
From Incremental Test to Continuous Running at Fixed Lactate Thresholds: Individual Responses on %VO2max, %HRmax, Lactate Accumulation, and RPE


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
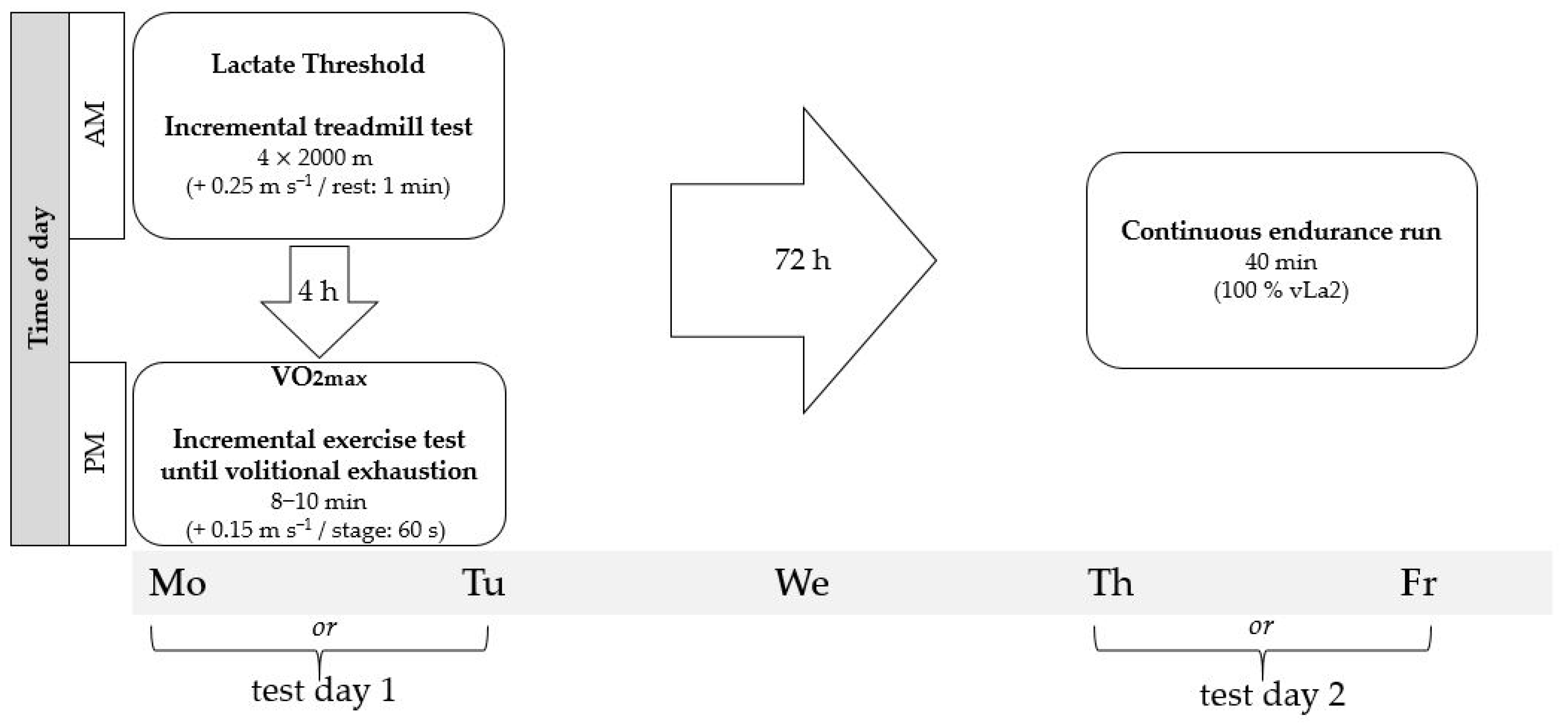
2.2. Protocol and Test Design
2.3. Data Analysis
2.4. Statistics
3. Results
3.1. %VO2max, %HRmax, and RPE at vLa2 during Incremental Test
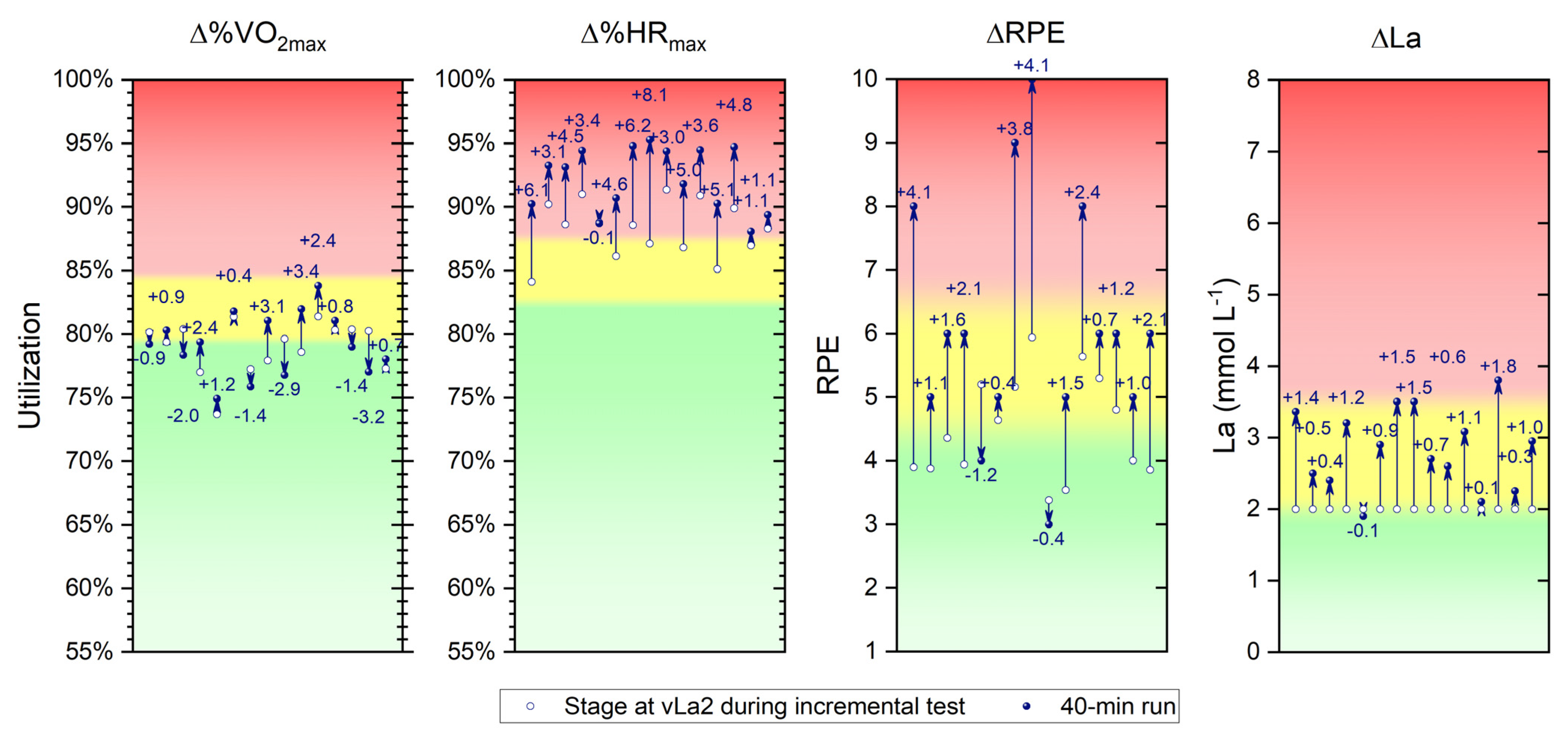
3.2. ∆%VO2max, ∆%HRmax, ∆RPE, and ∆La from Incremental Test to Continous Running
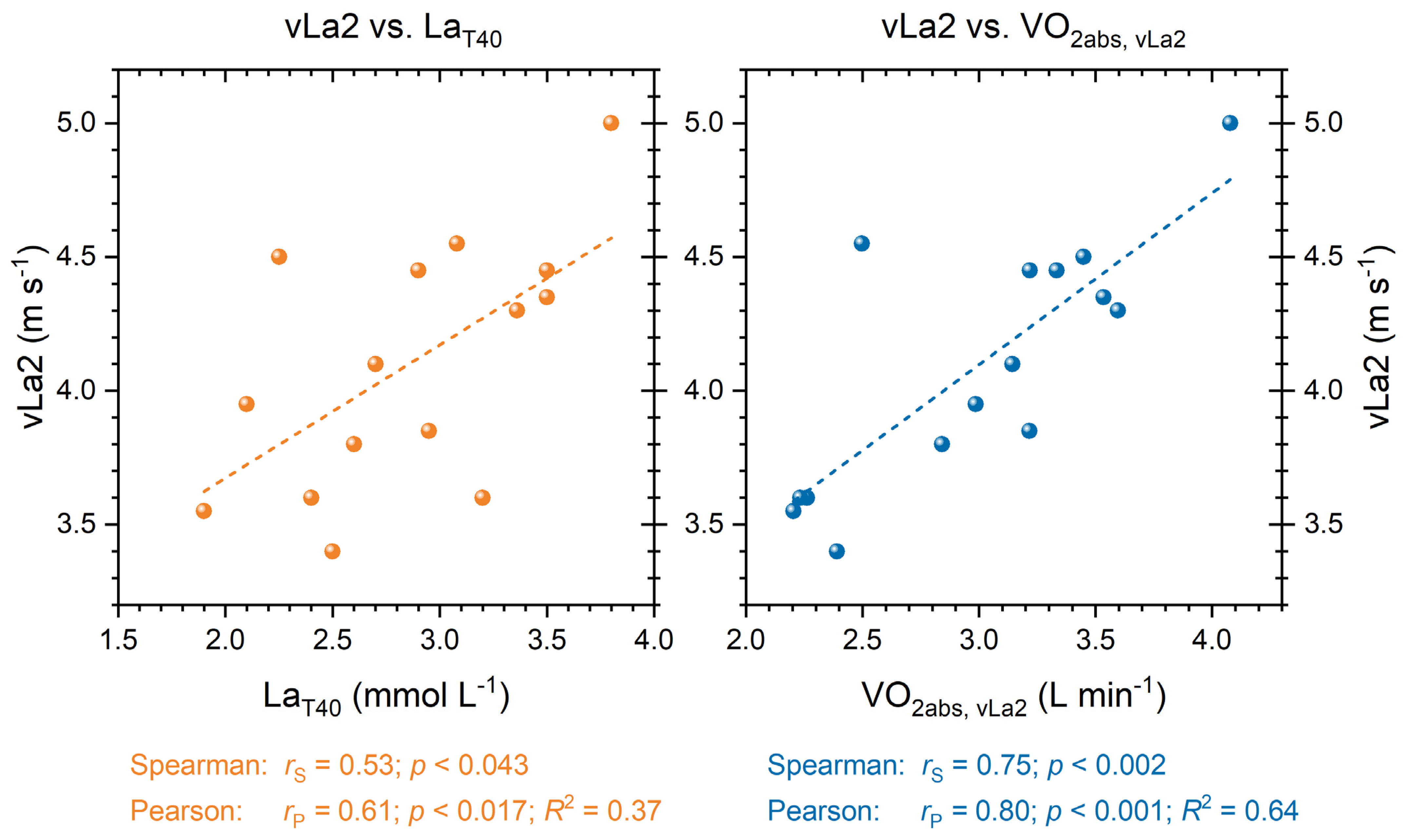
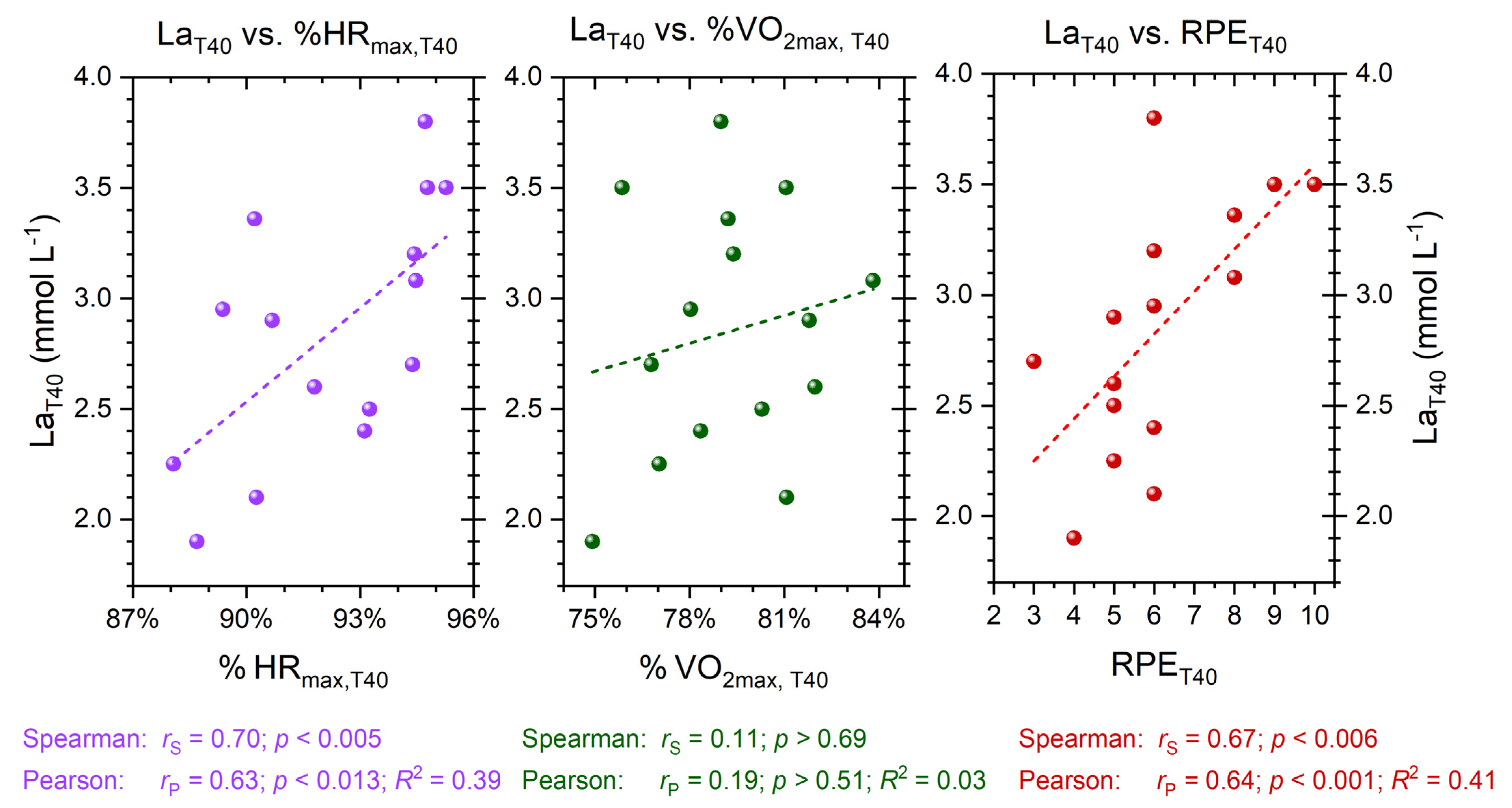
3.3. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Noakes, T.D.; Myburgh, K.H.; Schall, R. Peak treadmill running velocity during the VO2 max test predicts running performance. J. Sports Sci. 1990, 8, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Ingham, S.A.; Whyte, G.P.; Pedlar, C.; Bailey, D.M.; Dunman, N.; Nevill, A.M. Determinants of 800-m and 1500-m Running Performance Using Allometric Models. Med. Sci. Sports Exerc. 2008, 40, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Foster, C. VO2 max and training indices as determinants of competitive running performance. J. Sports Sci. 1983, 1, 13–22. [Google Scholar] [CrossRef]
- Bosquet, L.; Léger, L.; Legros, P. Methods to Determine Aerobic Endurance. Sports Med. 2002, 32, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Conley, D.L.; Krahenbuhl, G.S. Running economy and distance running performance of highly trained athletes. Med. Sci. Sports Exerc. 1980, 12, 357–360. [Google Scholar] [CrossRef]
- Morgan, D.W.; Martin, P.E.; Krahenbuhl, G.S. Factors affecting running economy. Sports Med. 1989, 7, 310–330. [Google Scholar] [CrossRef]
- Foster, C.; Lucia, A. Running Economy: The Forgotten Factor in Elite Performance. Sports Med. 2007, 37, 316–319. [Google Scholar] [CrossRef]
- Billat, L.V. Use of Blood Lactate Measurements for Prediction of Exercise Performance and for Control of Training. Sports Med. 1996, 22, 157–175. [Google Scholar] [CrossRef]
- Weltman, A.; Snead, D.; Seip, R.; Schurrer, R.; Levine, S.; Rutt, R.; Reilly, T.; Weltman, J.; Rogol, A. Prediction of lactate threshold and fixed blood lactate concentrations from 3200-m running performance in male runners. Int. J. Sports Med. 1987, 8, 401–406. [Google Scholar] [CrossRef]
- Roecker, K.; Schotte, O.; Niess, A.M.; Horstmann, T.; Dickhuth, H.H. Predicting competition performance in long-distance running by means of a treadmill test. Med. Sci. Sports Exerc. 1998, 30, 1552–1557. [Google Scholar] [CrossRef]
- Faude, O.; Kindermann, W.; Meyer, T. Lactate Threshold Concepts: How Valid are They? Sports Med. 2009, 39, 469–490. [Google Scholar] [CrossRef] [PubMed]
- Bassett, D.R.; Howley, E.T. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med. Sci. Sports Exerc. 2000, 32, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M.; Kirby, B.S.; Clark, I.E.; Rice, H.M.; Fulkerson, E.; Wylie, L.J.; Wilkerson, D.P.; Vanhatalo, A.; Wilkins, B.W. Physiological demands of running at 2-h marathon race pace. J. Appl. Physiol. 2021, 130, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Konopka, M.J.; Zeegers, M.P.; Solberg, P.A.; Delhaije, L.; Meeusen, R.; Ruigrok, G.; Rietjens, G.; Sperlich, B. Factors associated with high-level endurance performance: An expert consensus derived via the Delphi technique. PLoS ONE 2022, 17, e0279492. [Google Scholar] [CrossRef]
- Halson, S.L. Monitoring training load to understand fatigue in athletes. Sports Med. 2014, 44 (Suppl. 2), 139–147. [Google Scholar] [CrossRef]
- Foster, C.; Rodriguez-Marroyo, J.A.; de Koning, J.J. Monitoring Training Loads: The Past, the Present, and the Future. Int. J. Sports Physiol. Perform. 2017, 12, S2-2–S2-8. [Google Scholar] [CrossRef]
- Roos, L.; Taube, W.; Brandt, M.; Heyer, L.; Wyss, T. Monitoring of daily training load and training load responses in endurance sports: What do coaches want? Schweiz. Z. Fur Sportmed. Und Sport. 2013, 61, 30–36. [Google Scholar]
- Bourdon, P.C.; Cardinale, M.; Murray, A.; Gastin, P.; Kellmann, M.; Varley, M.C.; Gabbett, T.J.; Coutts, A.J.; Burgess, D.J.; Gregson, W.; et al. Monitoring Athlete Training Loads: Consensus Statement. Int. J. Sports Physiol. Perform. 2017, 12, S2-161–S2-170. [Google Scholar] [CrossRef]
- Kaikkonen, P.; Hynynen, E.; Mann, T.; Rusko, H.; Nummela, A. Can HRV be used to evaluate training load in constant load exercises? Eur. J. Appl. Physiol. 2010, 108, 435–442. [Google Scholar] [CrossRef]
- Boullosa, D.; Claudino, J.G.; Fernandez-Fernandez, J.; Bok, D.; Loturco, I.; Stults-Kolehmainen, M.; García-López, J.; Foster, C. The Fine-Tuning Approach for Training Monitoring. Int. J. Sports Physiol. Perform 2023, 1, 1–6. [Google Scholar] [CrossRef]
- Casado, A.; Foster, C.; Bakken, M.; Tjelta, L.I. Does Lactate-Guided Threshold Interval Training within a High-Volume Low-Intensity Approach Represent the “Next Step” in the Evolution of Distance Running Training? Int. J. Environ. Res. Public Health 2023, 20, 3782. [Google Scholar] [PubMed]
- Jamnick, N.A.; Pettitt, R.W.; Granata, C.; Pyne, D.B.; Bishop, D.J. An Examination and Critique of Current Methods to Determine Exercise Intensity. Sports Med. 2020, 50, 1729–1756. [Google Scholar] [CrossRef] [PubMed]
- Foxdal, P.; Sjödin, A.; Sjödin, B. Comparison of blood lactate concentrations obtained during incremental and constant intensity exercise. Int. J. Sports Med. 1996, 17, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Föhrenbach, R.; Mader, A.; Hollmann, W. Determination of endurance capacity and prediction of exercise intensities for training and competition in marathon runners. Int. J. Sports Med. 1987, 8, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Oyono-Enguelle, S.; Heitz, A.; Marbach, J.; Ott, C.; Gartner, M.; Pape, A.; Vollmer, J.C.; Freund, H. Blood lactate during constant-load exercise at aerobic and anaerobic thresholds. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 60, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Borresen, J.; Lambert, M.I. The Quantification of Training Load, the Training Response and the Effect on Performance. Sports Med. 2009, 39, 779–795. [Google Scholar] [CrossRef]
- Yoon, B.K.; Kravitz, L.; Robergs, R. VO2max, protocol duration, and the VO2 plateau. Med. Sci. Sports Exerc. 2007, 39, 1186–1192. [Google Scholar] [CrossRef]
- Hollander, K.; Riebe, D.; Campe, S.; Braumann, K.M.; Zech, A. Effects of footwear on treadmill running biomechanics in preadolescent children. Gait Posture 2014, 40, 381–385. [Google Scholar] [CrossRef]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshal, P.; Dodge, C. A new approach to monitoring exercise training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar]
- Thevenet, D.; Tardieu-Berger, M.; Berthoin, S.; Prioux, J. Influence of recovery mode (passive vs. active) on time spent at maximal oxygen uptake during an intermittent session in young and endurance-trained athletes. Eur. J. Appl. Physiol. 2007, 99, 133–142. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Haugen, T.; Sandbakk, Ø.; Seiler, S.; Tønnessen, E. The Training Characteristics of World-Class Distance Runners: An Integration of Scientific Literature and Results-Proven Practice. Sports Med. Open 2022, 8, 46. [Google Scholar] [CrossRef] [PubMed]
- Seiler, K.S.; Kjerland, G. Quantifying training intensity distribution in elite endurance athletes: Is there evidence for an “optimal” distribution? Scand. J. Med. Sci Sports 2006, 16, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Maunder, E.; Seiler, S.; Mildenhall, M.J.; Kilding, A.E.; Plews, D.J. The Importance of ‘Durability’ in the Physiological Profiling of Endurance Athletes. Sports Med. 2021, 51, 1619–1628. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.A.; Stannard, S.R.; Thompson, M.W. Muscle Triglyceride and Glycogen in Endurance Exercise. Sports Med. 2004, 34, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Bucher Sandbakk, S.; Walther, J.; Solli, G.S.; Tønnessen, E.; Haugen, T. Training Quality—What Is It and How Can We Improve It? Int. J. Sports Physiol. Perform. 2023, 18, 557–560. [Google Scholar] [CrossRef]
- Hofmann, P.; Tschakert, G. Intensity- and Duration-Based Options to Regulate Endurance Training. Front. Physiol. 2017, 8, 337. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure | All (n = 15) Mean ± SD (Min–Max) | Male (n = 10) Mean ± SD (Min–Max) | Female (n = 5) Mean ± SD (Min–Max) |
|---|---|---|---|
| Age (years) | 18.6 ± 3.3 (15–25) | 19.4 ± 3.4 (15–25) | 17.0 ± 2.2 (15–21) |
| Body mass (kg) | 63.6 ± 7.2 (50.2–72.9) | 68.1 ± 2.8 (64.0–72.9) | 54.7 ± 3.5 (50.2–59.5) |
| Body height (cm) | 176.7 ± 8.2 (160–186) | 181.5 ± 3.6 (175–186) | 167.0 ± 4.8 (160–174) |
| VO2max (mL min−1 kg−1) | 59.3 ± 5.9 (50.6–69.6) | 61.8 ± 4.4 (53.1–69.6) | 54.3 ± 4.4 (50.6–59.8) |
| HRmax (beats min−1) | 201 ± 10 (186–222) | 201 ± 8 (186–212) | 202 ± 11 (192–222) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fleckenstein, D.; Seelhöfer, J.; Walter, N.; Ueberschär, O. From Incremental Test to Continuous Running at Fixed Lactate Thresholds: Individual Responses on %VO2max, %HRmax, Lactate Accumulation, and RPE. Sports 2023, 11, 198. https://doi.org/10.3390/sports11100198
Fleckenstein D, Seelhöfer J, Walter N, Ueberschär O. From Incremental Test to Continuous Running at Fixed Lactate Thresholds: Individual Responses on %VO2max, %HRmax, Lactate Accumulation, and RPE. Sports. 2023; 11(10):198. https://doi.org/10.3390/sports11100198
Chicago/Turabian StyleFleckenstein, Daniel, Jannik Seelhöfer, Nico Walter, and Olaf Ueberschär. 2023. "From Incremental Test to Continuous Running at Fixed Lactate Thresholds: Individual Responses on %VO2max, %HRmax, Lactate Accumulation, and RPE" Sports 11, no. 10: 198. https://doi.org/10.3390/sports11100198
APA StyleFleckenstein, D., Seelhöfer, J., Walter, N., & Ueberschär, O. (2023). From Incremental Test to Continuous Running at Fixed Lactate Thresholds: Individual Responses on %VO2max, %HRmax, Lactate Accumulation, and RPE. Sports, 11(10), 198. https://doi.org/10.3390/sports11100198