Med. Rehabil. 2015, 7, 3. [Google Scholar] [CrossRef]
- Heinrich, K.M.; Patel, P.M.; O’Neal, J.L.; Heinrich, B.S. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: An intervention study. BMC Public Health 2014, 14, 789. [Google Scholar] [CrossRef] [Green Version]
- Vella, C.A.; Taylor, K.; Drummer, D. High-intensity interval and moderate-intensity continuous training elicit similar enjoyment and adherence levels in overweight and obese adults. Eur. J. Sport Sci. 2017, 17, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, S.O.; Wilson, O.J.; Taylor, A.S.; Thogersen-Ntoumani, C.; Adlan, A.M.; Wagenmakers, A.J.; Shaw, C.S. Low-Volume High-Intensity Interval Training in a Gym Setting Improves Cardio-Metabolic and Psychological Health. PLoS ONE 2015, 10, e0139056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batrakoulis, A.; Jamurtas, A.Z.; Draganidis, D.; Georgakouli, K.; Tsimeas, P.; Poulios, A.; Syrou, N.; Deli, C.K.; Papanikolaou, K.; Tournis, S.; et al. Hybrid Neuromuscular Training Improves Cardiometabolic Health and Alters Redox Status in Inactive Overweight and Obese Women: A Randomized Controlled Trial. Antioxidants 2021, 10, 1601. [Google Scholar] [CrossRef] [PubMed]
- Batrakoulis, A.; Jamurtas, A.Z.; Georgakouli, K.; Draganidis, D.; Deli, C.K.; Papanikolaou, K.; Avloniti, A.; Chatzinikolaou, A.; Leontsini, D.; Tsimeas, P.; et al. High intensity, circuit-type integrated neuromuscular training alters energy balance and reduces body mass and fat in obese women: A 10-month training-detraining randomized controlled trial. PLoS ONE 2018, 13, e0202390. [Google Scholar] [CrossRef] [Green Version]
- Batrakoulis, A.; Jamurtas, A.Z.; Tsimeas, P.; Poulios, A.; Perivoliotis, K.; Syrou, N.; Papanikolaou, K.; Draganidis, D.; Deli, C.K.; Metsios, G.S.; et al. Hybrid-type, multicomponent interval training upregulates musculoskeletal fitness of adults with overweight and obesity in a volume-dependent manner: A 1-year dose-response randomised controlled trial. Eur. J. Sport Sci. 2022, 1–62. [Google Scholar] [CrossRef]
- Batrakoulis, A.; Tsimeas, P.; Deli, C.K.; Vlachopoulos, D.; Ubago-Guisado, E.; Poulios, A.; Chatzinikolaou, A.; Draganidis, D.; Papanikolaou, K.; Georgakouli, K.; et al. Hybrid neuromuscular training promotes musculoskeletal adaptations in inactive overweight and obese women: A training-detraining randomized controlled trial. J. Sports Sci. 2021, 39, 503–512. [Google Scholar] [CrossRef]
- Wewege, M.; van den Berg, R.; Ward, R.E.; Keech, A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 635–646. [Google Scholar] [CrossRef]
- Moroshko, I.; Brennan, L.; O’Brien, P. Predictors of dropout in weight loss interventions: A systematic review of the literature. Obes. Rev. 2011, 12, 912–934. [Google Scholar] [CrossRef]
- Reljic, D.; Lampe, D.; Wolf, F.; Zopf, Y.; Herrmann, H.J.; Fischer, J. Prevalence and predictors of dropout from high-intensity interval training in sedentary individuals: A meta-analysis. Scand. J. Med. Sci. Sports 2019, 29, 1288–1304. [Google Scholar] [CrossRef]
- Lox, S.L.; Martin Ginis, K.A.; Petruzzello, S.J. The Psychology of Exercise: Integrating Theory and Practice, 4th ed.; Routledge: New York, NY, USA, 2014. [Google Scholar]
- Ekkekakis, P.; Lind, E.; Vazou, S. Affective responses to increasing levels of exercise intensity in normal-weight, overweight, and obese middle-aged women. Obesity 2010, 18, 79–85. [Google Scholar] [CrossRef]
- Chu, I.H.; Wu, P.T.; Wu, W.L.; Yu, H.C.; Yu, T.C.; Chang, Y.K. Affective Responses during High-Intensity Interval Exercise Compared with Moderate-Intensity Continuous Exercise in Inactive Women. Int. J. Environ. Res. Public Health 2021, 18, 5393. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, B.R.; Slama, F.A.; Deslandes, A.C.; Furtado, E.S.; Santos, T.M. Continuous and high-intensity interval training: Which promotes higher pleasure? PLoS ONE 2013, 8, e79965. [Google Scholar] [CrossRef] [PubMed]
- Frazao, D.T.; de Farias Junior, L.F.; Dantas, T.C.; Krinski, K.; Elsangedy, H.M.; Prestes, J.; Hardcastle, S.J.; Costa, E.C. Feeling of Pleasure to High-Intensity Interval Exercise Is Dependent of the Number of Work Bouts and Physical Activity Status. PLoS ONE 2016, 11, e0152752. [Google Scholar]
- Ram, A.; Marcos, L.; Morey, R.; Clark, T.; Hakansson, S.; Ristov, M.; Franklin, A.; McCarthy, C.; De Carli, L.; Jones, M.D.; et al. Exercise for affect and enjoyment in overweight or obese males: A comparison of high-intensity interval training and moderate-intensity continuous training. Psychol. Health Med. 2021, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Boyd, J.C.; Simpson, C.A.; Jung, M.E.; Gurd, B.J. Reducing the intensity and volume of interval training diminishes cardiovascular adaptation but not mitochondrial biogenesis in overweight/obese men. PLoS ONE 2013, 8, e68091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, J.P.; Jung, M.E.; Wright, A.E.; Wright, W.; Manders, R.J. Effects of high-intensity interval exercise versus continuous moderate-intensity exercise on postprandial glycemic control assessed by continuous glucose monitoring in obese adults. Appl. Physiol. Nutr. Metab. 2014, 39, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Sim, A.Y.; Wallman, K.E.; Fairchild, T.J.; Guelfi, K.J. High-intensity intermittent exercise attenuates ad-libitum energy intake. Int. J. Obes. 2014, 38, 417–422. [Google Scholar] [CrossRef]
- Martinez, N.; Kilpatrick, M.W.; Salomon, K.; Jung, M.E.; Little, J.P. Affective and Enjoyment Responses to High-Intensity Interval Training in Overweight-to-Obese and Insufficiently Active Adults. J. Sport Exerc. Psychol. 2015, 37, 138–149. [Google Scholar] [CrossRef]
- Astorino, T.A.; Clark, A.; De La Rosa, A.; De Revere, J.L. Enjoyment and affective responses to two regimes of high intensity interval training in inactive women with obesity. Eur. J. Sport Sci. 2019, 19, 1377–1385. [Google Scholar] [CrossRef]
- Decker, E.S.; Ekkekakis, P. More efficient, perhaps, but at what price? Pleasure and enjoyment responses to high-intensity interval exercise in low-active women with obesity. Psychol. Sport Exerc. 2017, 28, 1–10. [Google Scholar] [CrossRef]
- Santos, A.; Stork, M.J.; Locke, S.R.; Jung, M.E. Psychological responses to HIIT and MICT over a 2-week progressive randomized trial among individuals at risk of type 2 diabetes. J. Sports Sci. 2021, 39, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Kong, Z.; Fan, X.; Sun, S.; Song, L.; Shi, Q.; Nie, J. Comparison of High-Intensity Interval Training and Moderate-to-Vigorous Continuous Training for Cardiometabolic Health and Exercise Enjoyment in Obese Young Women: A Randomized Controlled Trial. PLoS ONE 2016, 11, e0158589. [Google Scholar] [CrossRef] [PubMed]
- Smith-Ryan, A.E. Enjoyment of high-intensity interval training in an overweight/obese cohort: A short report. Clin. Physiol. Funct. Imaging 2017, 37, 89–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thum, J.S.; Parsons, G.; Whittle, T.; Astorino, T.A. High-Intensity Interval Training Elicits Higher Enjoyment than Moderate Intensity Continuous Exercise. PLoS ONE 2017, 12, e0166299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartlett, J.D.; Close, G.L.; MacLaren, D.P.; Gregson, W.; Drust, B.; Morton, J.P. High-intensity interval running is perceived to be more enjoyable than moderate-intensity continuous exercise: Implications for exercise adherence. J. Sports Sci. 2011, 29, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Heisz, J.J.; Tejada, M.G.; Paolucci, E.M.; Muir, C. Enjoyment for High-Intensity Interval Exercise Increases during the First Six Weeks of Training: Implications for Promoting Exercise Adherence in Sedentary Adults. PLoS ONE 2016, 11, e0168534. [Google Scholar] [CrossRef]
- Taylor, V.H.; Forhan, M.; Vigod, S.N.; McIntyre, R.S.; Morrison, K.M. The impact of obesity on quality of life. Best. Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 139–146. [Google Scholar] [CrossRef]
- Hassan, M.K.; Joshi, A.V.; Madhavan, S.S.; Amonkar, M.M. Obesity and health-related quality of life: A cross-sectional analysis of the US population. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1227–1232. [Google Scholar] [CrossRef] [Green Version]
- Ul-Haq, Z.; Mackay, D.F.; Fenwick, E.; Pell, J.P. Meta-analysis of the association between body mass index and health-related quality of life among adults, assessed by the SF-36. Obesity 2013, 21, E322–E327. [Google Scholar] [CrossRef]
- Slagter, S.N.; van Vliet-Ostaptchouk, J.V.; van Beek, A.P.; Keers, J.C.; Lutgers, H.L.; van der Klauw, M.M.; Wolffenbuttel, B.H. Health-Related Quality of Life in Relation to Obesity Grade, Type 2 Diabetes, Metabolic Syndrome and Inflammation. PLoS ONE 2015, 10, e0140599. [Google Scholar] [CrossRef]
- Sperlich, B.; Wallmann-Sperlich, B.; Zinner, C.; Von Stauffenberg, V.; Losert, H.; Holmberg, H.C. Functional High-Intensity Circuit Training Improves Body Composition, Peak Oxygen Uptake, Strength, and Alters Certain Dimensions of Quality of Life in Overweight Women. Front. Physiol. 2017, 8, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tous-Espelosin, M.; Gorostegi-Anduaga, I.; Corres, P.; MartinezAguirre-Betolaza, A.; Maldonado-Martin, S. Impact on Health-Related Quality of Life after Different Aerobic Exercise Programs in Physically Inactive Adults with Overweight/Obesity and Primary Hypertension: Data from the EXERDIET-HTA Study. Int. J. Environ. Res. Public Health 2020, 17, 9349. [Google Scholar] [CrossRef] [PubMed]
- Arboleda-Serna, V.H.; Patiño-Villada, F.A.; Pinzón-Castro, D.A.; Arango-Vélez, E.F. Effects of low-volume, high-intensity interval training on maximal oxygen consumption, body fat percentage and health-related quality of life in women with overweight: A randomized controlled trial. J. Exerc. Sci. Fit. 2022, 20, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Freese, E.C.; Acitelli, R.M.; Gist, N.H.; Cureton, K.J.; Evans, E.M.; O’Connor, P.J. Effect of six weeks of sprint interval training on mood and perceived health in women at risk for metabolic syndrome. J. Sport Exerc. Psychol. 2014, 36, 610–618. [Google Scholar] [CrossRef]
- Reljic, D.; Frenk, F.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Low-volume high-intensity interval training improves cardiometabolic health, work ability and well-being in severely obese individuals: A randomized-controlled trial sub-study. J. Transl. Med. 2020, 18, 419. [Google Scholar] [CrossRef]
- Stavrinou, P.S.; Bogdanis, G.C.; Giannaki, C.D.; Terzis, G.; Hadjicharalambous, M. Effects of high-intensity interval training frequency on perceptual responses and future physical activity participation. Appl. Physiol. Nutr. Metab. 2019, 44, 952–957. [Google Scholar] [CrossRef]
- Stavrinou, P.S.; Bogdanis, G.C.; Giannaki, C.D.; Terzis, G.; Hadjicharalambous, M. High-intensity Interval Training Frequency: Cardiometabolic Effects and Quality of Life. Int. J. Sports Med. 2018, 39, 210–217. [Google Scholar] [CrossRef]
- Alarcon-Gomez, J.; Chulvi-Medrano, I.; Martin-Rivera, F.; Calatayud, J. Effect of High-Intensity Interval Training on Quality of Life, Sleep Quality, Exercise Motivation and Enjoyment in Sedentary People with Type 1 Diabetes Mellitus. Int. J. Environ. Res. Public Health 2021, 18, 12612. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Duraes, A.R.; Reis, H.; Neves, V.R.; Martinez, B.P.; Carvalho, V.O. High-intensity interval training versus moderate-intensity continuous training on exercise capacity and quality of life in patients with coronary artery disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2017, 24, 1696–1707. [Google Scholar] [CrossRef]
- Brown, D.W.; Balluz, L.S.; Heath, G.W.; Moriarty, D.G.; Ford, E.S.; Giles, W.H.; Mokdad, A.H. Associations between recommended levels of physical activity and health-related quality of life. Findings from the 2001 Behavioral Risk Factor Surveillance System (BRFSS) survey. Prev. Med. 2003, 37, 520–528. [Google Scholar] [CrossRef]
- Vuillemin, A.; Boini, S.; Bertrais, S.; Tessier, S.; Oppert, J.M.; Hercberg, S.; Guillemin, F.; Briancon, S. Leisure time physical activity and health-related quality of life. Prev. Med. 2005, 41, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Sareen, J.; Jacobi, F.; Cox, B.J.; Belik, S.L.; Clara, I.; Stein, M.B. Disability and poor quality of life associated with comorbid anxiety disorders and physical conditions. Arch. Intern. Med. 2006, 166, 2109–2116. [Google Scholar] [CrossRef] [PubMed]
- Dunn, A.L.; Trivedi, M.H.; O’Neal, H.A. Physical activity dose-response effects on outcomes of depression and anxiety. Med. Sci. Sports Exerc. 2001, 33 (Suppl. S6), S587–S597, discussion 609–610. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Brownell, K.D. Psychosocial origins of obesity stigma: Toward changing a powerful and pervasive bias. Obes. Rev. 2003, 4, 213–227. [Google Scholar] [CrossRef]
- Dinas, P.C.; Koutedakis, Y.; Flouris, A.D. Effects of exercise and physical activity on depression. Ir. J. Med. Sci. 2011, 180, 319–325. [Google Scholar] [CrossRef]
- Sander, C.; Ueck, P.; Mergl, R.; Gordon, G.; Hegerl, U.; Himmerich, H. Physical activity in depressed and non-depressed patients with obesity. Eat. Weight Disord. 2018, 23, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Ouerghi, N.; Selmi, O.; Ben Khalifa, W.; Ben Fradj, M.K.; Feki, M.; Kaabachi, N.; Bouassida, A. Effect of High-intensity Intermittent Training Program on Mood State in Overweight/Obese Young Men. Iran. J. Public Health 2016, 45, 951–952. [Google Scholar]
- Min, L.; Wang, D.; You, Y.; Fu, Y.; Ma, X. Effects of High-Intensity Interval Training on Sleep: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10973. [Google Scholar] [CrossRef]
- Viana, R.B.; Gentil, P.; Naves, J.P.A.; Rebelo, A.C.S.; Santos, D.A.T.; Braga, M.A.O.; de Lira, C.A.B. Interval Training Improves Depressive Symptoms but Not Anxious Symptoms in Healthy Women. Front. Psychiatry 2019, 10, 661. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, N.A.; Kersting, A.; Riedel-Heller, S.G.; Luck-Sikorski, C. Body Dissatisfaction in Individuals with Obesity Compared to Normal-Weight Individuals: A Systematic Review and Meta-Analysis. Obes. Facts 2016, 9, 424–441. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.; Sirois-Leclerc, H.; Tulloch, H. The Impact of Long-Term Physical Activity Interventions for Overweight/Obese Postmenopausal Women on Adiposity Indicators, Physical Capacity, and Mental Health Outcomes: A Systematic Review. J. Obes. 2016, 2016, 6169890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ten Hoor, G.A.; Kok, G.; Peters, G.Y.; Frissen, T.; Schols, A.; Plasqui, G. The Psychological Effects of Strength Exercises in People who are Overweight or Obese: A Systematic Review. Sports Med. 2017, 47, 2069–2081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martland, R.; Mondelli, V.; Gaughran, F.; Stubbs, B. Can high-intensity interval training improve physical and mental health outcomes? A meta-review of 33 systematic reviews across the lifespan. J. Sports Sci. 2020, 38, 430–469. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129 (Suppl. S2), S102–S138. [Google Scholar] [CrossRef] [Green Version]
- Burgess, E.; Hassmen, P.; Welvaert, M.; Pumpa, K.L. Behavioural treatment strategies improve adherence to lifestyle intervention programmes in adults with obesity: A systematic review and meta-analysis. Clin. Obes. 2017, 7, 105–114. [Google Scholar] [CrossRef]
- Leijon, M.E.; Bendtsen, P.; Stahle, A.; Ekberg, K.; Festin, K.; Nilsen, P. Factors associated with patients self-reported adherence to prescribed physical activity in routine primary health care. BMC Fam. Pract. 2010, 11, 38. [Google Scholar] [CrossRef] [Green Version]
- Stork, M.J.; Banfield, L.E.; Gibala, M.J.; Martin Ginis, K.A. A scoping review of the psychological responses to interval exercise: Is interval exercise a viable alternative to traditional exercise? Health Psychol. Rev. 2017, 11, 324–344. [Google Scholar] [CrossRef]
- Kilpatrick, M.W.; Greeley, S.J.; Collins, L.H. The Impact of Continuous and Interval Cycle Exercise on Affect and Enjoyment. Res. Q Exerc. Sport 2015, 86, 244–251. [Google Scholar] [CrossRef]
- Batrakoulis, A.; Fatouros, I.G.; Chatzinikolaou, A.; Draganidis, D.; Georgakouli, K.; Papanikolaou, K.; Deli, C.K.; Tsimeas, P.; Avloniti, A.; Syrou, N.; et al. Dose-response effects of high-intensity interval neuromuscular exercise training on weight loss, performance, health and quality of life in inactive obese adults: Study rationale, design and methods of the DoIT trial. Contemp. Clin. Trials. Commun. 2019, 15, 100386. [Google Scholar] [CrossRef]
- Hardcastle, S.J.; Ray, H.; Beale, L.; Hagger, M.S. Why sprint interval training is inappropriate for a largely sedentary population. Front. Psychol. 2014, 5, 1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
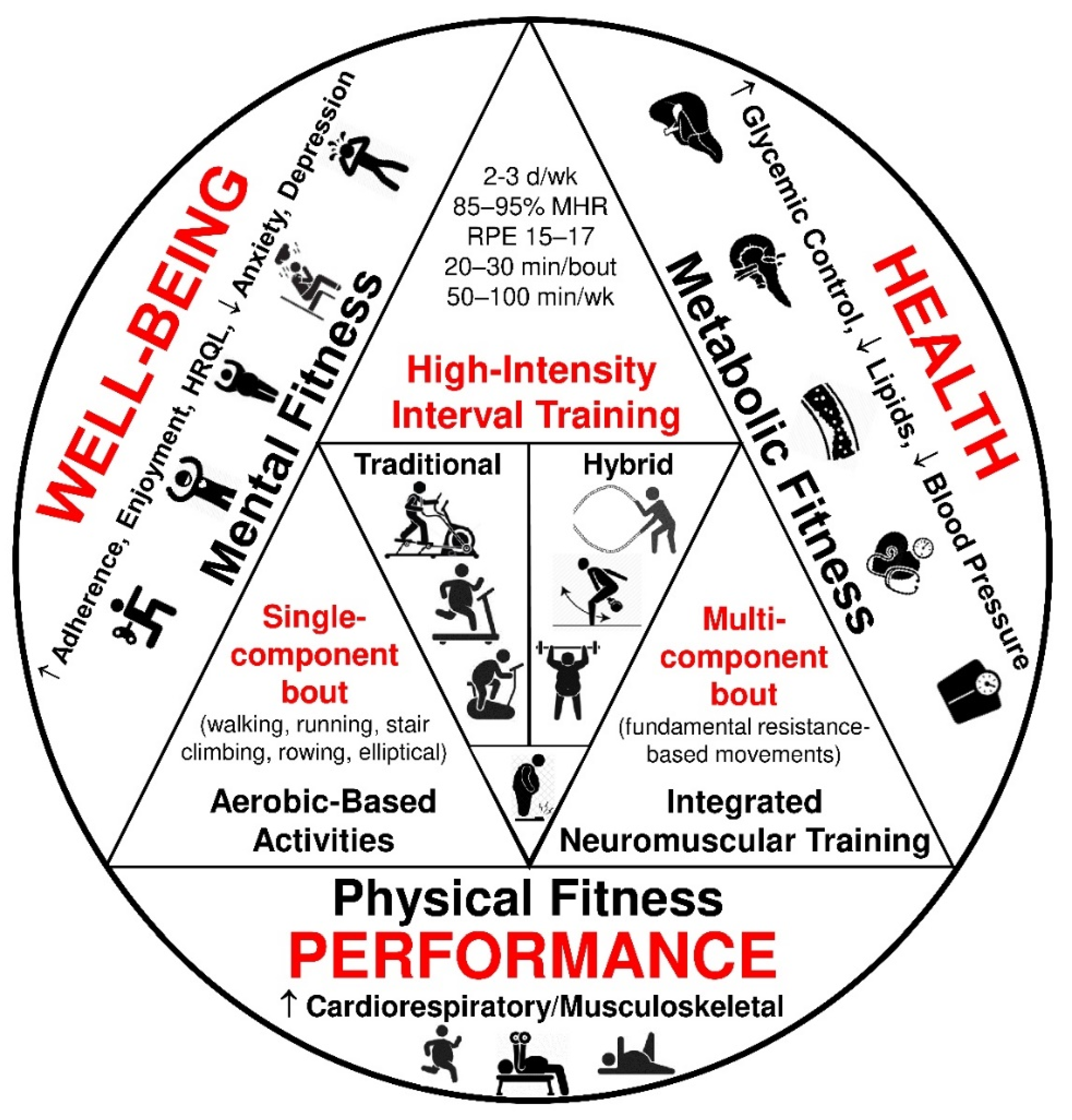
| Model | Format | Training Parameters | Modalities |
|---|---|---|---|
| Traditional | Single-component (aerobic-based) |
| One of the following:
|
| Hybrid | Multi-component (resistance-based) |
| Full-body movements using either body-weight 1 or integrated neuromuscular exercises 2 with adjunct equipment such as
|
| Article | Country | Duration (wks.) | Sample 1 N/F/M | Mean Age ± SD (yrs.) | Activity, BMI Classification | Study Design | HIIT Classification | Summary Description of HIIT Intervention (Frequency, Intensity, Time 2, Type) | Psychological Findings | Dropout 3 |
|---|---|---|---|---|---|---|---|---|---|---|
| Arad (2020) | United States | 14 | 28/28/0 | 29.0 ± 4.0 | Sedentary, Overweight/ Obese | Chronic, RCT | Traditional (single- component) | 3 d/wk.; work intervals: 75–90% HRR, 30–60 s; work/recovery ratio: 1:7–1:3; 24 min; cycling (supervised, lab-based) | adherence (↓) | 35% |
| Arboleda-Serna (2022) | Colombia | 8 | 35/35/0 | 29.6 ± 7.7 | Active, Overweight | Chronic, RCT | Traditional (single- component) | 3 d/wk.; work intervals: 15 × 30 s (90–95% HRmax), rest intervals: 60 s (50–60% HRmax), 21.5 min, walking, jogging, or running (supervised, field-based) | quality of life (↔) | 0% |
| Astorino (2019) | United States | 6 | 19/19/0 | 37.0 ± 10.0 | Inactive, Obese | Chronic, within- subject | Traditional (single- component) | 3 d/wk., work intervals: 6–10 × 60–120 s (70–110% PPO), rest intervals: 5–9 × 60–120 s, 19–26 min, walking, cycling, jogging, rowing, or elliptical machine (supervised, semi-field) | enjoyment (↔), affect (↔) | 11% |
| Batrakoulis (2020) | Greece | 40 | 49/49/0 | 36.4 ± 4.4 | Inactive, Overweight/ Obese | Chronic, RCT | Hybrid (multi- component) | 3 d/wk., work intervals: 8–10 × 20–40 s (73–88% HRmax), rest intervals: 20–40 s (passive), 1–3 rounds, 23–41 min, integrated neuromuscular training (supervised, field-based) | adherence (↑), vitality (↑), distress (↓) | 11% |
| Boyd (2013) | Canada | 3 | 19/0/19 | 22.7 ± 3.9 | Sedentary, Overweight/ Obese | Chronic, between-subject | Traditional (single- component) | 3 d/wk., work intervals: 8–10 × 60 s (70–100% PWR), rest intervals: 7–9 × 60 s (active/low-intensity), 15–19 min, cycling (supervised, lab-based) | adherence (↑), enjoyment (↑), affect (↑) | 0% |
| Cheema (2015) | Australia | 12 | 12/7/5 | 39.0 ± 17.0 | Inactive, Overweight/ Obese | Chronic, between-subject | Hybrid (multi- component) | 4 d/wk., work intervals: 2 min (>75% HRmax), rest intervals: 1 min (standing/pacing), 40 min, boxing (supervised, field-based) | adherence (↑), quality of life (↑) | 0% |
| Chu (2021) | Taiwan | – | 60/60/0 | 22.1 ± 2.0 | Inactive, Overweight/ Obese | Acute, within- subject (cross-over) | Traditional (single- component) | 1 bout, work intervals: 10 × 45 s (Wmax), rest intervals: 9 × 75 s (50 watts), 50 rpm throughout the session, 18 min, cycling (supervised, lab-based) | affect (↓) | 0% |
| Decker (2016) | United States | – | 30/30/0 | 39.3 ± 11.2 | Inactive, Obese | Acute, within- subject (cross-over) | Traditional (single- component) | 1 bout, work intervals: 4 × 3 min (115% of Watts at the ventilatory threshold), rest intervals: 4 × 2 min (85% of Watts at the ventilatory threshold), 20 min, cycling (supervised, lab-based) | affect (↓), enjoyment (↓) | 20% |
| Ekkekakis (2010) | United States | – | 27/27/0 | 42.5 ± 5.6 | Inactive, Overweight/ Obese | Acute, within- subject (cross-over) | Traditional (single- component) | 1 bout, incremental treadmill test began at a speed of 2.5 mph (1.11 m/s) and 0% grade for 2 min, walking (supervised, lab-based) | affect (↓) | 20% |
| Freese (2014) | United States | 6 | 47/47/0 | 52.1 ± 9.0 | Inactive, Overweight/ Obese | Chronic, RCT | Traditional (single- component) | 3 d/wk., work intervals: 4–8 × 30 s cycle (all-out sprints), rest intervals: 4–8 × 4 min (passive), 18–36 min, cycling (supervised, lab-based) | quality of life (↑) | 21% |
| Heinrich (2014) | United States | 8 | 23/13/10 | 26.8 ± 5.9 | Inactive, Obese | Chronic, between-subject | Hybrid (multi- component) | 3 d/wk., self-selected high-intensity, 30 min, aerobic (e.g., rowing), body-weight (9 fundamental movements), and weightlifting exercises in singular or multiple combinations (supervised, lab-based) | adherence (↑), enjoyment (↑) | 25% |
| Kong (2016) | China | 5 | 31/31/0 | 25.7 ± 2.4 | Sedentary, Overweight/ Obese | Chronic, between-subject | Traditional (single- component) | 4 d/wk., work intervals: 60 × 8 s (sprint), rest intervals: 60 × 12 s (passive), 20 min, cycling (supervised, lab-based) | enjoyment (↑) | 13% |
| Little (2014) | Canada | – | 10/8/2 | 40.6 ± 10.7 | Inactive, Overweight/ Obese | Acute, within- subject (cross-over) | Traditional (single- component) | 1 bout, work intervals: 10 × 1 min (~90% HRpeak), rest intervals: 10 × 1 min (passive), 20 min, cycling (supervised, lab-based) | affect (↔), enjoyment (↔) | 0% |
| Martinez (2015) | United States | – | 20/9/11 | 22.0 ± 4.0 | Inactive, Overweight/ Obese | Acute, within- subject (cross-over) | Traditional (single- component) | 1 bout, work intervals: 30, 60, and 90 s, rest intervals: 30, 60, and 90 s (passive), 24 min, cycling (supervised, lab-based) | affect (↓), enjoyment (↑) | 0% |
| Ouerghi (2016) | Tunisia | 8 | 12/0/12 | 18.2 ± 1.0 | Inactive, Overweight/ Obese | Chronic, comparative study | Traditional (single- component) | 3 d/wk., work intervals: 30 s (100–110% MAV), rest intervals: 30 s (active: 50% MAV), running (supervised, lab-based) | mood (including anxiety (↓) and depression (↓)) | 0% |
| Poon (2020) | Canada | 8 | 24/0/24 | 48.1 ± 5.2 | Inactive, Overweight/ Obese | Chronic, between-subject | Traditional (single- component) | 3 d/wk., work intervals: 6–10 × 1 min (80–90% HRmax), rest intervals: 1 min (walk, 50% HRmax), 21–29 min, running (semi-supervised, semi-field) | enjoyment (↔) | 0% |
| Ram (2021) | Australia | 6 | 28/0/28 | 28.3 ± 6.9 | Sedentary, Overweight/ Obese | Chronic, between-subject | Traditional (single- component) | 3 d/wk., work intervals: 10 × 1 min (90–100% Wpeak); rest intervals: 9 × 1 min (active: 15% Wpeak) 19 min, cycling (supervised, lab-based) | affect (↑), enjoyment (↔) | 16% |
| Reljic (2020) | Germany | 12 | 65/36/29 | 48.7 ± 9.9 | Sedentary, Obese | Chronic, RCT | Traditional (single- component) | 2 d/wk., work intervals: 5 × 1 min (80–95% HRmax), rest intervals: 4 × 1 min (active), 9 min, cycling (supervised, lab-based) | quality of life (↑) | 17% |
| Roy (2018) | New Zealand | 48 | 104/59/45 | 43.5 ± 10.2 | Sedentary, Overweight/ Obese | Chronic, within- subject | Traditional (single- component) | 3 d/wk., work intervals: 3 × 30 s (maximal effort), 5–10 × 1 min (≥80% HRmax, RPE: 8), or 1 × 4 min (at the highest intensity that could be maintained), rest intervals: 1–3 min (active), 21–24 min, home-based exercises, sprinting, hill-walking, cycling, and exercise machines (unsupervised, field-based) | adherence (↓), enjoyment (↑) | 20% |
| Santos (2021) | Canada | 2 | 99/70/29 | 51.9 ± 9.6 | Sedentary, Overweight/ Obese | Chronic, between-subject | Traditional (single- component) | 5 d/wk., work intervals: 4–10 × 1 min (~77–95% HRmax), rest intervals: 3–9 × 1 min (~60% HRmax), 7–19 min, cycling, walking, or elliptical machine (semi-supervised, semi-field) | affect (↔), enjoyment (↔) | 9% |
| Shepherd (2015) | United Kingdom | 10 | 90/60/30 | 42.0 ± 11.0 | Inactive, Overweight | Chronic, between-subject | Traditional (single- component) | 3 d/wk., work intervals: 15–60 s (>90% HRmax), rest intervals: 45–120 s (active), 18–25 min, cycling (supervised, field-based) | affect (↑), vitality (↑) | 9% |
| Sim (2014) | Australia | – | 17/0/17 | 30.0 ± 8.0 | Inactive, Overweight | Acute, within- subject (cross-over) | Traditional (single- component) | 1 bout, work intervals: 60 s (100% VO2peak) or 15 s (170% VO2peak), rest intervals: 240 s (50% VO2peak) or 60 s (32% VO2peak), 30 min, cycling (supervised, lab-based) | enjoyment (↑) | 0% |
| Smith-Ryan (2015) | United States | 3 | 42/22/20 | 35.9 ± 12.1 | Inactive, Overweight/ Obese | Chronic, between-subject | Traditional (single- component) | 3 d/wk., work intervals: 10 × 1 min (90% PPO) or 5 × 2 min (80–100% PPO), rest intervals: 9 × 1 min or 4 × 1 min (passive), 15–20 min, cycling (supervised, lab-based) | enjoyment (↑) | 0% |
| Sperlich (2017) | Germany | 9 | 22/22/0 | 23.0 ± 2.0 | Inactive, Overweight | Chronic, between-subject | Hybrid (multi- component) | 3 d/wk., work intervals: 5–7 × 30–60 s, rest intervals: 30–60 s (passive), 3–6 rounds, 23–41 min, multi-stimulating, circuit-like, multiple-joint training (supervised, lab-based) | quality of life (↑) | 0% |
| Vella (2017) | United States | 8 | 17/10/7 | 26.2 ± 7.8 | Sedentary, Overweight/ Obese | Chronic, between-subject | Traditional (single- component) | 4 d/wk., work intervals: rest intervals: 10 × 1 min (75–80% HRR), rest intervals: 10 × 1 min (35–40% HRR), 20 min, running, cycling, or elliptical machine (semi-supervised, semi-field) | adherence (↔), enjoyment (↔) | 11% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batrakoulis, A.; Fatouros, I.G. Psychological Adaptations to High-Intensity Interval Training in Overweight and Obese Adults: A Topical Review. Sports 2022, 10, 64. https://doi.org/10.3390/sports10050064
Batrakoulis A, Fatouros IG. Psychological Adaptations to High-Intensity Interval Training in Overweight and Obese Adults: A Topical Review. Sports. 2022; 10(5):64. https://doi.org/10.3390/sports10050064
Chicago/Turabian StyleBatrakoulis, Alexios, and Ioannis G. Fatouros. 2022. "Psychological Adaptations to High-Intensity Interval Training in Overweight and Obese Adults: A Topical Review" Sports 10, no. 5: 64. https://doi.org/10.3390/sports10050064
APA StyleBatrakoulis, A., & Fatouros, I. G. (2022). Psychological Adaptations to High-Intensity Interval Training in Overweight and Obese Adults: A Topical Review. Sports, 10(5), 64. https://doi.org/10.3390/sports10050064