Moderate Intensity Intermittent Exercise Modality May Prevent Cardiovascular Drift


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
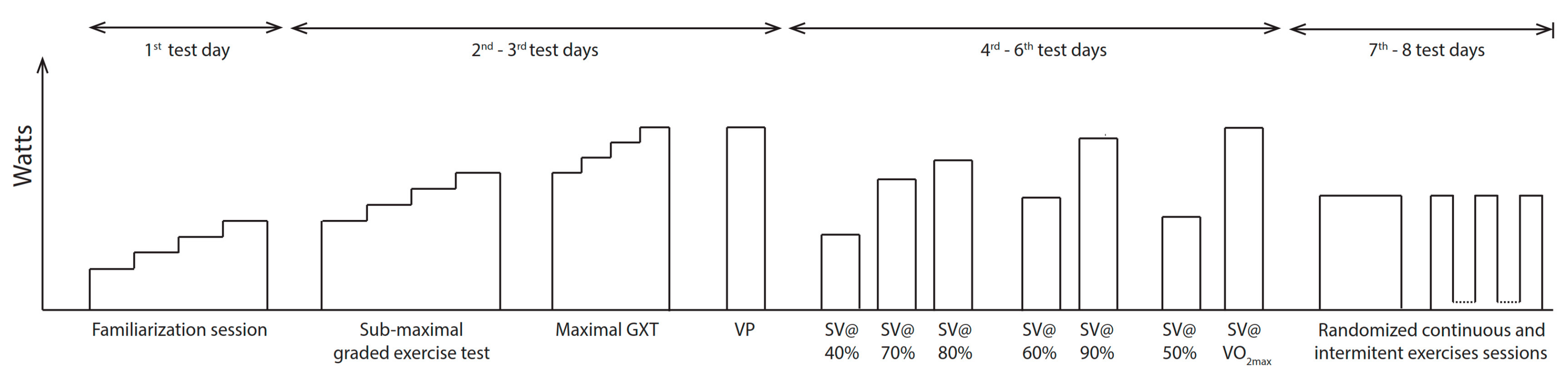
2.2. Experimental Design
2.3. Procedures
2.3.1. Cycle Ergometer
2.3.2. O2max Determination
2.3.3. SVmax Determination
2.3.4. Continuous and Intermittent Exercise Bouts
2.4. Statistical Analysis
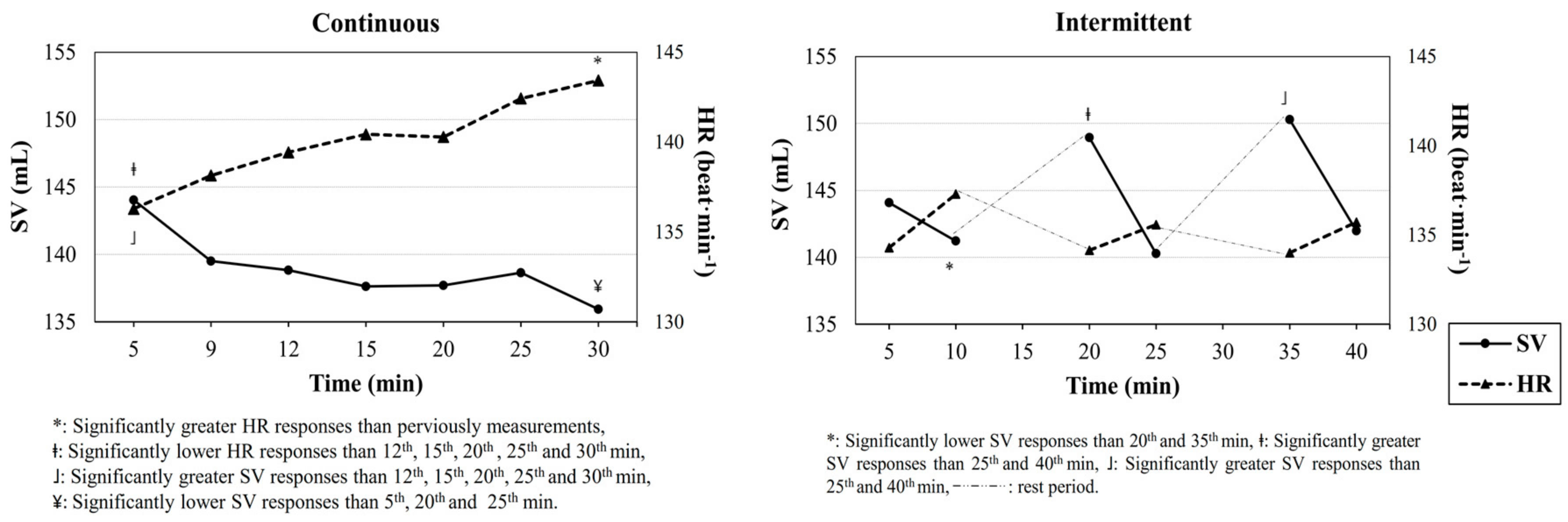
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Astrand, I. Aerobic work capacity in men and women with special reference to age. Acta Physiol. Scand. Suppl. 1960, 49, 1–92. [Google Scholar] [PubMed]
- Ekelund, L. Circulatory and respiratory adaptation during prolonged exercise of moderate intensity in the sitting position. Acta Physiol. Scand. 1967. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, L. G.; Holmgren, A. Circulatory and Respiratory Adaptation, during Long-Term, Non-Steady State Exercise, in the Sitting Position. Acta Physiol. Scand. 1964, 62, 240–255. [Google Scholar] [CrossRef] [PubMed]
- Coyle, E.F.; González-Alonso, J. Cardiovascular Drift during Prolonged Exercise: New Perspectives. Exerc. Sport Sci. Rev. 2001, 29, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Fritzsche, R.G.; Switzer, T.W.; Hodgkinson, B.J.; Coyle, E.F. Stroke volume decline during prolonged exercise is influenced by the increase in heart rate. J. Appl. Physiol. 1999, 86, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.; GonzaleZ-Alonso, J. Fluid replacement and glucose infusion during exercise prevent cardiovascular drift. J. Appl. 1991, 71, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Wingo, J.; Ganio, M.; Cureton, K. Cardiovascular drift during heat stress: Implications for exercise prescription. Exerc. Sport Sci. 2012, 40, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Kounalakis, S.; Keramidas, M.; Nassis, G. The role of muscle pump in the development of cardiovascular drift. Eur. J. Appl. Physiol. 2008, 103, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Trinity, J. Impact of Intensity and Body Temperature on Cardiovascular Responses to Exercise. Bachelor’s Thesis, The University of Texas at Austin, Austin, TX, USA, 2009. [Google Scholar]
- WHO Global 2010 Recommendation on Physical Activity for Health. 2010. Available online: www. who. int/dietphysicalactivity/factsheet_ recommendations/en (accessed on 12 August 2018).
- Gonzalez-Alonso, J.; Mora-Rodriguez, R. Dehydration reduces cardiac output and increases systemic and cutaneous vascular resistance during exercise. J. Appl. 1995, 79, 1487–1496. [Google Scholar] [CrossRef] [PubMed]
- Stanley, J.; Buchheit, M. Moderate recovery unnecessary to sustain high stroke volume during interval training. A brief report. J. Sports Sci. Med. 2014, 13, 393–396. [Google Scholar] [PubMed]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle: Part I: Cardiopulmonary emphasis. Sports Med. 2013, 43, 313–338. [Google Scholar] [CrossRef] [PubMed]
- Lepretre, P.M.; Koralsztein, J.P.; Billat, V.L. Effect of exercise intensity on relationship between V??O2max and cardiac output. Med. Sci. Sports Exerc. 2004, 36, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Vella, C.A.; Robergs, R.A. A review of the stroke volume response to upright exercise in healthy subjects. Br. J. Sports Med. 2005, 39, 190–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colakoglu, M.; Ozkaya, O.; Balci, G.A.; Yapicioglu, B. Shorter intervals at peak SV vs. VO2max may yield high SV with less physiological stress. Eur. J. Sport Sci. 2015, 15, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Colakoglu, M.; Ozkaya, O.; Balci, G.A.; Yapicioglu, B. Stroke volume responses may be related to the gap between peak and maximal O2consumption. Isokinet. Exerc. Sci. 2016, 24, 133–139. [Google Scholar] [CrossRef]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, S.C.; Monteiro, W.D.; Cunha, F.A.; Myers, J.; Farinatti, P.T.V. Determination of best criteria to determine final and initial speeds within ramp exercise testing protocols. Pulm. Med. 2012, 2012, 542402. [Google Scholar] [CrossRef] [PubMed]
- Midgley, A.W.; Carroll, S. Emergence of the verification phase procedure for confirming “true” O2max. Scand. J. Med. Sci. Sports 2009, 19, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Midgley, A.W.; Mcnaughton, L. Criteria for determination of maximal oxygen uptake : A brief critique and recommendations for future Criteria for Determination of Maximal A Brief Critique and Recommendations for Future Research. Sports Med. 2007, 12, 1019–1028. [Google Scholar] [CrossRef]
- Buchfuhrer, M.J.; Hansen, J.E.; Robinson, T.E.; Sue, D.Y.; Wasserman, K.; Whipp, B.J. Optimizing the exercise protocol for cardiopulmonary assessment. J. Appl. Physiol. 1983, 55, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Fontana, P.; Boutellier, U.; Toigo, M. Non-invasive haemodynamic assessments using InnocorTM during standard graded exercise tests. Eur. J. Appl. Physiol. 2010, 108, 573–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattsson, C.M.; Enqvist, J.K.; Brink-Elfegoun, T.; Johansson, P.H.; Bakkman, L.; Ekblom, B. Reversed drift in heart rate but increased oxygen uptake at fixed work rate during 24 h ultra-endurance exercise. Scand. J. Med. Sci. Sports 2010, 20, 298–304. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Continuous | Intermittent | t | p | Cohen’s d |
|---|---|---|---|---|---|
| HR (beat · min−1) | 140.1 (14.8) | 135.2 (11.6) | 3.414 | 0.014 | 0.38 |
| SV (mL) | 138.9 (17.9) | 144.5 (14.6) | −2.860 | 0.029 | −0.34 |
| t→SVmax (min) | 1.5 (0.5) | 10 (2) | 9.245 | 0.000 | −5.83 |
| Qc (L) | 19.3 (2.1) | 19.4 (1.5) | −0.393 | 0.708 | −0.32 |
| a-vO2difference (%) | 13.7 (1.6) | 13.2 (1) | 17.441 | 0.000 | −0.05 |
| O2 (mL · min−1 · kg−1) | 37.3 (2.8) | 36.2 (2.6) | 2.836 | 0.30 | 0.41 |
| RER | 0.86 (0.04) | 0.85 (0.06) | 1.362 | 0.222 | 0.20 |
| RPE | 11.1 (1.3) | 11 (1.8) | 0.420 | 0.689 | 0.06 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colakoglu, M.; Ozkaya, O.; Balci, G.A. Moderate Intensity Intermittent Exercise Modality May Prevent Cardiovascular Drift. Sports 2018, 6, 98. https://doi.org/10.3390/sports6030098
Colakoglu M, Ozkaya O, Balci GA. Moderate Intensity Intermittent Exercise Modality May Prevent Cardiovascular Drift. Sports. 2018; 6(3):98. https://doi.org/10.3390/sports6030098
Chicago/Turabian StyleColakoglu, Muzaffer, Ozgur Ozkaya, and Gorkem Aybars Balci. 2018. "Moderate Intensity Intermittent Exercise Modality May Prevent Cardiovascular Drift" Sports 6, no. 3: 98. https://doi.org/10.3390/sports6030098
APA StyleColakoglu, M., Ozkaya, O., & Balci, G. A. (2018). Moderate Intensity Intermittent Exercise Modality May Prevent Cardiovascular Drift. Sports, 6(3), 98. https://doi.org/10.3390/sports6030098