
Reliability and Validity of the Early Years Physical Activity Questionnaire (EY-PAQ)


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
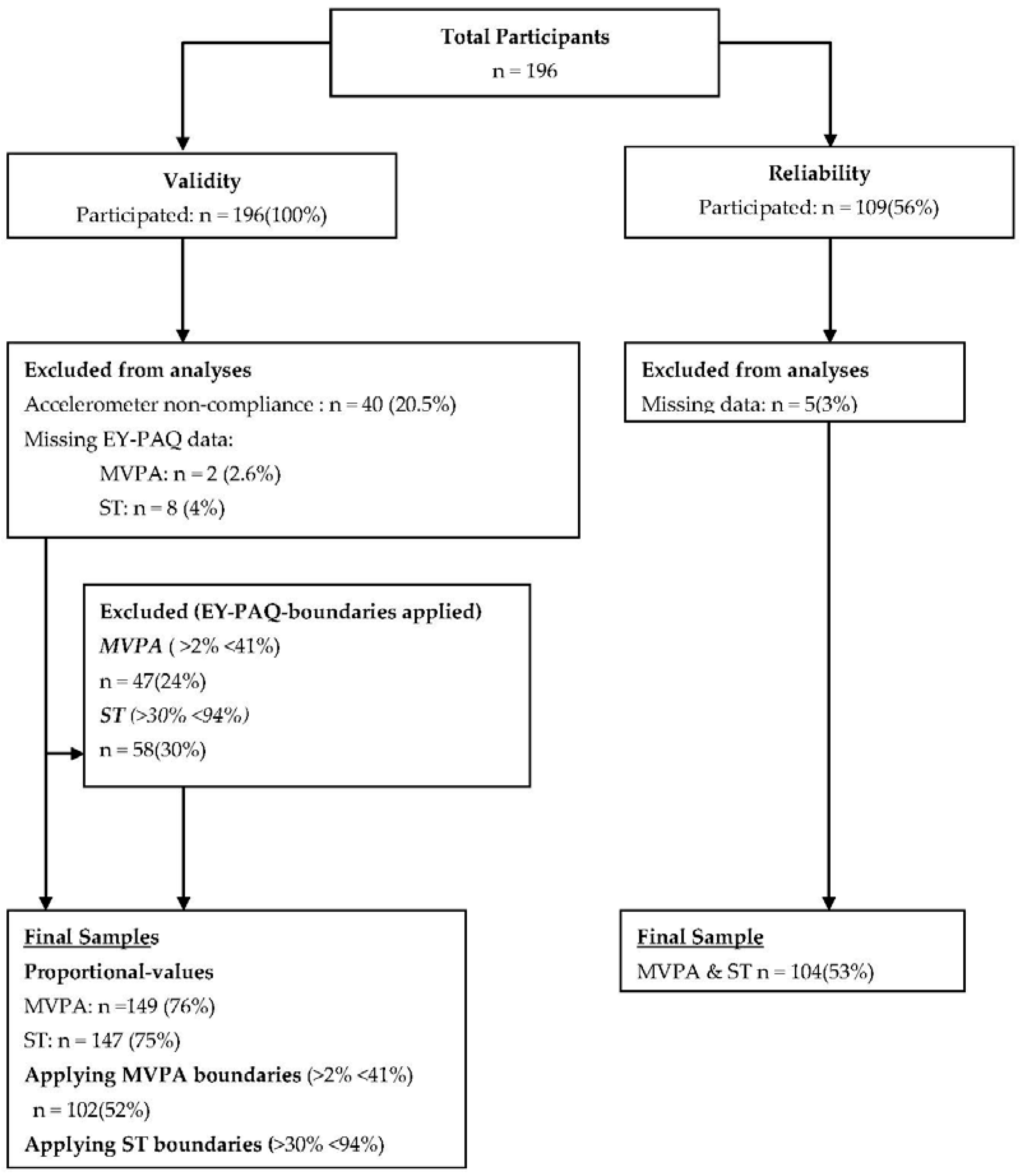
2.1. Participants and Setting
2.2. Procedure
2.3. Measures
2.3.1. The Early Years Physical Activity Questionnaire (EY-PAQ)
2.3.2. Accelerometry
2.4. Data Analysis
3. Results
3.1. Reliability
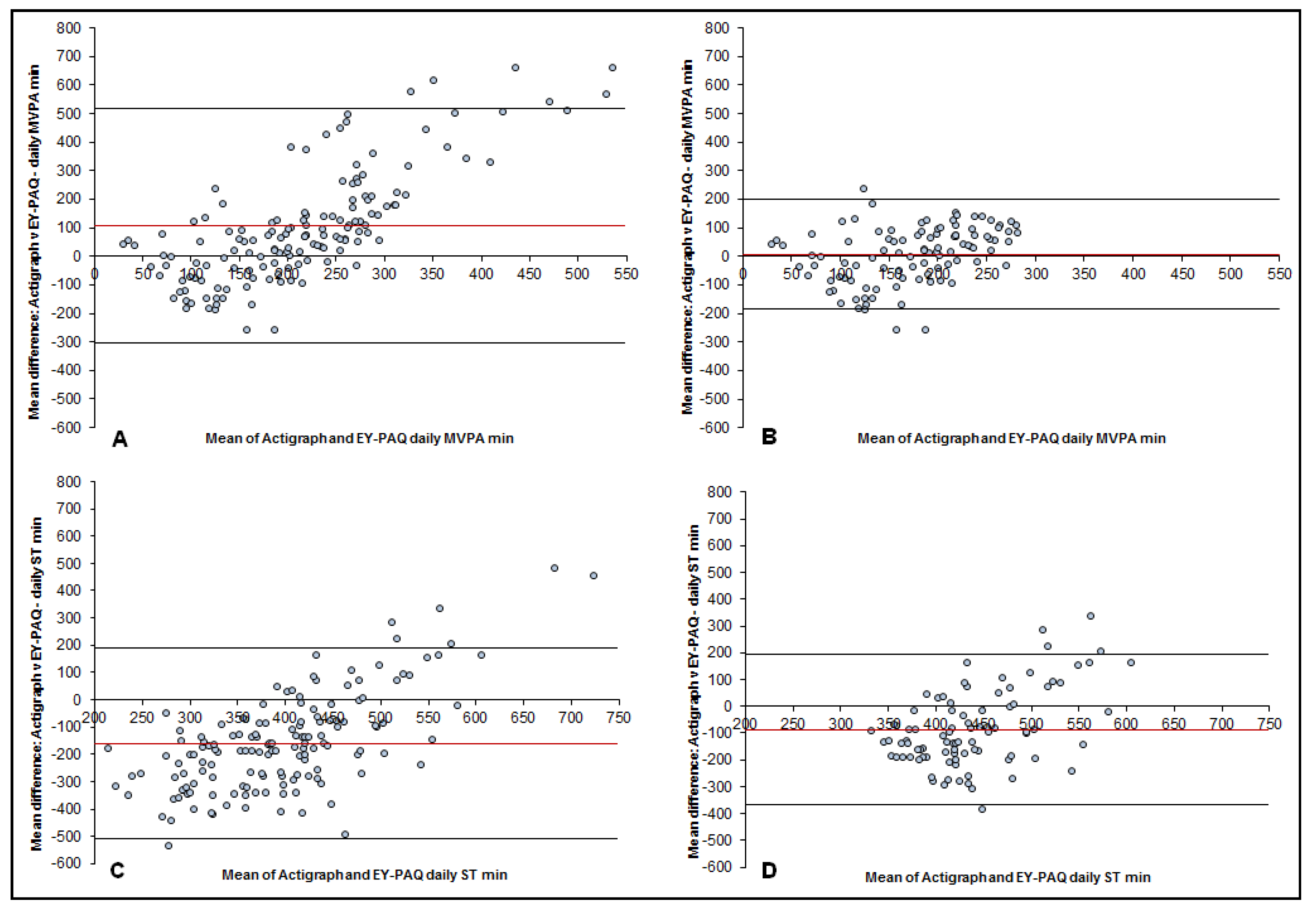
3.2. Validity
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| EY-PAQ | Early Years Physical Activity Questionnaire |
| TPA | Total Physical Activity |
| MVPA | Moderate to Vigorous Physical Activity |
| ST | Sedentary Time |
| BiB | Born in Bradford |
References
- Australian Government Department of Health and Ageing. Physical Activity Recommendations for Children 0–5; Australian Government Department of Health and Ageing: Canberra, Australia, 2009.
- Reilly, J.; Okely, A.; Almond, L.; Cardon, G.; Prosser, L. Making the Case for UK Physical Activity Guidelines for Early Years: Recommendations and Draft Summary Statements Based on the current Evidence; UK government: London, UK, 2011.
- Timmons, B.W.; LeBlanc, A.G.; Carson, V.; Gorber, S.C.; Dillman, C.; Janssen, I.; Kho, M.E.; Spence, J.C.; Stearns, J.A.; Tremblay, M.S. Systematic review of physical activity and health in the early years (aged 0–4 years). Appl. Physiol. Nutr. Metab. 2012, 37, 773–792. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Larouche, R.; Colley, R.C.; Goldfield, G.; Gorber, S.C. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Hildebrand, M.; Collings, P.J. Physical activity, sedentary time and adiposity during the first two decades of life. Proc. Nutr. Soc. 2014, 73, 319–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet, W. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpaa, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.; Raitakari, O.T. Tracking of physical activity from early childhood through youth into adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Telama, R.; Yang, X.; Viikari, J.; Valimaki, I.; Wanne, O.; Raitakari, O. Physical activity from childhood to adulthood: A 21-year tracking study. Am. J. Prev. Med. 2005, 28, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef] [PubMed]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.A.; Hinkley, T.; Okely, A.D.; Salmon, J. Tracking Physical Activity and Sedentary Behavior in Childhood A Systematic Review. Am. J. Prev. Med. 2013, 44, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Cliff, D.P.; Reilly, J.J.; Okely, A.D. Methodological considerations in using accelerometers to assess habitual physical activity in children aged 0–5 years. J. Sci. Med. Sport 2009, 12, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Almeida, M.J.; McIver, K.L.; Pfeiffer, K.A.; Dowda, M. Validation and calibration of an accelerometer in preschool children. Obesity 2006, 14, 2000–2006. [Google Scholar] [CrossRef] [PubMed]
- Cain, K.L.; Sallis, J.F.; Conway, T.L.; van Dyck, D.; Calhoon, L. Using accelerometers in youth physical activity studies: A review of methods. J. Phys. Act. Health 2013, 10, 437–450. [Google Scholar] [PubMed]
- Hnatiuk, J.A.; Salmon, J.; Hinkley, T.; Okely, A.D.; Trost, S. A review of preschool children’s physical activity and sedentary time using objective measures. Am. J. Prev. Med. 2014, 47, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.-M.; Shiroma, E.J. Using accelerometers to measure physical activity in large-scale epidemiological studies: Issues and challenges. Br. J. Sports Med. 2014, 48, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Oliver, M.; Schofield, G.M.; Kolt, G.S. Physical activity in preschoolers: Understanding prevalence and measurement issues. Sports Med. 2007, 37, 1045–1070. [Google Scholar] [CrossRef] [PubMed]
- Fulton, J.E.; Burgeson, C.R.; Perry, G.R.; Sherry, B.; Galuska, D.A.; Alexander, M.P.; Wechsler, H.; Caspersen, C.J. Assessment of Physical Activity and Sedentary Behavior in Preschool-Age Children: Priorities for Research. Pediatr. Exerc. Sci. 2001, 13, 113–126. [Google Scholar]
- Taveras, E.M.; Gillman, M.W.; Kleinman, K.; Rich-Edwards, J.W.; Rifas-Shiman, S.L. Racial/ethnic differences in early life risk factors for childhood obesity. Pediatrics 2010, 125. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.; Khurana, L.; Vikram, N.K.; Goel, A.; Wasir, J.S. Metabolic syndrome in children: Current issues and South Asian perspective. Nutrition 2007, 23, 895–910. [Google Scholar] [CrossRef] [PubMed]
- Bhopal, R. Epidemic of cardiovascular disease in South Asians: Prevention must start in childhood. Br. Med. J. 2002, 324, 625–626. [Google Scholar] [CrossRef]
- Bhopal, R. What is the risk of coronary heart disease in South Asians? A review of UK research. J. Public Health Med. 2000, 22, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.; Small, N.; Raynor, P.; Tuffnell, D.; Bhopal, R.; Cameron, N.; Fairley, L.; Lawlor, D.A.; Parslow, R.; Petherick, E.S.; Pickett, K.E.; Waiblinger, D.; West, J.; Born, G. Cohort profile: The Born in Bradford multi-ethnic family cohort study. Int. J. Epidemiol. 2013, 42, 978–991. [Google Scholar] [CrossRef] [PubMed]
- Bryant, M.; Santorelli, G.; Fairley, L.; West, J.; Lawlor, D.A.; Bhopal, R.; Petherick, E.; Sahota, P.; Hill, A.; Cameron, N.; et al. Design and characteristics of a new birth cohort, to study the early origins and ethnic variation of childhood obesity: The BiB1000 study. Longitud. Life Course Stud. 2013, 4, 119–135. [Google Scholar]
- Barber, S.E.; Jackson, C.; Akhtar, S.; Bingham, D.D.; Ainsworth, H.; Hewitt, C.; Richardson, G.; Summerbell, C.D.; Pickett, K.E.; Moore, H.J.; et al. “Pre-schoolers in the playground” an outdoor physical activity intervention for children aged 18 months to 4 years old: Study protocol for a pilot cluster randomised controlled trial. Trials 2013, 14, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raynor, P. Born in Bradford, a cohort study of babies born in Bradford, and their parents: Protocol for the recruitment phase. BMC Public Health 2008, 8, 327–339. [Google Scholar] [PubMed]
- Dwyer, G.M.; Hardy, L.L.; Peat, J.K.; Baur, L.A. The validity and reliability of a home environment preschool-age physical activity questionnaire (Pre-PAQ). Int. J. Behav. Nutr. Phys. Act. 2011, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Collings, P.J.; Brage, S.; Ridgway, C.L.; Harvey, N.C.; Godfrey, K.M.; Inskip, H.M.; Cooper, C.; Wareham, N.J.; Ekelund, U. Physical activity intensity, sedentary time, and body composition in preschoolers. Am. J. Clin. Nutr. 2013, 97, 1020–1028. [Google Scholar] [CrossRef] [PubMed]
- Saint-Maurice, P.F.; Welk, G.J.; Beyler, N.K.; Bartee, R.T.; Heelan, K.A. Calibration of self-report tools for physical activity research: The Physical Activity Questionnaire (PAQ). BMC Public Health 2014, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Helmerhorst, H.J.F.; Brage, S.; Warren, J.; Besson, H.; Ekelund, U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int. J. Behav. Nutr. Phys. Act. 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.; Barber, S.E.; Cameron, N.; Clemes, S.A. Calibration and validation of the ActiGraph GT3X+ in 2–3 year olds. J. Sci. Med. Sport 2014, 17, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Addy, C.L.; Trilk, J.L.; Dowda, M.; Byun, W.; Pate, R.R. Assessing Preschool Children’s Physical Activity: How Many Days of Accelerometry Measurement. Pediatr. Exerc. Sci. 2014, 26, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Hnatiuk, J.; Ridgers, N.D.; Salmon, J.; Campbell, K.; McCallum, Z.; Hesketh, K. Physical Activity Levels and Patterns of 19-Month-Old Children. Med. Sci. Sports Exerc. 2012, 44, 1715–1720. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.; Barber, S.E.; Griffiths, P.L.; Cameron, N.; Clemes, S.A. Qualitative feasibility of using three accelerometers with 2–3-year-old children and both parents. Res. Q. Exerc. Sport 2013, 84, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Costa, S. The Measurement of Physical Activity and Sedentary Behaviour in a Sample of 2 to 3 Year Old South Asian and White British Children; Loughborough Univeristy: Leicestershire, UK, 2014. [Google Scholar]
- Metcalf, B.S.; Jeffery, A.N.; Hosking, J.; Voss, L.D.; Sattar, N.; Wilkin, T.J. Objectively Measured Physical Activity and Its Association With Adiponectin and Other Novel Metabolic Markers A Longitudinal study in children (EarlyBird 38). Diabetes Care 2009, 32, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Fees, B.S.; Haar, S.J.; Murray, A.D.; Crowe, L.K. Identification and validity of accelerometer cut-points for toddlers. Obesity 2012, 20, 2317–2319. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, M.; Lancaster, G.A.; Umar, E.; Nyirenda, M.; Kayira, E.; van den Broek, N.R.; Smyth, R.L. The Malawi Developmental Assessment Tool (MDAT): The Creation, Validation, and Reliability of a Tool to Assess Child Development in Rural African Settings. PLoS Med. 2010, 7, e1000273. [Google Scholar] [CrossRef] [PubMed]
- Bingham, D.D.; Costa, S.; Clemes, S.A.; Routen, A.C.; Moore, H.J.; Barber, S.E. Accelerometer data requirements for reliable estimation of habitual physical activity and sedentary time of children during the early years—A worked example following a stepped approach. J. Sports Sci. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use; OUP Oxford: Oxford, UK, 2008. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- London, K.C. Q9.10 What Size of Index Indicates “Good Reliability”? Available online: http://www.kcl.ac.uk/ioppn/depts/biostatistics/SAS/faqs9.aspx#a9_2 (accessed on 2 Februray 2016).
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Corder, K.; van Sluijs, E.M.F.; Wright, A.; Whincup, P.; Wareham, N.J.; Ekelund, U. Is it possible to assess free-living physical activity and energy expenditure in young people by self-report? Am. J. Clin. Nutr. 2009, 89, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Nevill, A.M. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Hinkley, T.; Salmon, J.; Okely, A.D.; Crawford, D.; Hesketh, K. Preschoolers’ physical activity, screen time, and compliance with recommendations. Med. Sci. Sports Exerc. 2012, 44, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Lobo, Y.B.; Winsler, A. The effects of a creative dance and movement program on the social competence of head start preschoolers. Soc. Dev. 2006, 15, 501–519. [Google Scholar] [CrossRef]
- Hart, T.L.; Ainsworth, B.E.; Tudor-Locke, C. Objective and subjective measures of sedentary behavior and physical activity. Med. Sci. Sports Exerc. 2011, 43, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Atkin, A.J.; Gorely, T.; Clemes, S.A.; Yates, T.; Edwardson, C.; Brage, S.; Salmon, J.; Marshall, S.J.; Biddle, S.J. Methods of Measurement in epidemiology: Sedentary Behaviour. Int. J. Epidemiol. 2012, 41, 1460–1471. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, K.; McMinn, A.; Ekelund, U.; Sharp, S.; Collings, P.; Harvey, N.; Godfrey, K.; Inskip, H.; Cooper, C.; van Sluijs, E. Objectively measured physical activity in four-year-old British children: A cross-sectional analysis of activity patterns segmented across the day. Int. J. Behav. Nutr. Phys. Act. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Collings, P.J.; Wijndaele, K.; Corder, K.; Westgate, K.; Ridgway, C.L.; Dunn, V.; Goodyer, I.; Ekelund, U.; Brage, S. Levels and patterns of objectively-measured physical activity volume and intensity distribution in UK adolescents: The ROOTS study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 23–23. [Google Scholar] [CrossRef] [PubMed]
- Hinkley, T.; O’Connell, E.; Okely, A.D.; Crawford, D.; Hesketh, K.; Salmon, J. Assessing volume of accelerometry data for reliability in preschool children. Med. Sci. Sports Exerc. 2012, 44, 2436–2441. [Google Scholar] [CrossRef] [PubMed]
- Hislop, J.; Law, J.; Rush, R.; Grainger, A.; Bulley, C.; Reilly, J.J.; Mercer, T. An investigation into the minimum accelerometry wear time for reliable estimates of habitual physical activity and definition of a standard measurement day in pre-school children. Physiol. Meas. 2014, 35, 2213–2228. [Google Scholar] [CrossRef] [PubMed]
- Collings, P.J.; Brage, S.; Bingham, D.D.; Costa, S.; West, J.; McEachan, R.R.C.; Wright, J.; Barber, S.E.; Bradford Institute for Health Research, Bradford, UK. Unpublished work. 2016.



{kind=link}
{kind=link}
| Demographic and Outcome Variables | All * | Validity ** | Reliability | |||||
|---|---|---|---|---|---|---|---|---|
| n = 196 | ST (n = 89) *** | MVPA (n = 102) **** | n = 104 | |||||
| n (%) | Mean (SD) | n (%) | Mean (SD) | n (%) | Mean (SD) | n (%) | Mean (SD) | |
| Sex | ||||||||
| Boys | 99 (50.5) | 47 (52.8) | 56 (54.9) | 52 (48) | ||||
| Girls | 97 (49.5) | 42 (47.2) | 46 (45.1) | 57 (53) | ||||
| Ethnicity | ||||||||
| White British | 82 (41.8) | 30 (33.7) | 37 (36.3) | 33 (30) | ||||
| South Asian | 96 (49) | 52 (58.4) | 55 (53.9) | 67 (62) | ||||
| Other | 18 (9.2) | 7 (7.9) | 10 (9.8) | 9 (8) | ||||
| Age | ||||||||
| Years | 3.2 (0.8) | 3.2 (0.8) | 3.2 (0.8) | 3.3 (0.8) | ||||
| Language | ||||||||
| English | 156 (79.6) | 69 (77.5) | 84 (82.4) | 82 (75) | ||||
| Urdu | 40 (20.4) | 20 (22.5) | 18 (17.6) | 27 (25) | ||||
| EY-PAQ | ||||||||
| Proportion estimates (%) | 47.0 (13.6) | 21.2 (11) | ||||||
| Actigraph GT3X+ | ||||||||
| Wear time (min per day) | 594.8 (100.7) | 582.1 (127.3) | ||||||
| Minutes per day | 344.1 (88.0) | 118.4 (7.5) | ||||||
| Proportion estimates (%) | 57.5 (7.9) | 20.3 (7.6) | ||||||
| EY-PAQ Test 1 vs. Test 2 | Reliability | |||
|---|---|---|---|---|
| n(%) | Mean Daily Difference in Minutes [95% CI] | ICC (2,1) | 95% Confidence Interval | |
| MVPA | 104 (93.7) | 25.5 [−23.9, 74.8] | 0.35 * | 0.17–0.50 |
| ST | 104 (93.7) | 1.7 [−36.5, 39.9] | 0.47 * | 0.3–0.61 |
| EY-PAQ vs. Accelerometer | Validity | ||||||
|---|---|---|---|---|---|---|---|
| N (%) | rho | Mean Daily Difference in Minutes [95% CI] | LOA † | Error Correlations (r) | Heteroskedasicity p-Value | Ratio LOA † | |
| MVPA: No boundaries | 149 (76.0) | 0.03 | 106.3 [72.5, 140.2] | −303.7 to 516.4 | −0.80 * | 0.94 | 1.20 (×/÷ 10.6) |
| MVPA: Boundary applied >2% (16.8 min)<41% (344.3 min)# | 102 (52.0) | 0.30 * | 7.1 [−12.3, 26.4] | −185.9 to 200.1 | −0.37 * | <0.01 | 1.03 (×/÷ 5.8) |
| ST: No boundaries | 147 (75.0) | 0.02 | −160.0 [−189.1, −30.9] | −509.9 to 190.0 | −0.67 * | <0.01 | 1.72 (×/÷ 3.6) |
| ST: Boundary applied >30% (252 min) <94% (789.6 min) # | 89 (45.4) | 0.19 | −87.5 [−117.6, −57.4] | −367.6 to 192.7 | −0.50 * | <0.01 | 1.26 (×/÷ 1.9) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bingham, D.D.; Collings, P.J.; Clemes, S.A.; Costa, S.; Santorelli, G.; Griffiths, P.; Barber, S.E. Reliability and Validity of the Early Years Physical Activity Questionnaire (EY-PAQ). Sports 2016, 4, 30. https://doi.org/10.3390/sports4020030
Bingham DD, Collings PJ, Clemes SA, Costa S, Santorelli G, Griffiths P, Barber SE. Reliability and Validity of the Early Years Physical Activity Questionnaire (EY-PAQ). Sports. 2016; 4(2):30. https://doi.org/10.3390/sports4020030
Chicago/Turabian StyleBingham, Daniel D., Paul J. Collings, Stacy A. Clemes, Silvia Costa, Gillian Santorelli, Paula Griffiths, and Sally E. Barber. 2016. "Reliability and Validity of the Early Years Physical Activity Questionnaire (EY-PAQ)" Sports 4, no. 2: 30. https://doi.org/10.3390/sports4020030
APA StyleBingham, D. D., Collings, P. J., Clemes, S. A., Costa, S., Santorelli, G., Griffiths, P., & Barber, S. E. (2016). Reliability and Validity of the Early Years Physical Activity Questionnaire (EY-PAQ). Sports, 4(2), 30. https://doi.org/10.3390/sports4020030