The Effects of Exercise Induced Muscle Damage on Knee Joint Torque and Balance Performance


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Measures
2.3.1. Knee and Ankle Joint Torque
2.3.2. Balance
2.4. Statistical Analysis
3. Results
3.1. Total Volume-Load
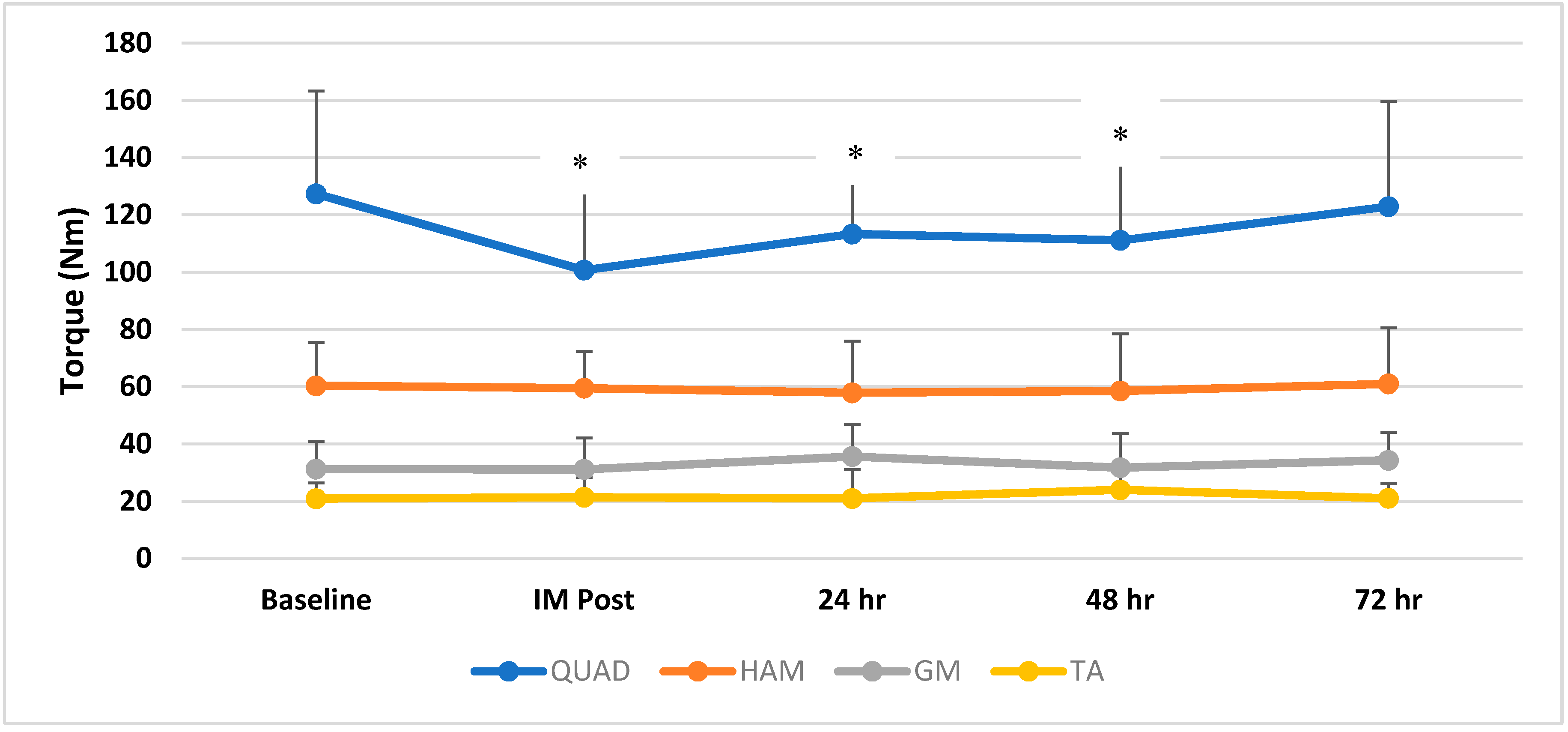
3.2. Torque Measures
3.3. Balance Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Clarkson, P.M.; Sayers, S.P. Etiology of exercise-induced muscle damage. Can. J. Appl. Physiol. 1999, 24, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.; Twist, C.; Eston, R. Neuromuscular function after exercise induced muscle damage. Sports Med. 2004, 34, 49–69. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, P.M.; Hubal, M.J. Exercise induced muscle damage in humans. Am. J. Phys. Med. Rehab. 2002, 8, S52–S69. [Google Scholar] [CrossRef]
- Dabbs, N.C.; Black, C.; Garner, J.C. Effects of whole body vibration on muscle contractile properties in exercse induced muscle damaged females. Electromyogr. Kinesiol. 2016, 30, 119–125. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Health-Related Physical Fitness Assessment Manual, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Chander, H.; Dabbs, N.C. Balance Performance and Training among Female Athletes. Strength Cond. J. 2016, 38, 8–13. [Google Scholar] [CrossRef]
- Levangie, P.K.; Norkin, C.C. Joint Structure and Function: A Comprehensive Analysis, 4th ed.; F.A. Davis Company: Philadelphia, PA, USA, 2006. [Google Scholar]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Lepers, R.; Bigard, A.X.; Diard, J.P.; Gouteyron, J.F.; Guezennec, C.Y. Posture control after prolonged exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1997, 76, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Corbeil, P.; Blouin, J.; Begin, F.; Nougier, V.; Teasdale, N. Perturbation of the postural control system inducted by muscular fatigue. Gait Posture 2003, 18, 92–100. [Google Scholar] [CrossRef]
- Chander, H.; Garner, J.C.; Wade, C. The influence of occupational footwear on dynamic balance perturbations. Footwear Sci. 2015, 7, 115–126. [Google Scholar] [CrossRef]
- Guskiewicz, K.M.; Perrin, D.H. Research and clinical applications of assessing balance. J. Sport Rehab. 1996, 5, 45–63. [Google Scholar] [CrossRef]
- Guskiewicz, K.; Perrin, D.; Gansneder, B. Effect of mild head injury on postural stability in athletes. J. Athl. Train. 1996, 31, 300–306. [Google Scholar] [PubMed]
- Warren, G.L.; Lowe, D.A.; Armstrong, R.B. Measurement tools used in the study of eccentric contraction-induced injury. Sports Med. 1999, 27, 43–59. [Google Scholar] [CrossRef] [PubMed]
- Pline, K.; Madigan, M.; Nussbaum, M. Influence of fatigue time and level on increases in postural sway. Ergonomics 2006, 49, 1639–1648. [Google Scholar] [CrossRef] [PubMed]
- Yaggie, J.A.; McGregor, S.J. Effects of isokinetic ankle fatigue on the maintenance of balance and postural limits. Arch. Phys. Med. Rehabil. 2002, 83, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Vuillerme, N.; Danion, F.; Forestier, N.; Nougier, V. Postural sway under muscle vibration and muscle fatigue in humans. Neurosci. Lett. 2002, 333, 131–135. [Google Scholar] [CrossRef]
- Caron, O. Is there interaction between vision and local fatigue of the lower limbs on postural control and postural stability in human posture? Neurosci. Lett. 2004, 363, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Hertel, J. Effect of lower-extremity muscle fatigue on postural control. Arch. Phys. Med. Rehabil. 2004, 85, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Chander, H.; MacDonald, C.J.; Dabbs, N.C.; Allen, C.R.; Lamont, H.S.; Garner, J.C. Balance Performance in Female Collegiate Athletes. J. Sports Sci. 2014, 2, 13–20. [Google Scholar]
- Matsuda, S.; Demura, S.; Uchiyama, M. Centre of Pressure Sway Characteristics during Static One-Legged Stance of Athletes from Different Sports. J. Sports Sci. 2008, 26, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Gerbino, P.G.; Griffin, E.D.; Zurakowski, D. Comparison of standing balance between female collegiate dancers and soccer players. Gait Posture 2007, 26, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Hrysomallis, C.; McLaughlin, P.; Goodman, C. Relationship between Static and Dynamic Balance Tests among Elite Australian Footballers. J. Sci. Med. Sport 2006, 9, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Knight, A.; Holmes, M.; Chander, H.; Kimble, A.; Stewart, J. Assessment of Balance among adolescent track and field athletes. Sports Biomech. 2016, 15, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Harriss, D.J.; Macsween, A.; Atkinson, G. Standards for Ethics in Sport and Exercise Reearch: 2018 Update. Int. J. Sports Med. 2017, 38, 1126–1131. [Google Scholar] [PubMed]
- Dabbs, N.C.; Black, C.; Garner, J.C. Whole-Body Vibration While Squatting and Delayed-Onset Muscle Soreness in Women. J. Athl. Train. 2015, 50, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Dabbs, N.C.; Brown, L.E.; Garner, J.C. Effects of Whole Body Vibration on Vertical Jump Performance Following Exercise Induced Muscle Damage. Intern. J. Kines Sports Sci. 2014, 2, 24–30. [Google Scholar] [CrossRef]
- Twist, C.; Eston, R. The effects of exercise induced muscle damage on maximal intensity intermittent exercise performance. Eur. J. Appl. Physiol. 2005, 94, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Nardone, A.; Tarantola, J.; Giordano, A.; Schieppati, M. Fatigue Effects on body balance. Electroencephalogr. Clin. Neurophysiol. 1997, 105, 309–320. [Google Scholar] [CrossRef]
- Caron, O. Effects of local fatigue of the lower limbs on postural control and postural stability in standing posture. Neurosci. Lett. 2003, 340, 83–86. [Google Scholar] [CrossRef]
- Chander, H.; Garner, J.C.; Wade, C. Impact on balance while walking in occupational footwear. Footwear Sci. 2014, 6, 59–66. [Google Scholar] [CrossRef]
- Turner, A.J.; Swain, J.C.; McWhirter, K.L.; Knight, A.C.; Carruth, D.W.; Chander, H. Impact of Occupational Footwear and Workload on Lower Extremity Muscular Exertion. Int. J. Exerc. Sci. 2018, 11, 331–341. [Google Scholar]
- Lin, W.; Liu, Y.; Hsieh, C.; Lee, A. Ankle eversion to inversion strength ratio and static balance control in the dominant and non-dominant limbs of young adults. J. Sports Sci. Med. 2009, 12, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.; Schrader, J.; Applegate, T.; Koceja, D. Unilateral postural control of the functionally dominant and nondominant extremities of healthy subjects. Journal of athletic training. J. Athl. Train. 2009, 33, 319–322. [Google Scholar]
- Gstöttner, M.; Neher, A.; Scholtz, A.; Milllonig, M.; Lembert, S.; Raschner, C. Balance ability and muscle response of the preferred and nonpreferred leg in soccer players. Mot. Control 2009, 13, 218–231. [Google Scholar] [CrossRef]


{kind=link}
| Balance Condition | Balance Direction | Baseline | IM Post | 24 h Post | 48 h Post | 72 h Post |
|---|---|---|---|---|---|---|
| Static DL | Overall | 0.35 ± 0.15 | 0.66 ± 0.59 | 0.81 ± 1.18 | 0.45 ± 0.51 | 0.47 ± 0.37 |
| AP | 0.26 ± 0.14 | 0.53 ± 0.54 | 0.73 ± 1.17 | 0.40 ± 0.52 | 0.34 ± 0.24 | |
| ML | 0.16 ± 0.09 | 0.25 ± 0.27 | 0.22 ± 0.22 | 0.17 ± 0.13 | 0.22 ± 0.28 | |
| Static RL | Overall | 1.57 ± 1.10 | 1.37 ± 0.95 | 1.25 ± 0.73 | 1.26 ± 0.78 | 1.04 ± 0.56 |
| AP | 1.10 ± 1.09 | 0.92 ± 0.90 | 0.83 ± 0.50 | 0.76 ± 0.43 | 0.61 ± 0.29 | |
| ML | 0.91 ± 0.53 | 0.88 ± 0.57 | 0.83 ± 0.57 | 0.86 ± 0.72 | 0.73 ± 0.56 | |
| Unstable DL | Overall | 1.38 ± 0.72 | 1.55 ± 1.52 | 1.39 ± 0.84 | 1.28 ± 0.84 | 1.21 ± 0.71 |
| AP | 1.13 ± 0.63 | 1.32 ± 1.26 | 1.12 ± 0.70 | 0.91 ± 0.55 | 0.96 ± 0.58 | |
| ML | 0.57 ± 0.41 | 0.70 ± 0.73 | 0.57 ± 0.51 | 0.66 ± 0.64 | 0.56 ± 0.38 | |
| Unstable RL | Overall | 2.21 ± 1.27 | 2.14 ± 1.24 | 1.94 ± 0.98 | 1.72 ± 1.25 | 1.59 ± 0.85 |
| AP | 1.37 ± 0.91 | 1.6 ± 0.93 | 1.33 ± 0.74 | 1.04 ± 0.65 | 1.02 ± 0.49 | |
| ML | 1.57 ± 1.02 | 1.36 ± 0.84 | 1.14 ± 0.87 | 1.18 ± 1.18 | 1.11 ± 0.65 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dabbs, N.C.; Chander, H. The Effects of Exercise Induced Muscle Damage on Knee Joint Torque and Balance Performance. Sports 2018, 6, 101. https://doi.org/10.3390/sports6030101
Dabbs NC, Chander H. The Effects of Exercise Induced Muscle Damage on Knee Joint Torque and Balance Performance. Sports. 2018; 6(3):101. https://doi.org/10.3390/sports6030101
Chicago/Turabian StyleDabbs, Nicole C., and Harish Chander. 2018. "The Effects of Exercise Induced Muscle Damage on Knee Joint Torque and Balance Performance" Sports 6, no. 3: 101. https://doi.org/10.3390/sports6030101
APA StyleDabbs, N. C., & Chander, H. (2018). The Effects of Exercise Induced Muscle Damage on Knee Joint Torque and Balance Performance. Sports, 6(3), 101. https://doi.org/10.3390/sports6030101