
Functional Assessment and Injury Risk in a Professional Soccer Team


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
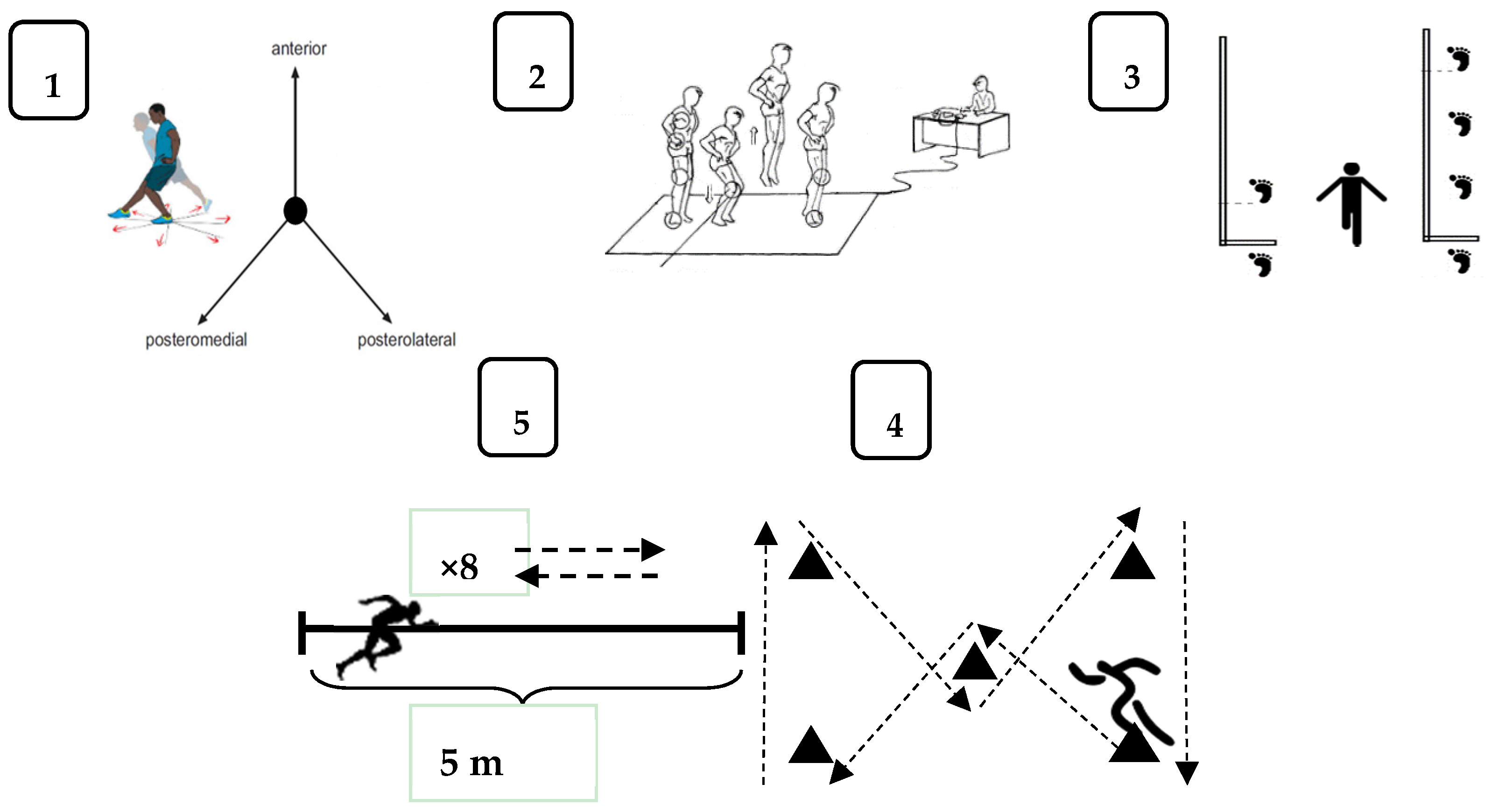
2.3. Functional Tests
2.4. Y Balance Test/Posture Control
2.5. CMJ/Bipodal Vertical Jump
2.6. Hop Test/Unipodal Jump Test
2.7. The 5 m Shuttle Run Sprint Test and Barrow Test/High Speed Changes of Direction
2.8. Data Analysis
3. Results
4. Discussion
5. Conclusions
- -
- For the single hop, triple hop, Y balance, barrow and 8 × 5 m sprint tests, the values obtained by the soccer players who had from one to three injuries and from four to eight injuries during the season were similar to those obtained by the group with zero injuries suffered.
- -
- For the single hop, triple hop, Y balance, barrow and 8 × 5 m sprint tests, the values obtained by the soccer players who were absent from one to 15 days, 16 to 28 days and more than 28 days during the season were similar to those obtained by the group that had no absence days.
- -
- The players with zero injuries and zero absence days had lower values than the remainder in the CMJ test.
- -
- There was no linear correlation among the functional values reached by the professional soccer players and the number of injuries and absence days suffered throughout the season.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Goncalves, G.; Santoro, P.; Runco, J.L.; Cohen, M. The Brazilian football association model for epidemiological studies on professional soccer player injuries. Clinics 2011, 66, 1707–1712. [Google Scholar]
- Meeuwisse, W.H. Assessing causation in sport injury: A multifactorial model. Clin. J. Sport Med. 1994, 4, 166–170. [Google Scholar] [CrossRef]
- Murphy, D.; Connolly, D.; Beynnon, B. Risk factors for lower extremity injury: A review of the literature. Br. J. Sports Med. 2003, 36, 13–29. [Google Scholar] [CrossRef]
- Emery, C.; Cassidy, J.; Klassen, T.; Rosychuk, R.; Rowe, B. Effectiveness of a home-based balance-training program in reducing sports-related injuries among healthy adolescents: A cluster randomized controlled trial. Can. Med. Assoc. J. 2005, 172, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Frisch, A.; Urhausen, A.; Seil, R.; Croisier, J.L.; Windal, T.; Theisen, D. Association between preseason functional tests and injuries in youth football: A prospective follow-up. Scand. J. Med. Sci. Sports 2011, 21, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Steffen, K.; Myklebust, G.; Andersen, T.E.; Holme, I.; Bahr, R. Self-reported injury history and lower limb function as risk factors for injuries in female youth soccer. Am. J. Sports Med. 2008, 36, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, J.; Junge, A.; Chomiak, J.; Graf-Baumann, T.; Peterson, L.; Rosch, D.; Hodgson, R. Risk factor analysis for injuries in football players. Possibilities for a prevention program. Am. J. Sports Med. 2000, 28, 69–74. [Google Scholar] [CrossRef]
- Galambos, S.; Terry, P.; Moyle, M.; Locke, S. Psychological predictors of injury among elite athletes. Br. J. Sports Med. 2005, 39, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, M.; Waldén, M.; Bahr, R.; Ekstrand, J. Methods for epidemiological study of injuries to professional football players: Developing the UEFA model. Br. J. Sports Med. 2005, 39, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Inklaar, H. Soccer injuries I: Incidence and severity. Sports Med. 1994, 18, 55–73. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.; Hamer, P.; Finch, C.; Elliot, B.; Kresnow, M. Sport, age, and sex specific incidence of sports injuries in Western Australia. Br. J. Sports Med. 2000, 34, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Backous, D.D.; Frield, K.E.; Smith, N.J.; Parr, T.J.; Carpine, W. Soccer injuries and their relation to physical maturity. Am. J. Dis. Child. 1988, 142, 839–842. [Google Scholar] [CrossRef] [PubMed]
- Arnason, A.; Sigurdsson, S.B.; Gudmundsson, A.; Holme, I.; Engebretsen, L.; Bahr, R. Physical fitness, injuries, and team performance in soccer. Med. Sci. Sports Exerc. 2004, 36, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Hopper, D.; Hopper, J.; Elliot, B.C. Do selected kinanthropometric and performance variables predict injuries in female netball players? J. Sports Sci. 1995, 13, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Ivarsson, A.; Johnson, U. Psychological factors as predictors of injuries among senior soccer players. A prospective study. J. Sports Sci. Med. 2010, 9, 347–352. [Google Scholar] [PubMed]
- Chomiak, J.; Junge, A.; Peterson, L.; Dvorak, J. Severe injuries in football players. Influencing factors. Am. J. Sports Med. 2000, 28, 58–68. [Google Scholar] [CrossRef]
- Ardern, C.; Glasgow, P.; Schneiders, A.; Witvrouw, E.; Clarsen, B.; Cools, A.; Gojanovic, B.; Griffin, S.; Khan, K.M.; Moksnes, H.; et al. Consensus statement on return to sport from the First World Congress in Sport Physical Therapy, Bern. Br. J. Sports Med. 2016, 50, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Hegedus, E.; Cook, C.E. Return to play and physical performance tests. Evidence-based, rough guess or charade? Br. J. Sports Med. 2015, 49, 1288–1289. [Google Scholar] [CrossRef] [PubMed]
- Brumitt, J.; Heiderscheit, B.; Manske, R.; Niemuth, P.; Rauh, M. Lower extremity functional tests and risk of injury in division III collegiate athletes. Int. J. Sports Phys. Ther. 2013, 8, 216–227. [Google Scholar] [PubMed]
- Okada, T.; Huxel, K.C.; Nesser, T.W. Relationship between core stability, functional movement, and performance. J. Strength Cond. Res. 2011, 25, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Haitz, K.; Shultz, R.; Hodgins, M.; Matheson, G. Test-retest and interrater reliability of the functional lower extremity evaluation. J. Orthop. Sports Phys. Ther. 2014, 44, 947–954. [Google Scholar] [CrossRef] [PubMed]
- McCall, A.; Carling, C.; Nedelec, M.; Davison, M.; Le Gall, F.; Berthoin, S.; Dupont, G. Risk factors, testing and preventative strategies for non-contact injuries in professional football: Current perceptions and practices of 44 teams from various premier leagues. Br. J. Sports Med. 2014. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R. Why screening tests to predict injury do not work and probably never will…: A critical review. Br. J. Sports Med. 2016, 50, 776–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiesel, K.; Plisky, P.; Voight, M. Can serious injury in professional football be predicted by a preseason functional movement screen? N. Am. J. Sports Phys. Ther. 2007, 2, 147–158. [Google Scholar] [PubMed]
- Plisky, P.; Rauh, M.; Kaminski, T.; Underwood, F. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. J. Orthop. Sports Phys. Ther. 2006, 36, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Arnold, B.L.; de La Motte, S.; Linens, S.; Ross, S.E. Ankle instability is associated with balance impairments: A meta-analysis. Med. Sci. Sports Exerc. 2009, 41, 1048–1062. [Google Scholar] [CrossRef] [PubMed]
- Gustavsson, A.; Neeter, C.; Thomee, P.; Silbernagel, K.; Augustsson, J.; Thomeé, R.; Karlsson, J. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Herrington, L.; Hatcher, J.; Hatcher, A.; McNicholas, M. A comparison of star excursion balance test reach distances between ACL deficient patients and asymptomatic controls. Knee 2009, 16, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hägglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand. J. Med. Sci. Sports 2006, 16, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Emery, C.; Meeuwisse, W.; Hartmann, S. Evaluation of risk factors for injury in adolescent soccer: Implementation and validation of an injury surveillance system. Am. J. Sports Med. 2005, 33, 1882–1891. [Google Scholar] [CrossRef] [PubMed]
- Hertel, J.; Braham, R.A.; Hale, S.A.; Olmsted, L.C. Simplifying the star excursion balance test: Analyses of subjects with and without chronic ankle instability. J. Orthop. Sports Phys. Ther. 2006, 36, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Bosco, C.; Luhtanen, P.; Komi, P.V. A simple method for measurement of mechanical power in jumping. Eur. J. Appl. Physiol. Occup. Phsysiol. 1983, 50, 273–282. [Google Scholar] [CrossRef]
- Noyes, F.R.; Barber, S.D.; Mangine, R.E. Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. Am. J. Sports Med. 1991, 19, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Barrow, H.; McGee, R. A Practical Approach to Measurement in Physical Education; Lea & Febiger: Philadelphia, PA, USA, 1971. [Google Scholar]
- Danelon, F.; Boldrini, L.; Canzi, M.; Pisoni, D.; Porcelli, S.; Roi, G.; Tavana, R. Objective reference values for assessing functional recovery after injuries in amateur soccer players. Med. Sci. Exerc. 2005. [Google Scholar] [CrossRef]
- Plisky, P.J.; Gorman, P.P.; Butler, R.J.; Kiesel, K.; Underwood, F.; Elkins, B. The reliability of an instrumented device for measuring components of the Star Excursion Balance Test. N. Am. J. Sports Phys. Ther. 2009, 4, 92–99. [Google Scholar] [PubMed]
- Olmsted, L.; Carcia, C.; Hertel, J.; Shultz, S. Efficacy of the Star excursion balance tests in detecting reach deficits in subjects with chronic ankle instability. J. Athl. Train. 2002, 37, 501–506. [Google Scholar] [PubMed]
- Gribble, P.A.; Hertel, J. Effect of lower-extremity muscle fatigue on postural control. Arch. Phys. Med. Rehabil. 2004, 85, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Coughlan, G.; Fullam, K.; Delahunt, E.; Gissane, C.; Caulfield, B. A comparison between performance on selected directions of the star excursion balance test and the Y balance test. J. Athl. Train. 2012, 47, 366–371. [Google Scholar] [PubMed]
- Vanezis, A.; Lees, A. A biomechanical analysis of good and poor performers of the vertical jump. Ergonomics 2005, 15, 1594–1603. [Google Scholar] [CrossRef] [PubMed]
- Twist, C.; Highton, J. Monitoring fatigue and recovery in rugby league players. Int. J. Sports Physiol. Perform. 2013, 8, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.; Birmingham, T.B.; Stratford, B.W.; Alcock, G.K.; Giffin, J.R. Hop testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Phys. Ther. 2007, 87, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Noyes, F.R.; Barber, S.D.; Mooar, L.A. A rationale for assessing sports activity levels and limitations in knee disorders. Clin. Orthop. Relat. Res. 1989, 246, 238–249. [Google Scholar] [CrossRef]
- Logerstedt, D.; Grindem, H.; Lynch, A.; Eitzen, I.; Engebretsen, L.; Risberg, M.A.; Snyder, L. Single-legged Hop Tests as predictors of self-reported knee function after Anterior Cruciate Ligament reconstruction. Am. J. Sports Med. 2012, 40, 2348–2356. [Google Scholar] [CrossRef] [PubMed]
- Müller, U.; Krüger, M.; Schmidt, M.; Rosemeyer, B. Predictive parameters for return to pre-injury level of sport 6 month following anterior cruciate ligament reconstruction surgery. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 3623–3631. [Google Scholar] [CrossRef] [PubMed]
- Daniel, D.M.; Malcolm, L.; Stone, M.L.; Perth, H.; Morgan, J. Quantification of knee stability and function. Contemp. Orthop. 1982, 5, 83–91. [Google Scholar]
- Rampinini, E.; Bishop, D.; Marcora, S.M.; Ferrari, D.; Sassi, R.; Impellizzeri, F.M. Validity of simple field tests as indicators of match-related physical performance in top-level professional soccer players. Int. J. Sports Med. 2007, 28, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Castagna, C.; Impellizzeri, F.; Cecchini, E.; Rampinini, E.; Alvarez, J.C. Effects of intermittent-endurance fitness on match performance in young male soccer players. J. Strength Cond. Res. 2009, 23, 1954–1959. [Google Scholar] [CrossRef] [PubMed]
- Chaouachi, A.; Manzi, V.; Chaalali, A.; Wong, D.P.; Chamari, K.; Castagna, C. Determinants analysis of change of direction ability in elite soccer players. J. Strength Cond. Res. 2012, 26, 2667–2676. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, A.; Olson, S.L.; Roddey, T.S.; Morales, J. Reliability of selected physical performance tests in young adult women. J. Strength Cond. Res. 2005, 19, 39–44. [Google Scholar] [PubMed]
- Hetzler, R.; Stickley, C.; Lundquist, K.; Kimura, I. Reliability and accuracy of handheld stopwatches compared with electronic timing in measuring sprint performance. J. Strength Cond. Res. 2008, 22, 1969–1976. [Google Scholar] [CrossRef] [PubMed]
- Ebben, W.; Petushek, E.; Clewein, R. A comparison of manual and electronic timing during 20 and 40 yards sprints. J. Exerc. Physiol. 2009, 12, 34–38. [Google Scholar]
- Lohmander, L.S.; Roos, E.M. The evidence base for orthopaedics and sports medicine. Br. J. Sports Med. 2015, 50, 564–565. [Google Scholar] [CrossRef] [PubMed]
- Munn, J.; Beard, D.; Refshauge, K.; Lee, R. Do functional performance tests detect impairment in subjects with ankle instability? J. Sport Rehabil. 2002, 11, 40–50. [Google Scholar] [CrossRef]
- Hegedus, E.J.; McDonough, S.; Bleakley, C.; Cook, C.; Baxter, G. Clinician-friendly lower extremity physical performance measures in athletes: A systematic review of measurement properties and correlation with injury, part 1. The tests for knee function including the hop tests. Br. J. Sports Med. 2015, 49, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Henry, T.; Evans, K.; Snodgrass, S.; Miller, A.; Callister, R. Risk factors for noncontact ankle injuries in amateur male soccer. Clin. J. Sport Med. 2016, 26, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, S.; Magarey, M.; Esterman, A.; Speechley, M.; Scase, E.; Heynen, M. The relationship between pre-season fitness testing and injury in elite junior Australian football players. J. Sci. Med. Sport 2013, 16, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, A.; Myklebust, G.; Holme, I.; Engebretsen, L.; Bahr, R. Intrinsic risk factor for groin injuries among male soccer players: A prospective cohort study. Am. J. Sports Med. 2010, 38, 2051–2057. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Krosshaug, T. Understanding injury mechanisms: A key component of preventing injuries in sport. Br. J. Sport Med. 2005, 39, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Meeuwisse, W.H.; Tyreman, H.; Hagel, B.; Emery, C. A dynamic model of etiology in sport injury: The recursive nature of risk and causation. Clin. J. Sport Med. 2007, 17, 215–219. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| TEST | AVERAGE | NORMALITY (K-S) |
|---|---|---|
| CMJ (cm) | 39.95 ± 4.16 | 0.20 |
| Barrow Test (s) | 7.46 ± 0.29 | 0.20 |
| 8 × 5 m Shuttle Run Sprint Test (s) | 10.88 ± 0.39 | 0.20 |
| Asymmetry Single Hop (%) | 2.94 ± 1.75 | 0.00 * |
| Asymmetry Triple Hop (%) | 2.39 ± 1.47 | 0.01 * |
| YB—Right difference (cm) | 4.92 ± 1.72 | 0.93 |
| YB—Left difference (cm) | 3.52 ± 2.09 | 0.27 |
| TEST | Uninjured (n = 5) | 1–3 Injuries (n = 36) | 4–8 Injuries (n = 11) | p |
|---|---|---|---|---|
| CMJ (cm) | 35.56 ± 3.94 | 40.43 ± 4.42 | 40.36 ± 1.75 | 0.04 * |
| Barrow Test (s) | 7.51 ± 0.28 | 7.47 ± 0.31 | 7.39 ± 0.22 | 0.68 |
| 8 × 5 m Shuttle Run Sprint Test (s) | 10.96 ± 0.27 | 10.88 ± 0.43 | 10.87 ± 0.28 | 0.91 |
| Asymmetry Single Hop (%) | 3.35 ± 1.49 | 2.93 ± 1.82 | 2.78 ± 1.74 | 0.75 |
| Asymmetry Triple Hop (%) | 2.74 ± 1.40 | 2.40 ± 1.59 | 2.20 ± 1.12 | 0.65 |
| YB—Right difference (cm) | 5.25 ± 1.76 | 4.95 ± 1.92 | 4.72 ± 1.29 | 0.93 |
| YB—Left difference (cm) | 5.83 ± 0.23 | 3.36 ± 2.15 | 3.22 ± 1.98 | 0.27 |
| TEST | 0 Days (n = 5) | 1–15 Days (n = 24) | 16–28 Days (n = 6) | +28 Days (n = 17) | p |
|---|---|---|---|---|---|
| CMJ (cm) | 35.56 ± 3.94 | 39.62 ± 4.60 | 40.30 ± 4.00 | 41.58 ± 2.64 | 0.03 * |
| Barrow Test (s) | 7.51 ± 0.28 | 7.47 ± 0.30 | 7.53 ± 0.36 | 7.39 ± 0.24 | 0.68 |
| 8 × 5 m Shuttle Run Sprint Test (s) | 10.96 ± 0.27 | 10.95 ± 0.42 | 10.79 ± 0.49 | 10.80 ± 0.34 | 0.55 |
| Asymmetry SLHT (%) | 3.35 ± 1.49 | 3.94 ± 1.92 | 3.14 ± 1.59 | 2.60 ± 1.70 | 0.68 |
| Asymmetry THT (%) | 2.74 ± 1.40 | 2.55 ± 1.80 | 2.63 ± 1.06 | 1.99 ± 1.04 | 0.61 |
| YB—Right difference (cm) | 5.25 ± 1.76 | 5.57 ± 1.77 | 2.83 ± 1.25 | 4.64 ± 1.28 | 0.08 |
| YB—Left difference (cm) | 5.83 ± 0.23 | 3.75 ± 2.11 | 3.16 ± 1.75 | 2.75 ± 2.20 | 0.30 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Piqueras, P.; González-Víllora, S.; Sainz de Baranda Andújar, M.D.P.; Contreras-Jordán, O.R. Functional Assessment and Injury Risk in a Professional Soccer Team. Sports 2017, 5, 9. https://doi.org/10.3390/sports5010009
Gómez-Piqueras P, González-Víllora S, Sainz de Baranda Andújar MDP, Contreras-Jordán OR. Functional Assessment and Injury Risk in a Professional Soccer Team. Sports. 2017; 5(1):9. https://doi.org/10.3390/sports5010009
Chicago/Turabian StyleGómez-Piqueras, Pedro, Sixto González-Víllora, María Del Pilar Sainz de Baranda Andújar, and Onofre R. Contreras-Jordán. 2017. "Functional Assessment and Injury Risk in a Professional Soccer Team" Sports 5, no. 1: 9. https://doi.org/10.3390/sports5010009
APA StyleGómez-Piqueras, P., González-Víllora, S., Sainz de Baranda Andújar, M. D. P., & Contreras-Jordán, O. R. (2017). Functional Assessment and Injury Risk in a Professional Soccer Team. Sports, 5(1), 9. https://doi.org/10.3390/sports5010009