
Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Procedures
2.2. Obtained Samples
2.3. Measures
2.3.1. Cardiorespiratory Physiology
2.3.2. Sleep
2.3.3. External Training Load
2.4. Statistical Analyses
2.4.1. Intra-Night Relationships
2.4.2. External Training Load
3. Results
3.1. Intra-Night Relationships
3.2. Training Load
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Humphreys, B.; Ruseski, J. The Size and Scope of the Sports Industry in the United States. In Proceedings of the 10th Annual International Association of Sports Economists Conference, Gijón, Spain, 29–31 August 2008. [Google Scholar]
- Dos Santos, M.L.; Uftring, M.; Stahl, C.A.; Lockie, R.G.; Alvar, B.; Mann, J.B.; Dawes, J.J. Stress in Academic and Athletic Performance in Collegiate Athletes: A Narrative Review of Sources and Monitoring Strategies. Front. Sports Act. Living 2020, 2, 42. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, F.; Neshasteh-Riz, A.; Ghadaksaz, A.; Fazeli, S.M.; Janzadeh, A.; Hamblin, M.R. Mechanistic Aspects of Photobiomodulation Therapy in the Nervous System. Lasers Med. Sci. 2021, 37, 11–18. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 348–364. [Google Scholar] [CrossRef] [Green Version]
- Dompe, C.; Moncrieff, L.; Matys, J.; Grzech-Leśniak, K.; Kocherova, I.; Bryja, A.; Bruska, M.; Dominiak, M.; Mozdziak, P.; Skiba, T.H.I.; et al. Photobiomodulation—Underlying Mechanism and Clinical Applications. J. Clin. Med. 2020, 9, 1724. [Google Scholar] [CrossRef] [PubMed]
- Sommer, A.P. Mitochondrial Cytochrome C Oxidase is Not the Primary Acceptor for Near Infrared Light—It is Mitochondrial Bound Water: The Principles of Low-Level Light Therapy. Ann. Transl. Med. 2019, 7, S13. [Google Scholar] [CrossRef]
- Hamblin, M.R. Mechanisms and Applications of the Anti-Inflammatory Effects of Photobiomodulation. AIMS Biophys. 2017, 4, 337–361. [Google Scholar] [CrossRef]
- Glass, G.E. Photobiomodulation: A Review of the Molecular Evidence for Low Level Light Therapy. J. Plast. Reconstr. Aesthet Surg. 2021, 74, 1050–1060. [Google Scholar] [CrossRef]
- Hamblin, M.R. Photobiomodulation for Alzheimer’s Disease: Has the Light Dawned? Photonics 2019, 6, 77. [Google Scholar] [CrossRef] [Green Version]
- Ravera, S.; Colombo, E.; Pasquale, C.; Benedicenti, S.; Solimei, L.; Signore, A.; Amaroli, A. Mitochondrial Bioenergetic, Photobiomodulation and Trigeminal Branches Nerve Damage, What’s the Connection? A Review. Int. J. Mol. Sci. 2021, 22, 4347. [Google Scholar] [CrossRef]
- Dos Santos, S.A.; Serra, A.J.; Stancker, T.G.; Simões, M.C.B.; Vieira, M.A.D.S.; Leal-Junior, E.C.; Prokic, M.; Vasconsuelo, A.; Santos, S.S.; Carvalho, P.D.T.C.D. Effects of Photobiomodulation Therapy on Oxidative Stress in Muscle Injury Animal Models: A Systematic Review. Oxidative Med. Cell. Longev. 2017, 2017, 5273403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toma, R.L.; Oliveira, M.X.; Renno, A.C.M.; Laakso, E.-L. Photobiomodulation (PBM) Therapy at 904 nm Mitigates Effects of Exercise-Induced Skeletal Muscle Fatigue in Young Women. Lasers Med. Sci. 2018, 33, 1197–1205. [Google Scholar] [CrossRef] [PubMed]
- Pinto, H.D.; Vanin, A.A.; Miranda, E.; Tomazoni, S.S.; Johnson, D.S.; Albuquerque-Pontes, G.M.; Aleixo, I.D.O.; Grandinetti, V.D.S.; Casalechi, H.L.; Carvalho, P.D.T.D.; et al. Photobiomodulation Therapy Improves Performance and Accelerates Recovery of High-Level Rugby Players in Field Test: A Randomized, Crossover, Double-Blind, Placebo-Controlled Clinical Study. J. Strength Cond. Res. 2016, 30, 3329–3338. [Google Scholar] [CrossRef] [PubMed]
- Miranda, E.F.; Vanin, A.A.; Tomazoni, S.S.; Grandinetti, V.d.S.; de Paiva, P.R.V.; Machado, C.d.S.M.; Monteiro, K.K.D.S.; Casalechi, H.L.; de Carvalho, P.d.T.C.; Leal-Junior, E.C.P. Using Pre-Exercise Photobiomodulation Therapy Combining Super-Pulsed Lasers and Light-Emitting Diodes to Improve Performance in Progressive Cardiopulmonary Exercise Tests. J. Athl. Train. 2016, 51, 129–135. [Google Scholar] [CrossRef] [Green Version]
- Dellagrana, R.A.; Rossato, M.; Sakugawa, R.L.; Lazzari, C.D.; Baroni, B.M.; Diefenthaeler, F. Dose-Response Effect of Photobiomodulation Therapy on Neuromuscular Economy during Submaximal Running. Lasers Med. Sci. 2018, 33, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Ferraresi, C.; Huang, Y.-Y.; Hamblin, M.R. Photobiomodulation in Human Muscle Tissue: An Advantage in Sports Performance? J. Biophotonics 2016, 9, 1273–1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Marchi, T.; Leal-Junior, E.C.P.; Lando, K.C.; Cimadon, F.; Vanin, A.A.; Pase da Rosa, D.; Salvador, M. Photobiomodulation Therapy Before Futsal Matches Improves the Staying Time of Athletes in the Court and Accelerates Post-Exercise Recovery. Lasers Med. Sci. 2019, 34, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Malta, E.d.S.; de Lira, F.S.; Machado, F.A.; Zago, A.S.; Amaral, S.L.d.; Zagatto, A.M. Photobiomodulation by LED Does Not Alter Muscle Recovery Indicators and Presents Similar Outcomes to Cold-Water Immersion and Active Recovery. Front. Physiol. 2019, 9, 1948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zagatto, A.M.; Dutra, Y.M.; Santos Lira, F.; Antunes, B.M.; Faustini, J.B.; Malta, E.d.S.; Lopes, V.H.F.; de Poli, R.A.B.; Brisola, G.M.P.; dos Santos, G.V.; et al. Full Body Photobiomodulation Therapy to Induce Faster Muscle Recovery in Water Polo Athletes: Preliminary Results. Photobiomodul. Photomed. Laser Surg. 2020, 38, 766–772. [Google Scholar] [CrossRef]
- Heiskanen, V.; Hamblin, M.R. Photobiomodulation: Lasers vs. light emitting diodes? Photochem. Photobiol. Sci. 2018, 17, 1003–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, A.C.; Fernandes, G.A.; Gonzaga, I.C.; de Barros Araujo, R.; de Oliveira, R.A.; Nicolau, R.A. Low-Level Laser and Light-Emitting Diode Therapy for Pain Control in Hyperglycemic and Normoglycemic Patients Who Underwent Coronary Bypass Surgery with Internal Mammary Artery Grafts: A Randomized, Double-Blind Study with Follow-Up. Photomed. Laser Surg. 2016, 34, 244–251. [Google Scholar] [CrossRef]
- Ammar, T.A. Monochromatic Infrared Photo Energy versus Low Level Laser Therapy in Patients with Knee Osteoarthritis. J. Lasers Med. Sci. 2014, 5, 176–182. [Google Scholar] [PubMed]
- Leal, E.C.P.; Lopes-Martins, R.A.B.; Baroni, B.M.; De Marchi, T.; Rossi, R.P.; Grosselli, D.; Generosi, R.A.; de Godoi, V.; Basso, M.; Mancalossi, J.L.; et al. Comparison Between Single-Diode Low-Level Laser Therapy (LLLT) and LED Multi-Diode (Cluster) Therapy (LEDT) Applications Before High-Intensity Exercise. Photomed. Laser Surg. 2009, 27, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Esper, M.A.L.R.; Nicolau, R.A.; Arisawa, E.A.L. The effect of two phototherapy protocols on pain control in orthodontic procedure-a preliminary clinical study. Lasers Med. Sci. 2011, 26, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Freitas, A.C.C.; Campos, L.; Brandao, T.B.; Cristofaro, M.; Eduardo, F.D.; Luiz, A.C.; Marques, M.M.; Eduardo, C.D.; Simoes, A. Chemotherapy-Induced Oral Mucositis: Effect of LED and Laser Phototherapy Treatment Protocols. Photomed. Laser Surg. 2014, 32, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Dellagrana, R.A.; Rossato, M.; Sakugawa, R.L.; Baroni, B.M.; Diefenthaeler, F. Photobiomodulation Therapy on Physiological and Performance Parameters During Running Tests: Dose–Response Effects. J. Strength Cond. Res. 2018, 32, 2807–2815. [Google Scholar] [CrossRef] [PubMed]
- Rossato, M.; Dellagrana, R.A.; Sakugawa, R.L.; Baroni, B.M.; Diefenthaeler, F. Dose–Response Effect of Photobiomodulation Therapy on Muscle Performance and Fatigue During a Multiple-Set Knee Extension Exercise: A Randomized, Crossover, Double-Blind Placebo Controlled Trial. Photobiomodul. Photomed. Laser Surg. 2020, 38, 758–765. [Google Scholar] [CrossRef]
- Tuner, J. Photobiomodulation: How Many Sessions and How Often? Photomed. Laser Surg. 2018, 36, 59–60. [Google Scholar] [CrossRef] [PubMed]
- Dutra, Y.M.; Claus, G.M.; Malta, E.d.S.; Brisola, G.M.P.; Esco, M.R.; Ferraresi, C.; Zagatto, A.M. Acute Photobiomodulation by LED Does Not Alter Muscle Fatigue and Cycling Performance. Med. Sci. Sports Exerc. 2020, 52, 2448–2458. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Tian, Y.; Nie, J.; Xu, J.; Liu, D. Red Light and the Sleep Quality and Endurance Performance of Chinese Female Basketball Players. J. Athl. Train. 2012, 47, 673–678. [Google Scholar] [CrossRef] [Green Version]
- Rossato, M.; Dellagrana, R.A.; Sakugawa, R.L.; Lazzari, C.D.; Baroni, B.M.; Diefenthaeler, F. Time Response of Photobiomodulation Therapy on Muscular Fatigue in Humans. J. Strength Cond. Res. 2018, 32, 3285–3293. [Google Scholar] [CrossRef]
- Ghigiarelli, J.J.; Fulop, A.M.; Burke, A.A.; Ferrara, A.J.; Sell, K.M.; Gonzalez, A.M.; Pelton, L.M.; Zimmerman, J.A.; Coke, S.G.; Marshall, D.G. The Effects of Whole-Body Photobiomodulation Light-Bed Therapy on Creatine Kinase and Salivary Interleukin-6 in a Sample of Trained Males: A Randomized, Crossover Study. Front. Sports Act. Living 2020, 2, 48. [Google Scholar] [CrossRef] [PubMed]
- Kiviniemi, A.M.; Hautala, A.J.; Kinnunen, H.; Tulppo, M.P. Endurance Training Guided Individually by Daily Heart Rate Variability Measurements. Eur. J. Appl. Physiol. 2007, 101, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M. Monitoring Training Status with HR Measures: Do All Roads Lead to Rome? Front. Physiol. 2014, 5, 73. [Google Scholar] [CrossRef] [Green Version]
- Al Haddad, H.; Laursen, P.B.; Chollet, D.; Ahmaidi, S.; Buchheit, M. Reliability of Resting and Postexercise Heart Rate Measures. Int. J. Sports Med. 2011, 32, 598–605. [Google Scholar] [CrossRef]
- Eyal, S.; Altman, Y.; Baharav, A. 1010 Sleep Related Recovery in Athletes: The Role of Heart Rate Variability Parameters. Sleep 2019, 42, A406–A407. [Google Scholar] [CrossRef]
- Chokroverty, S.; Cortelli, P. (Eds.) Autonomic Nervous System and Sleep: Order and Disorder; Springer Nature: New York, NY, USA, 2021. [Google Scholar]
- de Zambotti, M.; Trinder, J.; Silvani, A.; Colrain, I.M.; Baker, F.C. Dynamic Coupling Between the Central and Autonomic Nervous Systems During Sleep: A Review. Neurosci. Biobehav. Rev. 2018, 90, 84–103. [Google Scholar] [CrossRef] [PubMed]
- Roche, F.; Gaspoz, J.-M.; Court-Fortune, I.; Minini, P.; Pichot, V.; Duverney, D.; Costes, F.; Lacour, J.-R.; Barthélémy, J.-C. Screening of Obstructive Sleep Apnea Syndrome by Heart Rate Variability Analysis. Circulation 1999, 100, 1411–1415. [Google Scholar] [CrossRef] [PubMed]
- Otzenberger, H.; Gronfier, C.; Simon, C.; Charloux, A.; Ehrhart, J.; Piquard, F.; Brandenberger, G. Dynamic Heart Rate Variability: A Tool for Exploring Sympathovagal Balance Continuously During Sleep in Men. Am. J. Physiol. Heart Circ. Physiol. 1998, 275, H946–H950. [Google Scholar] [CrossRef]
- Waldeck, M.R.; Lambert, M.I. Heart Rate During Sleep: Implications for Monitoring Training Status. J. Sports Sci. Med. 2003, 2, 133–138. [Google Scholar]
- Burton, A.R.; Rahman, K.; Kadota, Y.; Lloyd, A.; Vollmer-Conna, U. Reduced Heart Rate Variability Predicts Poor Sleep Quality in a Case–Control Study of Chronic Fatigue Syndrome. Exp. Brain Res. 2010, 204, 71–78. [Google Scholar] [CrossRef]
- Pichot, V.; Roche, F.; Gaspoz, J.-M.; Enjolras, F.; Antoniadis, A.; Minini, P.; Costes, F.; Busso, T.; Lacour, J.-R.; Barthelemy, J.C. Relation Between Heart Rate Variability and Training Load in Middle-Distance Runners. Med. Sci. Sports Exerc. 2000, 32, 1729–1736. [Google Scholar] [CrossRef] [Green Version]
- Myllymaki, T.; Rusko, H.; Syvaoja, H.; Juuti, T.; Kinnunen, M.-L. Effects of Exercise Intensity and Duration on Nocturnal Heart Rate Variability and Sleep Quality. Eur. J. Appl. Physiol. 2012, 112, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Costa, J.; Figueiredo, P.; Nakamura, F.; Rago, V.; Rebelo, A.; Brito, J. Intra-Individual Variability of Sleep and Nocturnal Cardiac Autonomic Activity in Elite Female Soccer Players During an International Tournament. PLoS ONE 2019, 14, e0218635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, A.M. Sleep and Athletic Performance. Curr. Sports Med. Rep. 2017, 16, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Hainline, B.; Derman, W.; Vernec, A.; Budgett, R.; Deie, M.; Dvorak, J.; Harle, C.; Herring, S.A.; McNamee, M.; Meeuwisse, W.; et al. International Olympic Committee Consensus Statement on Pain Management in Elite Athletes. Br. J. Sports Med. 2017, 51, 1245–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, P.A.; Carroll, J.D. How to report low-level laser therapy (LLLT)/photomedicine dose and beam parameters in clinical and laboratory studies. Photomed. Laser Surg. 2011, 29, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Burgess, H.J.; Holmes, A.L.; Dawson, D. The Relationship Between Slow-wave Activity, Body Temperature, and Cardiac Activity During Nighttime Sleep. Sleep 2001, 24, 343–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandenberger, G.; Buchheit, M.; Ehrhart, J.; Simon, C.; Piquard, F. Is Slow Wave Sleep an Appropriate Recording Condition for Heart Rate Variability Analysis? Auton. Neurosci. 2005, 121, 81–86. [Google Scholar] [CrossRef]
- Costa, J.A.; Figueiredo, P.; Nakamura, F.Y.; Rebelo, A.; Brito, J. Monitoring Individual Sleep and Nocturnal Heart Rate Variability Indices: The Impact of Training and Match Schedule and Load in High-Level Female Soccer Players. Front. Physiol. 2021, 12, 678462. [Google Scholar] [CrossRef] [PubMed]
- Thornton, H.; Delaney, J.A.; Duthie, G.M.; Dascombe, B.J. Effects of Preseason Training on the Sleep Characteristics of Professional Rugby League Players. Int. J. Sports Physiol. Perform. 2018, 13, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Aloulou, A.; Duforez, F.; Bieuzen, F.; Nedelec, M. The Effect of Night-Time Exercise on Sleep Architecture Among Well-Trained Male Endurance Runners. J. Sleep Res. 2020, 29, e12964. [Google Scholar] [CrossRef] [PubMed]
- Taboada, L.D.; Yu, J.; El-Amouri, S.; Gattoni-Celli, S.; Richieri, S.; McCarthy, T.; Streeter, J.; Kindy, M.S. Transcranial Laser Therapy Attenuates Amyloid-β Peptide Neuropathology in Amyloid-β Protein Precursor Transgenic Mice. J. Alzheimers Dis. 2011, 23, 521–535. [Google Scholar] [CrossRef] [PubMed]
- Grillo, S.L.; Duggett, N.A.; Ennaceur, A.; Chazot, P.L. Non-invasive Infra-red Therapy (1072 nm) Reduces b-Amyloid Protein Levels in the Brain of an Alzheimer’s Disease Mouse Model, TASTPM. J. Photochem. Photobiol. 2013, 123, 13–22. [Google Scholar] [CrossRef]
- Salehpour, F.; Majdi, A.; Pazhuhi, M.; Ghasemi, F.; Khademi, M.; Pashazadeh, F.; Hamblin, M.R.; Cassano, P. Transcranial Photobiomodulation Improves Cognitive Performance in Young Healthy Adults: A Systematic Review and Meta-Analysis. Photobiomodul. Photomed. Laser Surg. 2019, 37, 635–643. [Google Scholar] [CrossRef]
- Vanin, A.A.; Verhagen, E.; Barboza, S.D.; Pena Costa, L.O.; Leal-Junior, E.C.P. Photobiomodulation Therapy for the Improvement of Muscular Performance and Reduction of Muscular Fatigue Associated with Exercise in Healthy People: A Systematic Review and Meta-analysis. Lasers Med. Sci. 2018, 33, 181–214. [Google Scholar] [CrossRef]
- Soheilifar, S.; Fathi, H.; Naghdi, N. Photobiomodulation Therapy as a High Potential Treatment Modality for COVID-19. Lasers Med. Sci. 2021, 36, 935–938. [Google Scholar] [CrossRef] [PubMed]
- Rentz, L.E.; Ulman, H.K.; Galster, S.M. Deconstructing Commercial Wearable Technology: Contributions toward Accurate and Free-Living Monitoring of Sleep. Sensors 2021, 21, 5071. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.D.; Rentz, L.E.; Forsey, J.; Ramadan, J.; Markwald, R.R.; Finomore, V.S.; Galster, S.M.; Rezai, A.; Hagen, J.A. Evaluations of Commercial Sleep Technologies for Objective Monitoring During Routine Sleeping Conditions. Nat. Sci. Sleep 2020, 12, 821–842. [Google Scholar] [CrossRef] [PubMed]
- Kinnunen, H.; Rantanen, A.; Kentta, T.; Koskimaki, H. Feasible Assessment of Recovery and Cardiovascular Health: Accuracy of Nocturnal HR and HRV Assessed via Ring PPG in Comparison to Medical Grade ECG. Physiol. Meas. 2020, 41, 04NT01. [Google Scholar] [CrossRef]
- Stone, J.D.; Ulman, H.K.; Tran, K.; Thompson, A.G.; Halter, M.D.; Ramadan, J.H.; Stephenson, M.; Finomore, V.S.; Galster, S.M.; Rezai, A.R.; et al. Assessing the Accuracy of Popular Commercial Technologies That Measure Resting Heart Rate and Heart Rate Variability. Front. Sports Act. Living 2021, 3, 37. [Google Scholar] [CrossRef]
- de Zambotti, M.; Rosas, L.; Colrain, I.M.; Baker, F.C. The Sleep of the Ring: Comparison of the OURA sleep tracker against polysomnography. Behav. Sleep Med. 2019, 17, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Cao, R.; Azimi, I.; Sarhaddi, F.; Niela-Vilen, H.; Axelin, A.; Liljeberg, P.; Rahmani, A.M. Accuracy Assessment of Oura Ring Nocturnal Heart Rate and Heart Rate Variability in Comparison With Electrocardiography in Time and Frequency Domains: Comprehensive Analysis. J. Med. Internet. Res. 2022, 24, e27487. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Visible Red | NIR |
|---|---|---|
| Wavelength | 660 ± 25 nm | 850 ± 30 nm |
| LED Quantity | 1200 | 1200 |
| Power per LED | 0.267 W | 0.267 W |
| Irradiance (at patient skin) | 0.012 W/cm2 | 0.012 W/cm2 |
| Total Emitted Power | 321 W | 321 W |
| Treatment Time | 1200 s | 1200 s |
| Energy Emitted | 385,056 J | 385,056 J |
| Fluence | 14.4 J/cm2 | 14.4 J/cm2 |
| Variable | Pre | Post | Mean Difference | p-Value | d | |
|---|---|---|---|---|---|---|
| Physiology | Average HR (bpm) | 54.31 | 53.31 | 0.996 (0.300, 1.691) | 0.0055 * | 0.175 |
| Average HRV (ms) | 100.46 | 103.73 | −3.269 (−6.899, 0.362) | 0.0770 | 0.251 | |
| Average RR (rpm) | 16.85 | 16.80 | 0.058 (−0.094, 0.210) | 0.4504 | 0.022 | |
| Sleep | Total Sleep Time (h) | 7.93 | 7.29 | 0.635 (0.282, 0.989) | 0.0006 * | 0.156 |
| Awake Time (h) | 1.35 | 1.28 | 0.070 (−0.061, 0.200) | 0.2935 | 0.028 | |
| Sleep Efficiency (%) | 85.65 | 85.13 | 0.516 (−0.602, 1.634) | 0.3616 | 0.071 | |
| Light Duration (h) | 4.62 | 4.30 | 0.322 (0.031, 0.613) | 0.0307 * | 0.087 | |
| Deep Duration (h) | 2.24 | 2.12 | 0.114 (−0.030, 0.258) | 0.1188 | 0.044 | |
| REM Duration (h) | 1.07 | 0.87 | 0.200 (0.075, 0.324) | 0.0019 * | 0.083 | |
| % Light | 57.84 | 58.70 | −0.862 (−3.178, 1.453) | 0.4614 | 0.083 | |
| % Deep | 28.97 | 29.90 | −0.933 (−3.109, 1.243) | 0.3966 | 0.092 | |
| % REM | 13.21 | 11.41 | 1.798 (0.41, 3.185) | 0.0117 * | 0.223 |
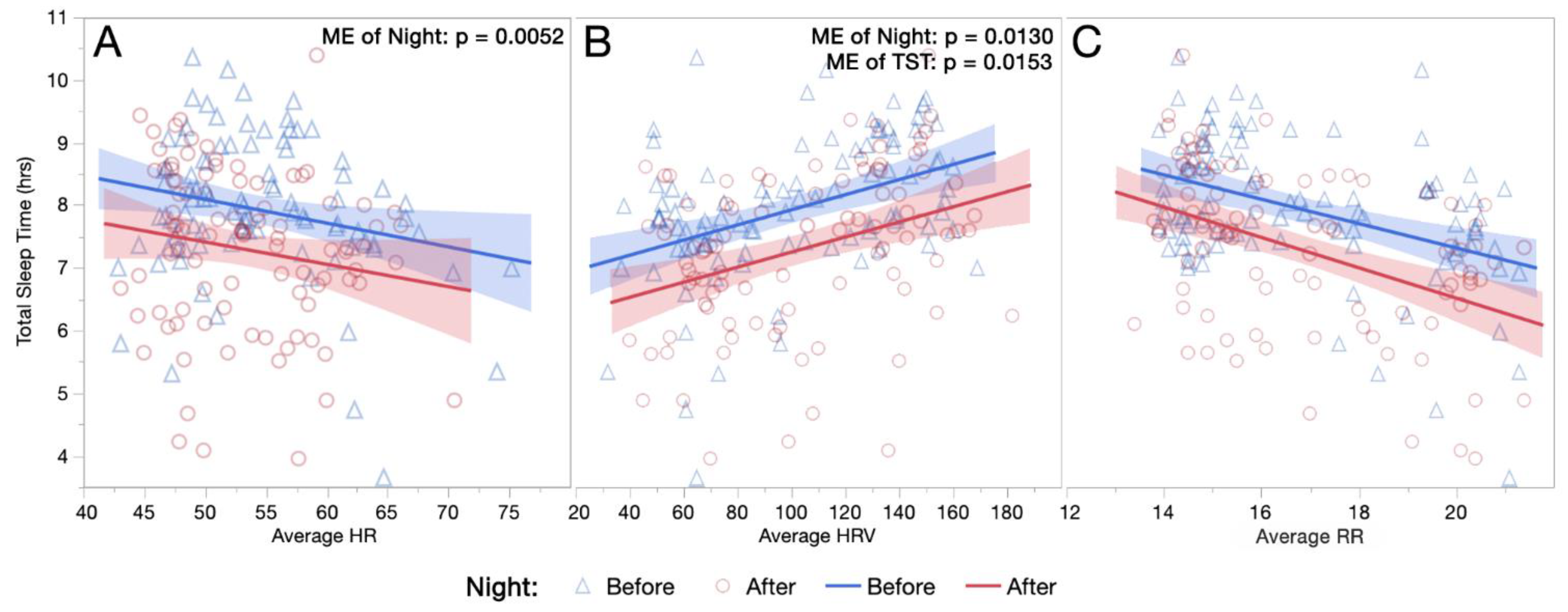
| Outcome Measure | Fixed Effect | F | df | p-Value |
|---|---|---|---|---|
| Average HR | Night | 8.18 | 1, 90.7 | 0.0052 * |
| TST | 0.41 | 1, 102.4 | 0.5254 | |
| Night*TST | 0.59 | 1, 102.7 | 0.4451 | |
| Average HRV | Night | 6.43 | 1, 89.0 | 0.0130 * |
| TST | 6.09 | 1, 98.5 | 0.0153 * | |
| Night*TST | 3.05 | 1, 98.8 | 0.0839 | |
| Average RR | Night | 1.05 | 1, 88.9 | 0.3090 |
| TST | 0.86 | 1, 93.0 | 0.3552 | |
| Night*TST | 0.01 | 1, 93.1 | 0.9051 |
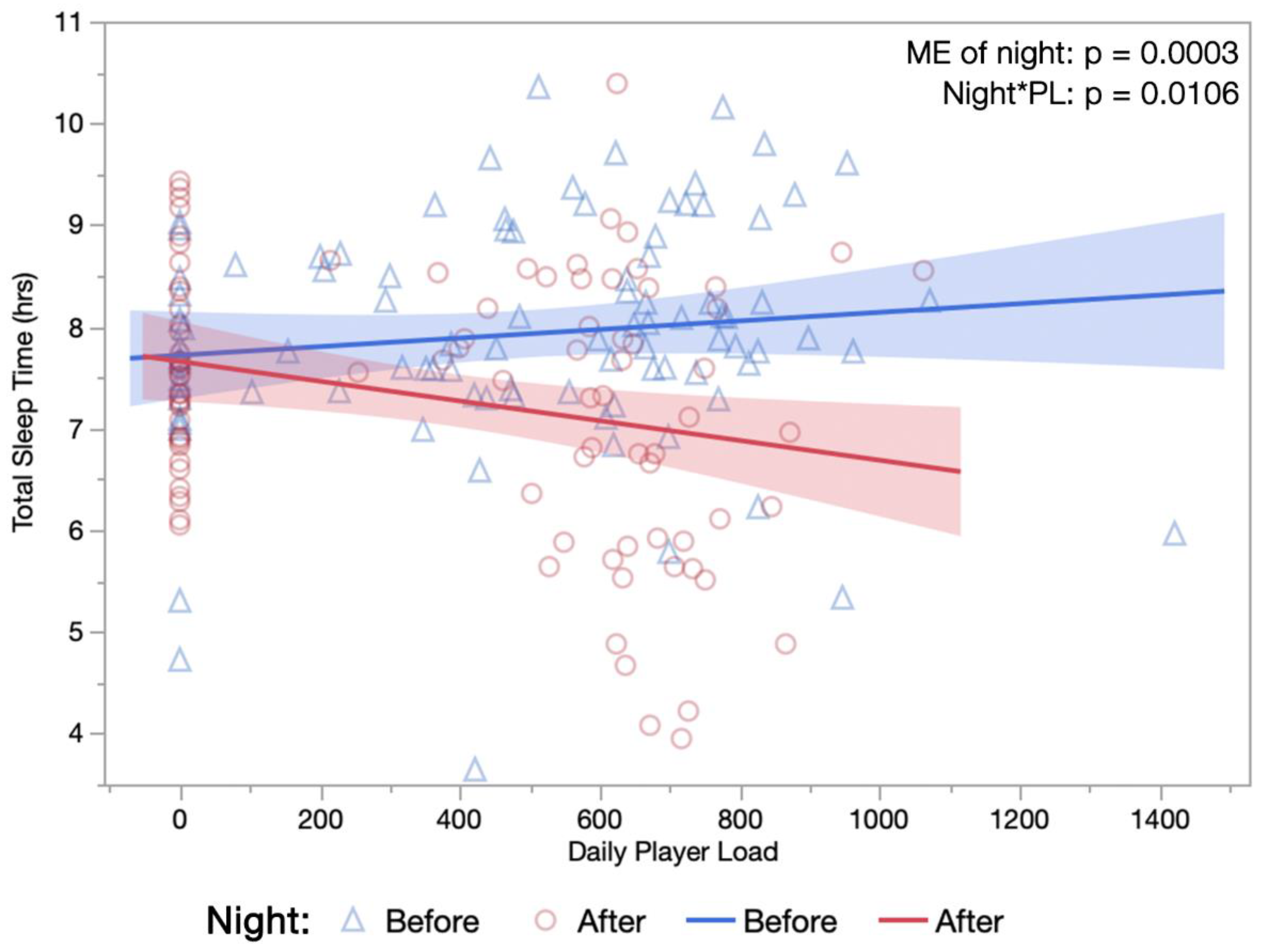
| Single-Day PL | 4D Cumulative PL | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Night | PL | Night*PL | Night | PL | Night*PL | |
| Physiology | Average HR (bpm) | 0.0643 | <0.0001 * | 0.0761 | 0.0089 * | 0.0132 * | 0.6472 |
| Average HRV (ms) | 0.1598 | 0.1793 | 0.1916 | 0.0912 | 0.5113 | 0.6187 | |
| Average RR (rpm) | 0.8956 | 0.0004 * | 0.0549 | 0.6076 | 0.0140 * | 0.6390 | |
| Sleep | Total Sleep Time (h) | 0.0003 * | 0.3309 | 0.0106 * | 0.0005 * | 0.1993 | 0.8867 |
| Awake Time (h) | 0.2438 | 0.4530 | 0.9029 | 0.2798 | 0.4659 | 0.9330 | |
| Sleep Efficiency (%) | 0.4060 | 0.7732 | 0.2514 | 0.3742 | 0.8003 | 0.8906 | |
| Light Duration (h) | 0.0299 * | 0.8949 | 0.0401 * | 0.0301 * | 0.7022 | 0.7982 | |
| Deep Duration (h) | 0.0881 | 0.3869 | 0.1862 | 0.1087 | 0.3192 | 0.5547 | |
| REM Duration (h) | 0.0016 * | 0.6175 | 0.2155 | 0.0018 * | 0.3259 | 0.7460 | |
| % Light | 0.4304 | 0.7136 | 0.9402 | 0.4461 | 0.5736 | 0.4394 | |
| % Deep | 0.4016 | 0.9552 | 0.4968 | 0.3929 | 0.8361 | 0.7182 | |
| % REM | 0.0098 * | 0.6314 | 0.2001 | 0.010 5 * | 0.3244 | 0.4464 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rentz, L.E.; Bryner, R.W.; Ramadan, J.; Rezai, A.; Galster, S.M. Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery. Sports 2022, 10, 119. https://doi.org/10.3390/sports10080119
Rentz LE, Bryner RW, Ramadan J, Rezai A, Galster SM. Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery. Sports. 2022; 10(8):119. https://doi.org/10.3390/sports10080119
Chicago/Turabian StyleRentz, Lauren E., Randy W. Bryner, Jad Ramadan, Ali Rezai, and Scott M. Galster. 2022. "Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery" Sports 10, no. 8: 119. https://doi.org/10.3390/sports10080119
APA StyleRentz, L. E., Bryner, R. W., Ramadan, J., Rezai, A., & Galster, S. M. (2022). Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery. Sports, 10(8), 119. https://doi.org/10.3390/sports10080119