
High-Intensity Training for Knee Osteoarthritis: A Narrative Review



Abstract
:1. Introduction
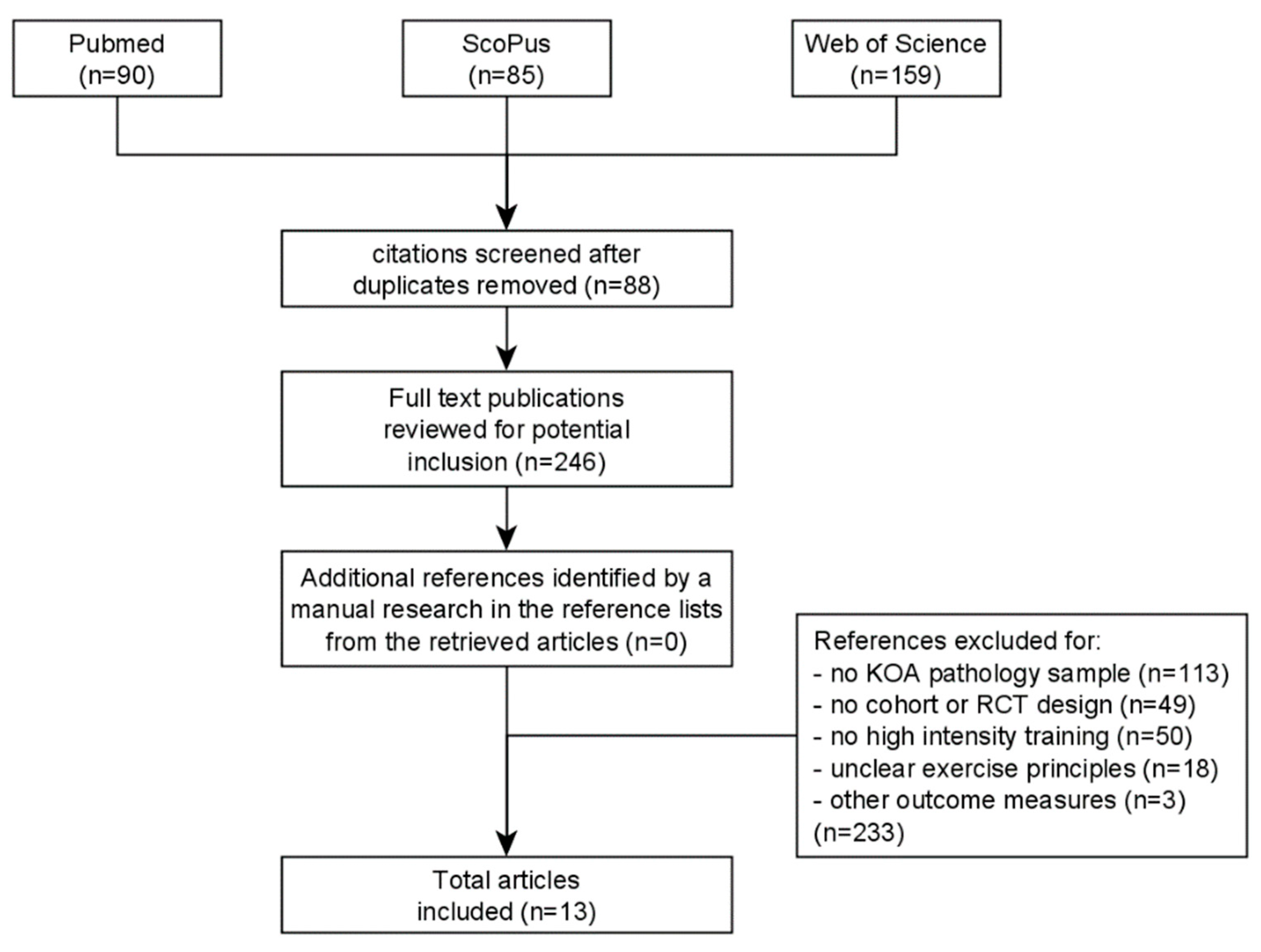
2. Materials and Methods
3. Results
3.1. HIT (without a Comparator Group)
3.2. HIT vs. MICT
3.3. HIT vs. LIT
3.4. HIT vs. CT
3.5. HIT vs. LIT vs. CT
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Implications
4.3. Future Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnson, V.L.; Hunter, D.J. The epidemiology of osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2014, 28, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Neogi, T.; Zhang, Y. Epidemiology of osteoarthritis. Rheum. Dis. Clin. N. Am. 2013, 39, 1–19. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef] [PubMed]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef] [PubMed]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef]
- Aamot, I.L.; Karlsen, T.; Dalen, H.; Støylen, A. Long-term Exercise Adherence After High-intensity Interval Training in Cardiac Rehabilitation: A Randomized Study. Physiother. Res. Int. 2016, 21, 54–64. [Google Scholar] [CrossRef]
- Gibala, M.J. High-intensity Interval Training: A Time-efficient Strategy for Health Promotion? Curr. Sports Med. Rep. 2007, 6, 211–213. [Google Scholar] [CrossRef]
- Fransen, M.; McConnell, S.; Harmer, A.R.; Van der Esch, M.; Simic, M.; Bennell, K.L. Exercise for osteoarthritis of the knee. Cochrane Database Syst. Rev. 2015, 1, CD004376. [Google Scholar] [CrossRef]
- Nelson, A.E.; Allen, K.D.; Golightly, Y.M.; Goode, A.P.; Jordan, J.M. A systematic review of recommendations and guidelines for the management of osteoarthritis: The chronic osteoarthritis management initiative of the U.S. bone and joint initiative. Semin Arthritis Rheum. 2014, 43, 701–712. [Google Scholar] [CrossRef]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [PubMed]
- Persoon, S.; Kersten, M.J.; ChinAPaw, M.J.; Buffart, L.M.; Burghout, H.; Schep, G.; Brug, J.; Nollet, F. Design of the EXercise Intervention after Stem cell Transplantation (EXIST) study: A randomized controlled trial to evaluate the effectiveness and cost-effectiveness of an individualized high intensity physical exercise program on fitness and fatigue in patients with multiple myeloma or (non-) Hodgkin’s lymphoma treated with high dose chemotherapy and autologous stem cell transplantation. BMC Cancer 2010, 10, 671. [Google Scholar]
- Knowles, M.A.; Hurst, C.D. Molecular biology of bladder cancer: New insights into pathogenesis and clinical diversity. Nat. Rev. Cancer 2015, 15, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Bressel, E.; Wing, J.E.; Miller, A.I.; Dolny, D.G. High-Intensity Interval Training on an Aquatic Treadmill in Adults With Osteoarthritis: Effect on Pain, Balance, Function, and Mobility. J. Strength Cond. Res. 2014, 28, 2088–2096. [Google Scholar] [CrossRef]
- Fransen, M.; McConnell, S. Exercise for osteoarthritis of the knee. Cochrane Database Syst. Rev. 2008, 4, CD004376. [Google Scholar]
- Farr, J.N.; Going, S.B.; Lohman, T.G.; Rankin, L.L.; Kasle, S.; Cornett, M.; Cussler, E.C. Physical activity levels in patients with early knee osteoarthritis measured by accelerometry. Arthritis Rheum. 2008, 59, 1229–1236. [Google Scholar] [CrossRef]
- Wallis, J.A.; Webster, K.E.; Levinger, P.; Taylor, N.F. What proportion of people with hip and knee osteoarthritis meet physical activity guidelines? A systematic review and meta-analysis. Osteoarthr. Cartil. 2013, 21, 1648–1659. [Google Scholar] [CrossRef]
- Aglamiş, B.; Toraman, N.F.; Yaman, H. Change of quality of life due to exercise training in knee osteoarthritis: SF-36 and WOMAC. J. Back Musculoskelet. Rehabil. 2009, 22, 43–48. [Google Scholar] [CrossRef]
- Tucker, J.M.; Welk, G.J.; Beyler, N.K. Physical Activity in U.S. Adults: Compliance with the Physical Activity Guidelines for Americans. Am. J. Prev. Med. 2011, 40, 454–461. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef]
- Fransen, M.; McConnell, S. Land-based exercise for osteoarthritis of the knee: A metaanalysis of randomized controlled trials. J. Rheumatol. 2009, 36, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Golightly, Y.M.; Allen, K.D.; Caine, D.J. A comprehensive review of the effectiveness of different exercise programs for patients with osteoarthritis. Phys. Sportsmed. 2012, 40, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.Y.; Zhang, Z.R.; Tang, Z.M.; Hua, F.Z. Benefits and Mechanisms of Exercise Training for Knee Osteoarthritis. Front. Physiol. 2021, 12, 794062. [Google Scholar] [CrossRef]
- Hall, M.; Hinman, R.S.; Wrigley, T.V.; Kasza, J.; Lim, B.W.; Bennell, K.L. Knee extensor strength gains mediate symptom improvement in knee osteoarthritis: Secondary analysis of a randomised controlled trial. Osteoarthr. Cartil. 2018, 26, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.A.; Clements, K.M.; Fiatarone, M.A. A randomized controlled trial of progressive resistance training in depressed elders. J. Gerontol. A Biol. Sci. Med. Sci. 1997, 52, M27–M35. [Google Scholar] [CrossRef]
- Otterness, I.G.; Eskra, J.D.; Bliven, M.L.; Shay, A.K.; Pelletier, J.P.; Milici, A.J. Exercise protects against articular cartilage degeneration in the hamster. Arthritis Rheum. 1998, 41, 2068–2076. [Google Scholar] [CrossRef]
- Van den Hoogen, B.M.; van de Lest, C.H.; van Weeren, P.R.; Lafeber, F.P.; Lopes-Cardozo, M.; van Golde, L.M.; Barneveld, A. Loading-induced changes in synovial fluid affect cartilage metabolism. Br. J. Rheumatol. 1998, 37, 671–676. [Google Scholar] [CrossRef]
- Ferenczi, M.A.; Bershitsky, S.Y.; Koubassova, N.A.; Kopylova, G.V.; Fernandez, M.; Narayanan, T.; Tsaturyan, A.K. Why muscle is an efficient shock absorber. PLoS ONE 2014, 9, e85739. [Google Scholar] [CrossRef]
- NICE. Overview. Osteoarthritis in over 16s: Diagnosis and Management. Guidance. 2022. Available online: https://www.nice.org.uk/guidance/ng226 (accessed on 5 March 2023).
- Raposo, F.; Ramos, M.; Lúcia Cruz, A. Effects of exercise on knee osteoarthritis: A systematic review. Musculoskelet. Care 2021, 19, 399–435. [Google Scholar] [CrossRef]
- Smith-Ryan, A.E.; Blue, M.N.; Anderson, K.C.; Hirsch, K.R.; Allen, K.D.; Huebner, J.L.; Muehlbauer, M.J.; Ilkayeva, O.R.; Kraus, V.B.; Kraus, W.E.; et al. Metabolic and physiological effects of high intensity interval training in patients with knee osteoarthritis: A pilot and feasibility study. Osteoarthr. Cartil. Open 2020, 2, 100083. [Google Scholar] [CrossRef]
- Verbrugghe, J.; Agten, A.; Stevens, S.; Hansen, D.; Demoulin, C.; Eijnde, B.O.; Vandenabeele, F.; Timmermans, A. Exercise Intensity Matters in Chronic Nonspecific Low Back Pain Rehabilitation. Med. Sci. Sports Exerc. 2019, 51, 2434–2442. [Google Scholar] [CrossRef]
- Peterson, M.D.; Rhea, M.R.; Sen, A.; Gordon, P.M. Resistance exercise for muscular strength in older adults: A meta-analysis. Ageing Res. Rev. 2010, 9, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Bartholdy, C.; Juhl, C.; Christensen, R.; Lund, H.; Zhang, W.; Henriksen, M. The role of muscle strengthening in exercise therapy for knee osteoarthritis: A systematic review and meta-regression analysis of randomized trials. Semin. Arthritis Rheum. 2017, 47, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Weston, K.S.; Wisløff, U.; Coombes, J.S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Little, J.P.; Macdonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Sveaas, S.H.; Bilberg, A.; Berg, I.J.; Provan, S.A.; Rollefstad, S.; Semb, A.G.; Hagen, K.B.; Johansen, M.W.; Pedersen, E.; Dagfinrud, H. High intensity exercise for 3 months reduces disease activity in axial spondyloarthritis (axSpA): A multicentre randomised trial of 100 patients. Br. J. Sports Med. 2020, 54, 292–297. [Google Scholar] [CrossRef]
- Wewege, M.A.; Booth, J.; Parmenter, B.J. Aerobic vs. resistance exercise for chronic non-specific low back pain: A systematic review and meta-analysis. J. Back Musculoskelet. Rehabil. 2018, 31, 889–899. [Google Scholar] [CrossRef]
- Verbrugghe, J.; Agten, A.; Eijnde, B.O.; Olivieri, E.; Huybrechts, X.; Seelen, H.; Vandenabeele, F.; Timmermans, A. Feasibility of high intensity training in nonspecific chronic low back pain: A clinical trial. J. Back Musculoskelet. Rehabil. 2018, 31, 657–666. [Google Scholar] [CrossRef]
- Verbrugghe, J.; Agten, A.; Stevens, S.; Hansen, D.; Demoulin, C.; Eijnde, B.O.; Vandenabeele, F.; Timmermans, A. High Intensity Training to Treat Chronic Nonspecific Low Back Pain: Effectiveness of Various Exercise Modes. J. Clin. Med. 2020, 9, 2401. [Google Scholar] [CrossRef]
- Agten, A.; Verbrugghe, J.; Stevens, S.; Eijnde, B.O.; Timmermans, A.; Vandenabeele, F. High Intensity Training Increases Muscle Area Occupied by Type II Muscle Fibers of the Multifidus Muscle in Persons with Non-Specific Chronic Low Back Pain: A Pilot Trial. Appl. Sci. 2021, 11, 3306. [Google Scholar] [CrossRef]
- Verbrugghe, J.; Hansen, D.; Demoulin, C.; Verbunt, J.; Roussel, N.A.; Timmermans, A. High Intensity Training Is an Effective Modality to Improve Long-Term Disability and Exercise Capacity in Chronic Nonspecific Low Back Pain: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 10779. [Google Scholar] [CrossRef] [PubMed]
- Verbrugghe, J.; Agten, A.; Stevens, S.; Vandenabeele, F.; Roussel, N.; Verbunt, J.; Goossens, N.; Timmermans, A. High intensity training improves symptoms of central sensitization at six-month follow-up in persons with chronic nonspecific low back pain: Secondary analysis of a randomized controlled trial. Braz. J. Phys. Ther. 2023, 27, 100496. [Google Scholar] [CrossRef] [PubMed]
- Zebis, M.K.; Andersen, L.L.; Pedersen, M.T.; Mortensen, P.; Andersen, C.H.; Pedersen, M.M.; Boysen, M.; Roessler, K.K.; Hannerz, H.; Mortensen, O.S.; et al. Implementation of neck/shoulder exercises for pain relief among industrial workers: A randomized controlled trial. BMC Musculoskelet. Disord. 2011, 12, 205. [Google Scholar] [CrossRef] [PubMed]
- Farup, J.; Dalgas, U.; Keytsman, C.; Eijnde, B.O.; Wens, I. High Intensity Training May Reverse the Fiber Type Specific Decline in Myogenic Stem Cells in Multiple Sclerosis Patients. Front. Physiol. 2016, 7, 193. [Google Scholar] [CrossRef]
- Guiraud, T.; Nigam, A.; Gremeaux, V.; Meyer, P.; Juneau, M.; Bosquet, L. High-Intensity Interval Training in Cardiac Rehabilitation. Sports Med. 2012, 42, 587–605. [Google Scholar] [CrossRef]
- Gloeckl, R.; Marinov, B.; Pitta, F. Practical recommendations for exercise training in patients with COPD. Eur. Respir. Rev. 2013, 22, 178–186. [Google Scholar] [CrossRef]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle. Part II: Anaerobic energy, neuromuscular load and practical applications. Sports Med. 2013, 43, 927–954. [Google Scholar] [CrossRef]
- Seynnes, O.R.; de Boer, M.; Narici, M.V. Early skeletal muscle hypertrophy and architectural changes in response to high-intensity resistance training. J. Appl. Physiol. 2007, 102, 368–373. [Google Scholar] [CrossRef]
- Fleg, J.L. Salutary effects of high-intensity interval training in persons with elevated cardiovascular risk. F1000Research 2016, 5, 2254. [Google Scholar] [CrossRef]
- Wen, D.; Utesch, T.; Wu, J.; Robertson, S.; Liu, J.; Hu, G.; Chen, H. Effects of different protocols of high intensity interval training for VO2max improvements in adults: A meta-analysis of randomised controlled trials. J. Sci. Med. Sport 2019, 22, 941–947. [Google Scholar] [CrossRef]
- Botta, R.M.; Palermi, S.; Tarantino, D.; Botta, R.M.; Palermi, S.; Tarantino, D. High-intensity interval training for chronic pain conditions: A narrative review. J. Exerc. Rehabil. 2022, 18, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Helgerud, J.; Høydal, K.; Wang, E.; Karlsen, T.; Berg, P.; Bjerkaas, M.; Simonsen, T.; Helgesen, C.; Hjorth, N.; Bach, R.; et al. Aerobic High-Intensity Intervals Improve V˙O2max More Than Moderate Training. Med. Sci. Sports Exerc. 2007, 39, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Milanović, Z.; Sporiš, G.; Weston, M. Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials. Sports Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L.; Dunlop, D.D.; Cahue, S.; Song, J.; Hayes, K.W. Quadriceps strength and osteoarthritis progression in malaligned and lax knees. Ann. Intern. Med. 2003, 138, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Jan, M.H.; Lin, J.J.; Liau, J.J.; Lin, Y.F.; Lin, D.H. Investigation of clinical effects of high- and low-resistance training for patients with knee osteoarthritis: A randomized controlled trial. Phys. Ther. 2008, 88, 427–436. [Google Scholar] [CrossRef]
- King, L.K.; Birmingham, T.B.; Kean, C.O.; Jones, I.C.; Bryant, D.M.; Giffin, J.R. Resistance training for medial compartment knee osteoarthritis and malalignment. Med. Sci. Sports Exerc. 2008, 40, 1376–1384. [Google Scholar] [CrossRef]
- Hurkmans, E.; van der Giesen, F.J.; Vliet Vlieland, T.P.; Schoones, J.; Van den Ende, E.C. Dynamic exercise programs (aerobic capacity and/or muscle strength training) in patients with rheumatoid arthritis. Cochrane Database Syst. Rev. 2009, 4, CD006853. [Google Scholar] [CrossRef]
- Baker, K.R.; Nelson, M.E.; Felson, D.T.; Layne, J.E.; Sarno, R.; Roubenoff, R. The efficacy of home based progressive strength training in older adults with knee osteoarthritis: A randomized controlled trial. J. Rheumatol. 2001, 28, 1655–1665. [Google Scholar]
- Gurd, B.J.; Perry, C.G.R.; Heigenhauser, G.J.F.; Spriet, L.L.; Bonen, A. High-intensity interval training increases SIRT1 activity in human skeletal muscle. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2010, 35, 350–357. [Google Scholar] [CrossRef]
- Deng, Z.; Li, Y.; Liu, H.; Xiao, S.; Li, L.; Tian, J.; Cheng, C.; Zhang, G.; Zhang, F. The role of sirtuin 1 and its activator, resveratrol in osteoarthritis. Biosci. Rep. 2019, 39, BSR20190189. [Google Scholar] [CrossRef]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R. Consensus on Exercise Reporting Template (CERT): Explanation and Elaboration Statement. Br. J. Sports Med. 2016, 50, 1428–1437. [Google Scholar] [CrossRef] [PubMed]
- Golightly, Y.M.; Smith-Ryan, A.E.; Blue, M.N.M.; Alvarez, C.; Allen, K.D.; Nelson, A.E. High-Intensity Interval Training for Knee Osteoarthritis: A Pilot Study. ACR Open Rheumatol. 2021, 3, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Keogh, J.W.; Grigg, J.; Vertullo, C.J. Is high-intensity interval cycling feasible and more beneficial than continuous cycling for knee osteoarthritic patients? Results of a randomised control feasibility trial. PeerJ 2018, 6, e4738. [Google Scholar] [CrossRef] [PubMed]
- De Zwart, A.H.; Dekker, J.; Roorda, L.D.; van der Esch, M.; Lips, P.; van Schoor, N.M.; Heijboer, A.C.; Turkstra, F.; Gerritsen, M.; Häkkinen, A.; et al. High-intensity versus low-intensity resistance training in patients with knee osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2022, 36, 952–967. [Google Scholar] [CrossRef] [PubMed]
- Foroughi, N.; Smith, R.M.; Lange, A.K.; Singh, M.A.F.; Vanwanseele, B. Progressive resistance training and dynamic alignment in osteoarthritis: A single-blind randomised controlled trial. Clin. Biomech. 2011, 26, 71–77. [Google Scholar] [CrossRef]
- Mangione, K.K.; McCully, K.; Gloviak, A.; Lefebvre, I.; Hofmann, M.; Craik, R. The effects of high-intensity and low-intensity cycle ergometry in older adults with knee osteoarthritis. J. Gerontol. A Biol. Sci. Med. Sci. 1999, 54, M184–M190. [Google Scholar] [CrossRef]
- Thorstensson, C.A.; Roos, E.M.; Petersson, I.F.; Ekdahl, C. Six-week high-intensity exercise program for middle-aged patients with knee osteoarthritis: A randomized controlled trial [ISRCTN20244858]. BMC Musculoskelet. Disord. 2005, 6, 27. [Google Scholar] [CrossRef]
- Waller, B.; Munukka, M.; Rantalainen, T.; Lammentausta, E.; Nieminen, M.; Kiviranta, I.; Kautiainen, H.; Häkkinen, A.; Kujala, U.; Heinonen, A. Effects of high intensity resistance aquatic training on body composition and walking speed in women with mild knee osteoarthritis: A 4-month RCT with 12-month follow-up. Osteoarthr. Cartil. 2017, 25, 1238–1246. [Google Scholar] [CrossRef]
- Calatayud, J.; Casaña, J.; Ezzatvar, Y.; Jakobsen, M.D.; Sundstrup, E.; Andersen, L.L. High-intensity preoperative training improves physical and functional recovery in the early post-operative periods after total knee arthroplasty: A randomized controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2864–2872. [Google Scholar] [CrossRef]
- Messier, S.P.; Mihalko, S.L.; Beavers, D.P.; Nicklas, B.J.; DeVita, P.; Carr, J.J.; Hunter, D.J.; Lyles, M.; Guermazi, A.; Bennell, K.L.; et al. Effect of High-Intensity Strength Training on Knee Pain and Knee Joint Compressive Forces Among Adults With Knee Osteoarthritis: The START Randomized Clinical Trial. JAMA 2021, 325, 646–657. [Google Scholar] [CrossRef]
- Alkatan, M.; Baker, J.R.; Machin, D.R.; Park, W.; Akkari, A.S.; Pasha, E.P.; Tanaka, H. Improved Function and Reduced Pain after Swimming and Cycling Training in Patients with Osteoarthritis. J. Rheumatol. 2016, 43, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Rewald, S.; Mesters, I.; Emans, P.J.; Arts, J.J.C.; Lenssen, A.F.; de Bie, R.A. Aquatic circuit training including aqua-cycling in patients with knee osteoarthritis: A feasibility study. J. Rehabil. Med. 2015, 47, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Salacinski, A.J.; Krohn, K.; Lewis, S.F.; Holland, M.L.; Ireland, K.; Marchetti, G. The Effects of Group Cycling on Gait and Pain-Related Disability in Individuals With Mild-to-Moderate Knee Osteoarthritis: A Randomized Controlled Trial. J. Orthop. Sports Phys. Ther. 2012, 42, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Kroll, H.R. Exercise therapy for chronic pain. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 263–281. [Google Scholar] [CrossRef]
- Smith, B.E.; Hendrick, P.; Bateman, M.; Holden, S.; Littlewood, C.; Smith, T.O.; Logan, P. Musculoskeletal pain and exercise-challenging existing paradigms and introducing new. Br. J. Sports Med. 2019, 53, 907–912. [Google Scholar] [CrossRef]
- Beckwée, D.; Vaes, P.; Cnudde, M.; Swinnen, E.; Bautmans, I. Osteoarthritis of the knee: Why does exercise work? A qualitative study of the literature. Ageing Res. Rev. 2013, 12, 226–236. [Google Scholar] [CrossRef]
- Runhaar, J.; Luijsterburg, P.; Dekker, J.; Bierma-Zeinstra, S.M.A. Identifying potential working mechanisms behind the positive effects of exercise therapy on pain and function in osteoarthritis; a systematic review. Osteoarthr. Cartil. 2015, 23, 1071–1082. [Google Scholar] [CrossRef]
- Slade, S.C.; Finnegan, S.; Dionne, C.E.; Underwood, M.; Buchbinder, R. The Consensus on Exercise Reporting Template (CERT) applied to exercise interventions in musculoskeletal trials demonstrated good rater agreement and incomplete reporting. J. Clin. Epidemiol. 2018, 103, 120–130. [Google Scholar] [CrossRef]
- Goh, S.-L.; Persson, M.S.M.; Stocks, J.; Hou, Y.; Welton, N.J.; Lin, J.; Hall, M.C.; Doherty, M.; Zhang, W. Relative Efficacy of Different Exercises for Pain, Function, Performance and Quality of Life in Knee and Hip Osteoarthritis: Systematic Review and Network Meta-Analysis. Sports Med. 2019, 49, 743–761. [Google Scholar] [CrossRef]
- Sharp, T.; Grandou, C.; Coutts, A.J.; Wallace, L. The Effects of High-Intensity Multimodal Training in Apparently Healthy Populations: A Systematic Review. Sports Med. Open 2022, 8, 43. [Google Scholar] [CrossRef]
- Edwards, R.R.; Dworkin, R.H.; Turk, D.C.; Angst, M.S.; Dionne, R.; Freeman, R.; Hansson, P.; Haroutounian, S.; Arendt-Nielsen, L.; Attal, N.; et al. Patient phenotyping in clinical trials of chronic pain treatments: IMMPACT recommendations. Pain 2016, 157, 1851–1871. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, G.C.; Do Nascimento, M.R.; De Miranda, A.S.; Rocha, N.P.; Teixeira, A.L.; Scalzo, P.L. Effects of an exercise therapy protocol on inflammatory markers, perception of pain, and physical performance in individuals with knee osteoarthritis. Rheumatol. Int. 2015, 35, 525–531. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study and Year | What (Equipment) | Who (Experienced Therapist?) | How | Where | When, How Much | Tailoring (of Exercise Intensity, Based on…) | How Well (Delivered and Performed as Expected?) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Individual/Group (S/US) | Adherence/Adverse Events (Reported by...) | Motivation Strategies | Progression | Exercise Program Replicable/Home Program Available? | Non-Exercise Components | |||||||
| Golightly, 2021 [63] | Cycle ergometer or treadmill; chest strap heart rate monitor | Yes | Individual (S) | Physiotherapist: number of sessions attended or completed/ participant + investigator | N.A. | N.A. | Yes, except exercise progression/N.A. | In center | 20 min (without warm-up/ cooling-down); 10 reps of 1-min high-intensity bouts HI: 90% VO2peak Rest: 1 min complete rest between reps; 24 h between training sessions | Exercise modality; exercise intensity | Yes | |
| Smith-Ryan, 2020 [31] | Electronically braked cycle ergometer | Yes | Individual (S) | Physiotherapist: number of sessions completed or total available/ participant + investigator | N.A. | N.A. | Yes, except exercise progression/ N.A. | In center | 20 min (without warm-up/ cooling-down); 10 reps of 1-min high-intensity bouts HI: 90% peak power output Rest: 1 min between reps; 24 h between training sessions | Peak power output | Yes | |
| King, 2008 [57] | Cycle ergometer; dynamometer (and accompanying software) | Yes | N.A. (S) | Researcher/ participant | N.A. | New targets of 60% peak torques based on test protocols every 3 weeks | Yes/N.A. | In center | 45 min (including warm-up) Part 1 -> 3 sets; 10 reps; concentric isokinetic knee extension and flexion at 60, 90, and 120°/sec angular velocity; 60% of baseline strength Part 2 -> 3 sets; 15 reps; concentric isokinetic knee extension and flexion at 180°/sec angular velocity; maximum effort Rest: minimal 24 h between sessions | Peak torques | Minimal modification (due to increases in pain) | |
| Keogh, 2018 [64] | Stationary bicycle | N.A. | Individual (US) | Participant (training diary)/ participant | N.A. | N.A. | Yes/yes | Home based | 25 min HI: 7 min warm-up (progressively increasing intensity); 5 sets of high-intensity intervals at 110 rpm for 45 sec with 90 sec relative rest between sets at 70 rpm (low-intensity); 6–7 min cool-down (light-moderate intensity) Moderate-intensity: 3 min warm-up (light intensity); 20 min at 60–80 rpm (moderate intensity); 2 min cooldown (light intensity) | Personal experience | Yes | |
| De Zwart, 2022 [65] | Fitness devices; weighted vests; ankle weights; resistance band | Yes | 2×/week in group (S) | Physiotherapist/ participant + investigator | N.A. | ↑ 5% 1-RM/ week, based on 1-RM measurement from week 0, week 6, and week 10 | Yes/yes (paper hand-out) | 2×/week in center | 60 min; 3 sets; 10 reps HI: 70–80% 1-RM, weighted vests during weight-bearing exercises LI: 40–50% 1-RM, no additional weighted vests Rest: 90 sec between sets; 48 h between training sessions | % 1-RM | Yes | |
| 1x/week individual (US) | Log book/ participant + investigator | 1x/week home based | ||||||||||
| Foroughi, 2011 [66] | Fitness devices | Yes | N.A. (S) | Researcher/ participant | N.A. | ↑3% 1-RM | Yes/N.A. | In center | 3 sets; 8 reps (6–9 sec/rep); 80% 1 RM (equal to 15–18 on the Borg Rating of Perceived Exertion) Rest: 10–15 sec between reps; 1–2 min between sets C: minimal resistance; no progression | % 1-RM | Main protocol deviation: changing to an isometric form of training if the dynamic mode was causing pain, reducing the intensity of the intervention group and/ or limiting the range of motion | |
| Mangione, 1999 [67] | Cycle ergometer; heart rate monitor | N.A. | N.A. (S) | Researcher/ N.A. | N.A. | N.A. | Yes, except exercise progression/N.A. | In center | HI: 60 min (including warm-up and cool-down); 70% HR reserve LI: 60 min (including warm-up and cool-down); 40% HR reserve Target HR zone is reached by an increase in speed of pedaling instead of an increase in resistance | Maximum heart rate | Yes | |
| Bressel, 2014 [14] | Pool; water jet; aquatic treadmill | N.A. | N.A. (S) | Researcher/participant + investigator | Verbal motivation | Progression visualized in table in study article | Yes/N.A. | In center | 18–30 min; 3–6 reps HI: 14–19 RPE; 30 s–2 min 30 s Rest: 10 RPE; 1 min–1 min 30 s C: maintenance of typical activities of daily living; no new treatment | RPE | Yes | |
| Thorstensson, 2005 [68] | Heart rate monitor (not obligatory); Thera-band | Yes | Group (S) | Researcher/N.A. | N.A. | Gradual increase in intensity by increased lever arm or range of motion | Yes/yes | In center + home based | Weight-bearing exercises; 1 h; minimal 60% maximum HR | Maximum heart rate | Yes | |
| Waller, 2017 [69] | Pool; heart rate monitors; Thera-bands; Hydro-boots | Yes | Group (S) | Researcher/ investigator | N.A. | Progression from barefoot to small resistance fins and large resistance boots | Yes/N.A. | In center | 1 h (i.e., 15 min warm-up, 30 min intensive aquatic resistance training program, 10–15 min cool-down); as hard and fast as possible C: maintenance of usual leisure time activities with the possibility to participate in 2 sessions of 1 h, including light stretching, relaxation, social interaction | RPE, heart rate, blood lactates | Yes | |
| Calatayud, 2017 [70] | Fitness devices; Bosu® Balance Trainer | Yes | N.A. (S) | N.A./ N.A. | N.A. | Adding a maximum of 2 or 3 kg | Yes/N.A. | In center | 1 h (i.e., 15 min warm-up, 5 sets of 10 reps of each exercise, 5 min cool-down); 10-RM C: treatment including exercise which may explain the absence of between-group difference Rest: at least 48 h between sessions; 1 min between sets | 1-RM | Yes | |
| Messier, 2021 [71] | Nautilus resistance training machine; Thera-bands | Yes | Group (S) | Participant/ participant | Frequent contact; positive feedback; incentives; establishing personal commitment; promoting a sense of community | ↑ 5% 1-RM/ 2 weeks, based on 1-RM measurement (measured each 9 weeks) | Yes/Yes | In center | 60 min; 3 sets HI: 4–8 reps; 75–90% 1-RM LI: 15 reps; 30–40% 1-RM C: 60 min educational workshops and seated stretching 2x/month for the first 6 months and the other months 1x/month Rest: 60–90 sec between sets | % 1-RM | Yes | |
| Jan, 2008 [56] | Leg press machine; bicycle (warm-up); cold pack (after exercise) | Yes | Individual (S) | Researcher/ N.A. | N.A. | ↑5% 1-RM/ 2 weeks | Yes/N.A. | In center | HI: 30 min; 60% 1-RM; 3 sets; 8 reps LI: 50 min; 10% 1-RM; 10 sets; 15 reps C: no intervention Rest: 1 min between sets; 5 min between left and right knee sessions | %1-RM | Yes | |
| Study and Year | Exercise Modality | NOS; Age (Mean, Years); Sex (Female, n) | Groups | Exercise Duration & Sessions | Outcomes | Results | Drop-Out Rate |
|---|---|---|---|---|---|---|---|
| Golightly, 2021 [63] | CIT: cycling or walking | 29; 63 ± 7; 19 | I: High-intensity interval training (n = 29) | 12 weeks; 24 sessions; 2×/week | Adverse events; feasibility; physical function; knee OA symptoms; balance; muscle strength; cardiorespiratory fitness; body composition | 70% adherence No adverse events related to the program ↑ Physical function * ↓ Knee OA symptoms* ↑ Balance * ↑ Muscle strength * ↑ Cardiorespiratory fitness* Body composition: no significant changes | 27.59% |
| Smith-Ryan, 2020 [31] | CIT: cycling | 16; 59.9 ± 8.3; 12 | I: High-intensity interval training (n = 16) | 6 weeks; 12 exercise sessions + 2 testing sessions at baseline + 2 post-test sessions; 2×/week exercise sessions | Primary: feasibility Secondary: cardiorespiratory fitness (i.e., VO2peak); knee OA symptoms; circulating biomarkers of metabolism | Moderate feasibility: no adverse events related to the program, >96% adherence ↑ Cardiorespiratory fitness * ↓ Knee OA symptoms * ↓ Amino acids (i.e., methionine*, phenylalanine *, tyrosine*, serine) ↑ Aspartate/ asparagine ↓ Acylcarnitine | 18.75% |
| King, 2008 [57] | RT: lower extremity | 14; 48.35 ± 6.51; 2 | I: High-intensity training (n = 14) | 12 weeks; 36 sessions; 3×/week | Primary: knee extensor and flexor strength; pain; adherence Secondary: dynamic knee joint loading; patient-reported outcomes; self-efficacy after training | No adverse events ↑ Knee extensor and flexor strength * No increases in pain during or after training High adherence Dynamic knee joint loading and patient-reported outcomes: no significant changes ↑ Self-efficacy after training (i.e., function subscale) * | N.A. |
| Keogh, 2018 [64] | CIT: cycling | 27; 62.4 ± 8.3; 13 | I1: High-intensity interval training (n = 9) I2: Moderate-intensity continuous training (n = 8) | 8 weeks; 32 sessions; 4×/week | Primary: feasibility (i.e., enrolment rate, withdrawal rate, exercise adherence, number of adverse events) Secondary: efficacy (i.e., health-related quality of life, physical function, body composition) | 54% enrolment rate 37% rate of withdrawal Very high exercise adherence 28 adverse events (24 related to one HIIT participant) ↑ Health-related quality of life * ↑ Physical function * Body composition: no significant changes | 37% |
| De Zwart, 2022 [65] | RT: lower extremity | 177; 67.7 ± 5.8; 107 | I1: High-intensity training (n = 89) I2: Low-intensity training (n = 88) | 12 weeks; 36 sessions; 3×/week | Primary: isokinetic muscle strength; estimated 1-RM Secondary: knee pain; physical functioning; knee OA symptoms | No adverse events related to the program ↑ Isokinetic muscle strength ↑ estimated 1-RM ** ↓ Knee pain ↑ Physical functioning ↓ Knee OA symptoms | 6% |
| Foroughi, 2011 [66] | RT: lower extremity | 54; 64 ± 7; 54 | I1: High-intensity training (n = 26) I2: Low-intensity training (n = 28) | 6 months; 78 sessions; 3×/week | Primary: dynamic shank angles; knee adduction angles; knee adduction moment of the most symptomatic knee Secondary: muscle strength; gait speed; osteoarthritis symptoms | Two minor adverse events in the control group Dynamic shank angles: knee adduction angles, knee adduction moment: no change over time ↑ Muscle strength ** ↑ Gait speed * ↓Osteoarthritis symptoms * | 9% |
| Mangione, 1999 [67] | Cardio-respiratory continuous training: cycling | 39; 71 ± 6.9; 26 | I1: High-intensity training (n = 19) I2: Low-intensity training (n = 20) | 10 weeks; 30 sessions; 3×/week | Functional status; gait; overall and acute pain; aerobic capacity | ↑ Functional status * ↑ Gait * ↓ Overall pain * No increase in acute pain ↑ Aerobic capacity * | 7.8% |
| Bressel, 2014 [14] | CIT + balance training: aquatic treadmill | 18; 64.5 ± 10.2; 16 | I: High-intensity interval training (n = 18) C: Control group (n = 18) | High-intensity: 6 weeks; 2–3×/week Control: 4 weeks | Pain; balance; physical function; mobility | No adverse events related to the program ↓ Pain ** ↑ Balance ** ↑ Physical function ** ↑ Mobility ** | 0% |
| Thorstensson, 2005 [68] | RT: lower extremity | 61; 56 ± 6; 31 | I: High-intensity training (n = 30) C: Control (n = 31) | 6 weeks; 12 sessions; 2×/week | Primary: self-reported pain; function; knee-related quality of life Secondary: health status; functional performance | Self-reported pain and function: no significant differences between groups ↑ Quality of life ** (at 6 weeks and 6 months) ↑ Health status ** (at 6 weeks) ↑ Functional performance* | 8% |
| Waller, 2017 [69] | RT: aquatic | 87; 63.8 ± 2.4; 87 | I: High-intensity training (n = 43) C: Control (n = 44) | 16 weeks; 48 sessions; 3×/week | Primary: body composition; walking speed Secondary: leisure time physical activity | High adherence ↓ Fat mass ** (after 4 months intervention) Lean mass: no significant changes ↑ Walking speed ** (after 4 months intervention and 12 months follow-up) Leisure time physical activity: significant effect on fat mass loss | 2% (after 16 weeks) 13% (after 12-months follow-up) |
| Calatayud, 2017 [70] | RT: lower extremity | 50; I: 66.8 ± 4.8, C: 66.7 ± 3.1; 37 | I: High-intensity training (n = 25) C: Control (n = 25) | 8 weeks; 24 sessions; 3×/week | WOMAC; SF-36; VAS; isometric knee flexion; isometric knee extension; isometric hip abduction; active knee range of motion; functional tasks | ↓WOMAC ** ↑ SF-36 ** ↓VAS ** ↑ Isometric knee flexion ** ↑ Isometric knee extension ** ↑ Isometric hip abduction ** ↑ Active knee range of motion (i.e., flexion and extension) ** ↑ Functional tasks ** | 12% |
| Messier, 2021 [71] | RT: lower & upper extremity, core | 377; 65; 151 | I1: High-intensity training (n = 127) I2: Low-intensity training (n = 126) C: Control (n = 124) | 18 months; 3×/week | Primary: knee pain; knee joint compressive force Secondary: physical function; mobility; disease progression; thigh skeletal muscle volume; thigh fat volume; IL-6 serum levels; knee extensor strength; hip abductor strength | 29 nonserious adverse events related to the program No statistically significant difference between high-intensity and control group or high-intensity and low-intensity group | 25% |
| Jan, 2008 [56] | RT | 102; 63.3 ± 6.6 (high-intensity), 61.8 ± 7.1 (low-intensity), 62.8 ± 7.1 (control); 79 | I1: High-intensity training (n = 34) I2: Low-intensity training (n = 34) C: Control (n = 34) | 8 weeks; 24 sessions; 3×/week | Pain; function; walking time; muscle torque | ↓ Pain * ↑Function * ↓Walking time * ↑Muscle torque * No statistically significant differences between the high-intensity and low-intensity groups | 4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarantino, D.; Theysmans, T.; Mottola, R.; Verbrugghe, J. High-Intensity Training for Knee Osteoarthritis: A Narrative Review. Sports 2023, 11, 91. https://doi.org/10.3390/sports11040091
Tarantino D, Theysmans T, Mottola R, Verbrugghe J. High-Intensity Training for Knee Osteoarthritis: A Narrative Review. Sports. 2023; 11(4):91. https://doi.org/10.3390/sports11040091
Chicago/Turabian StyleTarantino, Domiziano, Tine Theysmans, Rosita Mottola, and Jonas Verbrugghe. 2023. "High-Intensity Training for Knee Osteoarthritis: A Narrative Review" Sports 11, no. 4: 91. https://doi.org/10.3390/sports11040091
APA StyleTarantino, D., Theysmans, T., Mottola, R., & Verbrugghe, J. (2023). High-Intensity Training for Knee Osteoarthritis: A Narrative Review. Sports, 11(4), 91. https://doi.org/10.3390/sports11040091