
Could Proprioceptive Stimuli Change Saddle Pressure on Male Cyclists during Different Hand Positions? An Exploratory Study of the Effect of the Equistasi® Device





Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Acquisition Protocol
2.3. Instrumental Protocol
2.4. Equistasi® Device
2.5. Statistical Analysis
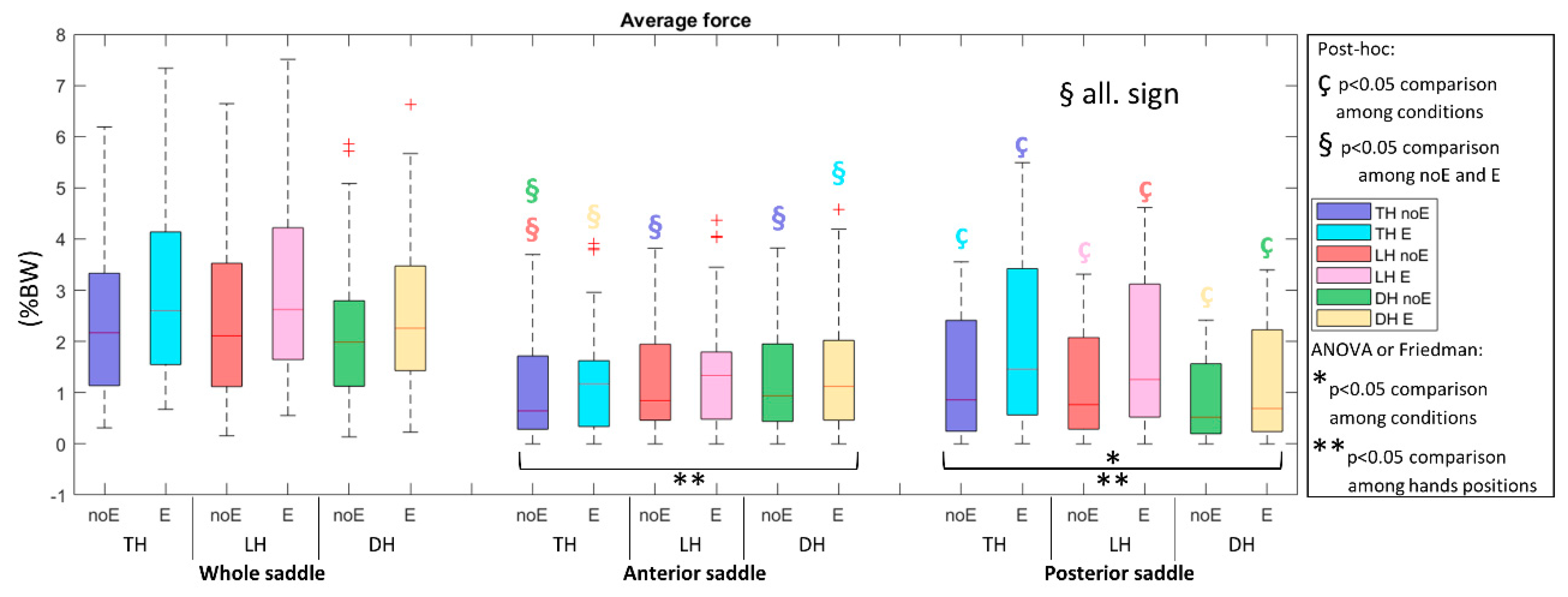
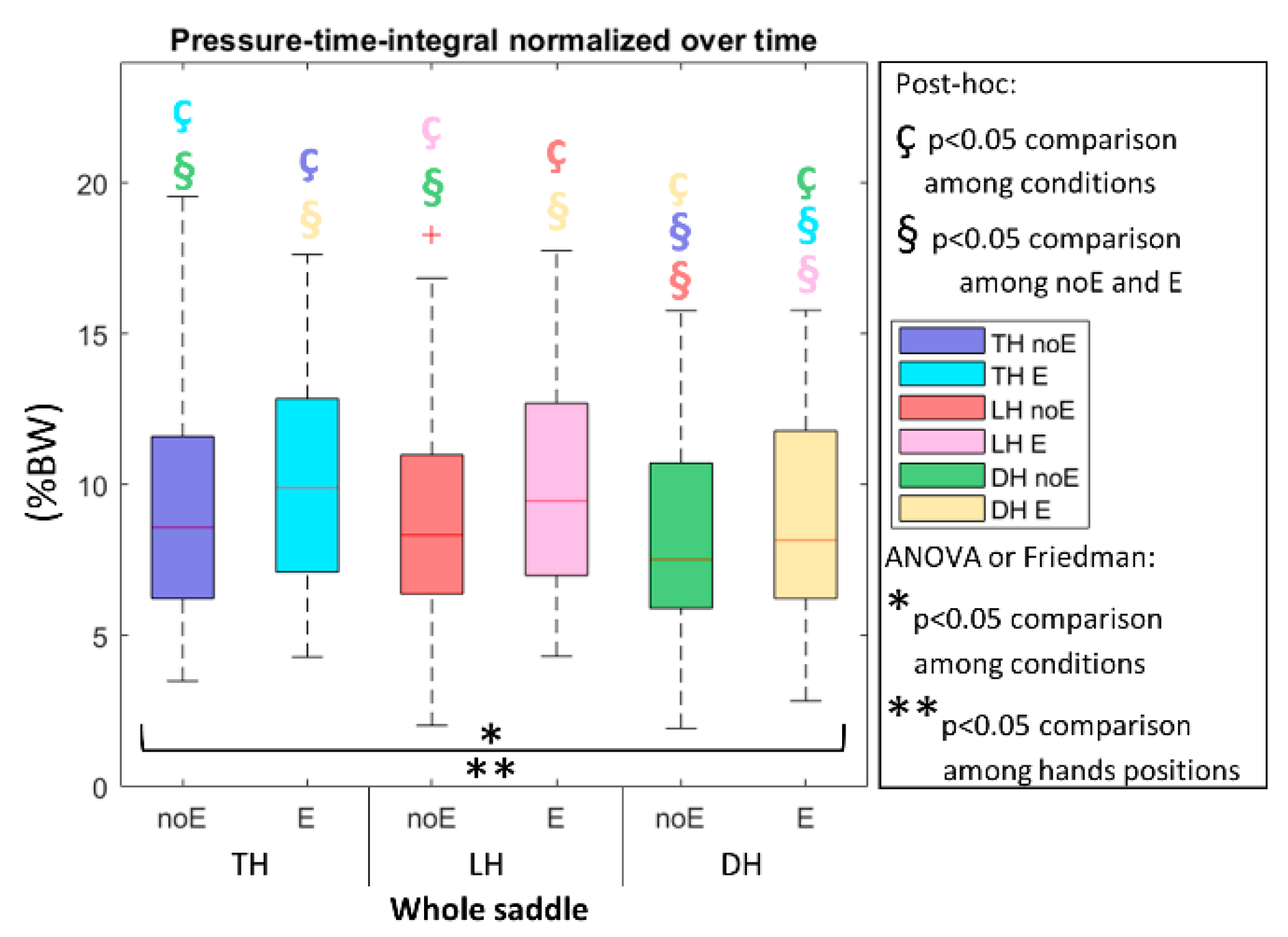
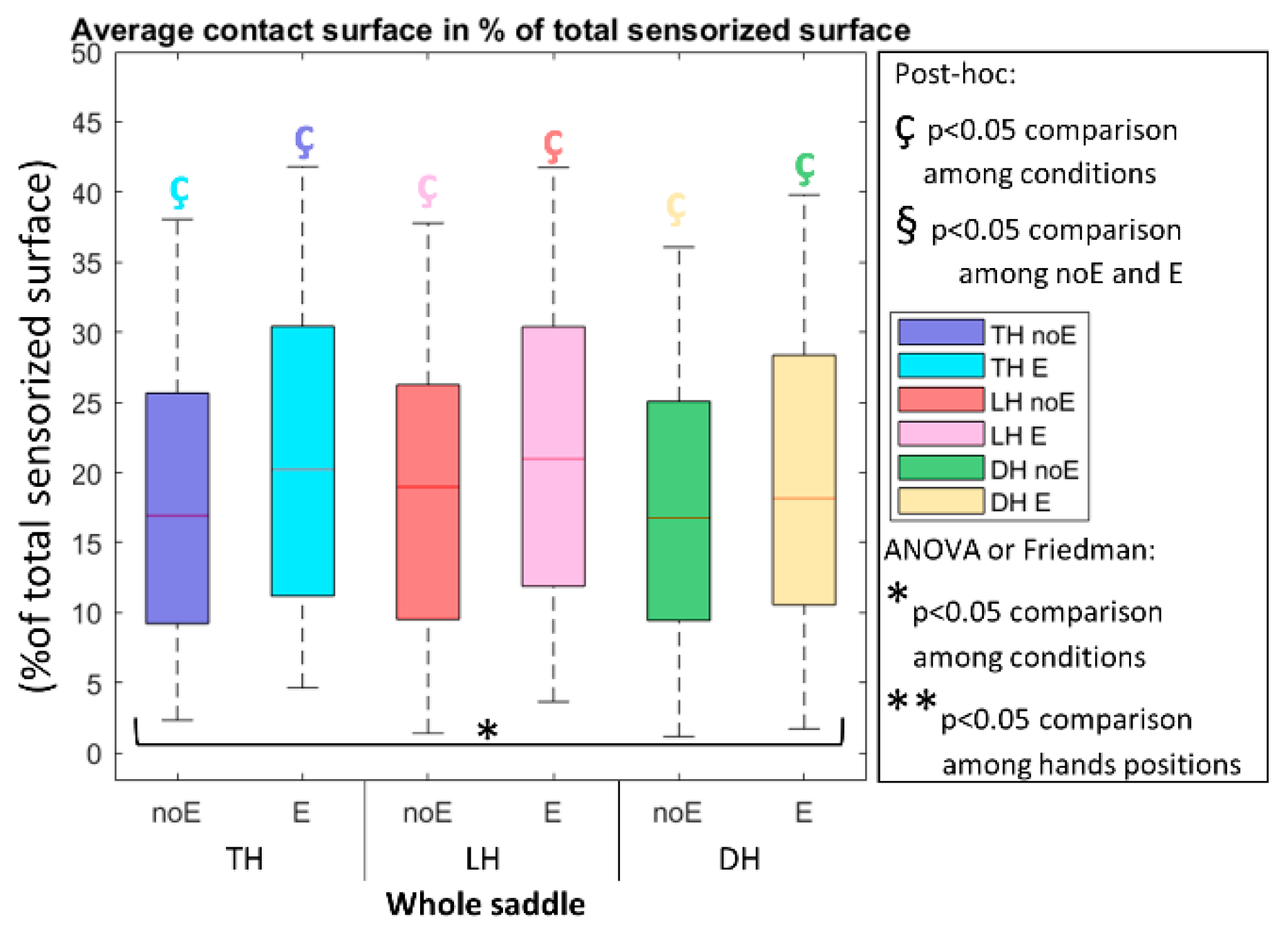
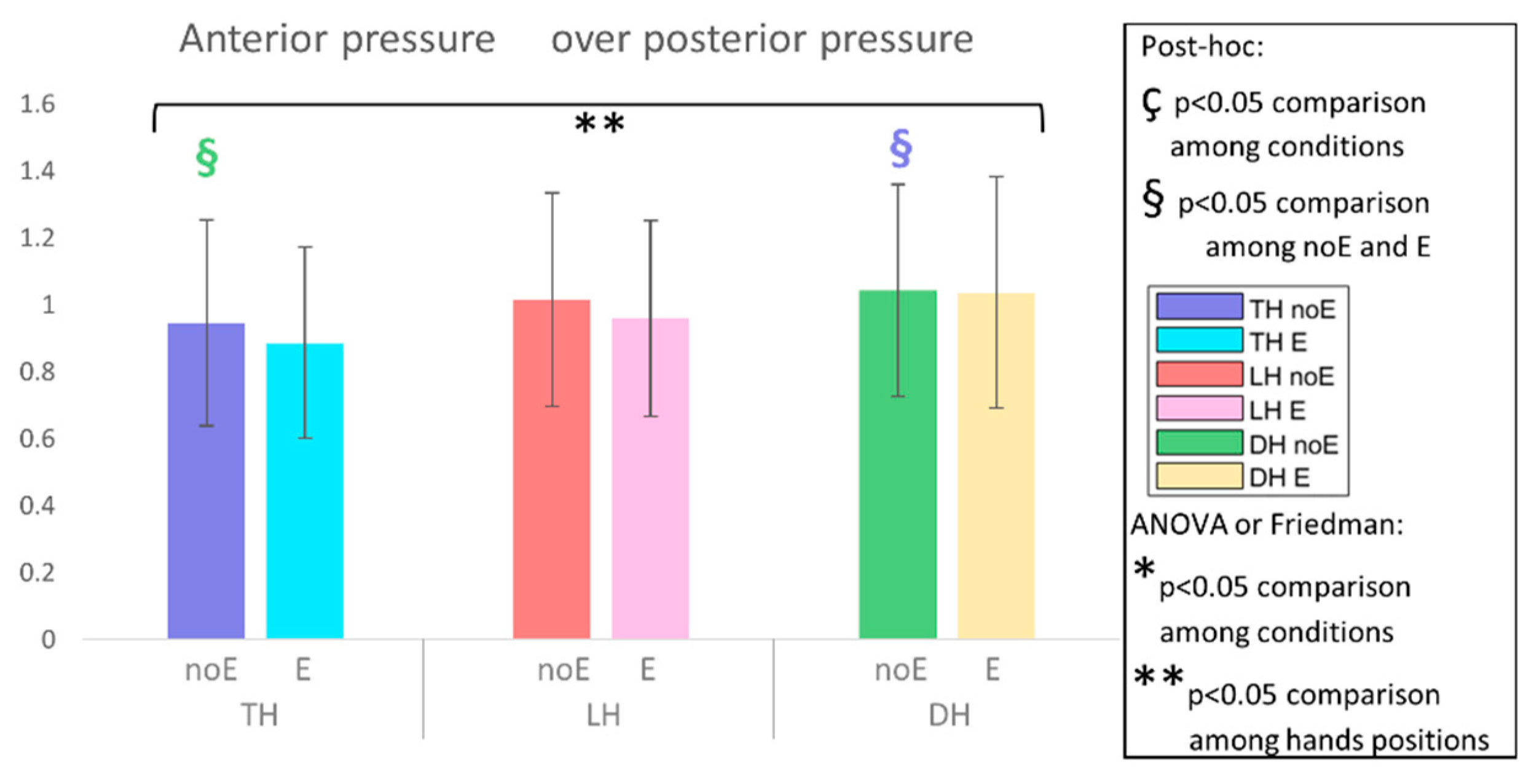
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bassett, D.R.; Pucher, J.; Buehler, R.; Thompson, D.L.; Crouter, S.E. Walking, Cycling, and Obesity Rates in Europe, North America, and Australia. J. Phys. Act. Health 2008, 5, 795–814. [Google Scholar] [CrossRef]
- Bauman, A.E.; Rissel, C. Cycling and Health: An Opportunity for Positive Change? Med. J. Aust. 2009, 190, 347–348. [Google Scholar] [CrossRef]
- Oja, P.; Titze, S.; Bauman, A.; de Geus, B.; Krenn, P.; Reger-Nash, B.; Kohlberger, T. Health Benefits of Cycling: A Systematic Review. Scand. J. Med. Sci. Sports 2011, 21, 496–509. [Google Scholar] [CrossRef]
- Dettori, N.J.; Norvell, D.C. Non-Traumatic Bicycle Injuries: A Review of the Literature. Sports Med. 2006, 36, 7–18. [Google Scholar] [CrossRef]
- Litwinowicz, K.; Choroszy, M.; Wróbel, A. Strategies for Reducing the Impact of Cycling on the Perineum in Healthy Males: Systematic Review and Meta-Analysis. Sports Med. 2021, 51, 275–287. [Google Scholar] [CrossRef]
- Marcolin, G.; Petrone, N.; Reggiani, C.; Panizzolo, F.A.; Paoli, A. Biomechanical Comparison of Shorts With Different Pads: An Insight into the Perineum Protection Issue. Medicine 2015, 94, e1186. [Google Scholar] [CrossRef]
- Leibovitch, I.; Mor, Y. The Vicious Cycling: Bicycling Related Urogenital Disorders. Eur. Urol. 2005, 47, 277–286, discussion 286–287. [Google Scholar] [CrossRef]
- Sommer, F.; Goldstein, I.; Korda, J.B. Bicycle Riding and Erectile Dysfunction: A Review. J. Sex. Med. 2010, 7, 2346–2358. [Google Scholar] [CrossRef]
- Gemery, J.M.; Nangia, A.K.; Mamourian, A.C.; Reid, S.K. Digital Three-Dimensional Modelling of the Male Pelvis and Bicycle Seats: Impact of Rider Position and Seat Design on Potential Penile Hypoxia and Erectile Dysfunction. BJU Int. 2007, 99, 135–140. [Google Scholar] [CrossRef]
- Bressel, E.; Reeve, T.; Parker, D.; Cronin, J. Influence of Bicycle Seat Pressure on Compression of the Perineum: A MRI Analysis. J. Biomech. 2007, 40, 198–202. [Google Scholar] [CrossRef]
- Lowe, B.D.; Schrader, S.M.; Breitenstein, M.J. Effect of Bicycle Saddle Designs on the Pressure to the Perineum of the Bicyclist. Med. Sci. Sports Exerc. 2004, 36, 1055–1062. [Google Scholar] [CrossRef]
- Bressel, E.; Cronin, J. Bicycle Seat Interface Pressure: Reliability, Validity, and Influence of Hand Position and Workload. J. Biomech. 2005, 38, 1325–1331. [Google Scholar] [CrossRef]
- Bressel, E.; Bliss, S.; Cronin, J. A Field-Based Approach for Examining Bicycle Seat Design Effects on Seat Pressure and Perceived Stability. Appl. Ergon. 2009, 40, 472–476. [Google Scholar] [CrossRef]
- Schrader, S.M.; Breitenstein, M.J.; Lowe, B.D. Cutting off the Nose to Save the Penis. J. Sex. Med. 2008, 5, 1932–1940. [Google Scholar] [CrossRef]
- Swart, J.; Holliday, W. Cycling Biomechanics Optimization-the (R) Evolution of Bicycle Fitting. Curr. Sports Med. Rep. 2019, 18, 490–496. [Google Scholar] [CrossRef]
- Bressel, E.; Nash, D.; Dolny, D. Association between Attributes of a Cyclist and Bicycle Seat Pressure. J. Sex. Med. 2010, 7, 3424–3433. [Google Scholar] [CrossRef]
- Cycling Biomechanics. Available online: https://www.physio-pedia.com/Cycling_Biomechanics (accessed on 14 October 2021).
- Seo, N.J.; Lakshminarayanan, K.; Bonilha, L.; Lauer, A.W.; Schmit, B.D. Effect of Imperceptible Vibratory Noise Applied to Wrist Skin on Fingertip Touch Evoked Potentials—An EEG Study. Physiol. Rep. 2015, 3, e12624. [Google Scholar] [CrossRef] [Green Version]
- Alfonsi, E.; Paone, P.; Tassorelli, C.; De Icco, R.; Moglia, A.; Alvisi, E.; Marchetta, L.; Fresia, M.; Montini, A.; Calabrese, M.; et al. Acute Effects of High-Frequency Microfocal Vibratory Stimulation on the H Reflex of the Soleus Muscle. A Double-Blind Study in Healthy Subjects. Funct. Neurol. 2015, 30, 269–274. [Google Scholar] [CrossRef]
- Nanhoe-Mahabier, W.; Allum, J.H.; Pasman, E.P.; Overeem, S.; Bloem, B.R. The Effects of Vibrotactile Biofeedback Training on Trunk Sway in Parkinson’s Disease Patients. Parkinsonism Relat. Disord. 2012, 18, 1017–1021. [Google Scholar] [CrossRef] [Green Version]
- De Nunzio, A.M.; Grasso, M.; Nardone, A.; Godi, M.; Schieppati, M. Alternate Rhythmic Vibratory Stimulation of Trunk Muscles Affects Walking Cadence and Velocity in Parkinson’s Disease. Clin. Neurophysiol. 2010, 121, 240–247. [Google Scholar] [CrossRef]
- Volpe, D.; Giantin, M.G.; Fasano, A. A Wearable Proprioceptive Stabilizer (Equistasi®) for Rehabilitation of Postural Instability in Parkinson’s Disease: A Phase II Randomized Double-Blind, Double-Dummy, Controlled Study. PLoS ONE 2014, 9, e112065. [Google Scholar] [CrossRef]
- Peppe, A.; Paravati, S.; Baldassarre, M.G.; Bakdounes, L.; Spolaor, F.; Guiotto, A.; Pavan, D.; Sawacha, Z.; Bottino, S.; Clerici, D.; et al. Proprioceptive Focal Stimulation (Equistasi®) May Improve the Quality of Gait in Middle-Moderate Parkinson’s Disease Patients. Double-Blind, Double-Dummy, Randomized, Crossover, Italian Multicentric Study. Front. Neurol. 2019, 10, 998. [Google Scholar] [CrossRef]
- Spolaor, F.; Romanato, M.; Annamaria, G.; Peppe, A.; Bakdounes, L.; To, D.-K.; Volpe, D.; Sawacha, Z. Relationship between Muscular Activity and Postural Control Changes after Proprioceptive Focal Stimulation (Equistasi®) in Middle-Moderate Parkinson’s Disease Patients: An Explorative Study. Sensors 2021, 21, 560. [Google Scholar] [CrossRef]
- Sawyer, S.M.; McNeil, R.; Francis, K.L.; Matskarofski, J.Z.; Patton, G.C.; Bhutta, Z.A.; Esangbedo, D.O.; Klein, J.D. The Age of Paediatrics. Lancet Child Adolesc. Health 2019, 3, 822–830. [Google Scholar] [CrossRef]
- Le Categorie di Tesseramento. Available online: https://amatoriale.federciclismo.it/it/infopage/le-categorie-di-tesseramento/2776054d-32a1-42d7-adef-2bb878e6135e/ (accessed on 9 May 2022).
- Thompson, M.; Medley, A. Forward and Lateral Sitting Functional Reach in Younger, Middle-Aged, and Older Adults. J. Geriatr. Phys. Ther. 2007, 30, 43–48. [Google Scholar] [CrossRef]
- Courtine, G.; De Nunzio, A.M.; Schmid, M.; Beretta, M.V.; Schieppati, M. Stance- and Locomotion-Dependent Processing of Vibration-Induced Proprioceptive Inflow from Multiple Muscles in Humans. J. Neurophysiol. 2007, 97, 772–779. [Google Scholar] [CrossRef]
- Larsen, A.S.; Larsen, F.G.; Sørensen, F.F.; Hedegaard, M.; Støttrup, N.; Hansen, E.A.; Madeleine, P. The Effect of Saddle Nose Width and Cutout on Saddle Pressure Distribution and Perceived Discomfort in Women during Ergometer Cycling. Appl. Ergon. 2018, 70, 175–181. [Google Scholar] [CrossRef]
- Carpes, F.P.; Dagnese, F.; Kleinpaul, J.F.; de Assis Martins, E.; Mota, C.B. Bicycle Saddle Pressure: Effects of Trunk Position and Saddle Design on Healthy Subjects. Urol. Int. 2009, 82, 8–11. [Google Scholar] [CrossRef]
- Wang, Y.; Liang, L.; Wang, D.; Tang, Y.; Wu, X.; Li, L.; Liu, Y. Cycling with Low Saddle Height Is Related to Increased Knee Adduction Moments in Healthy Recreational Cyclists. Eur. J. Sport Sci. 2020, 20, 461–467. [Google Scholar] [CrossRef]
- Holliday, W.; Fisher, J.; Swart, J. The Effects of Relative Cycling Intensity on Saddle Pressure Indexes. J. Sci. Med. Sport 2019, 22, 1097–1101. [Google Scholar] [CrossRef]
- Bolourchi, F.; Hull, M.L. Measurement of Rider Induced Loads during Simulated Bicycling. J. Appl. Biomech. 1985, 1, 308–329. [Google Scholar] [CrossRef] [Green Version]
- Stone, C.; Hull, M.L. The Effect of Rider Weight on Rider-Induced Loads during Common Cycling Situations. J. Biomech. 1995, 28, 365–375. [Google Scholar] [CrossRef]
- Wilson, C.; Bush, T.R. Interface Forces on the Seat during a Cycling Activity. Clin. Biomech. 2007, 22, 1017–1023. [Google Scholar] [CrossRef]
- Costes, A.; Turpin, N.A.; Villeger, D.; Moretto, P.; Watier, B. A Reduction of the Saddle Vertical Force Triggers the Sit-Stand Transition in Cycling. J. Biomech. 2015, 48, 2998–3003. [Google Scholar] [CrossRef] [Green Version]
- Schrader, S.M.; Breitenstein, M.J.; Clark, J.C.; Lowe, B.D.; Turner, T.W. Nocturnal Penile Tumescence and Rigidity Testing in Bicycling Patrol Officers. J. Androl. 2002, 23, 927–934. [Google Scholar]
- Bressel, E.; Larson, B.J. Bicycle Seat Designs and Their Effect on Pelvic Angle, Trunk Angle, and Comfort. Med. Sci. Sports Exerc. 2003, 35, 327–332. [Google Scholar] [CrossRef]
- Slane, J.; Timmerman, M.; Ploeg, H.-L.; Thelen, D.G. The Influence of Glove and Hand Position on Pressure over the Ulnar Nerve during Cycling. Clin. Biomech. 2011, 26, 642–648. [Google Scholar] [CrossRef] [Green Version]
- Spears, I.R.; Cummins, N.K.; Brenchley, Z.; Donohue, C.; Turnbull, C.; Burton, S.; Macho, G.A. The Effect of Saddle Design on Stresses in the Perineum during Cycling. Med. Sci. Sports Exerc. 2003, 35, 1620–1625. [Google Scholar] [CrossRef] [Green Version]
- Giacomozzi, C.; Caselli, A.; Macellari, V.; Giurato, L.; Lardieri, L.; Uccioli, L. Walking Strategy in Diabetic Patients With Peripheral Neuropathy. Diabetes Care 2002, 25, 1451–1457. [Google Scholar] [CrossRef] [Green Version]
- Ciniglio, A.; Guiotto, A.; Spolaor, F.; Sawacha, Z. The Design and Simulation of a 16-Sensors Plantar Pressure Insole Layout for Different Applications: From Sports to Clinics, a Pilot Study. Sensors 2021, 21, 1450. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VARIABLE | NAME OF THE VARIABLE | SADDLE ZONE | DEFINTION | CONDITION |
|---|---|---|---|---|
| average pressure | average pressure_noE and average pressure_E | WS, AS and PS | the average over all the time steps | without and with Equistasi® |
| peak pressure | peak pressure_noE and peak pressure_E | WS, AS and PS | the maximum pressure averaged over all the time steps | without and with Equistasi® |
| contact surface | surface_noE and surface_E | WS, AS and PS | sum of the sensors on, averaged over all the time steps | without and with Equistasi® |
| average force | force_noE and force_E | WS, AS and PS | “sensor pressure x sensor surface” and averaged over all the time steps | without and with Equistasi® |
| force in peak of pressure frame | force in peak_noE and force in peak_E | WS, AS and PS | force value corresponding to the frame of peak of pressure value | without and with Equistasi® |
| contact surface in peak of pressure frame | surface in peak_noE and surface in peak_E | WS, AS and PS | contact surface value in the frame of peak of pressure value | without and with Equistasi® |
| pressure-time-integral | pressure-time-integral_noE and pressure-time-integral_E | WS | area under the pressure-time curve over the entire acquisition, and normalized on the duration of the complete acquisition | without and with Equistasi® |
| contact surface in percentage | percentage surface_noE and percentage surface_E | WS | average of the contact surface in percentage of the total sensorized surface | without and with Equistasi® |
| ratio between AS and PS pressure | pressure ratio_noE and pressure ratio_E | WS | ratio between the average pressure on the AS and PS part of the saddle | without and with Equistasi® |
| antero-posterior position of the peak of pressure | peak position_noE and peak position_E | WS | position of the peak of pressure in the anterior-posterior direction, average over all the time steps | without and with Equistasi® |
| antero-posterior position of the COP | COP_noE and COP_E | WS | position of the COP in the anterior-posterior direction, average over all the time steps | without and with Equistasi® |
| WS | TH vs. LH | TH vs. DH | LH vs. DH | |||
|---|---|---|---|---|---|---|
| noE | E | noE | E | noE | E | |
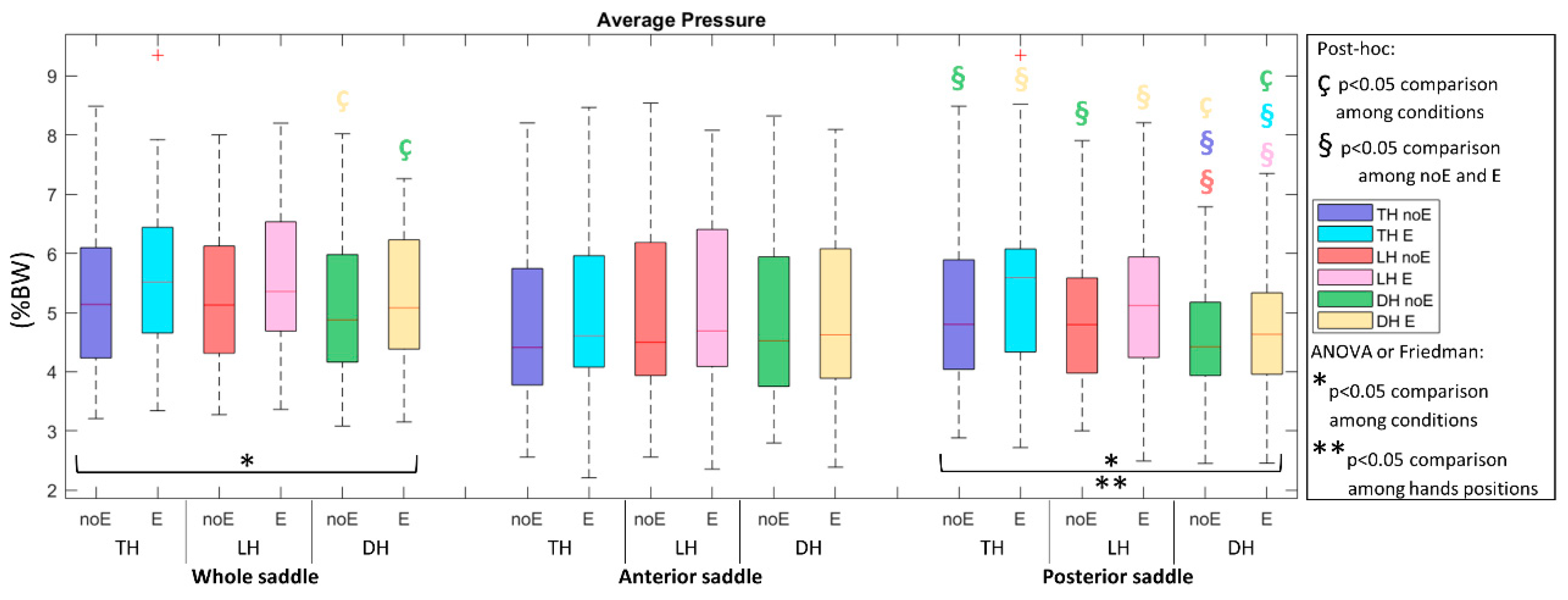
| average pressure | n.s. | n.s. | n.s. | n.s. | n.s. | n.s. |
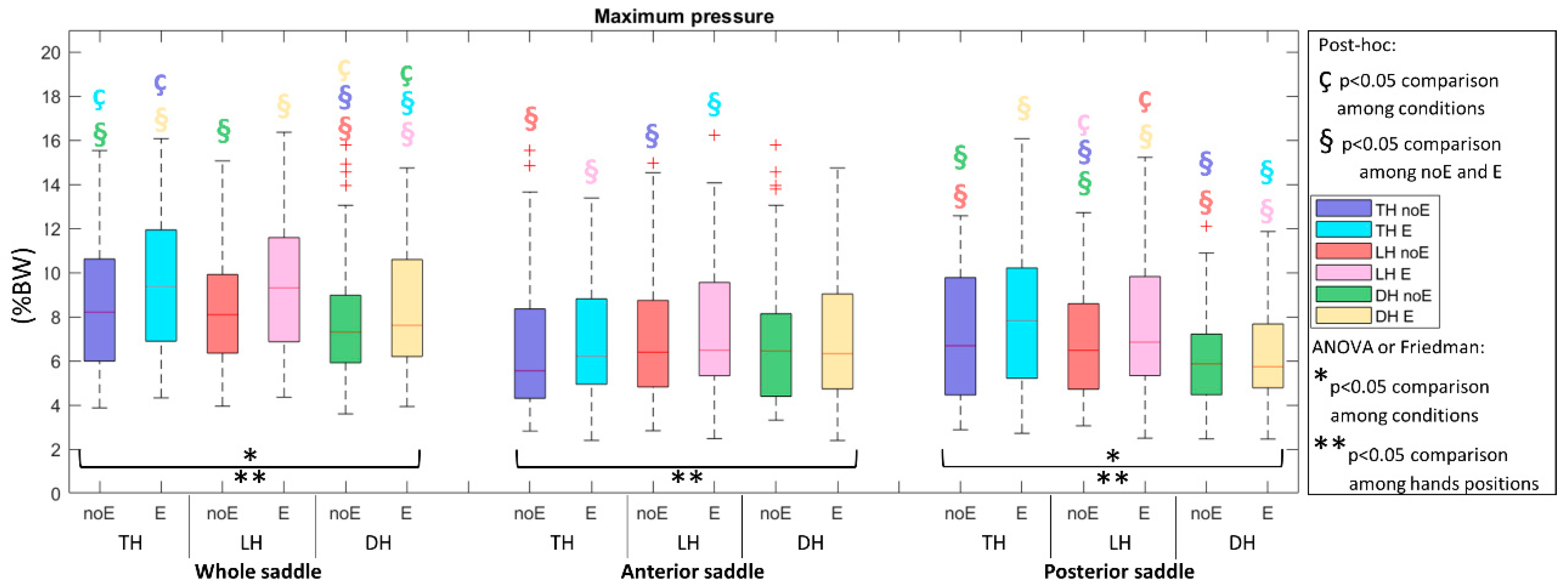
| peak of pressure | n.s. | n.s. | lower in DH (0.003) | lower in DH (<0.001) | lower in DH (0.001) | lower in DH (<0.001) |
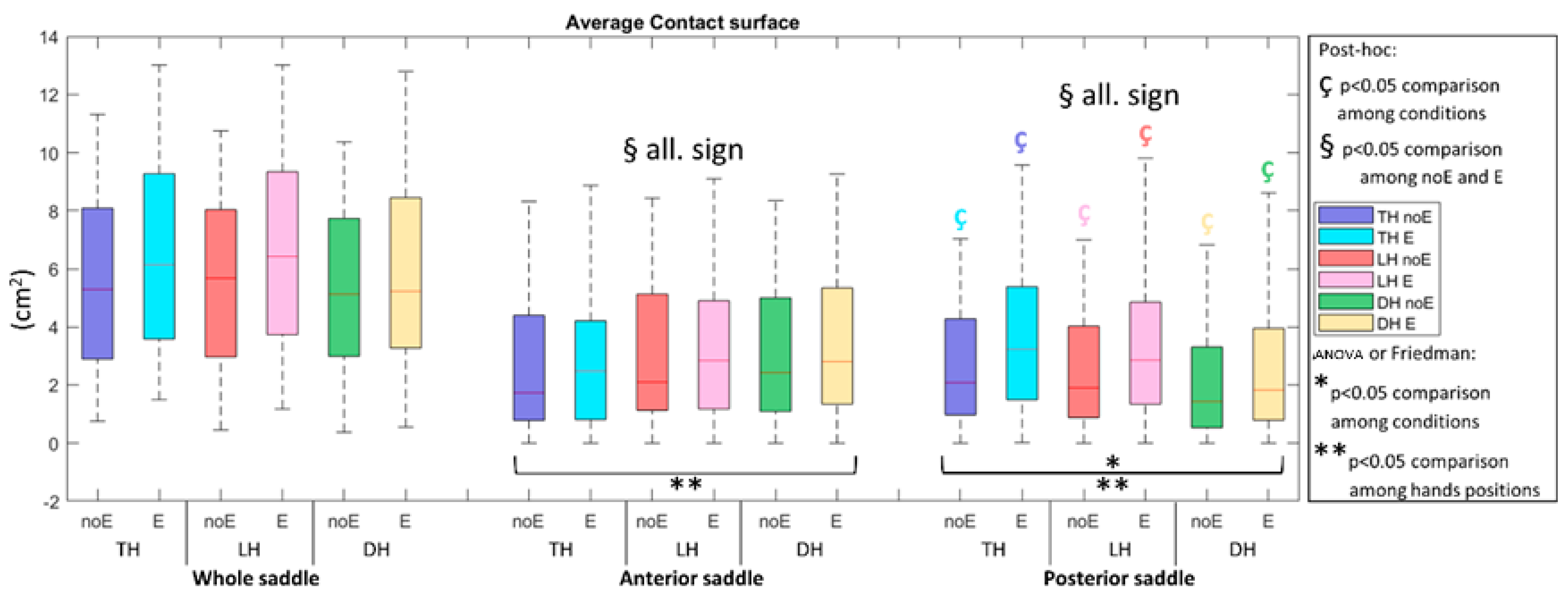
| contact surface | n.s. | n.s. | n.s. | n.s. | n.s. | n.s. |
| average force | n.s. | n.s. | n.s. | n.s. | n.s. | n.s. |
| Pressure-time-integral | n.s. | n.s. | lower in DH (<0.001) | lower in DH (<0.001) | lower in DH (<0.001) | n.s. |
| contact surface % | n.s. | n.s. | n.s. | higher in DH (0.014) | n.s. | n.s. |
| pressure ratio | n.s. | n.s. | n.s. | higher in DH (0.014) | n.s. | n.s. |
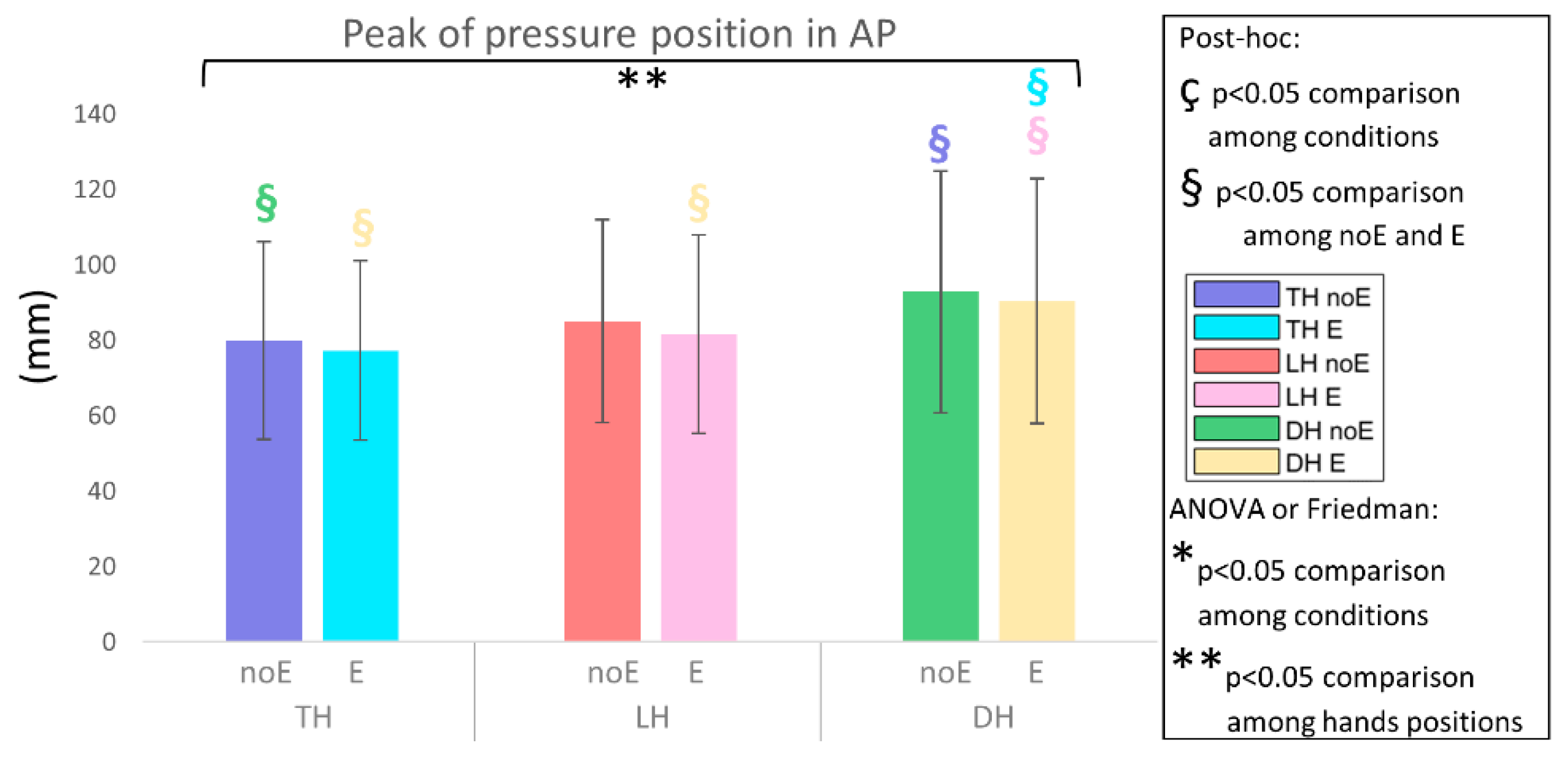
| peak position | n.s. | n.s. | anteriorized in DH (0.011) | anteriorized in DH (0.009) | n.s. | n.s. |
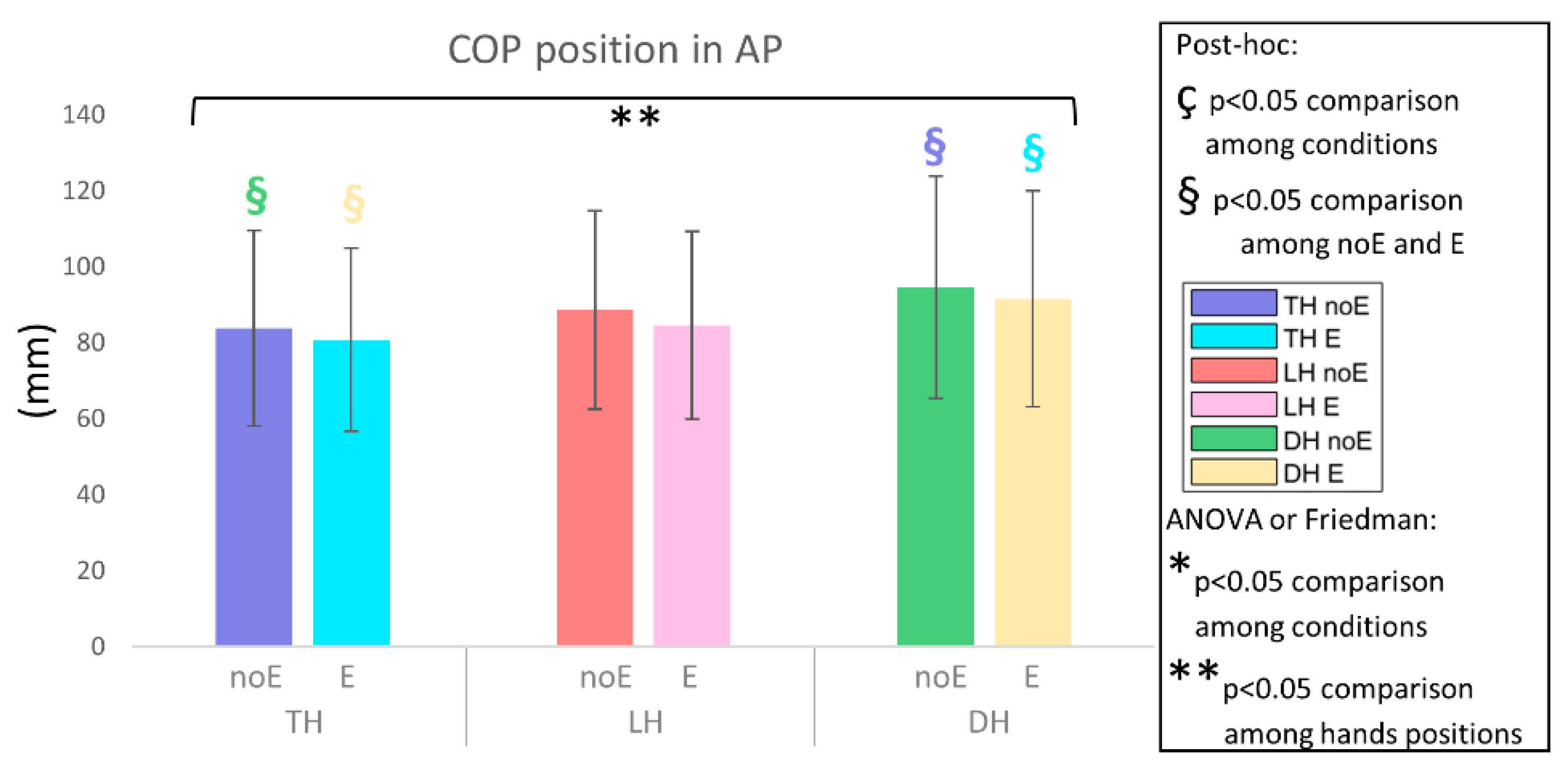
| COP position | n.s. | n.s. | anteriorized in DH (0.026) | anteriorized in DH (0.019) | n.s. | n.s. |
| AS | THvs. LH | THvs. DH | LHvs. DH | |||
| noE | E | noE | noE | E | ||
| average pressure | higher in LH (<0.001) | higher in LH (0.005) | n.s. | n.s. | n.s. | n.s. |
| peak of pressure | higher in LH (<0.001) | higher in LH (0.002) | n.s. | n.s. | n.s. | n.s. |
| contact surface | higher in LH (<0.001) | higher in LH (<0.001) | higher in DH (<0.001) | higher in DH (<0.001) | higher in DH (0.018) | higher in DH (0.025) |
| average force | higher in LH (<0.001) | n.s. | higher in DH (<0.001) | higher in DH (<0.001) | n.s. | n.s. |
| PS | THvs. LH | THvs. DH | LHvs. DH | |||
| noE | E | noE | noE | E | ||
| average pressure | n.s. | n.s. | lower in DH (<0.001) | lower in DH (0.002) | lower in DH (<0.001) | lower in DH (0.023) |
| peak of pressure | lower in LH (0.029) | n.s. | lower in DH (0.021) | lower in DH (0.001) | lower in DH (<0.001) | lower in DH (0.019) |
| contact surface | lower in LH (0.003) | n.s. | lower in DH (<0.001) | lower in DH (<0.001) | lower in DH (<0.001) | lower in DH (<0.001) |
| average force | lower in LH (0.002) | lower in LH (0.002) | lower in DH (<0.001) | lower in DH (<0.001) | lower in DH (<0.001) | lower in DH (<0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guiotto, A.; Spolaor, F.; Albani, G.; Sawacha, Z. Could Proprioceptive Stimuli Change Saddle Pressure on Male Cyclists during Different Hand Positions? An Exploratory Study of the Effect of the Equistasi® Device. Sports 2022, 10, 88. https://doi.org/10.3390/sports10060088
Guiotto A, Spolaor F, Albani G, Sawacha Z. Could Proprioceptive Stimuli Change Saddle Pressure on Male Cyclists during Different Hand Positions? An Exploratory Study of the Effect of the Equistasi® Device. Sports. 2022; 10(6):88. https://doi.org/10.3390/sports10060088
Chicago/Turabian StyleGuiotto, Annamaria, Fabiola Spolaor, Giovanni Albani, and Zimi Sawacha. 2022. "Could Proprioceptive Stimuli Change Saddle Pressure on Male Cyclists during Different Hand Positions? An Exploratory Study of the Effect of the Equistasi® Device" Sports 10, no. 6: 88. https://doi.org/10.3390/sports10060088
APA StyleGuiotto, A., Spolaor, F., Albani, G., & Sawacha, Z. (2022). Could Proprioceptive Stimuli Change Saddle Pressure on Male Cyclists during Different Hand Positions? An Exploratory Study of the Effect of the Equistasi® Device. Sports, 10(6), 88. https://doi.org/10.3390/sports10060088