
Long-Term Resistance–Endurance Combined Training Reduces Pro-Inflammatory Cytokines in Young Adult Females with Obesity

 ,
, 
 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Measurement of Body Composition and Physiological Parameters
2.3. Exercise Protocol and Blood Sampling
2.4. Measurement of Cytokines Pro-Inflammatory
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- González-Muniesa, P.; Mártinez-González, M.A.; Hu, F.B.; Després, J.P.; Matsuzawa, Y.; Loos, R.J.F.; Moreno, L.A.; Bray, G.A.; Martinez, J.A. Obesity. Nat. Rev. Dis. Primers 2017, 3, 17034. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 152, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Kinlen, D.; Cody, D.; O’Shea, D. Complications of obesity. QJM 2018, 111, 437–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basic Health Research (Riskesdas). National Report on Basic Health Research; Ministry of Health Indonesia: Jakarta, Indonesia, 2018.
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Rejeki, P.S.; Pranoto, A.; Prasetya, R.E.; Sugiharto, S. Irisin serum increasing pattern is higher at moderate-intensity continuous exercise than at moderate-intensity interval exercise in obese females. Comp. Exerc. Physiol. 2021, 17, 475–484. [Google Scholar] [CrossRef]
- Seravalle, G.; Grassi, G. Obesity and hypertension. Pharmacol. Res. 2017, 122, 1–7. [Google Scholar] [CrossRef]
- Lauterbach, M.A.; Wunderlich, F.T. Macrophage function in obesity-induced inflammation and insulin resistance. Pflugers Arch. 2017, 469, 385–396. [Google Scholar] [CrossRef] [Green Version]
- Ghaben, A.L.; Scherer, P.E. Adipogenesis and metabolic health. Nat. Rev. Mol. Cell. Biol. 2019, 20, 242–258. [Google Scholar] [CrossRef]
- Akhtari, M.; Zargar, S.J.; Vojdanian, M.; Jamshidi, A.; Mahmoudi, M. Monocyte-derived and M1 macrophages from ankylosing spondylitis patients released higher TNF-α and expressed more IL1B in response to BzATP than macrophages from healthy subjects. Sci. Rep. 2021, 11, 17842. [Google Scholar] [CrossRef]
- Ansari, S.; Haboubi, H.; Haboubi, N. Adult obesity complications: Challenges and clinical impact. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820934955. [Google Scholar] [CrossRef]
- Davarpasand, T.; Mohseni-Badalabadi, R.; Sadeghian, M.; Mortazavi, S.H.; Lalvand, A. Concomitant ventricular septal rupture and interventricular septal aneurysm in neglected inferior myocardial infarction misdiagnosed with congenital ventricular septal defect: A case report. Clin. Case Rep. 2021, 9, e04959. [Google Scholar] [CrossRef]
- Agofure, O. Prevalence of obesity among adults in Issele-Uku, Delta State Nigeria. Alex. J. Med. 2018, 54, 463–468. [Google Scholar] [CrossRef] [Green Version]
- Fan, J.G.; Kim, S.U.; Wong, V.W. New trends on obesity and NAFLD in Asia. J. Hepatol. 2017, 67, 862–873. [Google Scholar] [CrossRef] [Green Version]
- Kern, L.; Mittenbühler, M.J.; Vesting, A.J.; Ostermann, A.L.; Wunderlich, C.M.; Wunderlich, F.T. Obesity-Induced TNFα and IL-6 Signaling: The Missing Link between Obesity and Inflammation-Driven Liver and Colorectal Cancers. Cancers 2018, 11, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, A.M.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522. [Google Scholar] [CrossRef] [PubMed]
- Peeters, A.; Barendregt, J.J.; Willekens, F.; Mackenbach, J.P.; Al Mamun, A.; Bonneux, L.; NEDCOM, the Netherlands Epidemiology and Demography Compression of Morbidity Research Group. Obesity in adulthood and its consequences for life expectancy: A life-table analysis. Ann. Intern. Med. 2003, 138, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013 [published correction appears in Lancet. 2014 Aug 30;384(9945):746]. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández Bautista, R.J.; Mahmoud, A.M.; Königsberg, M.; López Díaz Guerrero, N.E. Obesity: Pathophysiology, monosodium glutamate-induced model and anti-obesity medicinal plants. Biomed. Pharmacother. 2019, 111, 503–516. [Google Scholar] [CrossRef]
- Sugiharto; Merawati, D.; Pranoto, A.; Susanto, H. Physiological response of endurance exercise as a growth hormone mediator in adolescent women’s. J. Basic Clin. Physiol. Pharmacol. 2022, 34, 61–67. [Google Scholar] [CrossRef]
- Andarianto, A.; Rejeki, P.S.; Sakina; Pranoto, A.; Seputra, T.W.A.; Sugiharto; Miftahussurur, M. Inflammatory markers in response to interval and continuous exercise in obese women. Comp. Exerc. Physiol. 2022, 18, 135–142. [Google Scholar] [CrossRef]
- Pedersen, B.K. Anti-inflammatory effects of exercise: Role in diabetes and cardiovascular disease. Eur. J. Clin. Investig. 2017, 47, 600–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambarish, V.; Chandrashekara, S.; Suresh, K.P. Moderate regular exercises reduce inflammatory response for physical stress. Indian J. Physiol. Pharmacol. 2012, 56, 7–14. [Google Scholar] [PubMed]
- Longo, M.; Zatterale, F.; Naderi, J.; Parrillo, L.; Formisano, P.; Raciti, G.A.; Beguinot, F.; Miele, C. Adipose Tissue Dysfunction as Determinant of Obesity-Associated Metabolic Complications. Int. J. Mol. Sci. 2019, 20, 2358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuster, J.J.; Ouchi, N.; Gokce, N.; Walsh, K. Obesity-Induced Changes in Adipose Tissue Microenvironment and Their Impact on Cardiovascular Disease. Circ. Res. 2016, 118, 1786–1807. [Google Scholar] [CrossRef] [Green Version]
- Chawla, A.; Nguyen, K.D.; Goh, Y.P. Macrophage-mediated inflammation in metabolic disease. Nat. Rev. Immunol. 2011, 11, 738–749. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.C.; Lin, T.H.; Wu, M.Y.; Chiu, Y.C.; Tang, C.H.; Hour, M.J.; Liou, H.C.; Tu, H.J.; Yang, R.S.; Fu, W.M. 5-Lipoxygenase inhibitors attenuate TNF-α-induced inflammation in human synovial fibroblasts. PLoS ONE 2014, 9, e107890. [Google Scholar] [CrossRef]
- Muscella, A.; Stefàno, E.; Lunetti, P.; Capobianco, L.; Marsigliante, S. The Regulation of Fat Metabolism During Aerobic Exercise. Biomolecules 2020, 10, 1699. [Google Scholar] [CrossRef]
- Kassouf, T.; Sumara, G. Impact of Conventional and Atypical MAPKs on the Development of Metabolic Diseases. Biomolecules 2020, 10, 1256. [Google Scholar] [CrossRef]
- Frühbeck, G.; Méndez-Giménez, L.; Fernández-Formoso, J.A.; Fernández, S.; Rodríguez, A. Regulation of adipocyte lipolysis. Nutr. Res. Rev. 2014, 27, 63–93. [Google Scholar] [CrossRef] [Green Version]
- Wedell-Neergaard, A.S.; Lang Lehrskov, L.; Christensen, R.H.; Legaard, G.E.; Dorph, E.; Larsen, M.K.; Launbo, N.; Fagerlind, S.R.; Seide, S.K.; Nymand, S.; et al. Exercise-Induced Changes in Visceral Adipose Tissue Mass Are Regulated by IL-6 Signaling: A Randomized Controlled Trial. Cell Metab. 2019, 29, 844–855. [Google Scholar] [CrossRef]
- Wueest, S.; Konrad, D. The controversial role of IL-6 in adipose tissue on obesity-induced dysregulation of glucose metabolism. Am. J. Physiol. Endocrinol. Metab. 2020, 319, E607–E613. [Google Scholar] [CrossRef]
- Murray, B.; Rosenbloom, C. Fundamentals of glycogen metabolism for coaches and athletes. Nutr. Rev. 2018, 76, 243–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, M.I.; Bourgeois, J.M.; Nederveen, J.P.; Leite, M.R.; Hettinga, B.P.; Bujak, A.L.; May, L.; Lin, E.; Crozier, M.; Rusiecki, D.R.; et al. Lifelong aerobic exercise protects against inflammaging and cancer. PLoS ONE 2019, 14, e0210863. [Google Scholar] [CrossRef] [PubMed]
- Brooks, G.A. The Precious Few Grams of Glucose During Exercise. Int. J. Mol. Sci. 2020, 21, 5733. [Google Scholar] [CrossRef] [PubMed]
- Hennigar, S.R.; McClung, J.P.; Pasiakos, S.M. Nutritional interventions and the IL-6 response to exercise. FASEB J. 2017, 31, 3719–3728. [Google Scholar] [CrossRef] [Green Version]
- Cerqueira, É.; Marinho, D.A.; Neiva, H.P.; Lourenço, O. Inflammatory Effects of High and Moderate Intensity Exercise-A Systematic Review. Front. Physiol. 2020, 10, 1550. [Google Scholar] [CrossRef] [Green Version]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef]
- Sabag, A.; Way, K.L.; Keating, S.E.; Sultana, R.N.; O’Connor, H.T.; Baker, M.K.; Chuter, V.H.; George, J.; Johnson, N.A. Exercise and ectopic fat in type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2017, 43, 195–210. [Google Scholar] [CrossRef]
- Silva, C.M.S.; Vieira-Junior, R.C.; Trombeta, J.C.R.; Lima, T.R.; Fraga, G.A.; Sena, M.S.; Ávila, E.T.P.; Tibana, R.A.; Prestes, J.; Navalta, J.W.; et al. Effects of aerobic and resistance training of long duration on pro- and anti-inflammatory cytokines in rats. Rev. Andal. Med. Deport. 2017, 10, 170–175. [Google Scholar] [CrossRef] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine; Liguori, G.; Feito, Y.; Fountaine, C.; Roy, B.A. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2021. [Google Scholar]
- Kercher, V.M.; Kercher, K.; Levy, P.; Bennion, T.; Alexander, C.; Amaral, P.C.; Batrakoulis, A.; Chávez, L.F.J.G.; Cortés-Almanzar, P.; Haro, J.L.; et al. Fitness Trends from Around the Globe. ACSMs Health Fit. J. 2023, 27, 19–30. [Google Scholar] [CrossRef]
- Rejeki, P.S.; Baskara, P.G.; Herawati, L.; Pranoto, A.; Setiawan, H.K.; Lesmana, R.; Halim, S. Moderate-intensity exercise decreases the circulating level of betatrophin and its correlation among markers of obesity in women. J. Basic Clin. Physiol. Pharmacol. 2022, 33, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Carpino, G.; Del Ben, M.; Pastori, D.; Carnevale, R.; Baratta, F.; Overi, D.; Francis, H.; Cardinale, V.; Onori, P.; Safarikia, S.; et al. Increased Liver Localization of Lipopolysaccharides in Human and Experimental NAFLD. Hepatology 2020, 72, 470–485. [Google Scholar] [CrossRef]
- Zhao, Q.; Liu, J.; Deng, H.; Ma, R.; Liao, J.Y.; Liang, H.; Hu, J.; Li, J.; Guo, Z.; Cai, J.; et al. Targeting Mitochondria-Located circRNA SCAR Alleviates NASH via Reducing mROS Output. Cell 2020, 183, 76–93. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.S.; Dhaliwal, S.S.; Hills, A.P.; Pal, S. Effects of chronic exercise training on inflammatory markers in Australian overweight and obese individuals in a randomized controlled trial. Inflammation 2013, 36, 625–632. [Google Scholar] [CrossRef]
- Parhampour, B.; Dadgoo, M.; Vasaghi-Gharamaleki, B.; Torkaman, G.; Ravanbod, R.; Mirzaii-Dizgah, I.; Reza Baghaipour, M.; Saneii, S.H. The effects of six-week resistance, aerobic and combined exercises on the proinflammatory and anti-inflammatory markers in overweight patients with moderate haemophilia A: A randomized controlled trial. Haemophilia 2019, 25, e257–e266. [Google Scholar]
- Ismail, I.; Keating, S.E.; Baker, M.K.; Johnson, N.A. A systematic review and meta-analysis of the effect of aerobic vs. resistance exercise training on visceral fat. Obes. Rev. 2012, 13, 68–91. [Google Scholar] [CrossRef]
- Batrakoulis, A.; Jamurtas, A.Z.; Metsios, G.S.; Perivoliotis, K.; Liguori, G.; Feito, Y.; Riebe, D.; Thompson, W.R.; Angelopoulos, T.J.; Krustrup, P.; et al. Comparative Efficacy of 5 Exercise Types on Cardiometabolic Health in Overweight and Obese Adults: A Systematic Review and Network Meta-Analysis of 81 Randomized Controlled Trials. Circulation. Circ. Cardiovasc. Qual. Outcomes 2022, 15, e008243. [Google Scholar] [CrossRef]
- Yang, Y.; Yang, G. Rosiglitazone regulates IL-6-stimulated lipolysis in porcine adipocytes. Biochem. Cell Biol. 2010, 88, 853–860. [Google Scholar] [CrossRef]
- Macêdo Santiago, L.Â.; Neto, L.G.L.; Borges Pereira, G.; Leite, R.D.; Mostarda, C.T.; de Oliveira Brito Monzani, J.; Sousa, W.R.; Rodrigues Pinheiro, A.; Navarro, F. Effects of Resistance Training on Immunoinflammatory Response, TNF-Alpha Gene Expression, and Body Composition in Elderly Women. J. Aging Res. 2018, 2018, 1467025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silveira, L.R.; Pinheiro, C.H.; Zoppi, C.C.; Hirabara, S.M.; Vitzel, K.F.; Bassit, R.A.; Barbosa, M.R.; Sampaio, I.H.; Melo, I.H.; Fiamoncini, J.; et al. Regulation of glucose and fatty acid metabolism in skeletal muscle during contraction. Arq. Bras. Endocrinol. Metabol. 2011, 55, 303–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, C.; Zhu, L.; Chen, X.; Gu, N.; Chen, L.; Zhu, L.; Yang, L.; Pang, L.; Guo, X.; Ji, C.; et al. IL-6 and TNF-α induced obesity-related inflammatory response through transcriptional regulation of miR-146b. J. Interferon Cytokine Res. 2014, 34, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Abdelaal, M.; le Roux, C.W.; Docherty, N.G. Morbidity and mortality associated with obesity. Ann. Transl. Med. 2017, 5, 161. [Google Scholar] [CrossRef] [Green Version]
- Bueno-Antequera, J.; Munguía-Izquierdo, D. Exercise and Schizophrenia. Adv. Exp. Med. Biol. 2020, 1228, 317–332. [Google Scholar]
- Erkens, R.; Suvorava, T.; Kramer, C.M.; Diederich, L.D.; Kelm, M.; Cortese-Krott, M.M. Modulation of Local and Systemic Heterocellular Communication by Mechanical Forces: A Role of Endothelial Nitric Oxide Synthase. Antioxid. Redox Signal. 2017, 26, 917–935. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameter | (CTRL; n = 9) | (MIET; n = 9) | (MIRT; n = 9) | (MICT; n = 9) | p-Value |
|---|---|---|---|---|---|
| Age, yrs | 22.22 ± 1.64 | 21.44 ± 1.67 | 21.78 ± 1.30 | 22.00 ± 1.00 | 0.695 |
| BH, m | 1.59 ± 0.06 | 1.55 ± 0.07 | 1.56 ± 0.06 | 1.57 ± 0.05 | 0.910 |
| BW, kg | 77.47 ± 10.06 | 74.13 ± 8.32 | 76.20 ± 9.98 | 76.51 ± 11.30 | 0.659 |
| BMI, kg/m2 | 30.69 ± 4.01 | 30.64 ± 3.39 | 31.20 ± 3.58 | 31.19 ± 3.61 | 0.979 |
| FM, kg | 35.25 ± 6.42 | 32.49 ± 5.12 | 34.57 ± 6.71 | 32.99 ± 6.34 | 0.755 |
| FM, % | 39.48 ± 7.46 | 43.63 ± 2.43 | 45.11 ± 3.94 | 42.70 ± 3.36 | 0.095 |
| FMI, kg/m2 | 13.03 ± 2.79 | 13.43 ± 2.12 | 14.24 ± 2.85 | 13.36 ± 2.23 | 0.770 |
| FFM, kg | 44.69 ± 3.96 | 41.65 ± 3.47 | 41.72 ± 4.79 | 43.95 ± 5.58 | 0.377 |
| FFMI, kg/m2 | 17.77 ± 1.43 | 17.20 ± 1.42 | 17.07 ± 1.08 | 17.82 ± 1.74 | 0.587 |
| SMM, kg | 19.91 ± 2.56 | 18.44 ± 2.05 | 19.94 ± 4.69 | 20.33 ± 3.19 | 0.632 |
| TBW, % | 32.88 ± 3.21 | 30.60 ± 2.56 | 31.43 ± 4.81 | 32.52 ± 4.18 | 0.572 |
| ECW, % | 15.00 ± 1.50 | 13.79 ± 1.26 | 14.20 ± 1.99 | 14.40 ± 1.83 | 0.491 |
| ECW/TBW, % | 45.72 ± 1.39 | 45.21 ± 1.31 | 45.27 ± 1.29 | 44.27 ± 0.86 | 0.106 |
| TEE, kcal/day | 2654.22 ± 149.78 | 2590.33 ± 153.71 | 2627.22 ± 181.74 | 2630.33 ± 204.23 | 0.891 |
| REE, kcal/day | 1551.78 ± 99.27 | 1523.78 ± 90.37 | 1545.44 ± 106.78 | 1547.33 ± 120.23 | 0.943 |
| WC, m | 0.93 ± 0.09 | 0.92 ± 0.11 | 0.91 ± 0.04 | 0.90 ± 0.05 | 0.792 |
| HC, m | 1.11 ± 0.09 | 1.12 ± 0.16 | 1.09 ± 0.05 | 1.14 ± 0.19 | 0.928 |
| WHR | 0.84 ± 0.06 | 0.83 ± 0.08 | 0.83 ± 0.05 | 0.80 ± 0.09 | 0.694 |
| SBP, mmHg | 115.67 ± 8.09 | 109.33 ± 8.41 | 114.89 ± 10.79 | 114.11 ± 10.77 | 0.507 |
| DBP, mmHg | 78.22 ± 8.01 | 78.67 ± 7.48 | 82.11 ± 8.41 | 80.67 ± 5.96 | 0.671 |
| RHR, bpm | 77.44 ± 9.51 | 76.56 ± 6.56 | 83.56 ± 7.58 | 82.00 ± 6.87 | 0.174 |
| SpO2, % | 97.89 ± 0.93 | 96.67 ± 3.39 | 98.11 ± 1.05 | 97.67 ± 1.41 | 0.430 |
| BT, °C | 36.21 ± 0.36 | 36.24 ± 0.22 | 36.28 ± 0.23 | 36.13 ± 0.18 | 0.666 |
| FBS, mg/dL | 90.89 ± 6.53 | 91.22 ± 5.85 | 91.00 ± 6.34 | 93.78 ± 5.07 | 0.700 |
| Hb, g/dL | 14.21 ± 2.70 | 15.44 ± 1.28 | 15.57 ± 1.34 | 15.75 ± 2.01 | 0.326 |
| Baseline IL-6 (pg/mL) | 531.93 ± 108.02 | 508.22 ± 158.55 | 530.90 ± 172.92 | 552.82 ± 117.37 | 0.930 |
| Baseline TNF-α (pg/mL) | 97.51 ± 55.64 | 98.35 ± 29.82 | 97.20 ± 29.35 | 97.65 ± 48.92 | 0.990 |
| Time | (CTRL; n = 9) | (MIET; n = 9) | (MIRT; n = 9) | (MICT; n = 9) | p-Value |
|---|---|---|---|---|---|
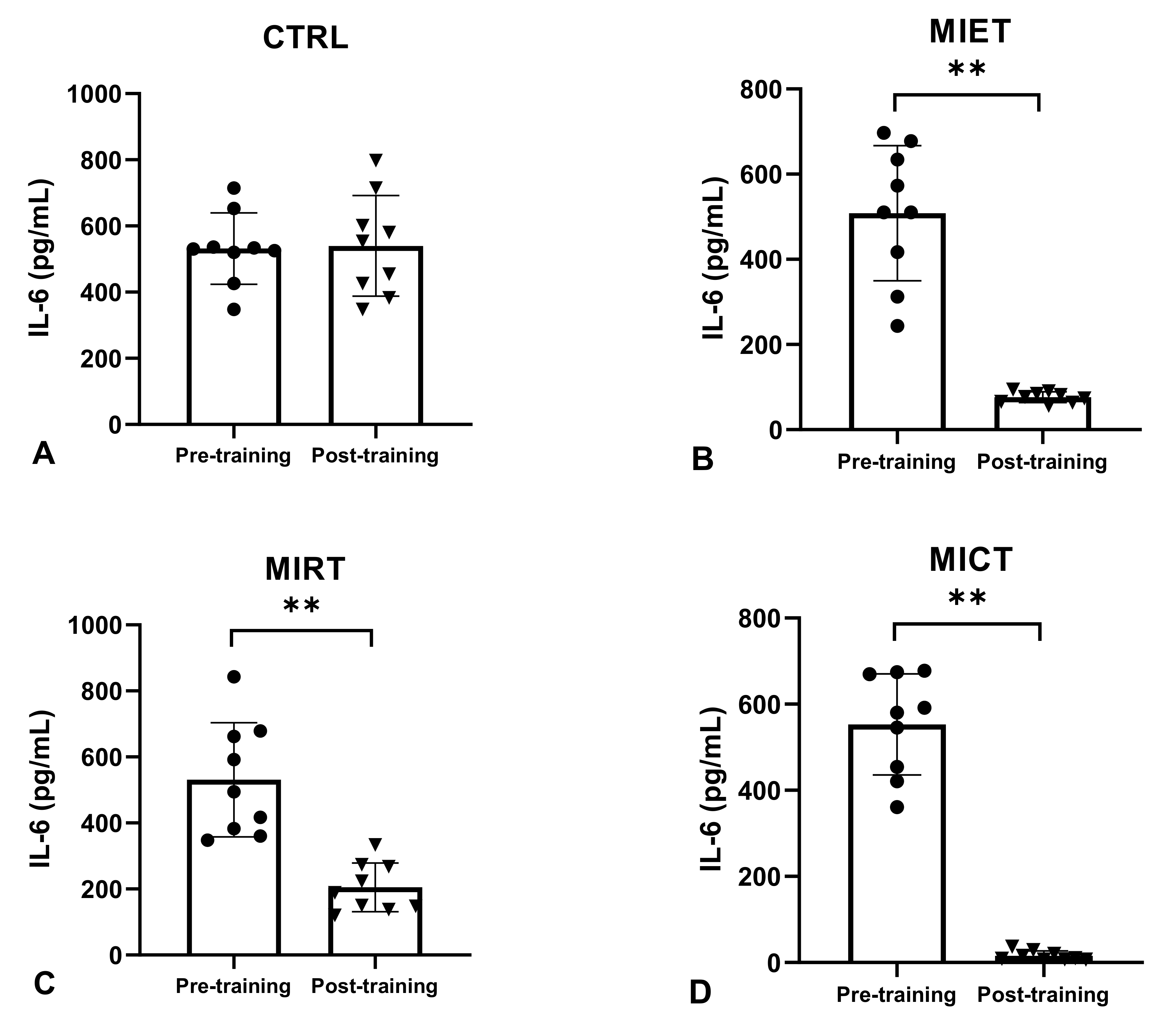
| Pre-training IL-6 (pg/mL) | 531.93 ± 108.02 | 508.22 ± 158.55 | 530.90 ± 172.92 | 552.82 ± 117.37 | 0.930 † |
| Post-training IL-6 (pg/mL) | 539.90 ± 151.91 | 76.20 ± 12.61 **& | 205.00 ± 74.08 ** | 15.92 ± 10.82 **$& | 0.000 # |
| Δ IL-6 (pg/mL) | 7.97 ± 70.93 | −432.02 ± 163.76 ** | −325.90 ± 170.31 ** | −536.90 ± 118.74 **& | 0.000 # |
| IL-6 percent changes from pre-training (%) | 0.76 ± 13.58 | −82.79 ± 8.73 **$ | −58.30 ± 18.05 ** | −96.91 ± 2.39 **$& | 0.000 # |
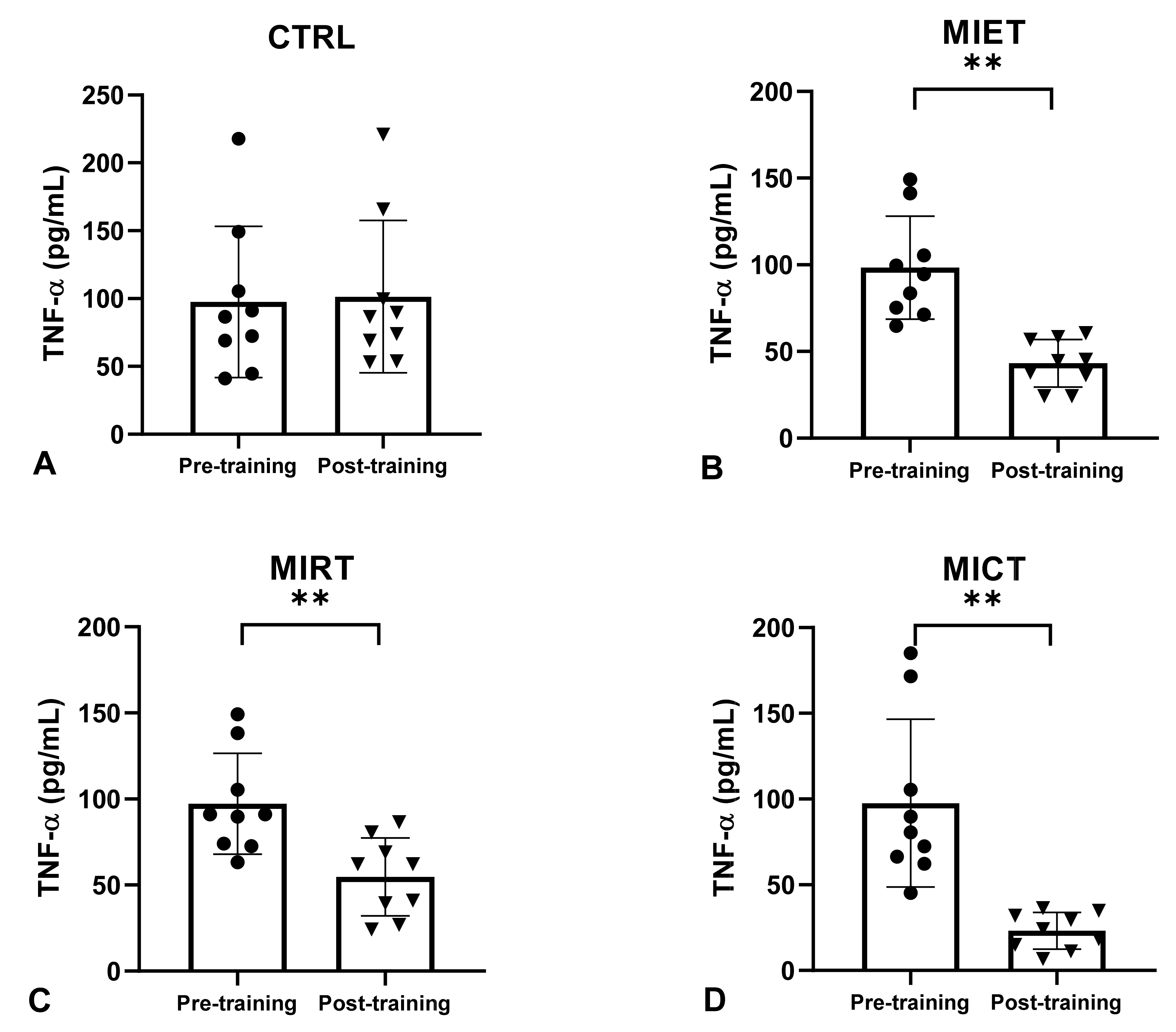
| Pre-training TNF-α (pg/mL) | 97.51 ± 55.64 | 98.35 ± 29.82 | 97.20 ± 29.35 | 97.65 ± 48.92 | 0.990 † |
| Post-training TNF-α (pg/mL) | 101.44 ± 56.12 | 43.17 ± 13.78 ** | 54.73 ± 22.71 * | 23.17 ± 10.80 **$& | 0.000 # |
| Δ TNF-α (pg/mL) | 3.93 ± 7.71 | −55.17 ± 29.95 ** | −42.47 ± 29.29 ** | −74.48 ± 45.15 ** | 0.000 # |
| TNF-α percent changes from pre-training (%) | 6.46 ± 12.13 | −53.11 ± 20.02 ** | −42.59 ± 21.64 ** | −73.41 ± 14.50 **& | 0.000 † |
| Parameter | Pro-inflammatory cytokines | |||
|---|---|---|---|---|
| Δ IL-6 (pg/mL) | Δ TNF-α (pg/mL) | |||
| R | p-Value | r | p-Value | |
| Δ Body mass index, kg/m2 | 0.622 ** | p ≤ 0.001 | 0.576 ** | p ≤ 0.001 |
| Δ Fat mass, kg | 0.728 ** | p ≤ 0.001 | 0.481 ** | p ≤ 0.001 |
| Δ Body fat percentage, % | 0.683 ** | p ≤ 0.001 | 0.560 ** | p ≤ 0.001 |
| Δ Fat-free mass, kg | 0.621 ** | p ≤ 0.001 | 0.480 ** | p ≤ 0.001 |
| Δ Skeletal muscle mass, kg | −0.614 ** | p ≤ 0.001 | −0.593 ** | p ≤ 0.001 |
| Δ Waist circumference, m | 0.671 ** | p ≤ 0.001 | 0.540 ** | p ≤ 0.001 |
| Δ Waist-to-hip ratio | 0.691 ** | p ≤ 0.001 | 0.650 ** | p ≤ 0.001 |
| Δ Adiponectin, ng/mL | −0.526 ** | p ≤ 0.001 | −0.542 ** | p ≤ 0.001 |
| Δ Leptin, ng/mL | 0.603 ** | p ≤ 0.001 | 0.454 ** | p ≤ 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pranoto, A.; Cahyono, M.B.A.; Yakobus, R.; Izzatunnisa, N.; Ramadhan, R.N.; Rejeki, P.S.; Miftahussurur, M.; Effendi, W.I.; Wungu, C.D.K.; Yamaoka, Y. Long-Term Resistance–Endurance Combined Training Reduces Pro-Inflammatory Cytokines in Young Adult Females with Obesity. Sports 2023, 11, 54. https://doi.org/10.3390/sports11030054
Pranoto A, Cahyono MBA, Yakobus R, Izzatunnisa N, Ramadhan RN, Rejeki PS, Miftahussurur M, Effendi WI, Wungu CDK, Yamaoka Y. Long-Term Resistance–Endurance Combined Training Reduces Pro-Inflammatory Cytokines in Young Adult Females with Obesity. Sports. 2023; 11(3):54. https://doi.org/10.3390/sports11030054
Chicago/Turabian StylePranoto, Adi, Maulana Bagus Adi Cahyono, Reinaldi Yakobus, Nabilah Izzatunnisa, Roy Novri Ramadhan, Purwo Sri Rejeki, Muhammad Miftahussurur, Wiwin Is Effendi, Citrawati Dyah Kencono Wungu, and Yoshio Yamaoka. 2023. "Long-Term Resistance–Endurance Combined Training Reduces Pro-Inflammatory Cytokines in Young Adult Females with Obesity" Sports 11, no. 3: 54. https://doi.org/10.3390/sports11030054
APA StylePranoto, A., Cahyono, M. B. A., Yakobus, R., Izzatunnisa, N., Ramadhan, R. N., Rejeki, P. S., Miftahussurur, M., Effendi, W. I., Wungu, C. D. K., & Yamaoka, Y. (2023). Long-Term Resistance–Endurance Combined Training Reduces Pro-Inflammatory Cytokines in Young Adult Females with Obesity. Sports, 11(3), 54. https://doi.org/10.3390/sports11030054