Impact of a Professional Nutrition Program on a Female Cross Country Collegiate Athlete: A Case Report


Abstract
:1. Introduction
2. Materials and Methods
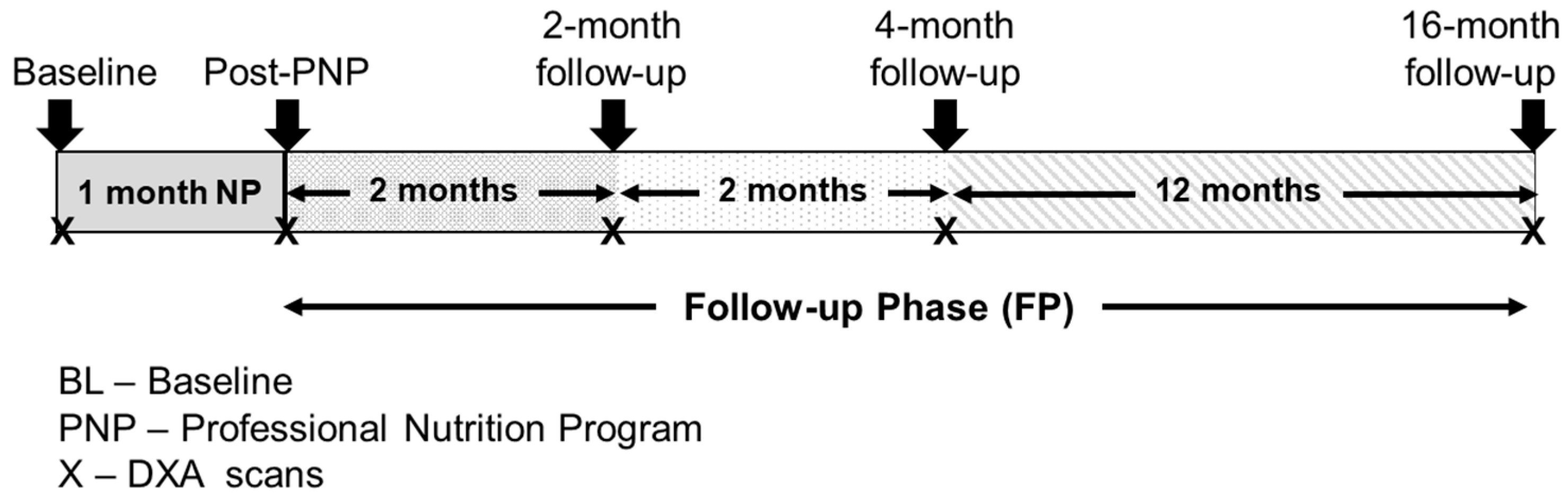
2.1. Case Report Design
2.2. Recruitment (RC)
2.3. Nutrition Program and Dietary Records
2.4. Measurements
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Committee on Adolescent Health Care. Committee opinion no.702: Female athlete triad. Obstet. Gynecol. 2017, 129, e160–e167. [Google Scholar] [CrossRef] [PubMed]
- Nattiv, A.; Loucks, A.B.; Manore, M.M.; Sanborn, C.F.; Sundgot-Borgen, J.; Warren, M.P. American College of Sports Medicine position stand. The female athlete triad. Med. Sci. Sports Exerc. 2007, 39, 1867–1882. [Google Scholar] [PubMed]
- Kim, B.Y.; Nattiv, A. Health considerations in female runners. Phys. Med. Rehabil. Clin. N. Am. 2016, 27, 151–178. [Google Scholar] [CrossRef] [PubMed]
- Beals, K.A.; Manore, M.M. Disorders of the female athlete triad among collegiate athletes. Int. J. Sport Nutr. Exerc. Metab. 2002, 12, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, P.; Hensley, S.; Roepke, J.B.; Whitaker, S.H.; Craig, B.W.; Drewnowski, A. Eating attitudes and energy intakes of female skaters. Med. Sci. Sports Exerc. 1998, 30, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Thein-Nissenbaum, J.; Hammer, E. Treatment strategies for the female athlete triad in the adolescent athlete: Current perspectives. J. Sports Med. 2017, 8, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Carter, S.; Constantini, N.; Lebrun, C.; Meyer, N.; Sherman, R.; Steffen, K.; Budgett, R.; et al. The ioc consensus statement: Beyond the female athlete triad—Relative energy deficiency in sport (red-s). Br. J. Sports Med. 2014, 48, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D. The female athlete triad: Causes, diagnosis, and treatment. Phys. Sportsmed. 1996, 24, 67–86. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.A.; Benedict, F.G. A biometric study of human basal metabolism. Proc. Natl. Acad. Sci. USA 1918, 4, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Manore, M.M. Nutritional needs of the female athlete. Clin. Sports Med. 1999, 18, 549–563. [Google Scholar] [CrossRef]
- Manore, M.M.; Kam, L.C.; Loucks, A.B. The female athlete triad: Components, nutrition issues, and health consequences. J. Sports Sci. 2007, 25 (Suppl. 1), S61–S71. [Google Scholar] [CrossRef] [PubMed]
- Taaffe, D.R.; Robinson, T.L.; Snow, C.M.; Marcus, R. High-impact exercise promotes bone gain in well-trained female athletes. J. Bone Miner. Res. 1997, 12, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Genant, H.K.; Cooper, C.; Poor, G.; Reid, I.; Ehrlich, G.; Kanis, J.; Nordin, B.E.; Barrett-Connor, E.; Black, D.; Bonjour, J.P.; et al. Interim report and recommendations of the world health organization task-force for osteoporosis. Osteoporos. Int. 1999, 10, 259–264. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Baseline | Post-PNP | 2-Month Follow-up | 4-Month Follow-up | 16-Month Follow-up |
|---|---|---|---|---|---|
| Age | 20.6 | 20.7 | 20.9 | 21.1 | 22.1 |
| Height (m) | 1.75 | 1.75 | 1.75 | 1.75 | 1.75 |
| Body weight (kg) | 56.70 | 57.32 | 56.25 | 56.96 | 58.66 |
| BMI (kg/m2) | 18.46 | 18.66 | 18.31 | 18.55 | 19.10 |
| BMR (kcal) 1 | 1428 | 1429 | 1418 | 1425 | 1436 |
| Energy requirements (kcal) 1 | 3141 | 3143 | 3120 | 3134 | 3160 |
| Fat mass (kg) | 2.54 | 3.66 | 3.08 | 3.26 | 5.89 |
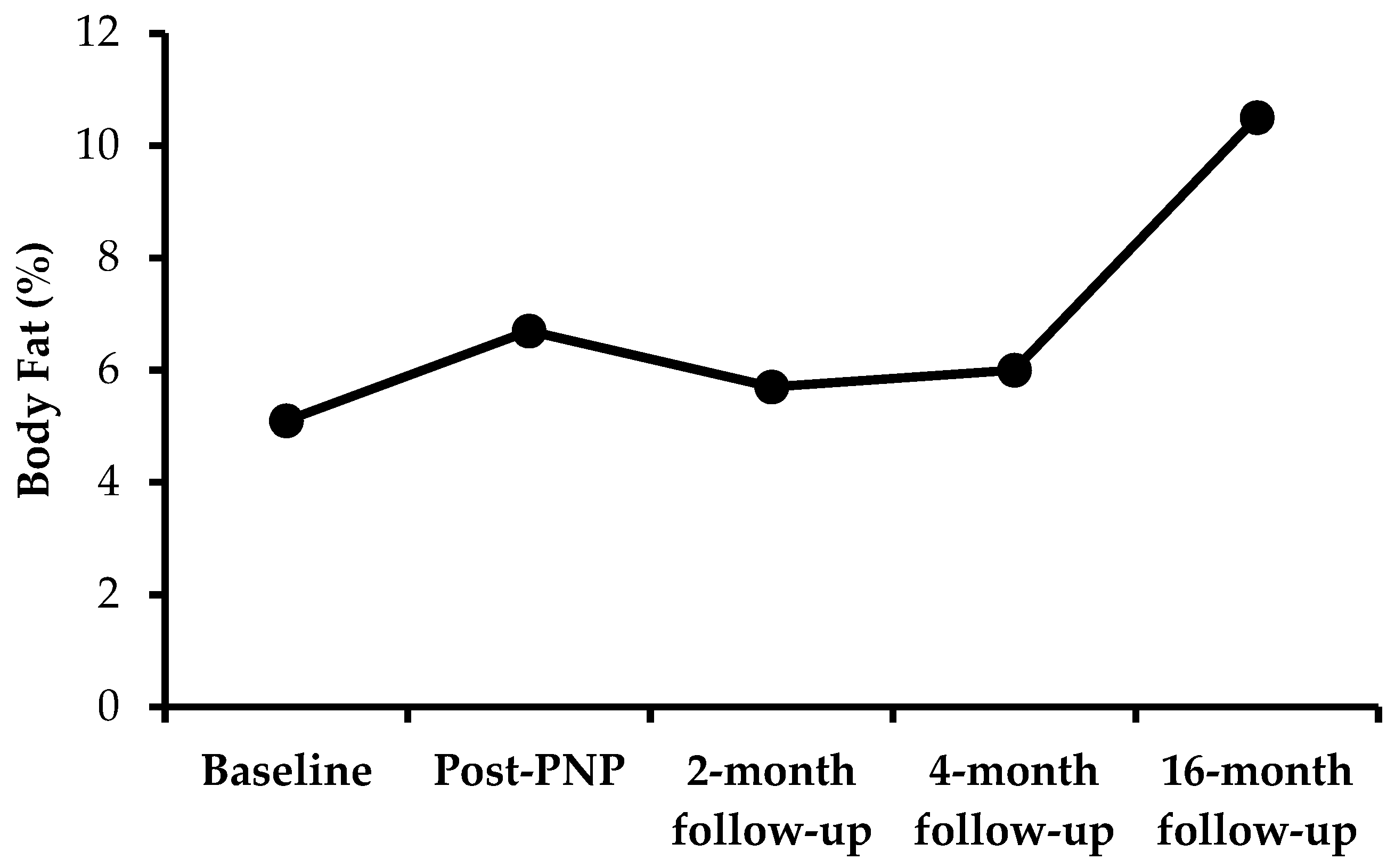
| Fat (%BW) | 4.7 | 6.7 | 5.7 | 6.0 | 10.5 |
| Lean mass (kg) | 51.61 | 51.12 | 50.67 | 51.16 | 50.31 |
| Lean mass (%BW) | 91.02 | 89.17 | 90.08 | 89.81 | 85.77 |
| BMD (g/cm2) | 1.188 | 1.197 | 1.206 | 1.169 | 1.192 |
| BMC (g) | 2561 | 2575 | 2560 | 2545 | 2520 |
| Energy Consumption/day | Baseline | Post-PNP | 2-Month Follow-up | 4-Month Follow-up |
| Kilocalories consumed | 2188 | 3187 | 2796 | 2781 |
| Fat (g) | 69 | 105 | 77 | 74 |
| Fat (% e) | 24.5 | 29.5 | 24.6 | 23.8 |
| Protein (g) | 100 | 128 | 117 | 115 |
| Protein (%e) | 18.3 | 16.0 | 16.7 | 16.6 |
| Carbohydrates (g) | 321 | 467 | 429 | 429 |
| Carbohydrates (%e) | 62.1 | 58.8 | 61.4 | 61.9 |
| Net carbs (g) | 276 | 400 | 358 | 353 |
| Fiber (g) | 45 | 64 | 66 | 71 |
| Trans fat (g) | 0.0 | 0.3 | 0.2 | 0.1 |
| Trans fat (%e) | 0.0 | 0.1 | 0.0 | 0.0 |
| Sat fat (g) | 16.4 | 25.5 | 18.9 | 18.4 |
| Sat fat (%e) | 5.8 | 7.2 | 6.1 | 6.0 |
| Sugars (g) | 118 | 180 | 174 | 173 |
| Cholesterol (mg) | 106 | 231 | 175 | 278 |
| Sodium (mg) | 4113 | 5346 | 3967 | 3914 |
| Energy Expenditure/day | Baseline | Post-PNP | 2-Month Follow-up | 4-Month Follow-up |
| Running distance (km) | 12.1 | 12.1 | 12.0 | 12.1 |
| Duration (min) | 90 | 79 | 79 | 67 |
| Energy expenditure | 1045 | 984 | 937 | 875 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syed-Abdul, M.M.; Soni, D.S.; Wagganer, J.D. Impact of a Professional Nutrition Program on a Female Cross Country Collegiate Athlete: A Case Report. Sports 2018, 6, 82. https://doi.org/10.3390/sports6030082
Syed-Abdul MM, Soni DS, Wagganer JD. Impact of a Professional Nutrition Program on a Female Cross Country Collegiate Athlete: A Case Report. Sports. 2018; 6(3):82. https://doi.org/10.3390/sports6030082
Chicago/Turabian StyleSyed-Abdul, Majid Mufaqam, Dhwani Satishkumar Soni, and Jason Daniel Wagganer. 2018. "Impact of a Professional Nutrition Program on a Female Cross Country Collegiate Athlete: A Case Report" Sports 6, no. 3: 82. https://doi.org/10.3390/sports6030082
APA StyleSyed-Abdul, M. M., Soni, D. S., & Wagganer, J. D. (2018). Impact of a Professional Nutrition Program on a Female Cross Country Collegiate Athlete: A Case Report. Sports, 6(3), 82. https://doi.org/10.3390/sports6030082