Motor Skill Improvement in Preschoolers: How Effective Are Activity Cards?

Abstract
:1. Introduction
2. Methods
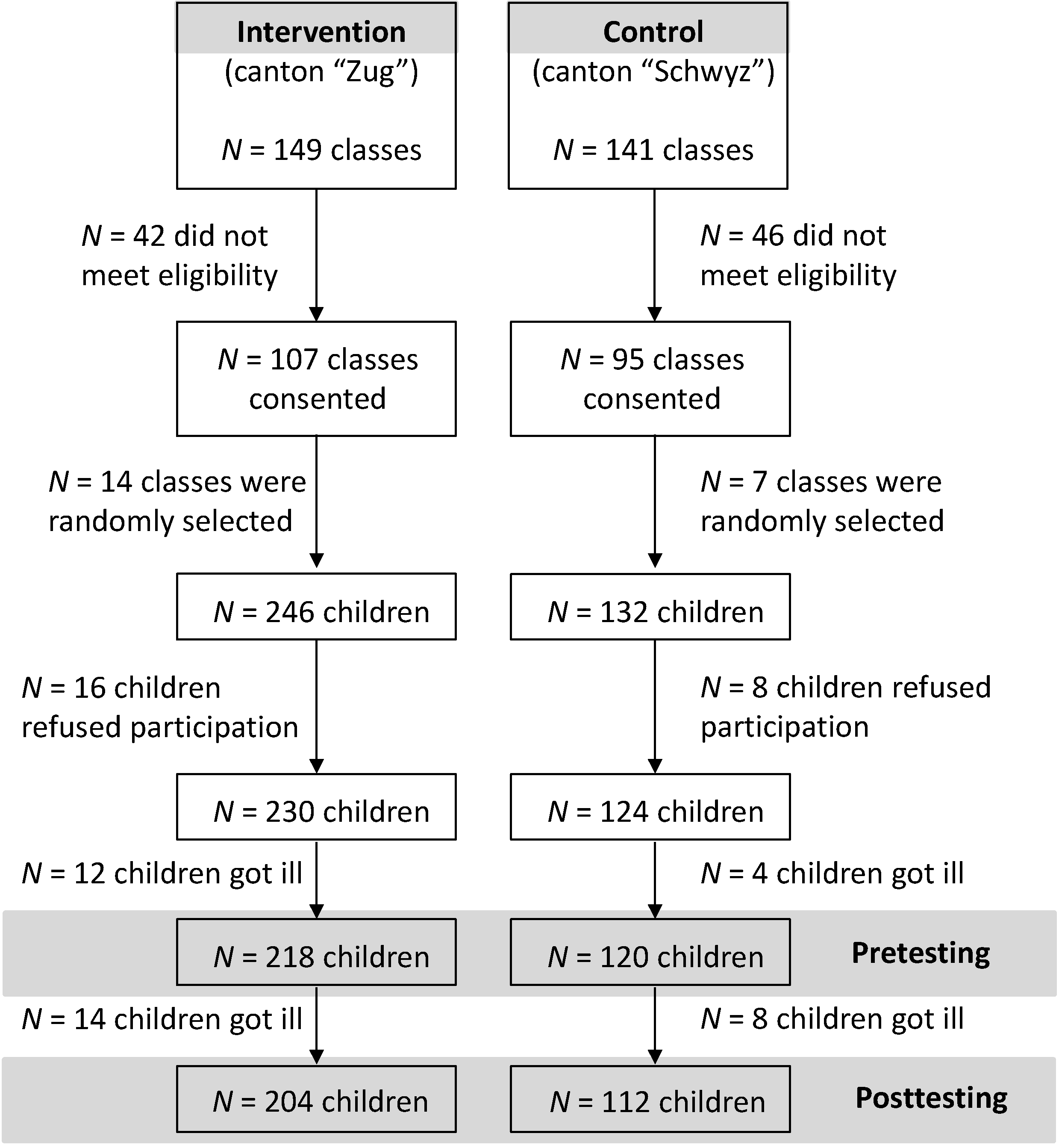
2.1. Study Design
2.2. Participants

2.3. Anthropometrics
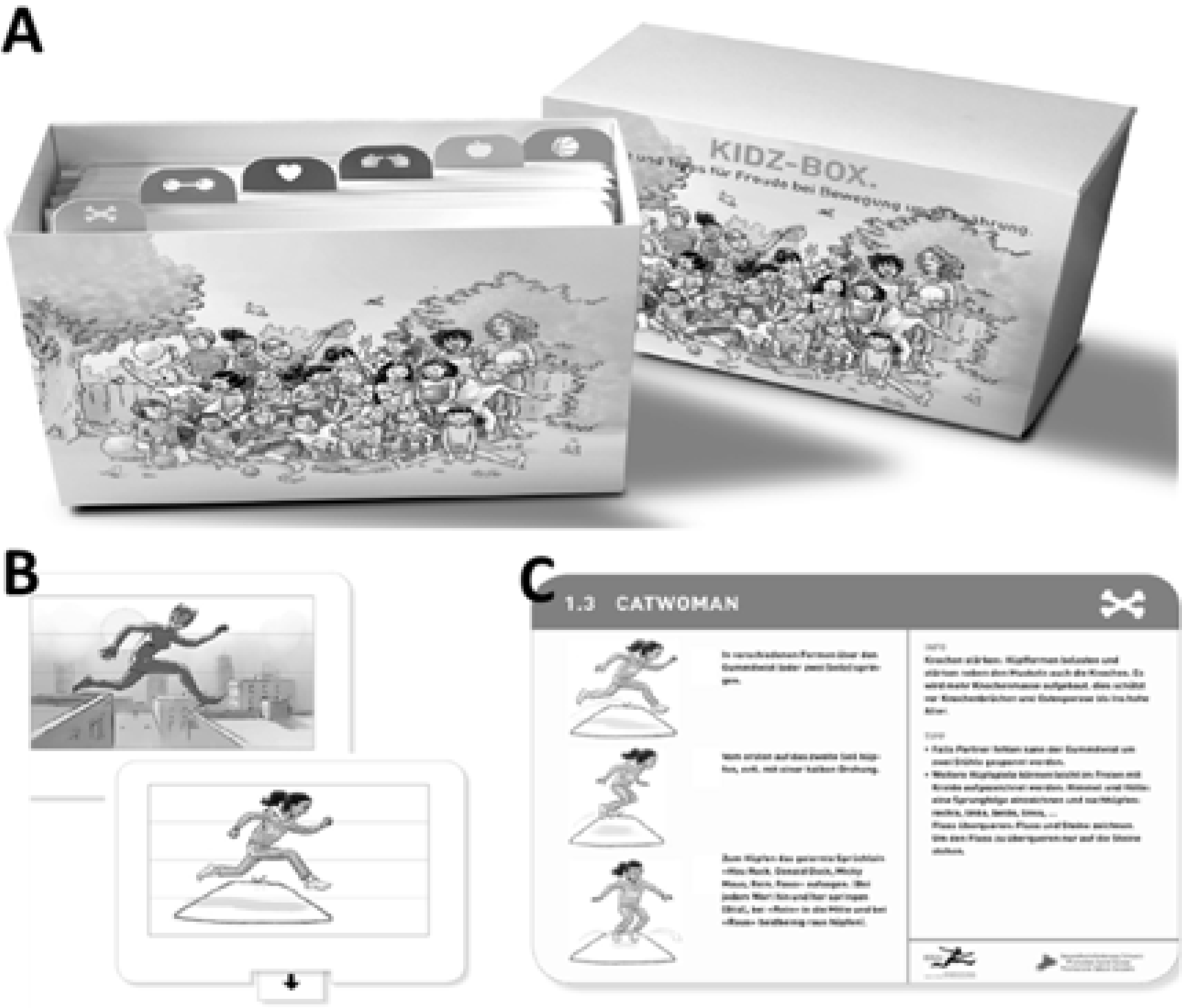
2.4. KIDZ-Box® Intervention

2.5. Motor Skill Testing
2.5.1. Agility
2.5.2. Jumping Performance
2.5.3. Balance
3. Statistics
4. Results

{kind=link}
{kind=link}
{kind=link}
| INT (N = 107) | CON (N = 107) | |
|---|---|---|
| Gender (n, female/male) | 64/43 | 64/43 |
| Age (years) | 5.5 ± 0.6 | 5.4 ± 0.6 |
| Height (m) | 1.13 ± 0.06 | 1.14 ± 0.06 |
| Weight (kg) | 20.0 ± 2.7 | 20.6 ± 3.7 |
| BMI (kg m−2) | 15.5 ± 1.2 | 15.7 ± 2.1 |
| Obese N (%) | 0 (0) | 5 (4.7) |
| Overweight N (%) | 5 (4.7) | 5 (4.7) |
4.1. Cross-Sectional Association between Motor Skills, Sex and Overweight
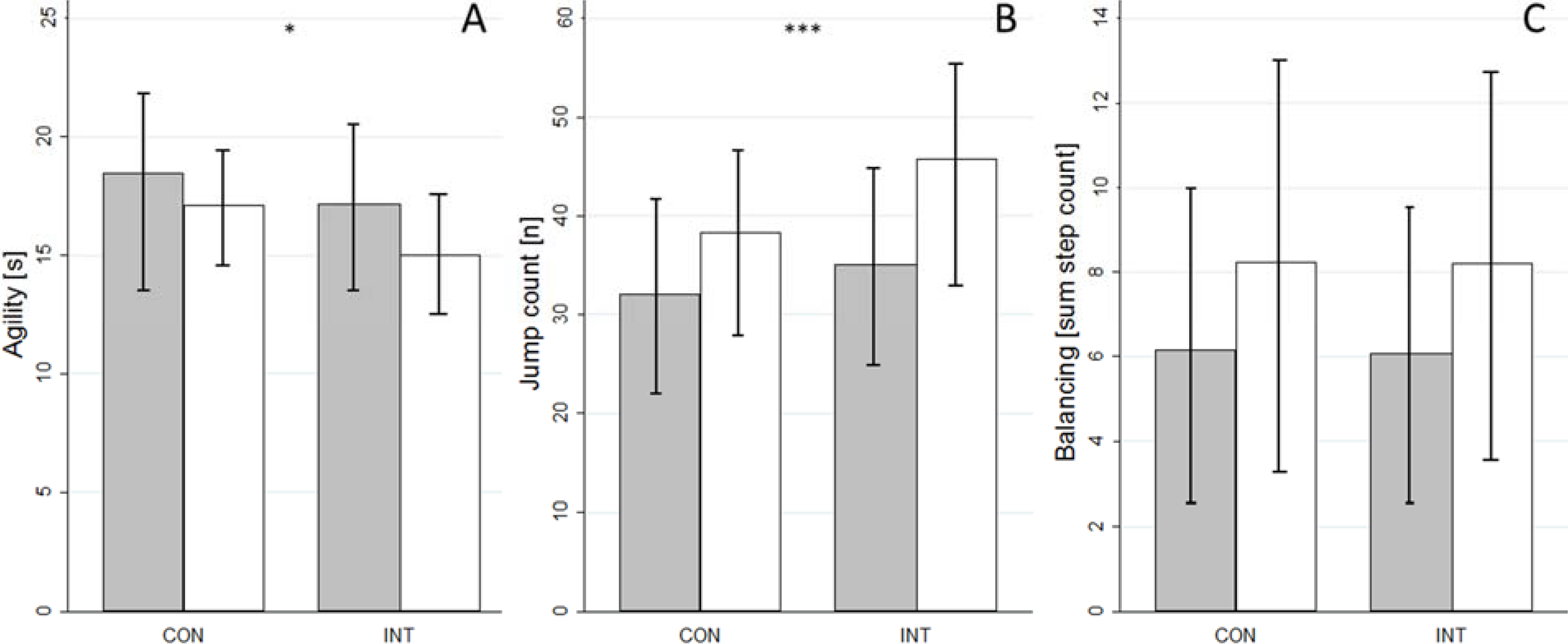
4.2. Interventional Changes of Anthropometry and Motor Skill Parameters
| Parameter | INT (N = 107) | CON (N = 107) | p (time) | ηp2 | p (treatment × time) | ηp2 | ||
|---|---|---|---|---|---|---|---|---|
| Pretest | Posttest | Pretest | Posttest | |||||
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |||||
| BMI (kg·m−2) * | 15.5 (1.2) | 15.6 (1.3) | 15.7 (2.1) | 15.7 (2.1) | 0.3 | 0.005 | 0.5 | 0.002 |
| Agility (s) | 17.2 (3.2) | 15.0 (2.4) | 18.5 (4.1) | 17.1 (2.6) | <0.001 | 0.3 | 0.03 | 0.02 |
| Side-to-side jumping (jump count) | 35.1 (10.9) | 45.8 (10.0) | 32.0 (3.5) | 38.3 (10.0) | <0.001 | 0.6 | <0.001 | 0.09 |
| Balancing (sum of step count) | 8.1 (3.7) | 8.2 (4.5) | 6.2 (3.8) | 8.2 (4.7) | <0.001 | 0.2 | 0.9 | <0.001 |

5. Discussion
5.1. Main Results
5.2. Associations of Motor Skills with Overweight and Sex
5.3. Interventional Changes in Motor Skills and Anthropometry
5.4. Strengths and Limitations
6. Conclusions and Perspectives
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wang, Y.; Lobstein, T. Worldwide trends in childhood overweight and obesity. Int. J. Pediatr. Obes. 2006, 1, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Aeberli, I.; Henschen, I.; Molinari, L.; Zimmermann, M.B. Stabilization of the prevalence of childhood obesity in Switzerland. Swiss Med. Wkly. 2010, 140, 1–3. [Google Scholar]
- Singh, A.S.; Mulder, C.; Twisk, J.W.; van Mechelen, W.; Chinapaw, M.J. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyachi, M.; Kawano, H.; Sugawara, J.; Takahashi, K.; Hayashi, K.; Yamazaki, K.; Tabata, I.; Tanaka, H. Unfavorable effects of resistance training on central arterial compliance: A randomized intervention study. Circulation 2004, 110, 2858–2863. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Health Improvement and Protection. In Start Active, Stay Active: A Report on Physical Activity from the Four Home Countries’ Chief Medical Officers; Department of Health: London, UK, 2011. [Google Scholar]
- Tremblay, M.S.; Leblanc, A.G.; Carson, V.; Choquette, L.; Connor Gorber, S.; Dillman, C.; Duggan, M.; Gordon, M.J.; Hicks, A.; Janssen, I.; et al. Canadian physical activity guidelines for the early years (aged 0–4 years). Appl. Physiol. Nutr. Metab. 2012, 37, 345–369. [Google Scholar] [CrossRef] [PubMed]
- Tucker, P. The physical activity levels of preschool-aged children: A systematic review. Early Child. Res. Q. 2008, 23, 547–558. [Google Scholar] [CrossRef]
- Reilly, J.J. Physical activity, sedentary behaviour and energy balance in the preschool child: Opportunities for early obesity prevention. Proc. Nutr. Soc. 2008, 67, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Burgi, F.; Meyer, U.; Granacher, U.; Schindler, C.; Marques-Vidal, P.; Kriemler, S.; Puder, J.J. Relationship of physical activity with motor skills, aerobic fitness and body fat in preschool children: A cross-sectional and longitudinal study (Ballabeina). Int. J. Obes. Lond. 2011, 35, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Eliakim, A.; Nemet, D.; Balakirski, Y.; Epstein, Y. The effects of nutritional-physical activity school-based intervention on fatness and fitness in preschool children. J. Pediatr. Endocrinol. Metab. 2007, 20, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Kelly, L.; Montgomery, C.; Williamson, A.; Fisher, A.; McColl, J.H.; Lo Conte, R.; Paton, J.Y.; Grant, S. Physical activity to prevent obesity in young children: Cluster randomised controlled trial. BMJ 2006, 333, 1041. [Google Scholar] [CrossRef] [PubMed]
- Okely, A.D.; Booth, M.L.; Chey, T. Relationships between body composition and fundamental movement skills among children and adolescents. Res. Q. Exerc. Sport 2004, 75, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.; Reilly, J.J.; Kelly, L.A.; Montgomery, C.; Williamson, A.; Paton, J.Y.; Grant, S. Fundamental movement skills and habitual physical activity in young children. Med. Sci. Sports Exerc. 2005, 37, 684–688. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.S.; Vaughn, A.; McWilliams, C.; Hales, D. Interventions for increasing physical activity at child care. Med. Sci. Sports Exerc. 2010, 42, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Okely, A.D.; Booth, M.L. Mastery of fundamental movement skills among children in New South Wales: Prevalence and sociodemographic distribution. J. Sci. Med. Sport 2004, 7, 358–372. [Google Scholar] [CrossRef] [PubMed]
- Logan, S.W.; Robinson, L.E.; Wilson, A.E.; Lucas, W.A. Getting the fundamentals of movement: A meta-analysis of the effectiveness of motor skill interventions in children. Child Care Health Dev. 2012, 38, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef] [PubMed]
- Roth, K.; Mauer, S.; Obinger, M.; Ruf, K.C.; Graf, C.; Kriemler, S.; Lenz, D.; Lehmacher, W.; Hebestreit, H. Prevention through Activity in Kindergarten Trial (PAKT): A cluster randomised controlled trial to assess the effects of an activity intervention in preschool children. BMC Public Health 2010, 10, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgi, F.; Niederer, I.; Schindler, C.; Bodenmann, P.; Marques-Vidal, P.; Kriemler, S.; Puder, J.J. Effect of a lifestyle intervention on adiposity and fitness in socially disadvantaged subgroups of preschoolers: A cluster-randomized trial (Ballabeina). Prev. Med. 2012, 54, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Niederer, I.; Kriemler, S.; Zahner, L.; Bürgi, F.; Ebenegger, V.; Hartmann, T.; Meyer, U.; Schindler, C.; Nydegger, A.; Marques-Vidal, P.; et al. Influence of a lifestyle intervention in preschool children on physiological and psychological parameters (Ballabeina): Study design of a cluster randomized controlled trial. BMC Public Health 2009, 9, 94. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavior Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Ehmig, S.; Dunkel, A.; Lenares, J. Evaluation des Modulprojekts Kidz-Box im Kanton Zug; Health Promotion Switzerland: Lugano, Switzerland, 2009. [Google Scholar]
- Castetbon, K.; Andreyeva, T. Obesity and motor skills among 4 to 6-year-old children in the United States: Nationally-representative surveys. BMC Pediatr. 2012, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Wirth, B.; Knecht, C.; Humphreys, K. Spine day 2012: Spinal pain in Swiss school children- epidemiology and risk factors. BMC Pediatr. 2013, 13, 159. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.A.; Okely, A.D.; Gregory, P.; Cliff, D.P. Relationships between weight status and child, parent and community characteristics in preschool children. Int. J. Pediatr. Obes. 2009, 4, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Graf, C.; Koch, B.; Kretschmann-Kandel, E.; Falkowski, G.; Christ, H.; Coburger, S.; Lehmacher, W.; Bjarnason-Wehrens, B.; Platen, P.; Tokarski, W.; et al. Correlation between BMI, leisure habits and motor abilities in childhood (CHILT-project). Int. J. Obes. Relat. Metab. Disord. 2004, 28, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Morano, M.; Colella, D.; Caroli, M. Gross motor skill performance in a sample of overweight and non-overweight preschool children. Int. J. Pediatr. Obes. 2011, 6 (Suppl. 2), 42–46. [Google Scholar] [CrossRef]
- Wearing, S.C.; Hennig, E.M.; Byrne, N.M.; Steele, J.R.; Hills, A.P. The impact of childhood obesity on musculoskeletal form. Obes. Rev. 2006, 7, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Hondt, E.; Deforche, B.; de Bourdeaudhuij, I.; Lenoir, M. Relationship between motor skill and body mass index in 5- to 10-year-old children. Adapt Phys. Activ. Q. 2009, 26, 21–37. [Google Scholar] [PubMed]
- Thomas, J.R.; French, K.E. Gender differences across age in motor performance a meta-analysis. Psychol. Bull. 1985, 98, 260–282. [Google Scholar] [CrossRef] [PubMed]
- Matthiass, H. Reifung, Wachstum und Wachstumsstörungen des Haltungs-und Bewegungsapparates im Jugendalter; Karger: Basel, Switzerland, 1966; p. 113. [Google Scholar]
- Baquet, G.; Stratton, G.; van Praagh, E.; Berthoin, S. Improving physical activity assessment in prepubertal children with high-frequency accelerometry monitoring: A methodological issue. Prev. Med. 2007, 44, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.C.; Olson, J.; Pepper, S.L.; Porszasz, J.; Barstow, T.J.; Cooper, D.M. The level and tempo of children’s physical activities: An observational study. Med. Sci. Sports Exerc. 1995, 27, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Meyer, U.; Romann, M.; Zahner, L.; Schindler, C.; Puder, J.J.; Kraenzlin, M.; Rizzoli, R.; Kriemler, S. Effect of a general school-based physical activity intervention on bone mineral content and density: A cluster-randomized controlled trial. Bone 2011, 48, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical acitivity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Vandorpe, B.; Vandendriessche, J.; Vaeyens, R.; Pion, J.; Matthys, S.; Lefevre, J.; Philippaerts, R.; Lenoir, M. Relationship between sports participation and the level of motor coordination in childhood: A longitudinal approach. J. Sci. Med. Sport 2012, 15, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Zahner, L.; Muehlbauer, T.; Schmid, M.; Meyer, U.; Puder, J.J.; Kriemler, S. Association of sports club participation with fitness and fatness in children. Med. Sci. Sports Exerc. 2009, 41, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Jaakkola, T.; Kalaja, S.; Liukkonen, J.; Jutila, A.; Virtanen, P.; Watt, A. Relations among physical activity patterns, lifestyle activities, and fundamental movement skills for Finnish students in grade 7. Percept. Mot. Skills 2009, 108, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Michaleff, Z.A.; Kamper, S.J.; Maher, C.G.; Evans, R.; Broderick, C.; Henschke, N. Low back pain in children and adolescents: A systematic review and meta-analysis evaluating the effectiveness of conservative interventions. Eur. Spine J. 2014, 23, 2046–2058. [Google Scholar] [CrossRef] [PubMed]
- Waddell, G. The Back Pain Revolution; Churchill Livingstone: Edinburgh, UK, 1998; Volume 2, p. 438. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donath, L.; Imhof, K.; Roth, R.; Zahner, L. Motor Skill Improvement in Preschoolers: How Effective Are Activity Cards? Sports 2014, 2, 140-151. https://doi.org/10.3390/sports2040140
Donath L, Imhof K, Roth R, Zahner L. Motor Skill Improvement in Preschoolers: How Effective Are Activity Cards? Sports. 2014; 2(4):140-151. https://doi.org/10.3390/sports2040140
Chicago/Turabian StyleDonath, Lars, Katharina Imhof, Ralf Roth, and Lukas Zahner. 2014. "Motor Skill Improvement in Preschoolers: How Effective Are Activity Cards?" Sports 2, no. 4: 140-151. https://doi.org/10.3390/sports2040140
APA StyleDonath, L., Imhof, K., Roth, R., & Zahner, L. (2014). Motor Skill Improvement in Preschoolers: How Effective Are Activity Cards? Sports, 2(4), 140-151. https://doi.org/10.3390/sports2040140